O. John Ma
EPIDEMIOLOGY
![]() The vast majority (80%) of traumatic brain injuries (TBIs) in the United States are mild.
The vast majority (80%) of traumatic brain injuries (TBIs) in the United States are mild.
![]() Approximately 40% of patients with moderate TBI have an abnormal finding on CT and 8% require neurosurgical intervention.
Approximately 40% of patients with moderate TBI have an abnormal finding on CT and 8% require neurosurgical intervention.
![]() Elderly individuals, children, and alcoholics are at greater risk for TBI.
Elderly individuals, children, and alcoholics are at greater risk for TBI.
PATHOPHYSIOLOGY
![]() Direct injury is caused immediately by the forces of an object striking the head or by penetrating injury.
Direct injury is caused immediately by the forces of an object striking the head or by penetrating injury.
![]() Indirect injuries are from acceleration/deceleration forces that result in the movement of the brain inside the skull.
Indirect injuries are from acceleration/deceleration forces that result in the movement of the brain inside the skull.
![]() Secondary insults that may worsen the clinical outcome of TBI patients include cerebral edema, hypoxemia, hypotension, anemia, and elevated intracranial pressure (ICP).
Secondary insults that may worsen the clinical outcome of TBI patients include cerebral edema, hypoxemia, hypotension, anemia, and elevated intracranial pressure (ICP).
![]() Cerebral perfusion pressure (CPP) is the difference between the mean arterial pressure (MAP) and the IC P. Elevation of the IC P and/or hypotension results in a depressed CPP and leads to further brain injury.
Cerebral perfusion pressure (CPP) is the difference between the mean arterial pressure (MAP) and the IC P. Elevation of the IC P and/or hypotension results in a depressed CPP and leads to further brain injury.
![]() Rapid rises in the ICP can lead to the “Cushing reflex,” which is characterized by hypertension, bradycardia, and respiratory irregularities. The Cushing reflex is seen uncommonly and usually occurs in children.
Rapid rises in the ICP can lead to the “Cushing reflex,” which is characterized by hypertension, bradycardia, and respiratory irregularities. The Cushing reflex is seen uncommonly and usually occurs in children.
CLINICAL FEATURES
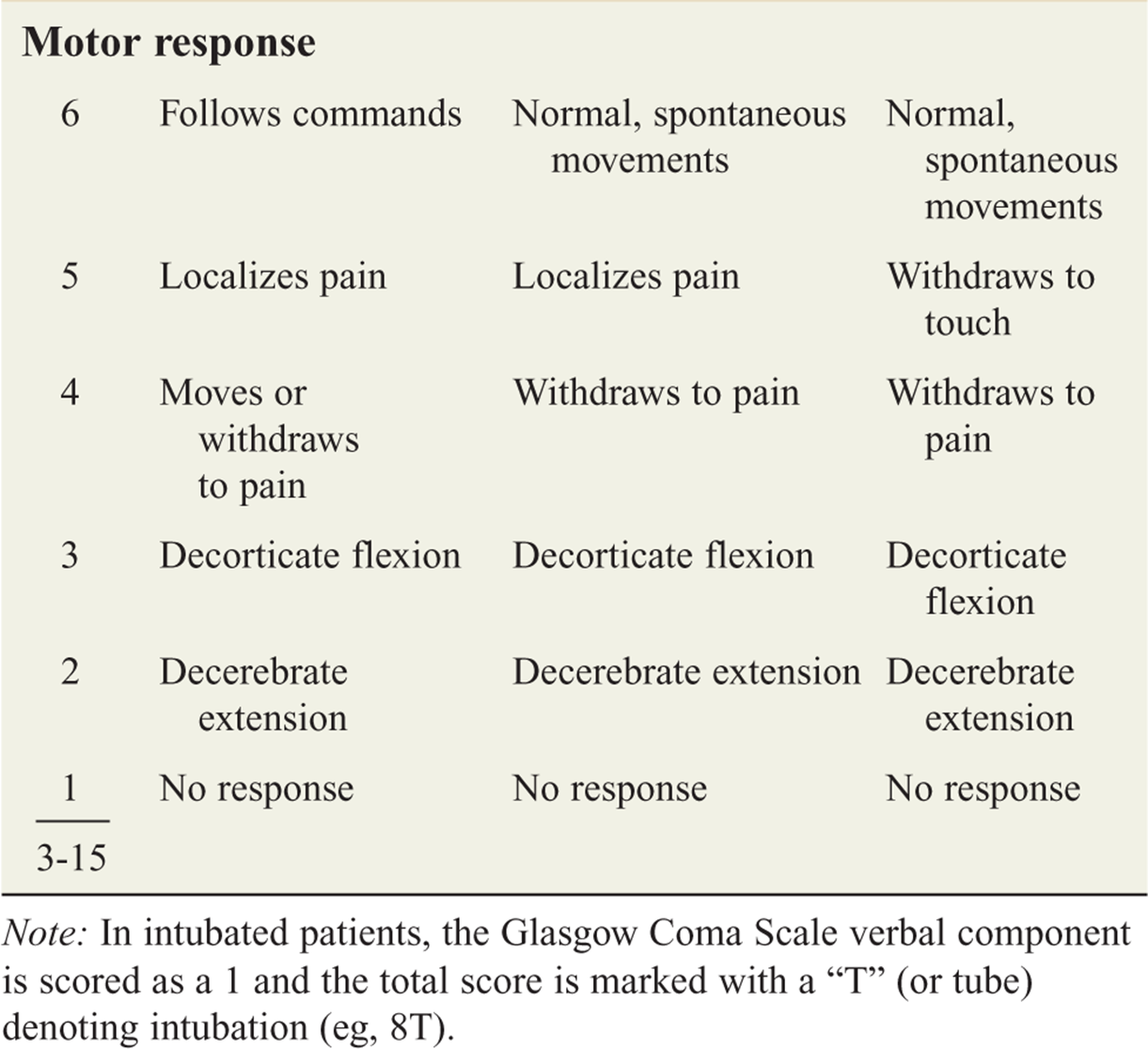
![]() TBI is classified as mild, moderate, or severe based on the Glasgow Coma Scale (GCS, see Table 162-1) score.
TBI is classified as mild, moderate, or severe based on the Glasgow Coma Scale (GCS, see Table 162-1) score.
![]() Mild TBIs include patients with a GCS score ≥14. Patients may be asymptomatic with only a history of head trauma, or may be confused and amnestic of the event. They may have experienced a brief loss of consciousness and complain of a diffuse headache, nausea, and vomiting. Patients at high risk in this subgroup include those with a skull fracture, large subgaleal swelling, focal neurologic findings, coagulopathy, age >60 years, or drug/alcohol intoxication.
Mild TBIs include patients with a GCS score ≥14. Patients may be asymptomatic with only a history of head trauma, or may be confused and amnestic of the event. They may have experienced a brief loss of consciousness and complain of a diffuse headache, nausea, and vomiting. Patients at high risk in this subgroup include those with a skull fracture, large subgaleal swelling, focal neurologic findings, coagulopathy, age >60 years, or drug/alcohol intoxication.
![]() Moderate TBIs include patients with a GCS score of 9 to 13.
Moderate TBIs include patients with a GCS score of 9 to 13.
![]() Severe TBI (GCS score <9) mortality approaches 40%. The immediate clinical priority in these patients is to prevent secondary brain injury, identify other life-threatening injuries, and identify treatable neurosurgical conditions.
Severe TBI (GCS score <9) mortality approaches 40%. The immediate clinical priority in these patients is to prevent secondary brain injury, identify other life-threatening injuries, and identify treatable neurosurgical conditions.
![]() Prehospital medical personnel often may provide critical parts of the history, including mechanism and time of injury, presence and length of unconsciousness, initial mental status, seizure activity, vomiting, verbalization, and movement of extremities. For an unresponsive patient, contact family and friends to gather key information, including past medical history, medications (especially anticoagulants), and recent use of alcohol or drugs.
Prehospital medical personnel often may provide critical parts of the history, including mechanism and time of injury, presence and length of unconsciousness, initial mental status, seizure activity, vomiting, verbalization, and movement of extremities. For an unresponsive patient, contact family and friends to gather key information, including past medical history, medications (especially anticoagulants), and recent use of alcohol or drugs.
![]() Clinically important features of the neurologic examination that should be addressed include assessing the mental status and GCS score; pupils for size, reactivity, and anisocoria; cranial nerve function; motor, sensory, and brain stem function; and noting any development of decorticate or decerebrate posturing.
Clinically important features of the neurologic examination that should be addressed include assessing the mental status and GCS score; pupils for size, reactivity, and anisocoria; cranial nerve function; motor, sensory, and brain stem function; and noting any development of decorticate or decerebrate posturing.
![]() Infants with TBI demonstrate a global diminished level of responsiveness. Pupillary or facial asymmetry, extremity motor function abnormality, or a decreased sucking reflex may be found. Signs of increased intracranial pressure in infants include decreased arousal, lethargy, seizure, vomiting, apnea, and bradycardia.
Infants with TBI demonstrate a global diminished level of responsiveness. Pupillary or facial asymmetry, extremity motor function abnormality, or a decreased sucking reflex may be found. Signs of increased intracranial pressure in infants include decreased arousal, lethargy, seizure, vomiting, apnea, and bradycardia.
![]() Signs or symptoms of TBI in the older child include headache, nausea, vomiting, diminished level of consciousness, motor weakness, visual changes, hypertension, bradycardia, and respiratory arrest.
Signs or symptoms of TBI in the older child include headache, nausea, vomiting, diminished level of consciousness, motor weakness, visual changes, hypertension, bradycardia, and respiratory arrest.
TABLE 162-1 Glasgow Coma Scale for All Age Groups

SPECIFIC INJURIES
SKULL FRACTURES
![]() Depressed skull fractures are classified as open or closed, depending on the integrity of the overlying scalp.
Depressed skull fractures are classified as open or closed, depending on the integrity of the overlying scalp.
![]() Although basilar skull fractures can occur at any point in the base of the skull, the typical location is in the petrous portion of the temporal bone. Findings associated with a basilar skull fracture include hemotympanum, cerebrospinal fluid (CSF) otorrhea or rhinorrhea, periorbital ecchymosis (“raccoon eyes”), and retroauricular ecchymosis (Battle’s sign).
Although basilar skull fractures can occur at any point in the base of the skull, the typical location is in the petrous portion of the temporal bone. Findings associated with a basilar skull fracture include hemotympanum, cerebrospinal fluid (CSF) otorrhea or rhinorrhea, periorbital ecchymosis (“raccoon eyes”), and retroauricular ecchymosis (Battle’s sign).
![]() In children, linear skull fractures that result from a fall from a small height (<4 ft) generally are not associated with the development of clinically significant intracranial lesions. Significant intracranial injuries in children often occur after falls from more extreme heights or higher impact collisions.
In children, linear skull fractures that result from a fall from a small height (<4 ft) generally are not associated with the development of clinically significant intracranial lesions. Significant intracranial injuries in children often occur after falls from more extreme heights or higher impact collisions.
CEREBRAL CONTUSION AND INTRACEREBRAL HEMORRHAGE
![]() Common locations for contusions are the frontal poles, the subfrontal cortex, and the temporal lobes.
Common locations for contusions are the frontal poles, the subfrontal cortex, and the temporal lobes.
![]() Contusions may occur directly under the site of impact or on the contralateral side (contrecoup lesion). The contused area is usually hemorrhagic with surrounding edema, and occasionally associated with subarachnoid hemorrhage.
Contusions may occur directly under the site of impact or on the contralateral side (contrecoup lesion). The contused area is usually hemorrhagic with surrounding edema, and occasionally associated with subarachnoid hemorrhage.
![]() Neurologic dysfunction may be profound and prolonged, with patients demonstrating mental confusion, obtundation, or coma. Focal neurologic deficits are usually present.
Neurologic dysfunction may be profound and prolonged, with patients demonstrating mental confusion, obtundation, or coma. Focal neurologic deficits are usually present.
TRAUMATIC SUBARACHNOID HEMORRHAGE
![]() This condition results from the disruption of subarachnoid vessels and presents with blood in the CSF. Patients may complain of diffuse headache, nausea, or photophobia.
This condition results from the disruption of subarachnoid vessels and presents with blood in the CSF. Patients may complain of diffuse headache, nausea, or photophobia.
![]() Traumatic subarachnoid hemorrhage may be the most common CT abnormality in patients with moderate or severe TBI. Some cases may be missed if the CT scan is obtained less than 6 hours after injury.
Traumatic subarachnoid hemorrhage may be the most common CT abnormality in patients with moderate or severe TBI. Some cases may be missed if the CT scan is obtained less than 6 hours after injury.
EPIDURAL HEMATOMA
![]() An epidural hematoma results from an acute collection of blood between the inner table of the skull and the dura mater. It is typically associated with a skull fracture that lacerates a meningeal artery, most commonly the middle meningeal artery.
An epidural hematoma results from an acute collection of blood between the inner table of the skull and the dura mater. It is typically associated with a skull fracture that lacerates a meningeal artery, most commonly the middle meningeal artery.
![]() Underlying injury to the brain may not necessarily be severe.
Underlying injury to the brain may not necessarily be severe.
![]() In the classic scenario, the patient experiences loss of consciousness after a head injury. The patient may present to the ED with clear mentation, signifying the “lucid interval,” and then begin to develop mental status deterioration in the ED. A fixed and dilated pupil on the side of the lesion with contralateral hemiparesis is a classic late finding.
In the classic scenario, the patient experiences loss of consciousness after a head injury. The patient may present to the ED with clear mentation, signifying the “lucid interval,” and then begin to develop mental status deterioration in the ED. A fixed and dilated pupil on the side of the lesion with contralateral hemiparesis is a classic late finding.
![]() The high-pressure arterial bleeding of an epidural hematoma can lead to herniation within hours of injury.
The high-pressure arterial bleeding of an epidural hematoma can lead to herniation within hours of injury.
![]() An epidural hematoma appears biconvex on CT scan.
An epidural hematoma appears biconvex on CT scan.
SUBDURAL HEMATOMA
![]() A subdural hematoma (SDH), which is a collection of venous blood between the dura mater and the arachnoid, results from tears of the bridging veins that extend from the subarachnoid space to the dural venous sinuses.
A subdural hematoma (SDH), which is a collection of venous blood between the dura mater and the arachnoid, results from tears of the bridging veins that extend from the subarachnoid space to the dural venous sinuses.
![]() A common mechanism is sudden acceleration–deceleration. Patients with brain atrophy, such as in alcoholics or the elderly, are more susceptible to an SDH.
A common mechanism is sudden acceleration–deceleration. Patients with brain atrophy, such as in alcoholics or the elderly, are more susceptible to an SDH.
![]() In infants, SDH is strongly associated with nonaccidental trauma. In acute SDH, patients present within 14 days of the injury, and most become symptomatic within 24 hours of injury.
In infants, SDH is strongly associated with nonaccidental trauma. In acute SDH, patients present within 14 days of the injury, and most become symptomatic within 24 hours of injury.
![]() After 2 weeks, patients are defined as having a chronic SDH.
After 2 weeks, patients are defined as having a chronic SDH.
![]() Symptoms may range from a headache to lethargy or coma. It is important to distinguish between acute and chronic SDHs by history, physical examination, and CT scan.
Symptoms may range from a headache to lethargy or coma. It is important to distinguish between acute and chronic SDHs by history, physical examination, and CT scan.
![]() An acute SDH appears as a hyperdense, crescentshaped lesion that crosses suture lines.
An acute SDH appears as a hyperdense, crescentshaped lesion that crosses suture lines.
HERNIATION
![]() Diffusely or focally increased ICP can result in herniation of the brain at several locations.
Diffusely or focally increased ICP can result in herniation of the brain at several locations.
![]() Transtentorial (uncal) herniation occurs when an SDH or temporal lobe mass forces the ipsilateral uncus of the temporal lobe through the tentorial hiatus into the space between the cerebral peduncle and the tentorium. This results in compression of the oculomotor nerve and parasympathetic paralysis of the ipsilateral pupil, causing it to become fixed and dilated. When the cerebral peduncle is further compressed, it results in contralateral motor paralysis. The increased ICP and brain stem compression result in progressive deterioration in the level of consciousness. Occasionally, the contralateral cerebral peduncle is forced against the free edge of the tentorium on the opposite side, resulting in paralysis ipsilateral to the lesion—false localizing sign.
Transtentorial (uncal) herniation occurs when an SDH or temporal lobe mass forces the ipsilateral uncus of the temporal lobe through the tentorial hiatus into the space between the cerebral peduncle and the tentorium. This results in compression of the oculomotor nerve and parasympathetic paralysis of the ipsilateral pupil, causing it to become fixed and dilated. When the cerebral peduncle is further compressed, it results in contralateral motor paralysis. The increased ICP and brain stem compression result in progressive deterioration in the level of consciousness. Occasionally, the contralateral cerebral peduncle is forced against the free edge of the tentorium on the opposite side, resulting in paralysis ipsilateral to the lesion—false localizing sign.
![]() Central transtentorial herniation occurs with midline lesions in the frontal or occipital lobes, or in the vertex. Bilateral pinpoint pupils, bilateral Babinski signs, and increased muscle tone are found initially, which eventually develop into fixed midpoint pupils, prolonged hyperventilation, and decorticate posturing.
Central transtentorial herniation occurs with midline lesions in the frontal or occipital lobes, or in the vertex. Bilateral pinpoint pupils, bilateral Babinski signs, and increased muscle tone are found initially, which eventually develop into fixed midpoint pupils, prolonged hyperventilation, and decorticate posturing.
![]() Cerebellotonsillar herniation through the foramen magnum occurs much less frequently. Medullary compression causes flaccid paralysis, bradycardia, respiratory arrest, and sudden death.
Cerebellotonsillar herniation through the foramen magnum occurs much less frequently. Medullary compression causes flaccid paralysis, bradycardia, respiratory arrest, and sudden death.
PENETRATING INJURIES
![]() Gunshot wounds and penetrating sharp objects can result in penetrating injury to the brain. The degree of neurologic injury will depend on the energy of the missile, whether the trajectory involves a single or multiple lobes or hemispheres of the brain, the amount of scatter of bone and metallic fragments, and whether a mass lesion is present.
Gunshot wounds and penetrating sharp objects can result in penetrating injury to the brain. The degree of neurologic injury will depend on the energy of the missile, whether the trajectory involves a single or multiple lobes or hemispheres of the brain, the amount of scatter of bone and metallic fragments, and whether a mass lesion is present.
SHAKEN BABY SYNDROME
![]() This potential life-threatening head injury in children <2 years is caused by rapid acceleration and rotation of the head. Shearing injuries of the brain or intracranial vessels and cervical spine injuries may result. Almost half of children found with this syndrome exhibit no external signs of trauma, so clinical vigilance must remain high.
This potential life-threatening head injury in children <2 years is caused by rapid acceleration and rotation of the head. Shearing injuries of the brain or intracranial vessels and cervical spine injuries may result. Almost half of children found with this syndrome exhibit no external signs of trauma, so clinical vigilance must remain high.
DIAGNOSIS AND DIFFERENTIAL
![]() Tables 162-2 and 162-3 provide evidence-based indications for obtaining a CT scan of the head after injury.
Tables 162-2 and 162-3 provide evidence-based indications for obtaining a CT scan of the head after injury.
![]() Approximately 8% of patients suffering a severe TBI will have an associated cervical spine fracture. Obtain imaging studies of the cervical spine on all trauma patients who present with altered mental status, neck pain, intoxication, neurologic deficit, or severe distracting injury, or if the mechanism of injury is deemed serious enough to potentially produce cervical spine injury.
Approximately 8% of patients suffering a severe TBI will have an associated cervical spine fracture. Obtain imaging studies of the cervical spine on all trauma patients who present with altered mental status, neck pain, intoxication, neurologic deficit, or severe distracting injury, or if the mechanism of injury is deemed serious enough to potentially produce cervical spine injury.
![]() Laboratory work should include type and crossmatching, complete blood count, basic metabolic panel, arterial blood gas analysis, directed toxicologic studies, and coagulation studies.
Laboratory work should include type and crossmatching, complete blood count, basic metabolic panel, arterial blood gas analysis, directed toxicologic studies, and coagulation studies.
TABLE 162-2 New Orleans and Canadian CT Clinical Decision Rules

TABLE 162-3 Summary of Indications for CT Scanning for Adults with Mild Traumatic Brain Injury (TBI)

EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Initiate standard protocols for evaluation and stabilization of trauma patients. Search carefully for other significant injuries.
Initiate standard protocols for evaluation and stabilization of trauma patients. Search carefully for other significant injuries.
![]() Administer 100% oxygen, and secure cardiac monitoring and two IV lines. For patients with severe TBI, endotracheal intubation (via rapid sequence intubation) to protect the airway and prevent hypoxemia is the top priority. Provide cervical spine immobilization, and use an adequate sedation/induction agent when securing the airway.
Administer 100% oxygen, and secure cardiac monitoring and two IV lines. For patients with severe TBI, endotracheal intubation (via rapid sequence intubation) to protect the airway and prevent hypoxemia is the top priority. Provide cervical spine immobilization, and use an adequate sedation/induction agent when securing the airway.
![]() Hypotension is associated with increased mortality rates. Restoration of an adequate blood pressure is vital to maintain cerebral perfusion. Resuscitation with IV crystalloid fluid to an MAP ≥80 mm Hg is indicated; if aggressive fluid resuscitation is not effective, then add vasopressors to maintain an MAP ≥80 mm Hg.
Hypotension is associated with increased mortality rates. Restoration of an adequate blood pressure is vital to maintain cerebral perfusion. Resuscitation with IV crystalloid fluid to an MAP ≥80 mm Hg is indicated; if aggressive fluid resuscitation is not effective, then add vasopressors to maintain an MAP ≥80 mm Hg.
![]() Obtain immediate neurosurgical consultation after a head CT scan demonstrating intracranial injury has been identified. Patients with new neurologic deficits from an acute epidural or SDH require emergent neurosurgical treatment.
Obtain immediate neurosurgical consultation after a head CT scan demonstrating intracranial injury has been identified. Patients with new neurologic deficits from an acute epidural or SDH require emergent neurosurgical treatment.
![]() All patients who demonstrate signs of increased IC P should have the head of their bed elevated 30 degrees (provided that the patient is not hypotensive), adequate sedation, and maintenance of adequate arterial oxygenation. If the patient is not hypotensive, consider administering mannitol, 0.25 to 1.0 gram/kg IV bolus.
All patients who demonstrate signs of increased IC P should have the head of their bed elevated 30 degrees (provided that the patient is not hypotensive), adequate sedation, and maintenance of adequate arterial oxygenation. If the patient is not hypotensive, consider administering mannitol, 0.25 to 1.0 gram/kg IV bolus.
![]() Hyperventilation is not recommended as a prophylactic intervention to lower ICP because of its potential to cause cerebral ischemia. Reserve hyperventilation as a last resort for lowering ICP; if used, implement it as a temporary measure and monitor the Pco2 closely to maintain a range of 30 to 35 mm Hg.
Hyperventilation is not recommended as a prophylactic intervention to lower ICP because of its potential to cause cerebral ischemia. Reserve hyperventilation as a last resort for lowering ICP; if used, implement it as a temporary measure and monitor the Pco2 closely to maintain a range of 30 to 35 mm Hg.
![]() Patients with signs of impending brain herniation may need emergency decompression by trephination (“burr holes”) when all other methods to control the elevated ICP have failed. CT scan prior to attempting trephination is recommended to localize the lesion and direct the decompression site.
Patients with signs of impending brain herniation may need emergency decompression by trephination (“burr holes”) when all other methods to control the elevated ICP have failed. CT scan prior to attempting trephination is recommended to localize the lesion and direct the decompression site.
![]() Treat seizures immediately with benzodiazepines, such as lorazepam, and fosphenytoin at a loading dose of 18 to 20 milligrams PE/kg IV.
Treat seizures immediately with benzodiazepines, such as lorazepam, and fosphenytoin at a loading dose of 18 to 20 milligrams PE/kg IV.
![]() Use of prophylactic anticonvulsants remains controversial, and its administration should be in consultation with the neurosurgeon.
Use of prophylactic anticonvulsants remains controversial, and its administration should be in consultation with the neurosurgeon.
![]() Admit patients with a basilar skull fracture or penetrating injuries (gunshot wound or stab wound) to the neurosurgical service, and start them on prophylactic antibiotic therapy (eg, ceftriaxone 1 gram every 12 hours).
Admit patients with a basilar skull fracture or penetrating injuries (gunshot wound or stab wound) to the neurosurgical service, and start them on prophylactic antibiotic therapy (eg, ceftriaxone 1 gram every 12 hours).
![]() Discharge patients who have an initial GCS score of 15 that is maintained during an observation period and who have normal serial neurologic examinations and a normal CT scan.
Discharge patients who have an initial GCS score of 15 that is maintained during an observation period and who have normal serial neurologic examinations and a normal CT scan.
![]() Those who have an abnormal CT scan require neurosurgical consultation and admission.
Those who have an abnormal CT scan require neurosurgical consultation and admission.
![]() Patients who have an initial GCS score of 14 and a normal CT scan should be observed in the ED. If their GCS score improves to 15 and they remain symptom free and neurologically intact after serial examinations, they can be discharged home.
Patients who have an initial GCS score of 14 and a normal CT scan should be observed in the ED. If their GCS score improves to 15 and they remain symptom free and neurologically intact after serial examinations, they can be discharged home.
![]() Discharge patients home with a reliable companion who can observe them for at least 24 hours, carry out appropriate discharge instructions, and follow the head injury sheet instructions.
Discharge patients home with a reliable companion who can observe them for at least 24 hours, carry out appropriate discharge instructions, and follow the head injury sheet instructions.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 254, “Head Trauma in Adults and Children,” by David W. Wright and Lisa H. Merck.