In the male urogenital region two layers of fascia, the superior and inferior fasciae of the urogenital diaphragm, enclose the sphincter urethrae and the deep transverse perineal muscles; together these fasciae and muscles are referred to as the urogenital diaphragm. The superior fascia is thin and ill-defined; the inferior fascia is thicker and termed the perineal membrane. These fascia enclose between them a deep perineal space (pouch) which contains the membranous part of the urethra, the internal pudendal vessels, the dorsal nerve of penis and perineal nerve at the sides, and the paired bulbourethral glands, in addition to the sphincter urethrae and deep transverse perineal muscles.
The perineal membrane is an unyielding sheet of fibrous tissue which forms the base upon which the penis and penile musculature are fixed (Fig. 5.71A). It is attached on either side to the ischiopubic rami from just behind the subpubic angle back to the level of the anterior part of the ischial tuberosities. Its anterior border forms the transverse perineal ligament, and there is a small gap between this and the arcuate pubic ligament through which the deep dorsal vein of the penis passes to reach the vesicoprostatic plexus. Its posterior border fuses centrally with the perineal body. When standing upright, the perineal membrane lies approximately horizontally. Above the membrane lies the membranous urethra surrounded by the urethral sphincter, below the apex of the prostate. The membrane is pierced by the urethra, the ducts of the bulbourethral glands, and by nerves and vessels.
After leaving the prostate just in front of the apex, the prostatic urethra (see p. 299) becomes the membranous urethra which passes down for about 1.5cm and pierces the perineal membrane, 2.5cm behind the pubic symphysis, to become the penile urethra. The membranous urethra is the shortest and least dilatable part of the urethra. In the upper part of its wall there are some smooth muscle fibres continuous with those of the prostatic urethra.
The sphincter urethrae, often called clinically the external urethral sphincter, is roughly pear-shaped. The thinner upper end of the ‘pear’ extends upwards out of the deep perineal pouch to surround the lower part of the prostatic urethra; the lower more bulbous part is below the apex of the prostate and above the perineal membrane. Some of its fibres arise from the pubic rami and pass as U-shaped loops in front of and behind the urethra, some run from the transverse perineal ligament to the perineal body, and some completely encircle the urethra. Although consisting of striated muscle, the sphincter fibres are of small diameter and are of the slow twitch variety. They are supplied by the perineal branch of the pudendal nerve (see p. 321). Above the posterior part of the perineal membrane the deep transverse perineal muscle extends from the ischial ramus to the perineal body, where its fibres decussate with those of the contralateral muscle and the external anal sphincter. It merges anteriorly with the sphincter urethrae and shares the same nerve supply.
The bulbourethral glands (of Cowper) lie one on each side of the membranous urethra in the deep perineal pouch, i.e. above (deep to) the perineal membrane, covered by the urethral sphincter. They are about 1cm in diameter. The single duct from each, about 2.5cm long, pierces the perineal membrane to open into the bulb of the penile urethra. The glands contribute a small amount to seminal fluid.
Deep to the skin of the urogenital region is the superficial perineal fascia (of Colles), a continuation into the perineum of the membranous fascia (of Scarpa) from the anterior abdominal wall (see p. 179). It is attached to the ischiopubic rami and the posterior margin of the perineal membrane, thus closing in a subfascial space, the superficial perineal space (pouch), that is in continuity with the space deep to the membranous (Scarpa's) fascia of the anterior abdominal wall (see Fig. 4.1, p. 180). From its marginal attachments in the urogenital region, this fascia is projected into a bulbous scrotal expansion and a cylindrical penile expansion (Fig. 5.71B), the distal end of the latter being attached round the corona of the glans penis. Rupture of the penile urethra permits extravasation of urine beneath Colles' fascia whence the collection distends the tissues of the scrotum and penis and can then pass upwards over the anterior abdominal wall beneath Scarpa's fascia. A deep perineal fascia intimately surrounds the cavernous bodies of the penis and clitoris and the superficial perineal muscles associated with them.
Penis
The penis has a root and a body. The root of the penis is attached to the inferior surface of the perineal membrane and consists of the (central) bulb of the penis with a crus on each side. Each crus is attached to the angle between the perineal membrane and the everted margin of the ischiopubic ramus, receives the deep artery of the penis near its anterior end, and continues forwards to become the corpus cavernosum. The bulb is the posterior end of the corpus spongiosum. At the front of the root area, below the subpubic angle, the two corpora cavernosa are bound together side by side with the corpus spongiosum behind them (when the penis is dependent, but ventral to them when erect) to form the body of the penis (Fig. 5.72). The penile urethra runs through the whole length of the corpus spongiosum from the bulb at the back to its expanded external end which is the glans penis. The glans forms the tip of the penis, overlapping the distal ends of the corpora cavernosa. The urethra enters the bulb from above near its front so that most of the bulge of the bulb is behind and below the urethra. The bulb has a slight (palpable) midline notch on its under surface and extends back towards the perineal body. The arteries of the bulb enter it near the urethra, which in this region receives the ducts of the bulbourethral glands.
|
|
|
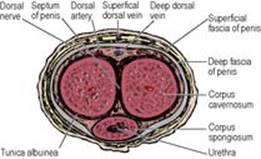
Figure 5.72 Cross-section of the body of the penis. |
The corpus spongiosum and the two corpora cavernosa (Fig. 5.72) are each surrounded by a tough fibrous sheath, the tunica albuginea of the corpus (not to be confused with the tunica albuginea of the testis); that of the corpus spongiosum enlarges distally to enclose the glans. From the tunica fibrous trabeculae pass into the corpora dividing their substance into numerous endothelial cell-lined cavernous spaces into which helicine arteries open (see p. 321). Between the corpora cavernosa there is a connective tissue septum which is partly divided into comb-like strands. The fibrous sheaths of the corpora are encircled by the deep fascia of the penis, an extension of the deep perineal fascia. This fascia is attached to the front surface of the pubic symphysis by a triangular sheet of fibrous tissue, the suspensory ligament of the penis. The midline deep dorsal vein, with a dorsal artery on each side and more laterally a dorsal nerve, lies deep to the deep fascia of the penis.
The skin is hairless and prolonged forwards in a fold, the prepuce, which partly overlaps the glans and doubles back to be attached to the neck of the glans. Beneath the skin is the superficial fascia of the penis (Buck's fascia), a cylindrical prolongation of Colles' fascia (see p. 318), and in the midline is the superficial dorsal vein which is accompanied by lymphatics from the skin and the anterior part of the urethra. On the inferior aspect of the glans, a fold of skin, the frenulum, passes from the prepuce to the ventral end of the urethral orifice.
Blood supply
The penis receives three pairs of arteries which are branches of the internal pudendals (see p. 309). The artery to the bulb supplies the corpus spongiosum, including the glans. The deep artery of the penis supplies the corpus cavernosum. The dorsal artery supplies skin, fascia and glans. There is anastomosis, via the continuity of corpus spongiosum and glans, between the artery of the bulb and the dorsal artery; the deep arteries supply the corpora cavernosa only. The skin of the penis is also supplied by the superficial external pudendal branches of the femoral arteries.
Venous return from the corpora is partly by way of veins that accompany the arteries and join the internal pudendal veins, but mostly by the deep dorsal vein which pierces the suspensory ligament, passes above the perineal membrane and enters the vesicoprostatic venous plexus. The superficial dorsal vein drains the dorsal skin of the penis and divides to join the superficial external pudendal tributaries of the great saphenous veins.
Lymph drainage
Lymphatics from the penile skin pass to superficial inguinal nodes, but the glans and the corpora drain to deep inguinal nodes.
Nerve supply
The skin of the penis is supplied by the pudendal nerves (see p. 311) via the posterior scrotal and dorsal nerves; the latter supply the glans. The dermatome mainly involved is S2. A small area of skin on the dorsum of the proximal penis is supplied by the ilioinguinal nerve (L1). The bulbocavernosus and ischiocavernosus muscles (see below) which contract spasmodically during ejaculation are supplied by the perineal nerve (from the pudendal, S2, 3). The sympathetic nerves necessary for the initial stages of ejaculation (see p. 322) are derived from L1 segment of the spinal cord via the superior and inferior hypogastric plexuses. The pelvic splanchnic nerves (S2, 3) provide the parasympathetic supply to the cavernous tissue of all three corpora and allow increased blood flow for erection (see p. 322).
Circumcision
Ritual circumcision for religious or racial reasons is probably the oldest operation in the world. In children or adults circumcision may be required for a tightly constricting prepuce (phimosis). The prepuce is incised on the dorsum from the tip towards the base of the glans, dissecting away any adhesions, and then the incision is carried circumferentially, followed by suture of the skin edges. Bleeding from a vessel in the frenulum needs to be controlled.
Superficial perineal muscles
The bulb and each crus of the penis are provided with overlying muscles: bulbospongiosus and ischiocavernosus, respectively (Fig. 5.71A). In addition there is a transverse pair (superficial transverse perineal) along the posterior border of the perineal membrane. The three superficial perineal muscles of each side thus form a triangular pattern when viewed in the lithotomy position.
Bulbospongiosus arises from the perineal body and in front of that from a median raphe that joins the pair together. Its posterior fibres are directed forwards and laterally over the bulb to be inserted into the perineal membrane and a dorsal fibrous expansion on the penis; the more posterior of these fibres clasp the corpus spongiosum, while the more anterior extend on to the corpora cavernosa. Bulbospongiosus acts to empty the urethra at the end of micturition, assists in erection (by compressing the deep dorsal vein of the penis) and contracts during ejaculation.
Ischiocavernosus arises from the posterior part of the perineal membrane and from the ischial ramus and is inserted by an aponeurosis on to the surface of the corpus cavernosum. Its function is to assist in the support of, and move slightly, the erect penis.
The superficial transverse perineal muscle arises from the ischial tuberosity and is inserted into the perineal body. It helps to stabilize the perineal body.
Nerve supply. All three muscles are supplied by the perineal branch of the pudendal nerve (S2, 3).
Male urethra
The urethra consists of prostatic, membranous and spongy parts, with a total length of about 20cm. The prostatic and membranous parts have already been described (see pp. 299 and 317).
The spongy or penile urethra, about 15cm long, is within the corpus spongiosum of the penis and can be divided into bulbous and pendulous parts. The posterior part of the corpus, attached to the undersurface of the perineal membrane, is enlarged as the bulb. After piercing the perineal membrane the urethra enters the bulb and at once takes a right-angled curve forwards within the bulb. The urethra continues through the corpus spongiosum beyond the root of the penis into its body. Just proximal to the external urethral meatus at the tip of the glans there is a short dilated region, the navicular fossa. The lining here is stratified squamous epithelium, in contrast to the whole of the rest of the urethra which possesses the transitional epithelium typical of the urinary tract. The urethral mucosa displays some very small blind-ending pockets (lacunae) and there are numerous mucous urethral glands (of Littre). The empty urethra is horizontal in cross-section but the meatus is a vertical slit, hence the spiral stream of urine.
The urethra is narrowest at the external meatus, and shows dilatations in the prostatic part, bulb and navicular fossa. When passing a catheter the 90° change of direction in the bulbar part before the membranous urethra is entered has to be kept in mind. On account of a particularly large lacuna on the roof of the navicular fossa, any instruments being passed through the external meatus should initially be pointed towards the floor of the fossa.
Blood supply
As with many tubular structures, there is no single ‘artery to the urethra’; the blood supply is from any adjacent vessels as it passes through the prostate, sphincter urethrae and corpus spongiosum.
Nerve supply
The mucous membrane of the penile part receives a branch from the perineal nerve, with filaments from the inferior hypogastric plexuses reaching more proximal parts. The urethral sphincters and the control of micturition have been described on page 297–298.
Development
The part of the urethra proximal to the openings of the ejaculatory ducts and prostatic utricle is formed, like the trigone of the bladder, from the lower ends of the mesonephric ducts and ureters that are absorbed into the bladder wall (see p. 29). The rest is from the pelvic and phallic parts of the urogenital sinus and the genital tubercle, supplemented ventrally in the penile part by the fusion of the urogenital folds (see p. 29). The epithelium of the navicular fossa (ectoderm from the genital tubercle) is a solid column that becomes canalized; if it fails to do so, and there is accompanying failure of complete fusion of the urogenital folds, the result is hypospadias—a midline opening on the ventral surface.
Scrotum
The scrotum is a pouch of skin containing the testes and spermatic cords. The subcutaneous tissue has no fat, but contains the dartos muscle which sends a sheet into the midline fibrous septum of the scrotum (Fig. 5.12). The rugosity of the skin is due to contraction of the dartos. The dartos is smooth muscle, and is supplied by sympathetic fibres probably carried by the genital branch of the genitofemoral nerve.
Blood supply
The blood supply of the skin is from the superficial and deep external pudendal arteries (from the femoral) and from scrotal branches of the perineal artery (from the internal pudendal). Venous drainage is mainly by external pudendal veins, superficial and deep, to the great saphenous vein (see Fig. 3.3, p. 114).
Lymph drainage
Lymph drainage is to the superficial inguinal nodes.
Nerve supply
The anterior axial line (see p. 14) crosses the scrotum. The anterior one-third of the scrotal skin is supplied by the ilioinguinal nerve (L1) and the genital branch of the genitofemoral nerve (L1). The posterior two-thirds is supplied by scrotal branches of the perineal nerve (S3), reinforced laterally by the perineal branch of the posterior femoral cutaneous nerve (S2).
Development
The scrotum develops from the labioscrotal swellings and the urogenital folds (see p. 29). Where the urogenital folds meet is marked by a midline cutaneous raphe on the scrotum, which continues on to the inferior surface of the penis. (In the female, the labioscrotal folds form the labia majora, and the urogenital folds remain separate as the labia minora.)
Perineal vessels and nerves
The internal pudendal artery (see p. 309) enters the deep perineal pouch from the anterior end of the pudendal canal and passes forwards along the ischiopubic ramus above the perineal membrane, with the dorsal nerve of penis above it and the perineal nerve below it. The perineal branch of the artery pierces the posterior angle of the perineal membrane and gives origin to posterior scrotal and transverse perineal branches. Further forward another branch, artery to the bulb, pierces the membrane alongside the urethra to enter the corpus spongiosum. It gives branches to the cavernous tissue of this corpus and passes forwards to supply the glans penis.
Near the anterior margin of the perineal membrane the internal pudendal artery divides into its terminal branches, the deep and dorsal arteries of the penis. The deep artery pierces the membrane to enter the crus of the penis and supplies, by its helicine branches, the erectile cavernous tissue of the corpus cavernosum. The dorsal artery pierces the membrane and passes between the crus and the pubic symphysis to pierce the suspensory ligament and run forward, alongside the median deep dorsal vein and with the dorsal nerves laterally, between the deep fascia of the penis and the fibrous sheaths of the corpora cavernosa. The arteries pass to the glans where they anastomose with the terminal branches of the arteries to the bulb.
The deep dorsal vein of the penis drains most of the blood from the corpora. It runs proximally in the midline, pierces the suspensory ligament and passes upwards in the gap between the pubic symphysis (arcuate pubic ligament) and the perineal membrane to enter the pelvis and join the vesicoprostatic plexus.
The pudendal nerve (see p. 311) divides within the pudendal canal into its terminal branches, the dorsal nerve of the penis and the perineal nerve. Both enter the deep perineal pouch, running forwards respectively above and below the internal pudendal artery. The dorsal nerve of the penis appears to be the direct continuation of the pudendal nerve. It pierces the anterior angle of the perineal membrane and then accompanies the dorsal artery on its lateral side. It supplies the skin of the penis and glans and gives branches to the corpus cavernosum. It has no branches in the deep perineal pouch.
The perineal nerve, which is the larger terminal branch of the pudendal, gives muscular branches to the superficial and deep perineal muscles and to the sphincter urethrae. The branch to bulbospongiosus supplies sensory fibres to the mucous membrane of the urethra. Either before or just after entering the deep perineal pouch the perineal nerve gives off the posterior scrotal branches which run forwards superficial to the perineal membrane to supply scrotal skin.
Erection and ejaculation
The neural controls of erection and ejaculation are different; erection is parasympathetic and ejaculation is sympathetic and somatic. Impulses in the genital branches of the pelvic splanchnic nerves (parasympathetic) lead to vasodilatation of the helicine arteries of the erectile tissue of the corpora cavernosa (hence the old name of nervi erigentes). As the spongy tissue becomes engorged there may be some compression of the draining veins, but erection (whether reflex from physical stimulation or psychogenic) occurs mainly by increased arterial flow following relaxation of smooth muscle in the trabeculae of the corpora, which is dependent on the production of nitrous oxide and cyclic GMP.
The sympathetic outflow from segments T11 to L2 to the epididymis, vas deferens, seminal vesicle, ejaculatory duct, prostate, superficial trigonal muscle of the bladder and circular muscle of the bladder neck causes contraction of the smooth muscle of those structures, so causing the flow of seminal fluid into the prostatic urethra (emission). The internal urethral opening of the bladder neck becomes constricted so that there is no retrograde flow into the bladder. Rhythmic contraction of bulbospongiosus (supplied by the perineal nerve) compresses the penile urethra and expels the fluid. Orgasmic sensations run in the spinothalamic tract and are abolished by cord transection, but in transections above the lower thoracic segments ejaculation can still occur.