Anesthesiologists face several preoperative challenges when patients with endocrine disorders need surgery. Patients may present with an endocrinopathy requiring surgery or more commonly have an endocrine abnormality, which complicates surgical and anesthetic management. Physiologic perturbations from the stress response of surgery may precipitate an endocrine crisis perioperatively.
Endocrine glands secrete hormones into the blood, which can act at distant sites (endocrine), adjacent to the site of origin (paracrine), at the site of origin (autocrine), and even within the site of origin (intracrine) to provoke a physiologic response. The endocrine system is evaluated by measuring hormone levels. In most cases, hormone output is regulated by a negative feedback system in which increased circulating plasma concentrations of the hormone decrease its subsequent release from the parent gland. The nervous system (via hypothalamic-releasing factors and peptides produced by the brain) and the immune system (via cortisol, cytokines, and interleukins) also modulate the endocrine system to regulate hormone levels. Defects in the pathway such as genetic receptor mutations or excessive circulating serum factors can cause endocrinologic dysfunction (hormone excess, hormone deficiency, and hormone resistance). Management of endocrinopathies includes hormone replacement and medical or surgical reduction of hormone levels produced by tumors.
Mechanism of Hormone Action
Hormones bind to membrane and nuclear receptors to trigger selective and diverse cellular responses. Membrane receptor binding (peptides and catecholamines) initiates signal transduction through enzymes such as adenylate cyclase, tyrosine kinase, and serine kinase. Receptor binding in the nucleus (steroids and vitamin D) regulates gene expression in the cytoplasm and nucleus to produce specific intracellular proteins and enzymes.
Hypothalamus and Pituitary Gland
The hypothalamus is located at the base of the brain and above the pituitary gland. Environmental factors such as light and temperature, adrenergic and dopaminergic receptors, pain signals, emotions, and olfactory sensations stimulate the hypothalamus to secrete hypothalamic-releasing and hypothalamic inhibitory hormones. The hypothalamus is a collecting and coordinating center for information and links the central nervous system and endocrine system to the environment.
Hormones designated as hypothalamic-releasing or hypothalamic inhibitory hormones originate in the hypothalamus and control secretions from the anterior pituitary (Table 37-1). The hormones travel via hypothalamic-hypophyseal portal vessels (undiluted by peripheral blood) to interact with cell membrane receptors in the anterior pituitary, which increase the intracellular concentrations of calcium ions and cyclic adenosine monophosphate (cAMP). Hypothalamic and pituitary secretion is pulsatile rather than tonic, and the pulses are superimposed on broader biologic rhythms such as the circadian release of adrenocorticotrophic hormone (ACTH), the sleep-entrained release of human growth hormone (HGH), and the monthly cycle of gonadotropins in females.

The pituitary gland lies in the sella turcica at the base of the brain and is connected to the hypothalamus by the pituitary stalk. Physiologically, the gland is outside the blood–brain barrier and is divided into the anterior pituitary (adenohypophysis) and posterior pituitary (neurohypophysis). The anterior pituitary synthesizes, stores, and secretes six tropic hormones. ACTH, prolactin, and HGH are polypeptides; thyroid-stimulating hormone (TSH), luteinizing hormone (LH), and follicle-stimulating hormone (FSH) are glycoproteins. The anterior pituitary also secretes β-lipotropin, which contains the amino acid sequences of several endorphins that bind to opioid receptors. The posterior pituitary stores and secretes two hormones—arginine vasopressin (AVP), formerly designated antidiuretic hormone (ADH) and oxytocin. Both are initially synthesized in the hypothalamus and subsequently transported (via axons) to the posterior pituitary (Table 37-2). During the perioperative period, secretion of pituitary hormones increases with activation of the sympathetic nervous system.1

The response to pituitary stalk destruction differs in the anterior and posterior pituitary gland. Stalk destruction causes axonal atrophy and subsequent loss of posterior pituitary function. After stalk destruction, the anterior pituitary can still respond to hypothalamic hormones in the peripheral blood via the inferior hypophyseal artery.
Anterior Pituitary
Anterior pituitary cells have been traditionally classified on the basis of their staining characteristics as agranular chromophobes or granular chromophils. Chromophils are subdivided into acidophils and basophils depending on the staining response to acidic or basic dyes. With more modern techniques, including electron microscopy and immunochemistry, it is possible to identify at least five types of cells, some of which secrete more than one tropic hormone (see Table 37-2).
Growth Hormone (Somatotropin)
Growth hormone (GH) is the most abundant anterior pituitary hormone. GH stimulates growth of all tissues in the body and evokes intense metabolic effects (Fig. 37-1).2 The most striking and specific effect is stimulation of linear bone growth that results from GH action on the epiphyseal cartilage plates of long bones. Excess secretion of GH before epiphyseal closure occurs causes gigantism. When excess GH secretion is excessive after epiphyseal closure and long bones can no longer increase in length but only in thickness, acromegaly results. The metabolic effects of GH include increased rates of protein synthesis (anabolic effect), increased mobilization of free fatty acids (ketogenic effect), antagonism of insulin action (diabetogenic effect) and sodium and water retention. Many of the activities of GH require the generation of a family of peptides known as somatomedins.

Releasing (growth hormone–releasing hormone) and inhibitory (somatostatin) hormones, physiologic events, and medications regulate GH secretion (Table 37-3). For example, perioperative anxiety and stress may evoke the release of GH.1 Plasma concentrations of GH characteristically increase during physiologic sleep. Drugs may influence the secretion of GH, presumably via effects on the hypothalamus. In this regard, large doses of corticosteroids suppress secretion of GH, which may be responsible for the inhibitory effects on growth observed in children receiving high doses of corticosteroids for prolonged periods of time. Conversely, dopaminergic agonists acutely increase the secretion of GH.

Prolactin
Prolactin has little metabolic activity but it prompts the growth and development of the breast in preparation for breast-feeding. Pregnancy stimulates the release of prolactin; dopamine inhibits its release (Table 37-4). Preoperative anxiety also increases plasma concentrations of prolactin.1 Prolactin secretion in response to suckling inhibits ovarian function, explaining the usual lack of ovulation and resulting infertility during breast-feeding.

Gonadotropins
LH and FSH are gonadotropins responsible for pubertal maturation and secretion of steroid sex hormones by the gonads of either sex. These hormones bind to cell membrane receptors in the ovaries or testes to stimulate the synthesis of cAMP.
Adrenocorticotrophic Hormone
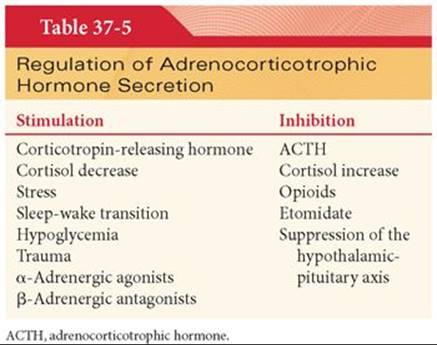
ACTH regulates secretions of the adrenal cortex, especially cortisol, and stimulates the formation of cholesterol in the adrenal cortex. Cholesterol is the initial building block for the synthesis of corticosteroids. Secretion of ACTH responds dramatically to stress under the control of corticotropin-releasing hormone from the hypothalamus, as well as a negative feedback mechanism from the circulating plasma concentration of cortisol (Table 37-5).3 Secretory rates of corticotropin-releasing hormone and ACTH are high in the morning and low in the evening. This diurnal variation results in high plasma cortisol concentrations in the morning (~20 µg/dL) and low levels (~5 µg/dL) around midnight. For this reason, plasma concentrations of cortisol are interpreted in terms of the time of day of the measurement. Surgical incision, reversal of anesthesia, and postoperative pain stimulate ACTH release.1,4,5
In the absence of ACTH, the adrenal cortex undergoes atrophy, but the zona glomerulosa, which secretes aldosterone, is least affected. Indeed, hypophysectomy has minimal effects on electrolyte balance because of the continued release of aldosterone from the adrenal cortex. Pigmentary changes that may accompany certain endocrine diseases most likely reflect changes in plasma concentrations of ACTH, revealing the melanocyte-stimulating effects of this hormone. For example, pallor is a hallmark of hypopituitarism. Conversely, hyperpigmentation in patients with adrenal insufficiency from primary adrenal gland disease reflects high concentrations of ACTH circulating in plasma as the anterior pituitary attempts to stimulate corticosteroid secretion.
Chronic administration of corticosteroids suppresses corticotropin-releasing hormone and leads to atrophy the hypothalamic-pituitary axis. Several months may be required for recovery of this axis after removal of the suppressive influence. In such patients, stressful events during the perioperative period might evoke life-threatening hypotension. For this reason, it is a common practice to administer supplemental exogenous corticosteroids (based on the magnitude of stress) to patients considered at risk for suppression of the hypothalamic-pituitary axis. There is little evidence, however, that supplemental corticosteroids in excess of normal daily physiologic secretion are necessary or beneficial intra- or postoperatively.6 See Chapter 40 for dosing of corticosteroids during the perioperative period.
Thyroid-Stimulating Hormone
TSH accelerates all the steps in the formation of thyroid hormones, including initial uptake of iodide into the thyroid gland. TSH causes proteolysis of thyroglobulin in the follicles of thyroid cells to release thyroid hormones into the circulation. Secretion of TSH from the anterior pituitary is under the control of thyrotropin-releasing hormone from the hypothalamus as well as a negative feedback mechanism, depending on the concentrations of thyroid hormones circulating in plasma. Sympathetic nervous system stimulation and corticosteroids also suppress the secretion of TSH and thus diminish activity of the thyroid gland. Thyrotropin-releasing hormone is widely distributed in the central nervous system and is a potent analeptic. TRH stimulates respiratory rate, induces tremor, and reduces sleep time.
A long-acting thyroid stimulator is an immunoglobulin A antibody that binds to receptor sites on thyroid cells. Binding can mimic the effects of TSH and account for hyperthyroidism, and patients with hyperthyroidism often have detectable circulating concentrations of these proteins. Hypothyroidism with increased plasma concentrations of TSH indicates a primary defect at the thyroid gland (primary hypothyroidism) and an attempt by the anterior pituitary to stimulate hormonal output by releasing TSH. A defect at the hypothalamus or anterior pituitary is indicated by low concentrations of both TSH and thyroid hormones circulating in plasma (secondary hypothyroidism).
Posterior Pituitary
The cells in the posterior pituitary act as supports for the terminal nerve endings of fibers from the supraoptic and paraventricular nuclei of the hypothalamus. AVP is synthesized in the supraoptic nuclei and oxytocin in the paraventricular nuclei. These hormones are transported in secretory granules along axons from corresponding nuclei in the hypothalamus to the posterior pituitary for subsequent release in response to appropriate stimuli.
Arginine Vasopressin
The physiologic functions of AVP include vasoconstriction, water retention, and corticotropin secretion. Decreases in blood volume, increased plasma osmolality, and decreased arterial pressure stimulate AVP release7 (Table 37-6). With hydration and establishment of an adequate blood volume before induction of anesthesia, urine output is maintained by blunting the release of AVP associated with painful stimulation or fluid deprivation before surgery. Concentrations of AVP in the plasma in response to acute decreases in the volume of extracellular fluid may exert direct vasopressor effects on arterioles and thus contribute to maintenance of systemic blood pressure. Administration of morphine, or other opioids, in the absence of painful stimulation does not evoke the release of AVP. Ethanol inhibits the secretion of AVP. Decreases in urine output and fluid retention previously attributed to release of AVP during positive pressure ventilation of the lungs are more likely the result of changes in cardiac filling pressures that impair the release of atrial natriuretic hormone.

There are three subtypes of AVP receptors, V1, V2, and V3. Stimulation of V1 receptors (found on vascular smooth muscle) causes vasoconstriction. AVP is used as a vasopressor during intraoperative hypotension, sepsis, and cardiopulmonary resuscitation. Activation of the V2 receptors, which are located on collecting duct cells in the kidney, increases reabsorption of water. AVP is transported in the blood to the kidneys, where it attaches to receptors on the capillary side of epithelial cells lining the distal convoluted renal tubules and collecting ducts of the renal medulla. The receptor-hormone interaction results in the formation of large amounts of cAMP, which causes insertion of aquaporin-2 into the collecting duct walls for exit of water to minimize osmolality. Hypokalemia, hypercalcemia, cortisol, and lithium also interfere with renal responsiveness to AVP. AVP binds to V3 receptors in the adenohypophysis to release corticotropin, which suggests that this hormone affects the stress response.7
Destruction of neurons in or near the supraoptic and paraventricular nuclei of the hypothalamus from pituitary surgery, trauma, cerebral ischemia, or malignancy may decrease vasopressin release to cause central diabetes insipidus.7 If the posterior pituitary alone is damaged, however, the transected fibers of the pituitary stalk can still continue to secrete AVP. Diabetes insipidus from lack of vasopressin release during pituitary surgery is usually transient. (See Chapter 40 for hormonal treatment of central diabetes insipidus.)
Unnecessary or excessive secretion of AVP with subsequent retention of water and dilutional hyponatremia may result from head injuries, intracranial tumors, meningitis, or pulmonary infections. Aberrant production of AVP is observed most commonly in patients with cancer, especially oat cell carcinoma, in which the tumor itself produces AVP. In cancer patients, the antibiotic demeclocycline promotes diuresis by antagonizing the effects of AVP on renal tubules.
Oxytocin
Breast suckling and cervical and vaginal dilation stimulate oxytocin secretion. Oxytocin ejects milk from the lactating mammary gland via contraction of the myoepithelial cells that surround the alveoli of the mammary glands. Oxytocin binds to G proteins on the surface of uterine myocytes to trigger the release of calcium from the sarcoplasmic reticulum, exerting a contracting effect on the pregnant uterus.8Oxytocin also augments the action potential of the uterine smooth muscle.9 Large amounts of oxytocin cause sustained uterine contraction as necessary for postpartum hemostasis. Oxytocin has only 0.5% to 1.0% the antidiuretic activity of AVP and can be released abruptly and independently of AVP.
Thyroid Gland
The thyroid gland maintains optimal metabolism for normal tissue function.10 The principal hormonal secretions of the thyroid gland are thyroxine (T4) and triiodothyronine (T3) (Fig. 37-2). T4, a prohormone synthesized from tyrosine, represents 80% of the body’s thyroid hormone production. T3, five times more active than T4, is produced directly from tyrosine metabolism or from conversion of T4 in peripheral tissues. Two distinct deiodases (located in the liver, kidneys, and central nervous system) metabolize T4 and T3 to inactive compounds. The half-lives of endogenously or exogenously administered T3 and T4are 1.5 and 7 days, respectively. T3 and T4 are both highly protein bound to albumin, thyroid-binding prealbumin, and thyroid-binding globulin with only 0.2% of T3 and 0.3% of T4 freely circulating unbound and pharmacologically active.10 It is of interest that iodine present in thyroid hormones is not necessary for biologic activity (see Fig. 37-2). In addition to thyroid hormones, the thyroid gland secretes calcitonin, which is important for calcium ion use.

The thyroid hormones increase oxygen consumption in nearly all tissues, except for the brain. Failure of thyroid hormones to greatly alter the oxygen consumption of the brain is consistent with the minimal changes in anesthetic requirements (MAC) that accompany hyperthyroidism or hypothyroidism.11 Cardiovascular changes are often the earliest clinical manifestations of abnormal thyroid hormone levels. Absence of thyroid gland hormones decreases minute oxygen consumption to approximately 40% less than normal; excesses of thyroid hormones can expand oxygen consumption as much as 100% more than normal. Thyroid hormones stimulate carbohydrate metabolism and facilitate the mobilization of free fatty acids. Despite the latter effect, plasma concentrations of cholesterol usually decrease, reflecting stimulation of low-density lipoprotein receptor synthesis by thyroid hormones.
Anatomically, the thyroid gland consists of two lobes connected by a bridge of tissues known as the thyroid isthmus (Fig. 37-3). The gland is highly vascularized and receives innervation from the autonomic nervous system. Structurally, the gland consists of multiple follicles (acini) that are filled with colloid, which consists principally of thyroglobulin. Thyroid hormones are stored in combination with thyroglobulin. Stimulation of proteases by TSH results in cleavage of hormones from thyroglobulin and their release into the systemic circulation.

Mechanism of Action
When thyroid hormones enter cells, T3 binds to nuclear receptors. T4 also binds to these receptors but not as avidly. Indeed, T4 serves principally as a prohormone for T3, so that the biologic effects of T4 are largely a result of its intracellular conversion to T3.
Thyroid hormones exert most, if not all, of their effects through control of protein synthesis. Thyroid hormones activate the DNA transcription process in the cell nucleus to form new cell proteins and enzymes. Sympathomimetic effects that accompany thyroid hormone stimulation most likely reflect a greater number and sensitivity of β-adrenergic receptors to release of T4 and T3. It has been proposed that thyroid hormones modulate conversion of α-adrenergic to β-adrenergic receptors. Cardiac cholinergic receptor numbers are decreased by thyroid hormones, which is consistent with an increase in heart rate that is out of proportion to the increase in cardiac output.
When thyroid hormones accelerate metabolism, tissues vasodilate and blood flow delivers necessary oxygen and carries away metabolites and heat. As a result, cardiac output often increases but systemic blood pressure is unchanged because peripheral vasodilation offsets the impact of more blood flow. Excess protein catabolism associated with greater secretion of thyroid hormones is the mechanism behind skeletal muscle weakness characteristic of hyperthyroidism. The fine muscle tremor that accompanies hyperthyroidism stems from the sensitivity of neuronal synapses in the area of the spinal cord that controls skeletal muscle tone. Diarrhea reflects additional motility in the gastrointestinal tract with excessive activity of the thyroid gland.
Calcitonin
Calcitonin, a polypeptide hormone secreted by the thyroid gland, decreases the concentration of calcium ions in plasma by weakening the activity of osteoclasts and strengthening the activity of osteoblasts. Calcitonin works in the early moments after ingestion of high-calcium meals. A total thyroidectomy and subsequent absence of calcitonin, however, does not measurably influence the plasma concentration of calcium, because of the predominance of parathyroid hormone.
Parathyroid Glands
The four parathyroid glands secrete parathyroid hormone (PTH), an amino and acid polypeptide that regulates plasma concentration of calcium ions. Secretion of PTH is inversely related to plasma ionized calcium concentration. Small declines in the plasma concentration of calcium ions stimulate the release of PTH. PTH promotes mobilization of bone calcium (osteoclastic activity); enhances conversion of vitamin D to its active form, 1,25-dihydroxycholecalciferol, to increase gastrointestinal absorption of calcium; increases renal tubular absorption of calcium; and inhibits renal reabsorption of phosphate to increase calcium and to decrease phosphate concentrations in plasma.
Parathyroid hormone exerts its effect on target cells in bones, renal tubules, and the gastrointestinal tract by stimulating the formation of cAMP. Because a portion of cAMP synthesized in the kidneys escapes into the urine, its assay serves as a measure of parathyroid gland activity.
Adrenal Cortex
The adrenal cortex secretes three major classes of corticosteroids: mineralocorticoids, glucocorticoids, and androgens. The precursor of all corticosteroids is cholesterol. More than 30 different corticosteroids have been isolated from the adrenal cortex, but only two are important: aldosterone, a mineralocorticoid, and cortisol, the principal glucocorticoid (Table 37-7). The corticosteroids are not stored in the adrenal cortex; the rate of synthesis determines the subsequent plasma concentration. Anatomically, the adrenal cortex is divided into three zones designated the (a) zona glomerulosa that secretes mineralocorticoids, (b) zona fasciculata that secretes glucocorticoids, and (c) zona reticularis that secretes androgens and estrogens.

Mineralocorticoids: Aldosterone
Aldosterone accounts for approximately 95% of the mineralocorticoid activity of the corticosteroids. Desoxycorticosterone, the other naturally occurring mineralocorticoid, has only 3% of the sodium ion–retaining potency of aldosterone. Cortisol induces retention of sodium ions and secretion of potassium ions but much less effectively than aldosterone.
Physiologic Effects
Aldosterone sustains extracellular fluid volume by conserving sodium and by maintaining a normal plasma concentration of potassium. Sodium ions are absorbed at the same time potassium ions are secreted by the lining of epithelial cells of the distal renal tubules and collecting ducts. As a result, sodium is conserved in the extracellular fluid, and potassium is excreted in the urine. Water follows sodium such that extracellular fluid volume changes in proportion to the rate of aldosterone secretion. If aldosterone secretion is excessive, extracellular fluid volume, cardiac output, and systemic blood pressure increase. If plasma concentration of potassium decreases approximately 50% after excess secretion of aldosterone, skeletal muscle weakens or paralysis occurs because nerve and muscle membranes are hyperpolarized and the transmission of action potentials is prevented.
Aldosterone affects sweat glands and salivary glands. It increases the reabsorption of sodium and secretion of potassium by sweat glands. This effect conserves sodium in hot environments or during excess salivation. Aldosterone also enhances sodium ion reabsorption by the gastrointestinal tract.
Mechanism of Action
Aldosterone diffuses to the interior of renal tubular epithelial cells, where it induces DNA to form messenger RNA (mRNA) necessary for the transport of sodium and potassium ions. It is speculated that this mRNA is a specific adenosine triphosphatase (ATPase) that catalyzes energy from cytoplasmic adenosine triphosphate (ATP) to the sodium ion transport mechanism of cell membranes. It takes as long as 30 minutes before the new mRNA appears and approximately 45 minutes before the rate of sodium ion transport begins to increase.
Regulation of Secretion
The most important stimulus for aldosterone secretion is an accumulation of potassium in the plasma. A powerful negative feedback system maintains the plasma concentration of potassium ions in a normal range. The renin-angiotensin system also affects aldosterone secretion (see Chapter 16). The elimination half time of aldosterone is approximately 20 minutes, and nearly 90% is cleared by the liver in a single passage. Mineralocorticoid secretion is not under the primary control of ACTH. For this reason, hypoaldosteronism does not accompany loss of ACTH secretion from the anterior pituitary.
Glucocorticoids: Cortisol
At least 95% of the glucocorticoid activity results from the secretion of cortisol. A small amount of glucocorticoid activity is provided by corticosterone and an even smaller amount by cortisone. Cortisol is one of the few hormones essential for life.
Physiologic Effects
Cortisol (a) increases gluconeogenesis, (b) breaks down protein, (c) mobilizes fatty acid, and (d) has antiinflammatory effects. Cortisol may improve cardiac function by increasing the number or responsiveness of β-adrenergic receptors. In addition to sustaining cardiac function and maintaining systemic blood pressure, cortisol promotes the normal responsiveness of arterioles to the constrictive action of catecholamines. Cortisol inhibits bone formation.
Developmental Changes
Plasma concentrations of cortisol increase progressively during the last trimester of pregnancy to reach a peak plasma concentration at term, so that systems critical for survival are mature for the onset of extrauterine life. These systems include production of pulmonary surfactant, maturation of various enzyme systems in the liver, and the expression of phenylethanolamine N-methyltransferase, the enzyme necessary for the synthesis of epinephrine from norepinephrine.
Gluconeogenesis
Cortisol stimulates gluconeogenesis by the liver as much as 10-fold. Amino acids are mobilized from extrahepatic sites and transferred to the liver for conversion to glucose. An accelerated rate of gluconeogenesis with a moderate decline in glucose use caused by cortisol results in larger concentrations of blood glucose known as adrenal diabetes. Adrenal diabetes is responsive to the administration of insulin.
Protein Catabolism
Cortisol breaks down protein stores in nearly all cells except hepatocytes, to mobilize amino acids for gluconeogenesis. When excesses of cortisol are sustained, skeletal muscle weakness may become pronounced.
Fatty Acid Mobilization
Cortisol promotes mobilization of fatty acids from adipose tissue and enhances oxidation of fatty acids in cells. Despite these effects, with excess amounts of cortisol, fat is deposited in the neck and chest regions, giving rise to a “buffalo-like” torso. Fat deposits at these sites at a rate that exceeds its mobilization.
Antiinflammatory Effects
In large amounts, cortisol has antiinflammatory effects when it stabilizes lysosomal membranes and stops migration of leukocytes into the inflamed area. When lysosomal membranes are stable, the release of inflammation-causing lysosomes is attenuated. Cortisol lessens capillary permeability to prevent loss of plasma into tissues. Even after inflammation has been well established, the administration of cortisol weakens its manifestations. This effect of cortisol is useful for disease states with inflammation such as rheumatoid arthritis and acute glomerulonephritis.
Cortisol minimizes the number of eosinophils and leukocytes in the blood within a few minutes after its administration. Atrophy of lymphoid tissue throughout the body reduces the production of antibodies. As a result, the level of immunity against bacterial or viral infection is diminished, and infection can fulminate. Conversely, suppressing immunity is useful to prevent immunologic rejection of transplanted tissues.
In the treatment of allergic reactions, cortisol prevents the life-threatening inflammatory responses of allergic reactions such as laryngeal edema. Cortisol may also interfere with activation of the complement pathway and formation of chemical mediators derived from arachidonic acid, such as leukotrienes. Cortisol does not, however, alter the antigen–antibody interaction or histamine release associated with allergic reactions.
Mechanism of Action
Steroids are intracrine hormones that interact with intracellular (often nuclear) receptors. Cortisol stimulates DNA-dependent synthesis of mRNA in the nuclei of responsive cells, leading to the synthesis of necessary enzymes.
Regulation of Secretion
The most important stimulus for the secretion of cortisol (13 to 20 mg daily) is the release of ACTH from the anterior pituitary (see Table 37-5). The secretion of ACTH in the anterior pituitary is determined by two hypothalamic neurohormones, diurnal release of corticotropin-releasing hormone and arginine vasopressin (AVP) that act synergistically. Circulating cortisol has a direct negative feedback effect on the hypothalamus and anterior pituitary to decrease the discharge of corticotropin-releasing hormone and ACTH from these respective sites. Immediately following migration from the adrenal gland, cortisol is bound to the α-globulin, transcortin (cortisol-binding globulin). Plasma concentrations of cortisol are higher in females than males with additional concentrations accompanying the menstrual cycle just before ovulation. If stress from the perioperative period overrides the normal negative feedback control mechanisms, plasma concentrations of cortisol increase. The beneficial effect of a greater plasma concentration of cortisol and other hormones in response to stressful stimuli may be the acute mobilization of cellular proteins and fat stores for energy and synthesis of other compounds, including glucose.
Cortisol is secreted and released by the adrenal cortex at a basal rate of approximately 20 to 30 mg daily. In response to maximal stressful stimuli (sepsis, burns), the output of cortisol is increased to approximately 150 mg daily.12This amount should be a sufficient replacement for patients who lack adrenal function and who are acutely ill or undergoing major surgery. The peak plasma cortisol concentration of 8 to 25 µg/dL occurs in the morning shortly after awakening. Stress-induced changes in the plasma concentration of cortisol are superimposed on the circadian tone and vary in onset, magnitude, and duration, depending on the intensity of the stress. In the systemic circulation, 80% to 90% of cortisol is bound to a specific globulin known as transcortin. It is the relatively small amount of unbound cortisol that exerts a biologic effect. The elimination half-time of cortisol is approximately 70 minutes. Cortisol is degraded mainly in the liver with the formation of inactive 17-hydroxycorticosteroids that appear in the urine. Cortisol is also filtered at the glomerulus and may be excreted unchanged in urine.
Effect of Anesthesia and Surgery
Perioperative stress stimulates hormonal secretion of ACTH and cortisol.1 This response may be diminished by less invasive surgeries such as laparoscopy and blunted by choice of anesthetic technique. During the perioperative period, ACTH stimulation, tissue damage, and proinflammatory mediators can release cortisol. As with other types of stress, the episodic release of cortisol remains intact but the amplitude of episodic releases is greater. Large concentrations of cortisol in plasma in the perioperative period may be prompted by baroreceptor and spinal reflexes that signal tissue injury to the hypothalamus.13
Plasma cortisol concentrations typically return to normal levels within 24 hours postoperatively but may remain elevated for as long as 72 hours, depending on the severity of the surgical trauma. In addition, disturbances in the circadian rhythm may be associated with postoperative fatigue and debility. Return of plasma cortisol concentrations to normal following surgery is characterized by increased plasma concentrations of ACTH and cortisol (consistent with sustained, stress-induced stimulation of the hypothalamus) followed by a second phase in which plasma ACTH concentrations are low and larger cortisol concentrations in plasma are independent of the hypothalamic-pituitary system. Cytokines released from traumatized tissue may stimulate synthesis of cortisol directly despite low plasma concentrations of ACTH. Alternatively, prior increases in ACTH concentrations in plasma may stimulate production of ACTH receptors in the adrenal glands resulting in greater cortisol production.
Plasma cortisol concentrations in the perioperative period are designed to provide protection during and after surgery. In adrenalectomized animals who received subphysiologic doses of cortisol, hemodynamic instability and mortality followed surgery. Animals treated with physiologic or supraphysiologic doses of cortisol were indistinguishable from control animals.14 A key feature of hypothalamic-pituitary-adrenal (HPA) physiology is negative feedback that suppresses release of ACTH by the pituitary by high levels of endogenous or exogenous glucocorticoids. Suppression of the hypothalamic-pituitary axis by regular administration of corticosteroids prevents the release of cortisol in response to stressful stimuli.
The acute phase response to surgery is also mediated by the release of proinflammatory cytokines such as interleukin-1, tumor necrosis factor-α, and interleukin-6 from damaged tissue and activation of the sympathetic nervous system. Cytokines may stimulate ACTH and cortisol production and are subject to a negative feedback system. Cytokine levels peak 24 hours after surgery and can remain elevated for several days. Hepatic production of acute phase proteins (C-reactive protein, fibrinogen, and α2-macroglobulin) is generated in response to trauma and surgery.1
In addition to surgical trauma, the choice of anesthetic drugs and techniques may influence the HPA response. Large doses of opioids may attenuate the cortisol response to surgical stimulation.15,16 Volatile anesthetics do not suppress the stress-induced endocrine response as much. Etomidate, unique among drugs administered to induce anesthesia, inhibits cortisol synthesis even in the absence of surgical stimulation (see Chapter 5). Although studies of regional anesthetics show a potential to decrease perioperative complications, a reduction in surgical stress-induced release of cortisol has not been proven in abdominal or thoracic surgeries.
Reproductive Glands
In both sexes, the reproductive glands (testes and ovaries) produce germ cells and steroid sex hormones.
Testes
The testes secrete male sex hormones, which are collectively designated androgens. All androgens are steroid compounds that can be synthesized from cholesterol. Testosterone, the most potent and abundant of the androgens, develops and maintains male sex characteristics. Skeletal muscle growth is an anabolic effect of testosterone in the male. Testosterone is produced in the testes only with stimulation from LH, and FSH is necessary for spermatogenesis. Puberty is characterized by the production of testosterone rapidly in response to hypothalamic-releasing hormones that evoke the release of LH and FSH. Hypertrophy of the laryngeal mucosa accompanies secretion of testosterone, leading to changes in voice at puberty. Testosterone increases secretion of sebaceous glands, leading to acne. Beard growth is the last manifestation of puberty. Testosterone production continues throughout life, although the amount produced lessens gradually after 40 years. At age 80 years, it is approximately one-fifth the peak value.
At most sites of action, testosterone is not the active form of the hormone. It is converted in target tissues to the more active dihydrotestosterone by a reductase enzyme. Dihydrotestosterone binds to a cytoplasmic protein receptor for synthesis of specific mRNA protein. In the absence of sufficient reductase enzyme, external genitalia fail to develop (pseudohermaphroditism) despite secretion of adequate amounts of testosterone. Not all target tissues, however, require the conversion of testosterone to dihydrotestosterone for activity. For example, effects of testosterone on skeletal muscles and bone marrow are mediated by the hormone or a metabolite other than dihydrotestosterone.
The adrenal cortex also secretes androgens, but the effects of these hormones are usually inconsequential unless a hormone-secreting tumor develops. For example, in males, approximately 10% of androgens are produced in the adrenal cortex, an insufficient amount to maintain spermatogenesis or secondary sexual features in an adult male. In abnormal conditions, such as the adrenogenital syndrome, the adrenal cortex can secrete large quantities of steroids and androgenic precursors.
Ovaries
The two ovarian hormones, estrogen and progesterone, are secreted in response to LH and FSH, which are released from the anterior pituitary in response to hypothalamic-releasing hormones. In postpubertal females, an orderly secretion of LH and FSH is necessary for menstruation, pregnancy, and lactation. The Stein-Leventhal syndrome is characterized by virilization when ovarian secretion of androgens is excessive.
Estrogens
Estrogens give the female sexual characteristics. In the nonpregnant female, most of the estrogen comes from the ovaries; small amounts are also secreted by the adrenal cortex. The three most important estrogens are β-estradiol, estrone, and estriol. These estrogens are conjugated in the liver to inactive metabolites that appear in urine.
Progesterone
Progesterone prepares the uterus for pregnancy and the breasts for lactation. Almost all of the progesterone in the nonpregnant female is secreted by the corpus luteum during the lateral phase of the menstrual cycle. The adrenal cortex forms small amounts of progesterone. Progesterone is metabolized to pregnanediol, which appears in the urine and is a valuable index of the secretion and metabolism of this hormone.
Menstruation
The overall duration of a normal menstrual cycle is 21 to 35 days and consists of three phases designated as follicular, ovulatory, and luteal. The follicular phase begins with the onset of menstrual bleeding after the plasma concentration of progesterone decreases. After a variable length of time, the follicular phase is followed by the ovulatory phase lasting 1 to 3 days and culminating in ovulation. The increase in body temperature (~0.5°C) that accompanies ovulation most likely reflects a thermogenic effect of progesterone. The luteal phase follows ovulation and is characterized by the development of a corpus luteum that secretes progesterone and estrogen. The corpus luteum degenerates after a fairly constant period of 13 to 14 days and the menstrual cycle repeats.
Pregnancy
During pregnancy, the placenta forms large amounts of estrogens, progesterone, chorionic gonadotropin, and chorionic somatomammotropin. Chorionic gonadotropin prevents the usual involution of the corpus luteum or the onset of menstrual bleeding. The first key hormone of pregnancy, chorionic gonadotropin, which can be detected in the maternal plasma within 9 days after conception, is the basis for pregnancy tests. After approximately 12 weeks, the placenta secretes sufficient amounts of progesterone and estrogens to maintain pregnancy and the corpus luteum involutes. Chorionic somatomammotropin attenuates insulin activity, making more glucose available to the fetus.
Circulating concentrations of estrogen enlarge the breasts and uterus; progesterone is necessary to develop decidual cells in the uterine endometrium and to suppress uterine contractions that could result in spontaneous abortion. Greater concentrations of progesterone in plasma and associated sedative effects during pregnancy may explain why requirements for volatile anesthetics lessen in gravid animals. In animals, anesthetic requirements return to nonpregnant values within 5 days postpartum, whereas the plasma concentration of progesterone remains increased, suggesting that the decrease in MAC cannot be attributed entirely to progesterone.17 Progesterone concentrations are the stimulus for increased alveolar ventilation that accompanies pregnancy. Near term, the ovaries secrete the hormone relaxin, which relaxes pelvic ligaments so the sacroiliac joints become limber and the symphysis pubis becomes elastic.
The parturient with asthma may experience unpredictable changes in airway reactivity. Exacerbation of asthma from bronchoconstriction is evoked by prostaglandins of the F series, which are present in all trimesters of pregnancy but especially during labor. Conversely, prostaglandins of the E series are bronchodilators and predominate during the third trimester. That corticosteroids alter airway responsiveness is questionable, because the plasma concentrations of cortisol associated with pregnancy are offset by the carrier protein transcortin, with the net effect being an unchanged level of available cortisol.
Menopause
Between the ages of 45 and 55 years, a woman’s ovaries gradually become unresponsive to the stimulatory effects of LH and FSH, and the sexual cycles disappear. Because the negative feedback control of estrogen and progesterone on the anterior pituitary is decreased, output of LH and FSH accumulates in circulating plasma concentrations. Sensations of warmth spreading from the trunk to the face (hot flashes) coincide with surges of LH secretion and are prevented by exogenous administration of estrogens.
Pancreas
The exocrine pancreas secretes digestive substances into the duodenum. The islets of Langerhans are organized endocrine cells that secrete four hormones (insulin, glucagon, somatostatin, and pancreatic polypeptide) into the systemic circulation. The pancreas contains 1 to 2 million islets, which, based on staining characteristics and morphology, are classified as α, β, δ, and pancreatic polypeptide cells.18 β cells account for about 60% of the islet cells and are the site of insulin production. The α cells account for 25% of islet cells and produce glucagon. Each islet receives a generous blood supply, which unlike any other endocrine organ, drains into the portal vein.
Insulin
Insulin is a 51-amino acid peptide hormone synthesized in the β cells of the islets of Langerhans as a single polypeptide proinsulin, which is the precursor molecule to insulin (Fig. 37-4).19,20 The peptide that connects the amino terminus of the A chain to the carboxyl terminus of the B chain is designated the connecting (C) peptide. Proinsulin is converted to insulin and C-peptide, and these two molecules are stored together in secretory granules. When pancreatic β cells are stimulated, equimolar amounts of insulin C-peptide are released. Thus, plasma concentrations of insulin C-peptide reflect functional activity of pancreatic β cells. Insulin is an anabolic hormone promoting the storage of glucose, fatty acids, and amino acids (Fig. 37-5).21 The amount of insulin secreted daily is equivalent to approximately 40 units. In the systemic circulation, insulin has an elimination half-time of approximately 5 minutes, with greater than 80% degraded in the liver and kidneys.


Insulin binds to a transmembrane, glycoprotein receptor with two distinct insulin-binding domains (an extracellular domain of α subunits and an intracellular domain of β subunits) to regulate metabolic function. When insulin binds to the extracellular domain, a conformational change of the α subunits facilitates ATP binding to the β subunits. As a result, tyrosine molecules in the intracelluar portions of the transmembrane receptors are autophosphorylated. The phosphorylated receptor phosphorylates other protein substrates such as insulin receptor substrates (IRS) that mediates enzyme activation (mitogen-activated protein), inactivation, and metabolic signaling. (Fig. 37-6).2 The insulin cascade stimulates translocation of glucose (GLUT-4) transporters from the cytosol to plasma membranes to (a) facilitate glucose diffusion into cells; (b) shift intracellular glucose metabolism toward glycogen storage via glycogen synthetase activation; (c) stimulate cellular uptake of amino acids, phosphate, potassium, and magnesium; (d) stimulate protein synthesis and inhibit proteolysis; and (e) regulate gene expression via insulin regulatory elements in target DNA molecules. Activation of sodium-potassium ATPase in cell membranes by insulin moves potassium ions into cells and decreases concentration of potassium in plasma.

Regulation of Secretion
The principal control of insulin secretion is via a negative feedback effect of the blood glucose concentration in the pancreas (Table 37-8). Virtually no insulin is secreted by the pancreas when the blood glucose concentrations are less than 50 mg/dL, and maximum stimulation for release of insulin is at concentrations greater than 300 mg/dL. Thus, blood glucose concentrations are maintained within a narrow range. The pancreas is richly innervated by the autonomic nervous system, so that insulin is released in response to β-adrenergic stimulation or to acetylcholine. Conversely, α-adrenergic stimulation or β-adrenergic blockade inhibits insulin release. Oral glucose is more effective than glucose administered intravenously in evoking the release of insulin, suggesting the presence of an anticipatory signal from the gastrointestinal tract to the pancreas. Glycosuria is more likely after intravenous rather than oral glucose administration. Glucagon, HGH, and corticosteroids potentiate glucose-induced stimulation of insulin secretion. Prolonged secretion of these hormones or their exogenous administration can exhaust pancreatic β cells and lead to diabetes mellitus. Indeed, diabetes mellitus is found in patients who develop acromegaly or in individuals with a diabetic tendency who are treated with corticosteroids.

Physiologic Effects
Insulin receptor expression is highest in tissues, which regulate glucose, lipid, and protein metabolism (adipose, skeletal muscle, and liver) via insulin. Insulin promotes the use of carbohydrates for energy while depressing the use of fats and amino acids. For example, insulin facilitates storage of fat in adipose cells by inhibiting lipase enzyme, which normally hydrolyzes triglycerides in fat cells. In the liver, insulin inhibits enzymes necessary for gluconeogenesis, thus conserving amino acid stores.
Insulin facilitates glucose uptake and storage in the liver through effects on specific enzymes. When insulin induces the activity of glucokinase, uptake of glucose into liver cells is enhanced. Glucokinase is the enzyme that causes initial phosphorylation of glucose after it diffuses into hepatocytes. Once phosphorylated, glucose is trapped and unable to diffuse back through cell membranes. Storage is further enhanced by insulin-induced inhibition of phosphorylase enzyme, which normally causes liver glycogen to split into glucose. The net effects of these actions of insulin on enzymes is to increase hepatic stores of glycogen up to a maximum of approximately 100 g. Ordinarily, approximately 60% of the glucose in a meal is stored in the liver as glycogen.
Resting skeletal muscles are almost impermeable to glucose except in the presence of insulin. Glucose that enters resting skeletal muscles under the influence of insulin is stored as glycogen for subsequent use as energy. The amount of glycogen that can be stored in skeletal muscles, however, is much less than the amount that can be stored in the liver. Furthermore, glycogen in skeletal muscles, unlike that stored in the liver, cannot be reconverted to glucose and released into the systemic circulation because skeletal muscles lack glucose phosphatase enzyme, which is necessary for splitting glycogen. Exercise increases the permeability of skeletal muscle membranes to glucose, perhaps because insulin is released from within the skeletal muscle itself or its vasculature.
Brain cells are unique in that the permeability of their membranes to glucose does not depend on the presence of insulin. This characteristic is crucial because brain cells use only glucose for energy, thus the importance of maintaining blood glucose concentrations above a critical level of approximately 50 mg/dL. Indeed, lack of insulin causes the use mainly of fat for energy to the exclusion of glucose, except by brain cells.
Deficiencies in insulin signaling are associated with insulin resistance. When an impaired intracellular signal decreases recruitment of proteins that transport glucose to the plasma membrane for glucose uptake, an individual is said to have insulin resistance. Compensatory hyperinsulinemia overcomes peripheral tissue resistance to insulin. A feedback loop exists between insulin responsiveness in target tissues and insulin secretion by pancreatic β cells.
Glucagon
Glucagon is a catabolic hormone acting to mobilize glucose, fatty acids, and amino acids into the systemic circulation (Fig. 37-7).21 These responses are the reciprocal of the insulin effects, emphasizing that these two hormones are also reciprocally secreted (Table 37-9). Indeed, the principal stimulus for secretion of glucagon is hypoglycemia. Glucagon abruptly increases the blood glucose concentration by stimulating glycogenolysis in the liver. Glucagon activates adenylate cyclase for the subsequent formation of cAMP. The metabolic effects of glucagon at the liver mimic those produced by epinephrine. Indeed, the study of the mechanism by which glucagon and epinephrine act as hyperglycemics led to the discovery of cAMP.22 Glucagon also causes hyperglycemia by stimulating gluconeogenesis in hepatocytes. Enhanced myocardial contractility and more secretion of bile are effects when exogenous administration increases plasma concentrations of glucagon far above normal levels Amino acids help the release of glucagon and thus prevent hypoglycemia from ingestion of a pure protein meal, which stimulates insulin secretion. Glucagon undergoes enzymatic degradation to inactive metabolites in the liver and kidneys and at receptor sites in cell membranes. The elimination half-time of glucagon is brief—only 3 to 6 minutes.


Somatostatin
Somatostatin regulates islet cell secretion, inhibits both insulin and glucagon release, and inhibits several gastrointestinal processes including gallbladder contraction, gastric motility, and splanchnic blood flow.23 This peptide is the same as growth hormone–releasing inhibitory hormone that is secreted by the hypothalamus.
Pancreatic Polypeptide
Pancreatic polypeptide inhibits pancreatic exocrine secretion, gallbladder contraction, vagally stimulated gastric acid secretion, and gut motility.24–26
References
1. Desborough JP. The stress response to trauma and surgery. Br J Anaesth. 2000;85:109–117.
2. Ganong WF. Review of Medical Physiology. 21st ed. New York, NY: Lange Medical Books/McGraw Hill; 2003.
3. Taylor AL, Fishman LM. Corticotropin-releasing hormone. N Engl J Med. 1988;319:213–221.
4. Udelsman R, Norton JA, Jelenich SE, et al. Responses of the hypothalamic-pituitary-adrenal and angiotensin axes and the sympathetic system during controlled surgical and anesthetic stress. J Clin Endocrinol Metab. 1987;64:986–994.
5. Raff H, Norton JA, Flemma RJ, et al. Inhibition of the adrenocorticotropin response to surgery in humans: interaction between dexamethasone and fentanyl. J Clin Endocrinol Metab. 1987;65:295–298.
6. Stoelting RK. Perioperative management of the patient receiving glucocorticoids. Curr Opin Anaesth. 1997;10:227–228.
7. Treschan T, Jurgen P. The vasopressin system: physiology and clinical strategies. Anesthesiology. 2006;105:599–612.
8. Gimpl G, Fahrenholz F. The oxytocin receptor system: structure, function, and regulation. Physiol Rev. 2001;81:629–683.
9. Nakao K, Inoue Y, Okabe K, et al. Oxytocin enhances action potentials in pregnant human myometrium: a study with microelectrodes. Am J Obstet Gynecol. 1997;177:222–228.
10. Bennett-Guerrero E, Kramer DC, Schwinn DA. Effect of chronic and acute thyroid hormone reduction on perioperative outcome. Anesth Analg. 1997;85:30–36.
11. Babad AA, Eger EI II. The effects of hyperthyroidism and hypothyroidism on halothane and oxygen requirements in dogs. Anesthesiology. 1968;29:1087–1093.
12. Hume DM, Bell CC, Bartter FC. Direct measurement of adrenal secretion during operative trauma and convalescence. Surgery. 1962;52:174–187.
13. Udelsmann R, Holbrook NJ. Endocrine and molecular responses to surgical stress. Curr Prob Surg. 1994;31:653–658.
14. Udelsman R, Goldstein DS, Loariaus DL, et al. Catecholamine-glucocorticoid interactions during surgical stress. J Surg Res. 1987;43:539–545.
15. Bovill JG, Sebel PS, Fiolet JW, et al. The influence of sufentanil on endocrine and metabolic responses to cardiac surgery. Anesth Analg. 1983;62:391–397.
16. Sebel PS, Bovill JG, Schellekens APM, et al. Hormonal responses to high-dose fentanyl anesthesia. Br J Anaesth. 1981;53:941–948.
17. Strout CD, Nahrwold ML. Halothane requirement during pregnancy and lactation in rats. Anesthesiology. 1981;55:322–323.
18. Collombat P, Hecksher-Sorensen J, Serup P, et al. Specifying pancreatic endocrine cell fates. Mech Dev. 2006;123:501–512.
19. Genuth S. Diabetes mellitus. Sci Am Med. 2001;9:VI:1–34.
20. Larner J. Insulin and oral hypoglycemic drugs: glucagon. In: Gilman AG, Goodman LS, Rall TW, et al, eds. The Pharmacological Basis of Therapeutics. 7th ed. New York, NY: MacMillan; 1985: 1490–1516.
21. Berne RM, Levy MN, Koeppen BM, et al. Physiology. 5th ed. St. Louis, MO: Mosby; 2004.
22. Rall TW, Sutherland EW. Formation of a cyclic adenine ribonucleotide by tissue particles. J Biol Chem. 1958;232:1065–1076.
23. Lamberts SWJ, van der Lely A, de Herder WW, et al. Octreotide. N Engl J Med. 1996;334:246–254.
24. Lin TM, Evans, DC, Chance RE, et al. Bovine pancreatic peptide: action on gastric and pancreatic secretion in dogs. Am J Physiol. 1977;232:E311–E315.
25. Hazelwood RL. The pancreatic polypeptide (PP-fold) family: gastrointestinal, vascular, and feeding behavioral implications. Proc Soc Exp Biol Med. 1993;202:44–63.
26. Adrian TE, Mitchenere P, Sagor G, et al. Effect of pancreatic polypeptide on gallbladder pressure and hepatic bile secretion. Am J Physiol. 1982;243:G204–G207.