Richard A. Walker
EPIDEMIOLOGY
![]() The three age-related peaks for drowning are (1) toddlers and young children, (2) adolescents and young adults, and (3) the elderly.
The three age-related peaks for drowning are (1) toddlers and young children, (2) adolescents and young adults, and (3) the elderly.
![]() The elderly are at increased risk of bathtub drowning.
The elderly are at increased risk of bathtub drowning.
![]() Warm, freshwater drowning (especially swimming pools) is more common than salt water drowning, even in coastal areas.
Warm, freshwater drowning (especially swimming pools) is more common than salt water drowning, even in coastal areas.
PATHOPHYSIOLOGY
![]() Prognosis after submersion injuries depends on the degree of pulmonary and central nervous system injury.
Prognosis after submersion injuries depends on the degree of pulmonary and central nervous system injury.
![]() The diving reflex is strongest in infants <6 months old, but decreases with age and may not provide as much cerebral protection as once thought.
The diving reflex is strongest in infants <6 months old, but decreases with age and may not provide as much cerebral protection as once thought.
![]() Cerebral protection in cold water submersion may result from rapid central nervous system (CNS) cooling.
Cerebral protection in cold water submersion may result from rapid central nervous system (CNS) cooling.
![]() “Dry drowning” results from laryngospasm that causes hypoxemia and varying degrees of neurologic insult, and represents up to 20% of submersion injuries.
“Dry drowning” results from laryngospasm that causes hypoxemia and varying degrees of neurologic insult, and represents up to 20% of submersion injuries.
![]() “Wet drowning” consists of aspiration of water into the lungs, causing washout of surfactant, which results in diminished alveolar gas transfer, atelectasis, and ventilation-perfusion mismatch.
“Wet drowning” consists of aspiration of water into the lungs, causing washout of surfactant, which results in diminished alveolar gas transfer, atelectasis, and ventilation-perfusion mismatch.
![]() The majority of patients who arrive at the hospital with stable cardiovascular signs and awake, alert neurologic function survive with minimal disability.
The majority of patients who arrive at the hospital with stable cardiovascular signs and awake, alert neurologic function survive with minimal disability.
![]() Those who arrive with unstable cardiovascular function and coma do poorly because of the hypoxic, ischemic CNS insult.
Those who arrive with unstable cardiovascular function and coma do poorly because of the hypoxic, ischemic CNS insult.
CLINICAL FEATURES
![]() Transient hemodilution may occur in freshwater drownings with large-volume aspiration resulting in hemolysis and hyponatremia.
Transient hemodilution may occur in freshwater drownings with large-volume aspiration resulting in hemolysis and hyponatremia.
![]() Hemoconcentration, hypernatremia, and hyperkale-mia may occur in salt water drowning.
Hemoconcentration, hypernatremia, and hyperkale-mia may occur in salt water drowning.
![]() Noncardiogenic pulmonary edema results from moderate to severe aspiration of water in “wet drowning” cases.
Noncardiogenic pulmonary edema results from moderate to severe aspiration of water in “wet drowning” cases.
![]() Physical examination may reveal clear lungs, rales, rhonchi, or wheezes.
Physical examination may reveal clear lungs, rales, rhonchi, or wheezes.
![]() Mental status may range from normal to comatose.
Mental status may range from normal to comatose.
DIAGNOSIS AND DIFFERENTIAL
![]() Injuries or disorders that precipitate or are associated with submersion events are shown in Table 126-1.
Injuries or disorders that precipitate or are associated with submersion events are shown in Table 126-1.
![]() Laboratory findings may include metabolic acidosis and electrolyte abnormalities if there is associated renal injury from hypoxemia, hemoglobinuria, or myoglobinuria.
Laboratory findings may include metabolic acidosis and electrolyte abnormalities if there is associated renal injury from hypoxemia, hemoglobinuria, or myoglobinuria.
![]() Disseminated intravascular coagulation is rare.
Disseminated intravascular coagulation is rare.
![]() The chest radiograph may be normal or show generalized pulmonary edema or perihilar infiltrates.
The chest radiograph may be normal or show generalized pulmonary edema or perihilar infiltrates.
![]() Since the chest radiograph findings may not correlate with the arterial Po2, an arterial blood gas (ABG) analysis to assess oxygen saturation and metabolic acidosis is important.
Since the chest radiograph findings may not correlate with the arterial Po2, an arterial blood gas (ABG) analysis to assess oxygen saturation and metabolic acidosis is important.
TABLE 126-1 Injuries and Disorders Associated with Submersion Events
Spinal cord injuries that occur after diving into shallow water or in boating mishaps
Hypothermia
Panicking
Syncope (eg, due to hyperventilation prior to underwater diving) Seizures
Other premorbid conditions (eg, dysrhythmias, heart disease)
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment for submersion events is summarized in Fig. 126-1.
Treatment for submersion events is summarized in Fig. 126-1.
![]() All patients should have their airway, ventilation, and oxygenation status assessed. The cervical spine should be stabilized and evaluated in cases of diving accidents, multiple trauma, or if the circumstances are unknown.
All patients should have their airway, ventilation, and oxygenation status assessed. The cervical spine should be stabilized and evaluated in cases of diving accidents, multiple trauma, or if the circumstances are unknown.
![]() Warmed IV normal saline and warming adjuncts (overhead warmer, bear hugger, etc.) should be used if the patient is hypothermie. The patient’s core temperature should be monitored.
Warmed IV normal saline and warming adjuncts (overhead warmer, bear hugger, etc.) should be used if the patient is hypothermie. The patient’s core temperature should be monitored.
![]() Patients with a Glasgow Coma Scale (GCS) score >14 and oxygen saturation (Sao2) ≥95% may be discharged home after a 4- to 6-hour observation period as long as their pulmonary and neurologic examinations and Sao2 remain normal.
Patients with a Glasgow Coma Scale (GCS) score >14 and oxygen saturation (Sao2) ≥95% may be discharged home after a 4- to 6-hour observation period as long as their pulmonary and neurologic examinations and Sao2 remain normal.
![]() The patient with an oxygen requirement or abnormal pulmonary examination after 4 to 6 hours should be admitted.
The patient with an oxygen requirement or abnormal pulmonary examination after 4 to 6 hours should be admitted.
![]() Patients with a GCS <14 should be administered supplemental oxygen. Intubation and mechanical ventilation are indicated if the Pao2 cannot be maintained >60 mm Hg in adults or >80 mm Hg in children, despite high-flow oxygen (40-60%).
Patients with a GCS <14 should be administered supplemental oxygen. Intubation and mechanical ventilation are indicated if the Pao2 cannot be maintained >60 mm Hg in adults or >80 mm Hg in children, despite high-flow oxygen (40-60%).
![]() Antibiotics are usually administered to treat pulmonary aspiration and possible contamination with Aeromonas species, but there is no data to support or refute this practice.
Antibiotics are usually administered to treat pulmonary aspiration and possible contamination with Aeromonas species, but there is no data to support or refute this practice.
![]() Childhood victims of freshwater near drowning rarely develop dilutional hyponatremia and seizures, which are usually easily controlled by correction of the electrolyte abnormality.
Childhood victims of freshwater near drowning rarely develop dilutional hyponatremia and seizures, which are usually easily controlled by correction of the electrolyte abnormality.
![]() Efforts at “brain resuscitation,” including the use of mannitol, loop diuretics, hypertonic saline, fluid restriction, mechanical hyperventilation, controlled hypothermia, barbiturate coma, and intracranial pressure monitoring have not shown benefit.
Efforts at “brain resuscitation,” including the use of mannitol, loop diuretics, hypertonic saline, fluid restriction, mechanical hyperventilation, controlled hypothermia, barbiturate coma, and intracranial pressure monitoring have not shown benefit.
![]() Continuous infusion of vasopressors may be required in the postresuscitation phase.
Continuous infusion of vasopressors may be required in the postresuscitation phase.
![]() Factors associated with after a poor prognosis in warm-water drowning include bystander CPR at the scene, cardiopulmonary resuscitation (CPR) in the ED, and asystole at the scene or in the ED.
Factors associated with after a poor prognosis in warm-water drowning include bystander CPR at the scene, cardiopulmonary resuscitation (CPR) in the ED, and asystole at the scene or in the ED.
![]() Consideration should be given to withholding resuscitation in patients with prolonged submersion and transport.
Consideration should be given to withholding resuscitation in patients with prolonged submersion and transport.
![]() Reports of complete and near-complete neurologic recovery after asystole in adults and children have been reported in prolonged icy-water submersion.
Reports of complete and near-complete neurologic recovery after asystole in adults and children have been reported in prolonged icy-water submersion.
![]() Hypothermic victims of cold-water submersion in cardiac arrest should undergo prolonged and aggressive resuscitation maneuvers until they are normothermic or considered not viable.
Hypothermic victims of cold-water submersion in cardiac arrest should undergo prolonged and aggressive resuscitation maneuvers until they are normothermic or considered not viable.
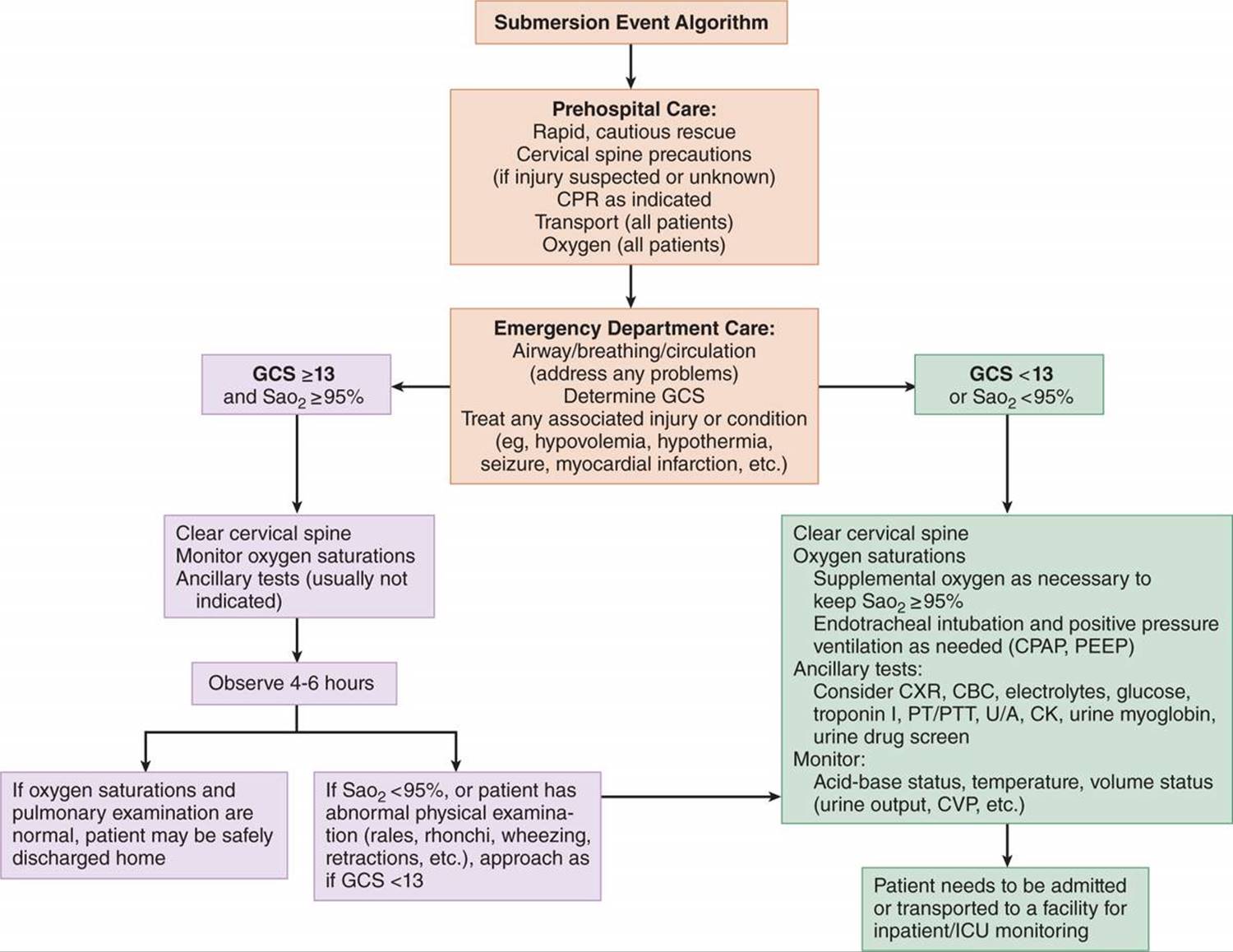
FIG. 126-1. Submersion event algorithm. CBC = complete blood count; CK = creatine kinase; CPAP = continuous positive airway pressure; CVP = central venous pressure; CXR = chest radiograph; GCS = Glasgow Coma Scale score; ICU = intensive care unit; PEEP = positive end-expiratory pressure; PT = prothrombin time; PTT = partial thromboplastin time; Sao2 = oxygen saturation (via pulse oximetry); U/A = urinalysis.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 209, “Near Drowning,” by Alan L. Causey and Mark A. Nichter.