Prevertebral muscles of the neck
Some relatively weak flexor muscles extend in front of the vertebral column from skull to superior mediastinum. They are covered anteriorly by the strong prevertebral fascia (Fig. 6.8).
|
|
|
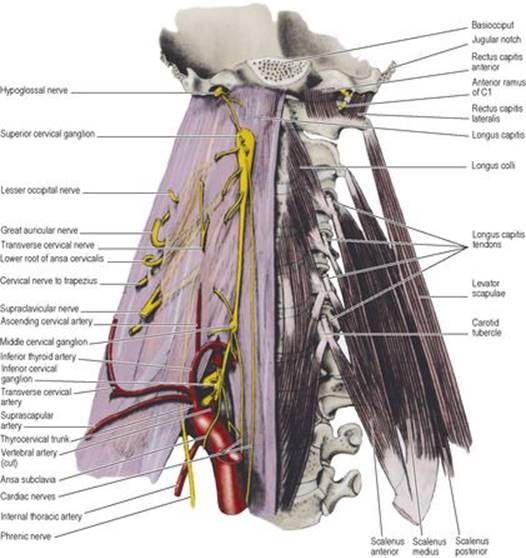
Figure 6.8 Prevertebral region of the neck. The right half of the prevertebral fascia is intact; on the left the prevertebral muscles are exposed. |
Rectus capitis anterior extends from just in front of the occipital condyle to the lateral mass of the atlas.
Rectus capitis lateralis lies edge to edge with the former muscle; it extends from the jugular process of the occipital bone to the transverse process of the atlas. The anterior ramus of C1, passing forwards lateral to the atlanto-occipital joint, supplies each muscle and then passes between them to sink into the overlying longus capitis muscle. It gives a branch to the hypoglossal nerve, which is distributed in the meningeal branch, the superior root of the ansa cervicalis and the branches to thyrohyoid and geniohyoid. These two small rectus muscles assist in flexion and lateral flexion of the head.
Longus capitis is attached to the basiocciput, in front of rectus capitis anterior and behind the wall of the nasopharynx (pharyngobasilar fascia, see p. 383), which it bulges forwards slightly. It is attached below by four tendons, in line with those of scalenus anterior, to the anterior tubercles of the transverse processes of the four ‘typical’ cervical vertebrae (C3–6). It is supplied by anterior rami of the upper four cervical nerves. It flexes the head.
Longus colli extends from the atlas into the superior mediastinum. It consists of upper, lower and central fibres, which together give the muscle a triangular shape, the elongated base of the triangle being close to the midline (Fig. 6.8). It is attached to the anterior tubercle of the altas, the front of the bodies of vertebrae C2–7 and T1–3, and to the anterior tubercles of the transverse processes of vertebrae C3–6.
Longus colli is supplied segmentally by the anterior rami of the spinal nerves. It is a flexor of the neck.
The prevertebral fascia is described on page 331.
Cervical sympathetic trunk
The cervical part of the sympathetic trunk (Fig. 6.8) ascends from the thorax across the neck of the first rib, medial to the highest intercostal vein. It runs up medial to the vertebral artery and lies in front of the prevertebral fascia, behind the carotid sheath and medial to the vagus nerve. It ends at the superior cervical ganglion.
The superior cervical ganglion, containing about 1 million cell bodies, is about 3cm long and lies in front of C2 and C3 vertebrae. The middle cervical ganglion is a small, inconstant ganglion lying medial to the carotid tubercle (C6 vertebra) and in front of the inferior thyroid artery. The inferior cervical ganglion lies behind the commencement of the vertebral artery. A small mass when separate, it is often fused with the first thoracic ganglion to form the cervicothoracic (stellate) ganglion, in front of the neck of the first rib. The middle ganglion is connected to the inferior (or stellate) ganglion by two or more strands, one of which loops down in front of and under the subclavian artery, the ansa subclavia (Fig. 6.8).
No white rami enter the ganglia from the cervical nerves: all the preganglionic fibres ascend from the thoracic part of the trunk. As elsewhere, the branches of the ganglia are somatic and visceral in their distribution.
Grey rami pass to all eight cervical nerves. The superior ganglion gives grey rami to the first four (i.e. to the cervical plexus), the middle ganglion to the next two (5 and 6) and the inferior ganglion to the last two (7 and 8) anterior rami (i.e. to the brachial plexus for distribution to the upper limb).
Each ganglion gives a cardiac branch. The branch from the upper left ganglion runs down to the superficial cardiac plexus, the others all pass to the deep plexus. All six cardiac branches pass down behind the common carotid and subclavian arteries to reach the superior mediastinum.
Vascular branches ‘hitch-hike’ their way along arteries. The superior ganglion gives branches to the internal carotid and external carotid arteries. The internal carotid nerve accompanies the internal carotid artery into the skull and forms the internal carotid plexus, from which fibres are distributed to all branches of the artery, the pterygopalatine ganglion and the eye, the latter including the motor supply of the dilator pupillae of the iris. The plexus on the external carotid artery accompanies all branches of the vessel and in addition supplies sympathetic fibres to the pharyngeal plexus and the submandibular and otic ganglia.
The middle cervical ganglion gives branches to the inferior thyroid artery.
The inferior cervical ganglion gives branches to the subclavian artery and a large branch to the vertebral artery, which forms the vertebral plexus.
Interruption of the cervical sympathetic pathway gives rise to Horner's syndrome, described on page 408.