The spleen, the largest of the lymphoid organs (see p. 9), lies under the diaphragm on the left side of the abdomen (Fig. 5.26), and although not part of the alimentary tract it drains to the portal venous system.
The odd numbers 1, 3, 5, 7, 9, 11 summarize some splenic statistics. It measures 1 × 3 × 5 inches, weighs 7 oz and lies deep to the left 9th to 11th ribs (H. A. Harris). These are average measurements; the size of the spleen varies considerably.
Being developed in the dorsal mesogastrium (see below), the spleen projects into the greater sac surrounded by peritoneum of the original left leaf of the dorsal mesogastrium. It lies at the left margin of the lesser sac (Fig. 5.49) below the diaphragm, and its diaphragmatic surface is moulded into a reciprocal convexity. Its hilum lies in the angle between the stomach and left kidney, each of which impresses a concavity alongside the attached splenic vessels (Fig. 5.41). Its long axis lies along the line of the tenth rib, and its lower pole does not normally project any further forward than the midaxillary line. A small colic area lies in contact with the splenic flexure and the phrenicocolic ligament. Its anterior border is notched, a relic of the fusion of the several ‘splenules’ from which the organ arises in the embryo.
|
|
|
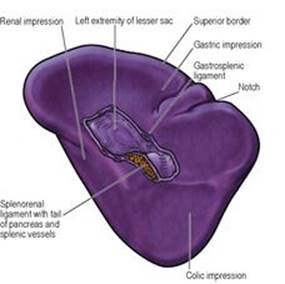
Figure 5.41 Visceral surface of the spleen, showing the impressions for adjacent viscera and the two layers of peritoneum that form the splenorenal and gastrosplenic ligaments. |
Its visceral peritoneum, or serous coat, invests all surfaces (gastric, diaphragmatic, colic and renal). The two leaves of the greater omentum pass from the hilum forwards to the greater curvature of the stomach (the gastrosplenic ligament) and backwards to the front of the left kidney (the splenorenal ligament) (Fig. 5.49). The hilum of the spleen makes contact with the tail of the pancreas, which lies within the splenorenal ligament.
If the spleen enlarges, its long axis extends downwards and forwards in the direction of the umbilicus, and its anterior border approaches the costal margin to the left of the greater curvature of the stomach. (A kidney enlarging downwards does so in the direction of the iliac fossa.) The spleen must at least double its normal size before its anterior border passes beyond the left costal margin. A palpable spleen is identified by the notch in its anterior border. In some diseases the spleen is grossly enlarged and may extend across the upper abdomen beyond the umbilicus towards the right iliac fossa. Whatever the degree of enlargement the spleen glides in contact with the diaphragm and anterior abdominal wall in front of the splenic flexure, which remains anchored by the phrenicocolic ligament, and no colonic resonance is found on percussion over the organ. Retroperitoneal tumours (e.g. of the left kidney) do not displace the overlying colon and they are crossed by a band of colonic resonance.
The structures that are related to the surfaces of the spleen can be identified by holding the convexity (diaphragmatic surface) of the detached organ in the hollow of the left hand, and rotating it until the notched anterior border lies to the front, near the thumb (Fig. 5.41). The concavity between the notched anterior border and the hilum is the gastric impression. Behind the hilum is the concave renal surface, while at the lower pole (at the tip of the little finger of the left hand) is the small colic impression.
The structure of the spleen has been referred to on page 9.
Blood supply
The splenic artery passes between the layers of the splenorenal ligament and at the hilum divides into two or three main branches, from which five or more branches enter the spleen. Veins accompany the arteries and unite to form the splenic vein. Based on the vascular arrangement, it is possible that the spleen consists of two or three segments, with intersegmental vessels being small and scanty, but the evidence for such segmentation is not conclusive.
Lymph drainage
Lymph drains into several nodes lying at the hilum and thence, by way of the pancreaticosplenic nodes, to the coeliac nodes.
Nerve supply
The spleen is supplied from the coeliac plexus with sympathetic fibres only.
Development
The spleen begins to develop in the sixth week as several condensations of mesodermal cells in the dorsal mesogastrium which, because of the splenic presence, becomes divided into the splenorenal and gastrosplenic ligaments (Fig. 5.21B). The spleen thus comes to lie at the left margin of the lesser sac. The original condensations become aggregated into a single organ; the splenic notch may represent a region where there is incomplete fusion. ‘Accessory spleens’ are the result of lack of fusion; one or several may be found, usually along the splenic vessels or in the peritoneal attachments. They occur in up to 20% of the population and are rarely larger than 2cm in diameter.
Surgical approach
Removal of the spleen (splenectomy) essentially involves cutting its two ‘pedicles’, the splenorenal and gastrosplenic ligaments. In an emergency after rupture with haemorrhage, the left or posterior layer of the splenorenal ligament is incised and the spleen turned medially so that the splenic vessels can be dissected away from the tail of the pancreas and ligated (arteries before veins). The short gastric vessels and the gastrosplenic ligament are then divided and removal completed. For an elective procedure it is usual to enter the lesser sac by dividing the gastrosplenic ligament and its vessels and then to deal with the splenic vessels and the splenorenal ligament. The stomach must not be perforated when ligating the short gastric vessels, and damage to the tail of the pancreas and splenic flexure of the colon must be avoided.