William J. Stewart
Mitral valve disease is a common valvular abnormality, resulting from various etiologies and having well-understood, varied, and interesting clinical manifestations. Tricuspid valve disease is less common, occurring most often as a functional result of left-sided heart disease and/or pulmonary hypertension.
MITRAL VALVE ANATOMY
The mitral valve apparatus consists of anterior and posterior leaflets, chordae tendineae, anterolateral and posteromedial papillary muscles, and mitral annulus. To be inclusive, it also includes the atrial and ventricular myocardium. Mitral valve dysfunction may result from aberrations of any portion of the mitral valve apparatus, as a result of mechanical, traumatic, infectious, degenerative, congenital, or metabolic causes.
MITRAL VALVE PROLAPSE
Mitral valve prolapse (MVP) is found in approximately 2% of the population and is equally common in men and women. It is the most common cause of mitral regurgitation (MR) in the United States. Most such patients have a minor amount of MR and therefore a benign prognosis, with no significant cardiovascular symptoms or manifestations such as congestive heart failure. The diagnosis of MVP is made usually by bedside physical examination, finding a mid-to-late systolic click or multiple clicks, sometimes associated with a late systolic or pansystolic murmur. The murmur becomes earlier and louder with standing and the Valsalva maneuver, resulting from reduction in preload, which brings the mitral leaflets closer together before left ventricular (LV) contraction. The murmur of mitral prolapse becomes softer and later with squatting due to an increase in preload.
The diagnosis of MVP is best confirmed echocardio-graphically. The best two-dimensional (2-D) echocardiogram criterion is leaflet displacement beyond the line of the mitral annulus in the long-axis view. Because of the saddleshaped configuration of the mitral valve, caution must be taken when MVP is diagnosed only from parasternal long-axis, apical four-chamber, and apical two-chamber views. M-mode criteria require 2 or 3 mm of displacement, either as late systolic or holosystolic hammocking (Fig. 34.1). The presence of an eccentric jet direction of MR makes the diagnosis of MVP more likely. In general, prolapse with leaflet thickness >5 mm is considered “classic” MVP, whereas prolapse with thinner valve leaflets is considered “nonclassic prolapse.”

FIGURE 34.1 M-mode echocardiography showing late-systolic prolapse (arrow) of the mitral valve.
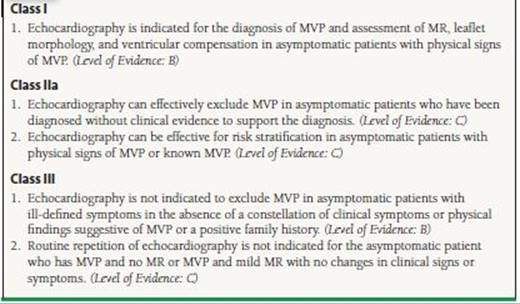
Accepted indications for performing echocardiographic study in mitral prolapse include establishing the diagnosis, determining the severity of MR, evaluating leaflet morphology, and defining LV size and function.1 The list implies that echocardiography should be used when it can add information to findings available from history and the physical examination. Indications for echocardiography may also include exclusion of MVP in patients diagnosed with MVP when there is no clinical evidence to support the diagnosis (Table 34.1). Subsequent or serial echocardiograms are not usually necessary if the patient is asymptomatic, unless there are clinical indications of severe or worsening MR.
TABLE
34.1 Evaluation and Management of the Asymptomatic Patient in MVP
From Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–e148, with permission from Elsevier.
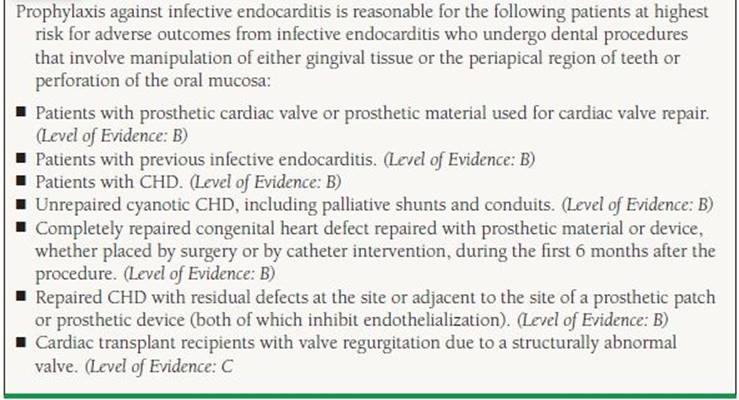
Most patients with mitral prolapse, even if there is a murmur, or if the echocardiogram shows significant MR, do not need antibiotic prophylaxis for endocarditis. Although that has been common practice prior to new guidelines that were published several years ago, the newest guidelines do not advise prophylaxis for native valve disease. Prophylaxis during procedures likely to cause bacteremia (including teeth cleaning) is recommended if the patient has had previous endocarditis or if a prosthetic valve has been implanted (Table 34.2).
TABLE
34.2 Recommendations for Infective Endocarditis Prophylaxis in Valvular Heart Disease
Adapted from Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Valvular Heart Disease). J Am Coll Cardiol. 2008;52:e1-e142; Wilson W Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116:1736-1754. Ref. (5,6).
The natural history of MVP is frequently benign. Follow-up studies in large population samples show that most patients with MVP do quite well, and most do not develop any significant congestive heart failure, atrial fibrillation (AF), stroke, or syncope. After a prolonged asymptomatic interval, a small percentage of patients with MVP develop more severe MR, ruptured mitral valve chordae (flail), left atrial and ventricular enlargement, or AF.2 In addition, with gradual progression of MR, LV dilatation and dysfunction may occur, leading to congestive heart failure. A substantial negative effect on survival has been seen in patients who develop LV dysfunction, AF, left atrial enlargement, age >50 years, and flail mitral leaflet. Recently, quantitatively severe regurgitation has also been associated with adverse prognosis.3,4
The development of infective endocarditis in patients with MVP is another mechanism of increase in MR. Predictors of infective endocarditis in patients with MVP include male gender, age >45 years, the presence of MR, and leaflet thickening and redundancy Patients with MVP with significant MR also have a small but significantly increased risk of sudden death, most likely secondary to ventricular tachyarrhythmias, which may be predicted by concomitant systolic dysfunction.
MVP has been associated with a pattern of multiple nonspecific symptoms such as palpitations, atypical chest pain, syncope, and anxiety, and this constellation has been frequently termed the “mitral valve prolapse syndrome.” No such associations have been found in multiple studies, but a small group of patients may have a complex set of symptoms associated with MVP For example, a few studies have shown a pattern of autonomic dysfunction, with increased catecholamines and decreased vagal tone, in patients with MVP.
The mainstay of medical management of patients with MVP is reassurance. Beta-blockers are the treatment of choice for patients with increased adrenergic symptoms such as palpitations, chest pain, or anxiety, though some of these effects may be the placebo effect. In patients with MVP and transient ischemic attacks (TIAs) or stroke, the treatment is usually just aspirin (81 to 325 mg/d). Warfarin may be indicated in some patients with MVP and recurrent TIA or stroke. In addition, in patients with AF, there should be a low threshold for instituting anticoagulation, individualized for the patient’s risks of stroke versus bleeding. Surgery for MVP is only a consideration in patients with more severe MR, similar to other forms of nonischemic MR, which is discussed later.
ACUTE MITRAL REGURGITATION
Acute MR is an uncommon medical condition of grave importance, requiring urgent medical and often surgical intervention. Acute MR also occurs due to disruption of mitral valve leaflets, chordae tendineae, or papillary muscles that may result from infective endocarditis, acute myocardial infarction, trauma, or rheumatic fever. The most common cause is probably acute myocardial ischemia leading to acute LV enlargement, severe MR, and acute pulmonary edema.
High left atrial pressure and reduced left atrial compliance secondary to severe MR are the mechanisms of pulmonary edema. A less common complication of severe acute MR is reduced forward flow with cardiogenic shock. Acute MR usually presents as sudden and marked increase in congestive heart failure symptoms, with weakness, fatigue, dyspnea, and sometimes respiratory failure and shock. Peripheral vasoconstriction, pallor, and diaphoresis are usually associated presenting signs. In some patients, a loud systolic murmur and a diastolic rumble or third heart sound are heard. In others, a very soft murmur or no murmur is heard, because the severity of MR and the lack of atrial compliance lead to midsystolic equalization of pressures between the left atrium and ventricle midway through systole. In addition, the acute nature of the condition obscures the mitral murmur by other aspects of the patient’s distress, including orthopnea, precluding a good exam in the left lateral decubitus position.
Echocardiography is the diagnostic procedure of choice. In acute coronary syndromes, emergency catheterization and cardiac surgery are life saving. There is little need for contrast LV angiography, except in cases where there is discrepancy in clinical and noninvasive findings. In some cases, hemodynamic measurements and monitoring may also be helpful in management.
Acute MR after myocardial infarction is discussed in detail in another chapter of this book. It is the cause of about 7% of cases of cardiogenic shock after myocardial infarction. The onset of the MR is most commonly between days 2 and 7 after myocardial infarction. The MR in most patients, like our example at the beginning of this chapter, involve a functional mechanism, from apical tethering of normal leaflets as a consequence of acute LV dysfunction and enlargement. Focal infarction most commonly involves the posteromedial papillary muscle, because it derives its blood supply solely from one artery, the right coronary artery. In contrast, the anterolateral papillary muscle has a dual blood supply, often derived partly from the circumflex and partly from left anterior descending artery. Despite the devastating effects of acute severe MR, the infarct size is not always large, with some smaller infarctions (<25% of LV), with a mild to moderate enzyme leak.
Hemodynamic stabilization with prompt surgical intervention is the most effective therapy for most cases of acute MR. Vasodilator therapy with intravenous nitroprusside and nitroglycerin may lead to decreased MR, increased forward flow, and reduced pulmonary congestion. Intra-aortic balloon pump (IABP) counterpulsation is also effective in reducing regurgitant volume and LV filling pressure, while increasing forward output and mean arterial pressure, and is frequently used for initial stabilization, as a bridge to prompt surgical intervention. However, if appreciable aortic regurgitation (AR) is present, IABP is contraindicated because it worsens the AR.
CHRONIC MITRAL REGURGITATION
The physiology of MR includes a number of classical features (Fig. 34.2). The patient with MR of any cause usually has a pansystolic murmur, best audible at the apex, often radiating to the axilla. In severe MR, this murmur also may be heard in the left paravertebral area of the back. The pulmonic component of the second heart sound may be louder than normal if there is pulmonary hypertension. An inflow sound (a third heart sound or an early diastolic rumble) at the apex may be heard in some patients if the MR is severe. The apical impulse is enlarged, displaced laterally, and exaggerated, reflecting the hyperdynamic LV motion. Left atrial pressure (and pulmonary capillary wedge pressure) is elevated by the regurgitant flow, with an associated systolic V wave, though its height is not a reliable measure of the severity of MR. The left atrium and the diastolic size of the left ventricle are enlarged. As pulmonary venous pressure becomes elevated, dyspnea or even pulmonary congestion may occur. In the later phase, pulmonary hypertension may develop, causing pulmonary artery dilation, right-sided heart failure, and systemic venous congestion.
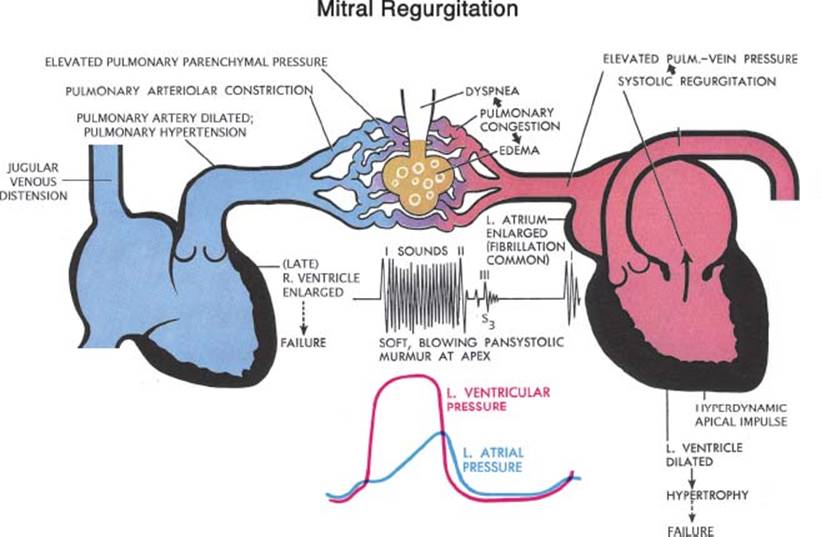
FIGURE 34.2 Schematic diagram representing pathologic complications of chronic MR. (Netter illustration adapted from www.netterimages.com. © Elsevier Inc. All rights reserved.)
Untreated chronic mitral valve abnormalities (including regurgitation or stenosis) often lead to a common endpoint, with left atrial enlargement, pulmonary hypertension, AF, and left-sided congestive heart failure. If the situation is not corrected, it may progress to include left atrial thrombosis, hemoptysis, and right-sided heart failure.7 Cardiac output is usually normal in the early phases, but may be reduced in the later phases of the disease if the MR goes untreated.
The natural history of chronic MR may involve many years of being asymptomatic, the so-called compensated phase of MR. In early years, chronic MR leads to increased LV size and mass and increased LV end-diastolic volume associated with a normal or elevated ejection fraction. At this stage there are few or no symptoms, because the dilated and compliant left atrium and LV allow accommodation of the regurgitant volume at normal filling pressures. However, as these mechanical changes progress, LV contractile dysfunction and hemodynamic derangements begin to occur, including pulmonary congestion, heart failure symptoms, and increases in LV end-systolic and end-diastolic diameter. Reduced forward flow is a very late occurrence.
The chest x-ray often shows left atrial enlargement with a double-density and widened carina, with no other findings early in the course of chronic MR. Later, the left ventricle dilates and there may be signs of pulmonary venous congestion. The lateral chest x-ray may show posterior protrusion of the left atrial cavity, a prominent pulmonary trunk, or small pleural effusions.
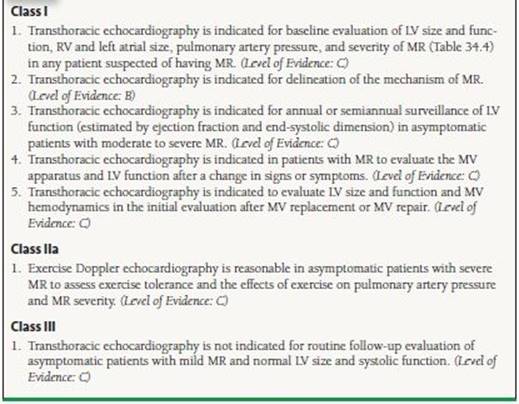
After clinical evaluation, a transthoracic echocardiogram (TTE) is useful for determining the MR severity, mechanism, etiology, presence of flail, LV size and function, left atrial size, abnormalities of other valves, and right ventricular (RV) systolic pressure (Table 34.3). It is also useful for assessing serial changes in LV size and function and evaluating the patient after a change in symptoms. An exercise echo is often useful for determining the change with exercise in LV size, LV function, or RV systolic pressure, and for discovering inducible symptoms or arrhythmias. Occasionally a transesophageal echocardiogram may be needed to better assess the severity and etiology of MR (Table 34.4). An exercise echocardiogram is often useful for determining the severity and effect of the disease on the patient’s exercise hemodynamics. It helps to detect latent myocardial dysfunction, and inducible problems not present at rest including pulmonary hypertension, arrhythmias, symptoms, and decreased ejection fraction. Cardiac catheterization for left ventriculography (Fig. 34.3) and hemodynamic measurements is helpful in rare specific conditions. Magnetic resonance imaging may also be of value, but its routine use in management of patients with chronic MR is unproven.
TABLE
34.3 Indications for Transthoracic Echocardiography in MR
From Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol.2006;48:e1–e148, with permission from Elsevier.
TABLE
34.4 Indications for TEE in MR

From Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48: e1–e148, with permission from Elsevier.

FIGURE 34.3 Left ventriculogram in the RAO projection in diastole (left) and systole (right), showing severe MR that completely fills the left atrium.
MECHANISM OF MITRAL REGURGIATION
The mechanism of MR can be determined by echocardiography by looking at leaflet motion and color Doppler jet direction.8 First, the patient’s leaflets are categorized by 2-D echocardiography into those with normal, excessive, or restricted motion. Then additional information is gained by looking at the location, and direction of the regurgitant jet by color Doppler.
Mitral valve disease may have numerous causes, including myxomatous degeneration, ischemic, rheumatic, congenital, endocarditis, autoimmune disorders, and post radiation valve lesions. In the last half-century, there has been a remarkable increase of the frequency of myxomatous degeneration in surgical populations, with a decline in postinflammatory (rheumatic) cases, while ischemic- and infective endocarditis–associated MR have continued at a relatively low frequency.
In myxomatous degeneration, the most significant abnormality is abnormal elasticity of various portions of the mitral valvular apparatus, including the mitral annulus, chordae tendineae, and leaflets. There may be a variable amount of redundancy and enlargement of the leaflets (which, in the extreme is called Barlow syndrome) and chordae (sometimes called fibroelastic deficiency). In long-axis views, it is easy to see which leaflet is moving into the atrial side of the coaptation line in systole, indicating prolapse or flail. Additionally, the direction of the regurgitant jet provides supplemental diagnostic information (Fig. 34.4). In patients with excessive leaflet motion, the jet is directed to the opposite side of the most affected leaflet. Intercommissural views (transthoracic apical two-chamber and midesophageal transesophageal views aligned parallel to the intercommissural line at about 60 degrees multiplane angle) are useful for determining which portion of a leaflet is abnormal. Parasternal short axis and the “surgeon’s view” from the left atrium by three dimensional (3-D) echo also is helpful in appreciating the exact location of various lesions (Fig. 34.5) and differentiating the presence of multiple mitral abnormalities.

FIGURE 34.4 Transthoracic apical four-chamber 2-D echo image (left) and color Doppler image (right) in a patient with posterior leaflet flail. Note that the MR jet is deflected to the opposite (anteromedial) side of the left atrium by the unsupported posterior leaflet. Also note the flow convergence on the LV side of the jet, with a measured aliasing radius of 0.77 cm, from which a ROA of 0.46 cm2 was calculated, based on a measured MR maximum velocity of 505 cm/s.
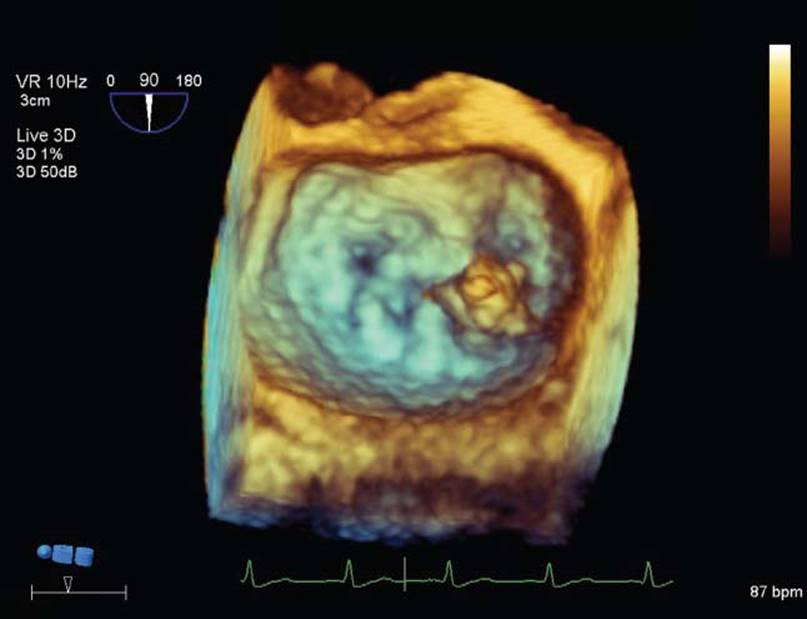
FIGURE 34.5 Transesophageal 3-D echo image using the “surgeon’s view,” showing that the morphology of the mitral valve causing regurgitation involved a flail portion (possible vegetation) located at the medial commissure (to the right on the image).
Rheumatic heart disease is characterized by leaflet thickening, diastolic mitral doming, valvular and subvalvular fibrosis, and various degrees of systolic and diastolic restriction of leaflet motion. In most cases of restriction involving both leaflets, the jet of MR is central. In some patients, the posterior leaflet is more restricted and the jet direction is posterior.
Ischemic MR most commonly represents “functional MR,” which results from remodeling, enlargement, and “sphericalization” of the left ventricle. Functional MR from nonischemic cardiomyopathy is very similar. Both are caused by “apical tethering” of normal leaflets (Fig. 34.6). The length of mitral tissue, including the leaflets, chordae, and papillary muscle, is fixed. As the left ventricle dilates, often after myocardial infarction, the LV wall and papillary muscles are displaced outward, which tethers all or part of the mitral leaflets downward away from the left atrium, reducing the amount of leaflet tissue available for coaptation. In many cases, the result is MR, with a central, or in some cases, a posterior jet direction. In rare cases, a focal infarction may cause elongation or disruption of the papillary muscle, leading to excessive leaflet motion (often involving both leaflets) most commonly the medial side of both leaflets from medial papillary muscle abnormalities.
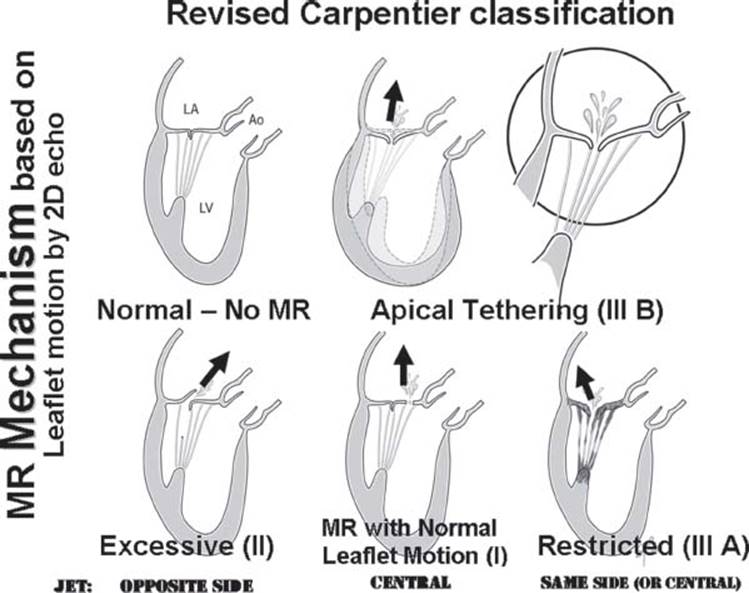
FIGURE 34.6 Artist’s renderings of the mechanisms of MR defined by determination of leaflet motion by echo imaging (similar to the Carpentier classification (I, II, IIIa, and IIIb) and determination of jet direction using color Doppler. Apical tethering, often from ischemic heart disease, due to LV enlargement (Carpentier Class IIIb) is often called “functional” MR. Though the annulus may be dilated in proportion to the ventricular enlargement, the primary problem is the ventricle, not the annular dilation.
Mitral valve endocarditis can cause leaflet or chordal disruption, flail, and perforations. These often cause MR with associated nodular hypermobile densities (vegetations) that are the echocardiographic hallmarks of the disease. Care should be taken to look at adjacent valves and the perivalvular tissue looking for abscess formation or paravalvular leakage. MR secondary to the phospholipid antibody syndrome (the Lupus anticoagulant) is associated with symmetric thickening of leaflets, noninfected vegetations, and, at a later stage of the disease, fibrosis and leaflet restriction.
QUANTITATION OF MITRAL REGURGITATION
MR may be quantitated using a variety of echo and Doppler methods, including spatial mapping, flow convergence, pulmonary vein velocity patterns, vena contracta width, continuous-wave Doppler density and shape, and quantitation of antegrade valvular flow volumes. It is best to use a “weighted average” of multiple methods, emphasizing more the methods that have good-quality data in that patient.9
The flow convergence method, also called the proximal isovelocity surface area (PISA) method, involves assessing the color images on the LV side of the MR (Fig. 34.7).10
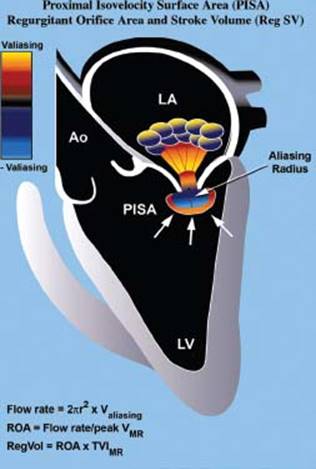
FIGURE 34.7 Method of quantifying the severity of MR using the PISA method (see text for details). (Adapted from Savage RM, Aronson S, Thomas JD, et al. Comprehensive Textbook of Intraoperative Transesophageal Echocardiography. Lippincott Williams & Wilkins. Chapter 28, 2005:512.)
This flow convergence zone is the location where the blood is accelerating, as the flow stream narrows progressively to the regurgitant orifice, where there is a pressure drop from LV pressure to left atrial pressure. Color Doppler tracks the location of increases in velocity on the LV side of the regurgitant orifice and shows this as color aliasing in the proximal convergence zone. When the shape of the aliasing contour is hemispheric, one can calculate the surface area of the aliasing hemisphere from the radius of the hemisphere. Flow can therefore be calculated from the aliasing velocity (v), extracted from the “color bar” (reflecting machine settings), and the measured radius (R) measured from the center of the jet to the transition of color aliasing. When this is combined with the maximum velocity, the maximum systolic area of the regurgitant orifice can be calculated according to the formula 2πR2v divided by maximum systolic velocity through the valve (Vmax) obtained by continuous-wave Doppler. The advantage of this formula is that it calculates the actual size of the regurgitant lesion, a fundamental parameter of valve integrity, which is less load dependent than other parameters. A maximum instantaneous regurgitant orifice area (ROA) > 0.4 cm2 is indicative of severe regurgitation, whereas <0.2 cm2 is considered mild.
Pulmonary vein flow profiles (Fig. 34.8) are also useful for determination of severity of MR.11 The normal pulmonary vein pattern includes a velocity during ventricular systole that is higher than antegrade velocity during diastole, a pattern that persists in mild and sometimes moderate MR. When the regurgitation is moderate or moderately severe, the systolic velocity of pulmonary vein flow becomes blunted, with systolic velocity less than diastolic velocity. With even more MR, there is cessation of systolic flow. In patients with severe MR, in one or the other pulmonary vein profile, there is often reversal of systolic flow, with retrograde flow occurring, away from the left atrium during ventricular systole. This occurs because of the large V wave during ventricular systole in the left atrial pressure, which transiently becomes higher than pulmonary parenchymal pressure.
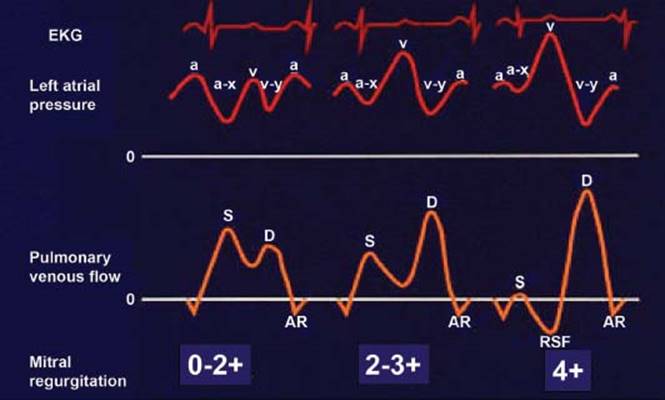
FIGURE 34.8 Stylistic ECGs, left atrial pressure waveforms, and pulmonary vein pulsed Doppler velocity recordings, in three patients: normal or mild or moderate MR (on the left), moderately severe or 2 to 3+ MR (in the middle); and severe, 4+ MR (on the right). Note the reversal of systolic flow (RSF) associated with severe MR, which results from the systolic V wave in the left atrial pressure. (Adapted from Klein AL, Obarski TP, Stewart WJ, et al. Transesophageal Doppler echocardiography of pulmonary venous flow: A new marker of mitral regurgitation severity. J Am Coll Cardiol. 1991;18:518–526.)
Medical management of patients with MR includes diuresis to correct any volume overload. Rate and rhythm control, often with beta-blockers, is often needed because many patients have AF. Aggressive blood-pressure control and risk-factor modification should be a routine part of management of these patients.
There are no large randomized studies comparing surgical with medical management of MR. Patients who have symptoms due to the MR should undergo surgery before LV dysfunction occurs.1 There are no randomized surgical studies in asymptomatic patients with severe MR. If the patient has repairable MR that is truly severe quantitatively, American College of Cardiology/American Heart Association (ACC/AHA) guidelines (Table 34.5) state that mitral valve surgery should be recommended if the patient has developed any decrease in LV ejection fraction (LVEF), significant dilation of end-systolic LV size (>4.5 cm systolic diameter), AF, or significant pulmonary hypertension. In addition, many centers recommend mitral valve surgery for selected patients with severe MR when they also have a flail mitral leaflet,12 or when there is exercise echo evidence of “latent LV dysfunction,” defined by a declining EF or increasing end systolic volume (ESV) with exercise.13,14
TABLE
34.5 Indications for Mitral Valve Operation
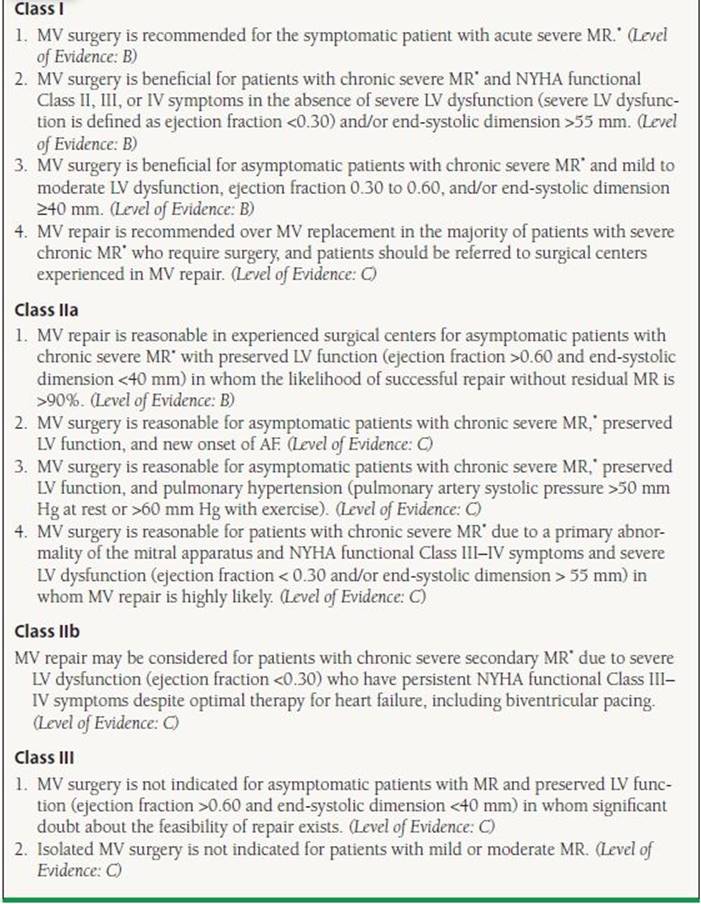
From Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–e148, with permission from Elsevier.
Guidelines do not advocate mitral valve surgery for patients with ejection fraction <30%. However, selected symptomatic patients with severe LV dysfunction may benefit from mitral valve operation, particularly if they have moderate ventricular dilation and very severe regurgitation (Fig. 34.10).

FIGURE 34.9 Transesophageal 3D image in the “surgeon’s view”, of a patient who had recurrence of mitral regurgitation after initially successful repair with a Geoform ™ mitral annuloplasty. Note the focal dehiscence of the ring, visible as the dark space just outside its mid posterior portion where the ring is indented inward by design.
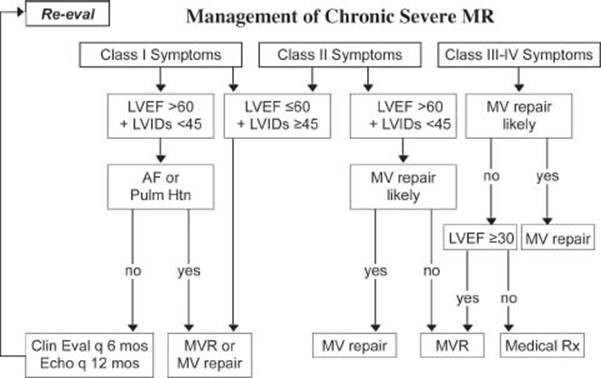
FIGURE 34.10 Flow chart summarizing management of chronic MR. (Adapted from Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–e148.)
Mitral valve repair is now the surgical management of choice for most cases of MR, which does not require anticoagulation as do mechanical mitral prostheses.7 In addition, repair preserves the mitral apparatus and leads to improved LV function and survival compared to mitral valve replacement (MVR) when the chordal are not preserved. However, for many conditions, such as rheumatic mitral valve disease or in those with significant subvalvular thickening and major loss of leaflet substance, MVR is the best option, because repair may not be feasible or durable with 0.5 to 1% of patients returning for reoperation per year after initially successful repair (figure 34.9). If so, the prosthesis should be implanted with preservation of the mitral valve chordal apparatus, as much as feasible.
Based on the guidelines, cardiac catheterization is indicated in patients with angina or previous myocardial infarction, individuals with one or more cardiac risk factors, and when ischemia is the cause of MR.1As long as there is no clinical suspicion of coronary artery disease, asymptomatic males <40 years of age, and asymptomatic females <50 years of age, do not need to undergo preoperative coronary angiography because of low likelihood of significant coronary disease (Table 34.6).
TABLE
34.6 Indications for Cardiac Catheterization in MR
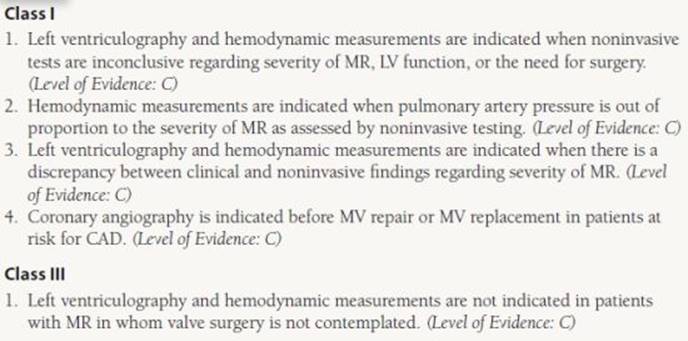
Adapted from Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–e148.
MITRAL VALVE STENOSIS
The primary cause of mitral stenosis (MS) is rheumatic heart disease, a chronic, postinfectious, inflammatory condition that leads to fusion and fibrosis of commissural, cuspal, and chordal portions of the mitral valve apparatus. Less commonly, MS is a complication of malignant carcinoid, radiation, systemic lupus erythematosus, rheumatoid arthritis, Whipple disease, and other rare connective tissue diseases. The mitral valve area of a normal person is 4.0 to 5.0 cm2. Symptomatic mitral valve stenosis occurs when the valve area is less than about 1.5 cm2. The first symptoms are mild exercise intolerance or dyspnea. The difficulties accelerate when the patient develops AF, particularly if the ventricular rate is rapid. The natural history of MS is a life-long,continuous, and slow process (Fig. 34.11) of progressive fibrosis of the mitral valve. In western countries, it usually takes 20 to 40 years after occurrence of a streptococcus infection and rheumatic fever for the patient to develop symptoms of rheumatic mitral valve disease. In underdeveloped countries where strep organisms are more virulent, this interval is much shorter. Dyspnea with exertion may occur several years before the patient experiences decompensated heart failure. Patients with MS and AF occasionally present with neurologic sequela, due to embolization of clot, occurring due to blood stasis in the left atrium. With progression of disease and increased left atrial pressure, orthopnea, paroxysmal nocturnal dyspnea, and occasionally hemoptysis may occur.
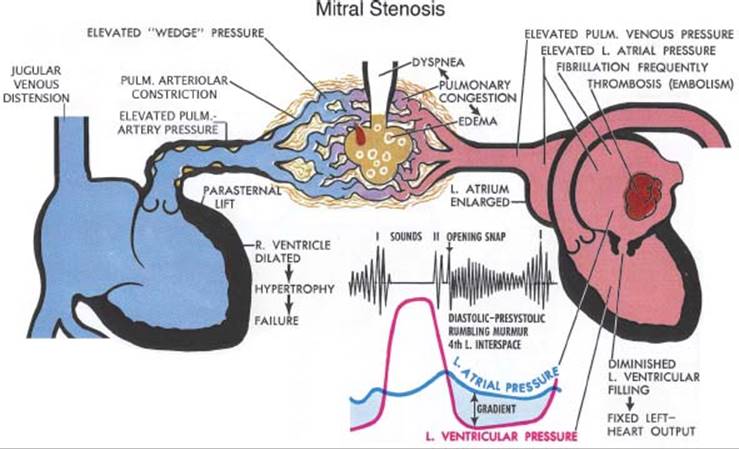
FIGURE 34.11 Schematic diagram representing pathologic complications of MS. (Netter illustration adapted from www.netterimages.com. © Elsevier Inc. All rights reserved.)
A loud first heart sound, an opening snap (OS), and a diastolic rumble are the classic auscultatory features of MS. The intensity of the pulmonic component of second heart sound is important in the bedside estimate of the severity of secondary pulmonary hypertension. The OS is caused by sudden tensing of the valve leaflet under the greater than usual diastolic gradient. The OS may occur between 50 and 120 milliseconds after the A2 component of the second heart sound. The time between A2 and OS is inversely associated with severity of MS; therefore, a short A2-OS interval is a bedside indication of severe MS, due to the gradient occurring on the more steep descending slope of LV pressure curve. However, patients with severe immobility of the mitral valve, despite significant MS, often have no OS, or it is soft in intensity.
The electrocardiographic (ECG) features of MS include left atrial enlargement, the so-called P mitrale, in patients in sinus rhythm, and occasionally right axis deviation or RV enlargement. AF is a frequent arrhythmia in these patients. Radiographic features of MS included the enlarged left atrium, enlarged pulmonary arteries, mitral valve calcium, and signs of congestive heart failure such as Kerley B lines.
Although the history, physical exam, chest x-ray (Fig. 34.12), and ECG may suggest MS, 2-D echo and Doppler echocardiography are the tools of choice for its diagnosis. The characteristic findings of MS on the 2-D echo are restriction of diastolic motion, with doming in diastole of the anterior and posterior leaflets (Fig. 34.13). There is often contraction and fibrosis of the various components of the mitral apparatus, often with thickening of the submitral chordae and papillary muscles. In the parasternal short-axis view, the mitral valve can be planimetered to determine the effective mitral valve area. To do so, one must scan up and down the mitral valve short axis, searching for the place where the early diastolic (maximum in time) orifice size is smallest (i.e., smallest in space) (Fig. 34.14). In order to provide accurate measurements, the gain settings must not be too high or too low. In addition, echo imaging is useful for assessing the degree of valve thickening, decreased mobility, calcification, and subvalvular disease (the “splittability index” or Wilkin score), which helps to predict the success and durability of percutaneous balloon valvotomy versus surgical options.15 Echo is also essential for exclusion of other valvular lesions, because it is common for patients with rheumatic mitral disease to have concomitant aortic and/or tricuspid valve disease.
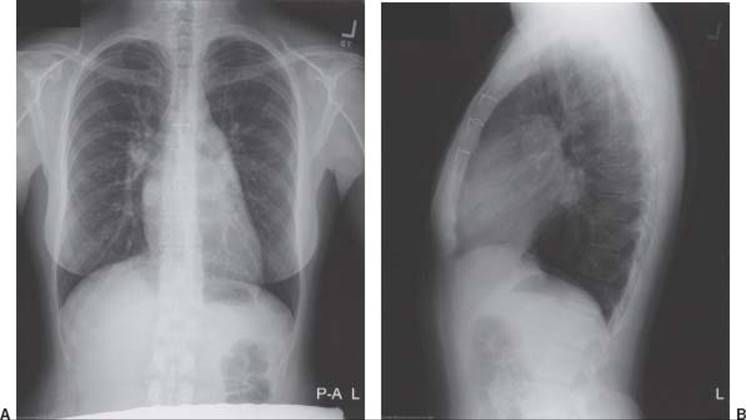
FIGURE 34-12 Posteroanterior chest x-ray (A) showing typical features of rheumatic MS, with an enlarged left atrium (note the widened carina and round double density), and prominent bilateral pulmonary artery shadows, with normal LV size. This patient was not in heart failure at the time of the study. Lateral chest x-ray (B) showing prominent pulmonary arteries and left atrial enlargement protruding from the cardiac silhouette posteriorly. This patient had midsternal wires from a previous thoracotomy.
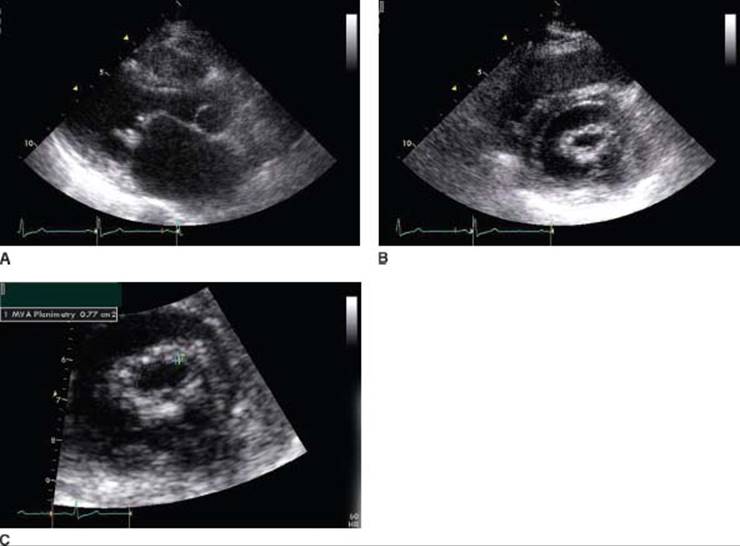
FIGURE 34.13 Diastolic stop frames from 2-D echo parasternal long-axis (A) and short-axis (B) views of a patient with severe rheumatic mitral valve stenosis. Note the diastolic doming and the leaflet thickening of the mitral valve; as well as left atrial enlargement and normal LV size. In (C), a magnified view of the maximum diastolic opening of the valve has been planimetered, finding a mitral valve area of 0.77 cm2, indicating severe stenosis.
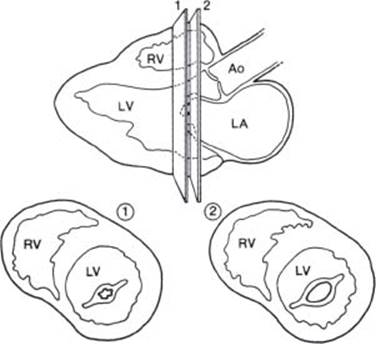
FIGURE 34.14 Artistic diagram of the parasternal long-axis transthoracic image (top), illustrating the technique of obtaining the various parasternal short axis transthoracic images (lower two diagrams). Planimetry to measure the flow-limiting valve area of MS would obtain a smaller orifice area in the image plane (1) on the lower left, than in image plane (2) on the lower right, because of the funnel-shaped mitral valve. RV, right ventricle. (Adapted from Salcedo E. Atlas of Echocardiography. W. B. Saunders, Philadelphia. 1985:73.)
Apical (transthoracic echo) or midesophageal (transesophageal echo) windows for recording of diastolic antegrade mitral velocity (V) are useful for quantitation of severity. Doppler accurately estimates mean mitral gradient, mitral valve area, and estimation of RV systolic pressure. The mean mitral gradient is the temporal average of instantaneous gradients throughout diastole, using the modified Bernoulli equation (4V2). However, this particular measurement is very subject to changes with increased heart rate, which reduces the diastolic interval and increases the mean mitral gradient. It is also subject to concomitant MR (which increases antegrade flow) and other changes in cardiac output (with low cardiac output causing a lower mitral gradient). Severity of MS can also be judged using the mitral pressure half-time (PHT— the time in milliseconds that it takes for the maximum transmitral velocity to fall to 71% of its initial velocity (Vmax divided by the square root of 2). Mitral valve area is calculated from the formula: 220/PHT (Fig. 34.15). In general, a valve area of 4 to 6 cm2 is normal, 1.6 to 2.0 cm2 is mild, 1.1 to 1.5 cm2 is moderate, and ≤1.0 cm2 is severe MS (Fig. 34.16). Estimation of RV systolic pressure is made from the maximum tricuspid regurgitation (TR) velocity.

FIGURE 34.15 Apical four-chamber echo image (A) and matching artistic drawing (B) from which was recorded a continuous-wave Doppler of mitral antegrade velocity (C) in MS. PHT (t1/2), measured as 295 ms, is divided into 220 milliseconds, to derive the mitral valve area, in square centimeters. (Adapted from Stewart et al. in Pohost GM Cardiac Imaging. Chicago: Yearbook Inc.; 1986:76.)
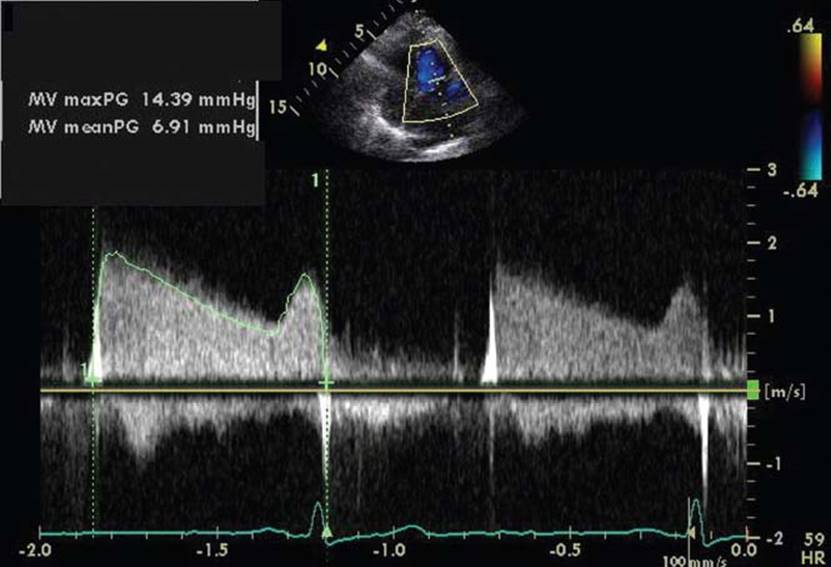
FIGURE 34.16 Continuous-wave Doppler recordings from apical four-chamber view of the same patient shown in Figure 34.13, showing in A: planimetry of the maximum velocity envelope to determine mean diastolic mitral gradient (6.9 mm Hg); and in B: measurement of the pressure half-time (271 milliseconds), indicating severe MS with a relatively low cardiac output.
Although often supplanted by a complete Doppler study, an invasive right and left heart catheterization should be reserved for patients with discrepancy between Doppler-derived hemodynamics and clinical symptoms or when there is elevation of pulmonary artery pressures out of proportion to mitral valve area or diastolic gradients (Table 34.7). Simultaneous Doppler and catheterization studies, using a transseptal measurement of left atrial pressure, have revealed that Doppler-derived mean mitral gradients and PHTs are accurate in most circumstances. Use of the pulmonary capillary wedge technique may overestimate the mitral gradient because of incomplete wedging and hence overestimation of the left atrial pressure.
TABLE
34.7 Indications for Echocardiography in MS

From Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48: e1–e148, with permission from Elsevier.
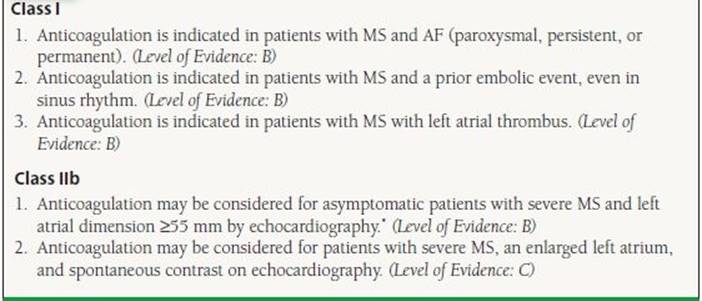
Medical management of patients with MS often should include aggressive anticoagulation in patients at high risk. Patients who have AF or previous systemic embolic events should definitely be anticoagulated with warfarin. The ACC/AHA guidelines recommend anticoagulation in all patients with MS with paroxysmal or chronic AF and in those with prior embolic events (Table 34.8).
TABLE
34.8 Medical Therapy for Prevention of Systemic Embolization in MS
From Bonow RO, Carabello BA, Chatteq’ee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48: e1–e148, with permission from Elsevier.
Patients with moderate or greater degree of MS should avoid strenuous physical activity sufficient to cause severe symptoms. In those with exertional symptoms, beta-blockers or calcium channel blockers may be beneficial to increase the duration of diastole, especially if symptoms occur with rapid heart rate. Salt restriction and diuretic use are necessary components for management of pulmonary congestion in these patients. The incidence of AF is around 30% to 40% in patients with MS.
AF causes loss of the atrial component of ventricular filling. When AF is rapid, there is also a decrease in percentage of time per minute of diastolic filling, increasing the average gradient across the stenotic mitral valve, because the mitral flow spends a greater portion of its time in the “early” portion of diastole when velocity is higher. Therefore, anything that accelerates ventricular rate has deleterious hemodynamic consequences in MS. In patients with rapid AF and hemodynamic instability or evidence of shock with ongoing end-organ underperfusion, direct-current cardioversion should be performed without delay.
At the onset of AF in any patient with MS, rapid assessment and management with agents such as beta-blockers, calcium channel blockers, or intravenous digoxin may be necessary. In general, stable patients should undergo transesophageal echocardiography (TEE) to look for thrombus, or be anticoagulated for 3 weeks prior to cardioversion and after the cardioversion, often indefinitely, due to the risk of recurrent embolization.
The decision to intervene with surgery or catheterbased therapy in patients with MS depends largely on the severity of symptoms, but also depends on the quantitative severity of MS, the level of pulmonary hypertension, the history of atrial arrhythmias, and thromboembolic complications. Congestive heart failure that is New York Heart Association (NYHA) Class II or above, with severe MS, <1.0 cm2 valve area, is a clear indication for intervention. The presence of pulmonary hypertension, with systolic pressures above 55 at rest or above 60 mm Hg with exercise, is considered an indication for intervention even without symptoms.
Based on these criteria, intervention may take the form of balloon valvotomy, open commissurotomy, or MVR (Table 34.9). Balloon valvotomy is a therapeutic technique, done through a transseptal catheterization, that can accomplish enlargement of the mitral orifice in selected patients with MS who have suitable anatomy. Balloon valvotomy is more likely to be feasible if the echo-derived “splittability index” is below about 9. Balloon valvotomy is reasonably safe and has results similar to that of open mitral commissurotomy. Prior to a transcatheter therapeutic procedure, transesophageal echo is warranted to exclude left atrial thrombus and moderately severe (3+ on a scale of 4+) or more MR, both of which are contraindications to the balloon valvotomy technique. In general, mitral valve area typically doubles with a successful balloon valvotomy procedure in which both commissures are split.
TABLE
34.9 Indications for Percutaneous Mitral Balloon Valvotomy In MS
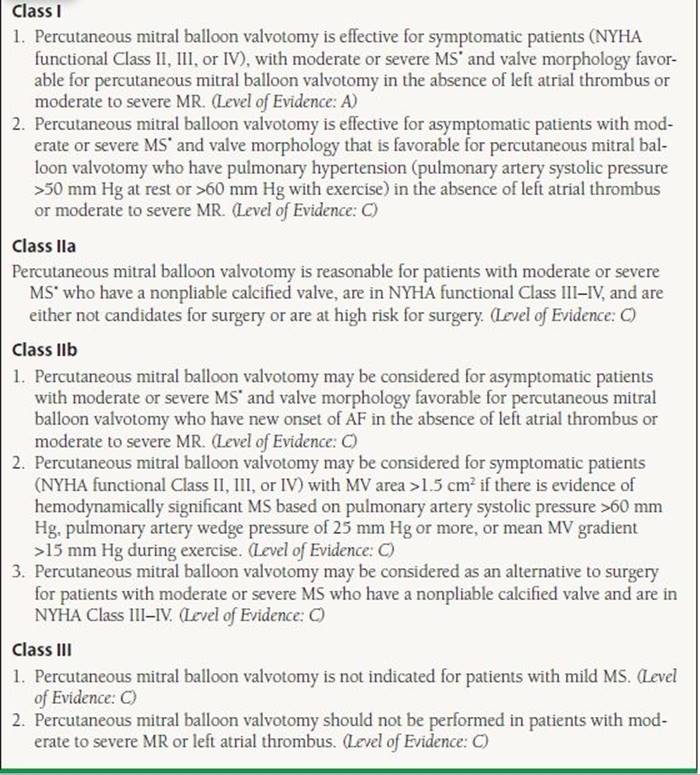
From Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48: e1–e148, with permission from Elsevier.
Patients with a left atrial thrombus, significant MR, or a high echo splittability index should be considered for valve repair or valve replacement rather than balloon procedures. Mitral valve repair can be accomplished in selected patients with MS, particularly when the valve has a moderate or lower splittability index, and is the procedure of choice when there is concomitant substantial MR, especially if there is a contraindication to anticoagulation.
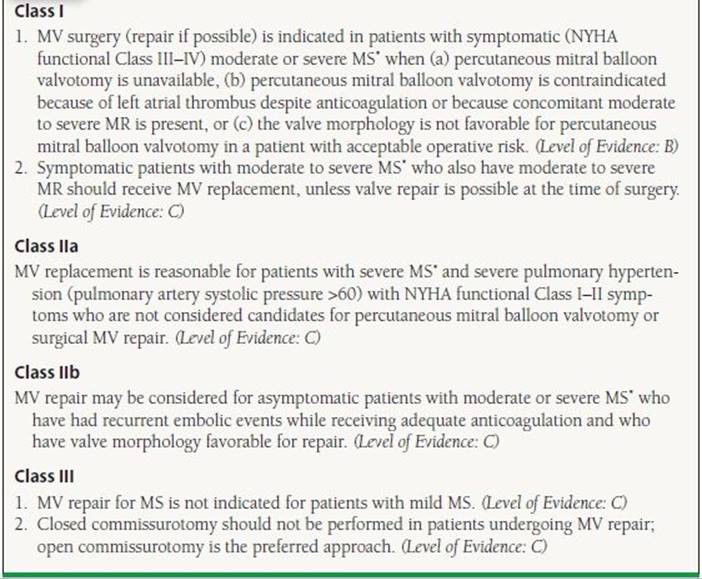
MVR is an alternative procedure for patients who are not candidates for percutaneous mitral valvotomy or surgical commissurotomy (Table 34.10). MVR is the surgery of choice in patients with heavily calcified, immobile, fibrotic valves with a high splittability index, where percutaneous mitral valvotomy or surgical commissurotomy may not be feasible, may leave the patient with substantial dysfunction, or may be prone to recurrence of dysfunction. Traditionally a mechanical valve is used for most patients having mitral replacement who are <50 to 60 years of age, whereas older patients undergo bioprosthetic valve replacement.
TABLE
34.10 Indications for Surgery for MS
From Bonow RO, Carabello BA, Chatteq’ee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48: e1–e148, with permission from Elsevier.
TRICUSPID VALVE REGURGITATION
TR is a very common valvular abnormality, but it is often mild or moderate in severity, and in those cases, usually asymptomatic. In severe TR, right-sided heart failure often occurs, and the patients develop ascites, hepatic congestion, and peripheral edema (Fig. 34.17). In addition, patients may complain of fatigue, shortness of breath, and exercise intolerance as a result of an inability to augment cardiac output because of the severe TR.
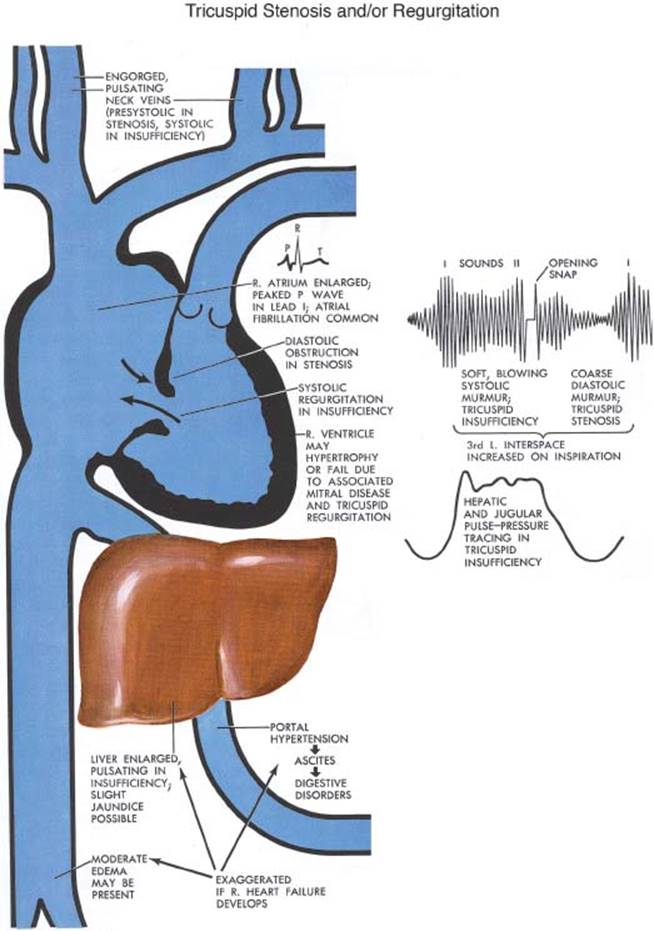
FIGURE 34.17Schematic diagram representing pathologic complications of tricuspid stenosis and regurgitation. (Netter illustration adapted from www.netterimages.com. © Elsevier Inc. All rights reserved.)
On physical exam, patients often have distended jugular veins, leg and pedal edema, and an enlarged liver. The jugular vein profile and the right atrial pressure waveforms show a positive systolic V wave from the effects of the TR. On cardiac auscultation, there may or may not be a holosystolic murmur, which may be high pitched, much lower pitched, or absent. The murmur is often heard best at the right or left sternal border, and classically increases with inhalation, though this is not a reliable finding. Maneuvers that increase venous return, such as leg raising, augment the intensity of the TR murmur. In severe TR, an S3 or an early diastolic rumble may be heard. When there is associated pulmonary hypertension, the second heart sound may be loud. Palpation of the heart often reveals a RV lift or heave. Palpation of the liver reveals pulsatile hepatomegaly, which may achieve vast proportions. In severe, long-standing TR, chronic passive congestion of the liver occurs, and the patient may develop numerous secondary phenomena. These include abdominal bloating and tenderness, early satiety, jaundice, ascites, and other “digestive symptoms.” Variable diffuse elevations of blood tests of liver function, cardiac cirrhosis, and progressive cachexia may also occur. Many patients with severe TR have been misdiagnosed as having various gastrointestinal disorders.
The most useful diagnostic modality is echocardiography. Color Doppler can define the severity and presence of the regurgitant flow (Fig. 34.18). Care should be give to the Nyquist setting in color imaging, as severe intrinsic TR may be low velocity and may not show color aliasing at the usual Nyquist settings. Two-dimensional echocardiography may identify other structural abnormalities involved in the etiology of the TR, such as leaflet prolapse, flail, fibrosis, or annular dilation. Enlargement of the right atrium and RV is common as is RV dysfunction. Other findings include paradoxical septal motion as a result of RV diastolic overload, and reversal of flow during ventricular systole in the inferior vena cava or hepatic veins by pulsed Doppler. Continuouswave Doppler is used to define the severity of pulmonary hypertension.
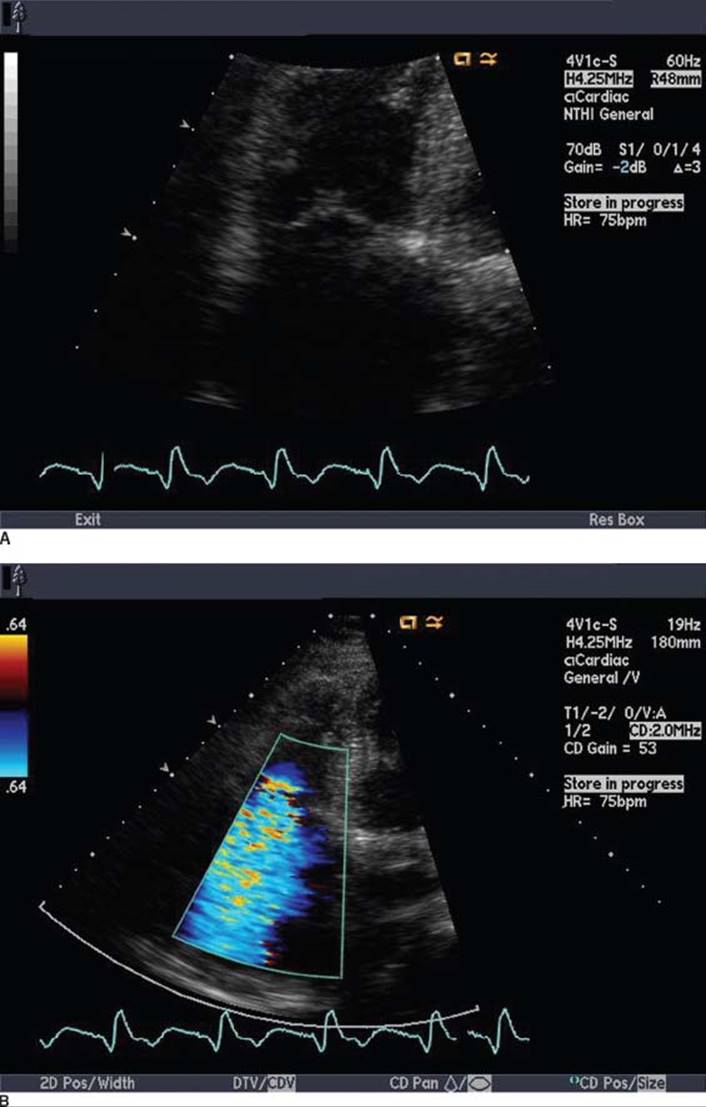
FIGURE 34.18 Transthoracic apical four-chamber systolic 2-D echo image (A) and color flow Doppler image (B) of a patient with severe TR due to apical tethering of tricuspid leaflets resulting from left-sided valve disease.
There are no specific ECG changes associated with TR; however, with severe pulmonary hypertension, the ECG pattern of RV hypertrophy may be seen. When right atrial enlargement is present, the ECG may show large P waves in the pattern “P pulmonale,” but in the chronic phase, most patients have AF. Chest x-ray often reveals cardiomegaly due to RV and right atrial enlargement, coupled with the findings that reflect their left-sided heart disease, if present.
Regarding etiology, the most common type of TR is termed “functional,” because it results from RV and tricuspid annular dilatation. Any cause of pulmonary hypertension may cause this type of TR, including left-sided heart failure due to LV dysfunction, MS or regurgitation, or less commonly, aortic valve disease. Functional TR also results from RV hypertension or enlargement caused by intrinsic pulmonary disease, primary pulmonary hypertension, pulmonic valve abnormalities, or left-to-right shunts. Right heart dilation also occurs directly as a result of various disorders of the RV myocardium, including RV infarction or dilated cardiomyopathy.
Regurgitation from intrinsic tricuspid valvular dysfunction is less common than functional TR. These etiologies include infective endocarditis, myxomatous degeneration (prolapse), rheumatic fever, congenital Ebstein anomaly, carcinoid syndrome, papillary muscle dysfunction or rupture, connective tissue disorders, trauma (including myocardial biopsy), rupture of chordae tendineae, marantic endocarditis, and endomyocardial fibrosis.
Treatment of TR involves correcting the primary cause. For example, if a correctable cause of acute or chronic pulmonary hypertension can be found, TR may improve or resolve. For example, diuresis of a patient in left heart failure may also diminish the severity of TR. Rhythm and rate control also are beneficial to patient well-being in appropriate patients. In some patients, vasodilator therapy may help by dilation of venous capacitance beds, or by reducing pulmonary arteriolar resistance.
Annuloplasty is the most frequent surgical treatment used for TR. However, when valve leaflets themselves are destroyed or diseased, a prosthesis is needed, and a biologic valve is usually used as there is a high prevalence of valve thrombosis with mechanical valves in the tricuspid position. The indications for tricuspid valve surgery are listed in Table 34.11. In patients with mitral valve dysfunction and TR requiring surgery,the improvement in pulmonary hypertension may relieve the RV dilation sufficient to correct the TR. However, there should be low threshold for annuloplasty; any patient with moderate 2+ TR or more on a scale of 4+ at any time prior to surgery may be a surgical candidate.
TABLE
34.11 Management of TR
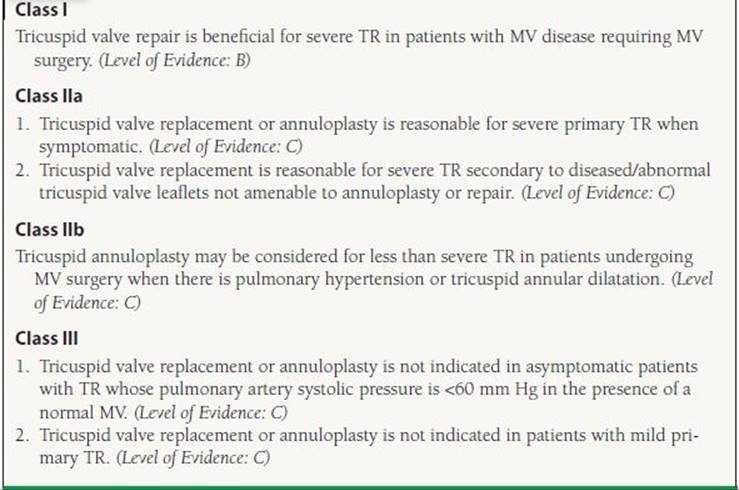
Adapted from Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–e148.
TRICUSPID VALVE STENOSIS
The primary cause of tricuspid valve stenosis (TS) is rheumatic heart disease and is almost always accompanied by severe TR. Stenosis is a consequence of chronic rheumatic fibrosis, as discussed above for MS, occurring for many years after the episode of acute rheumatic fever. It is almost never seen as an isolated valvular lesion and frequently presents later in the phase of rheumatic mitral and aortic valve disease. By the time TS is apparent, most patients have a long history of heart failure and most have already had mitral valve disease long enough to have had one or more cardiac surgical procedures, mostly on the mitral valve.
The symptoms and hemodynamic effects of TS are typically those of severe chronic right-sided congestive failure, and cannot be distinguished easily from those resulting from TR, and the frequent concomitant mitral and aortic valve dysfunction. Patients present with right-sided heart failure, with chronic and progressive symptoms of dyspnea, weakness, fatigue, edema, and anorexia. Common physical exam findings include elevated jugular venous pressure, a RV lift, ascites, peripheral edema, and a parasternal diastolic rumble. There is seldom a tricuspid OS. Electrocardiogram shows AF in most patients. The rare patient in sinus rhythm has abnormal P waves from left and right atrial enlargement. Chest x-ray often shows massive cardiomegaly, where the dilated right atrium is eclipsed by severe left atrial enlargement.
The findings by echocardiography include diastolic doming, thickening, and restricted motion of tricuspid leaflets (Fig. 34.19). Valve area and pressure gradients can be obtained by Doppler echocardiography, similar to MS, although the accuracy of these measurements is not as well validated.
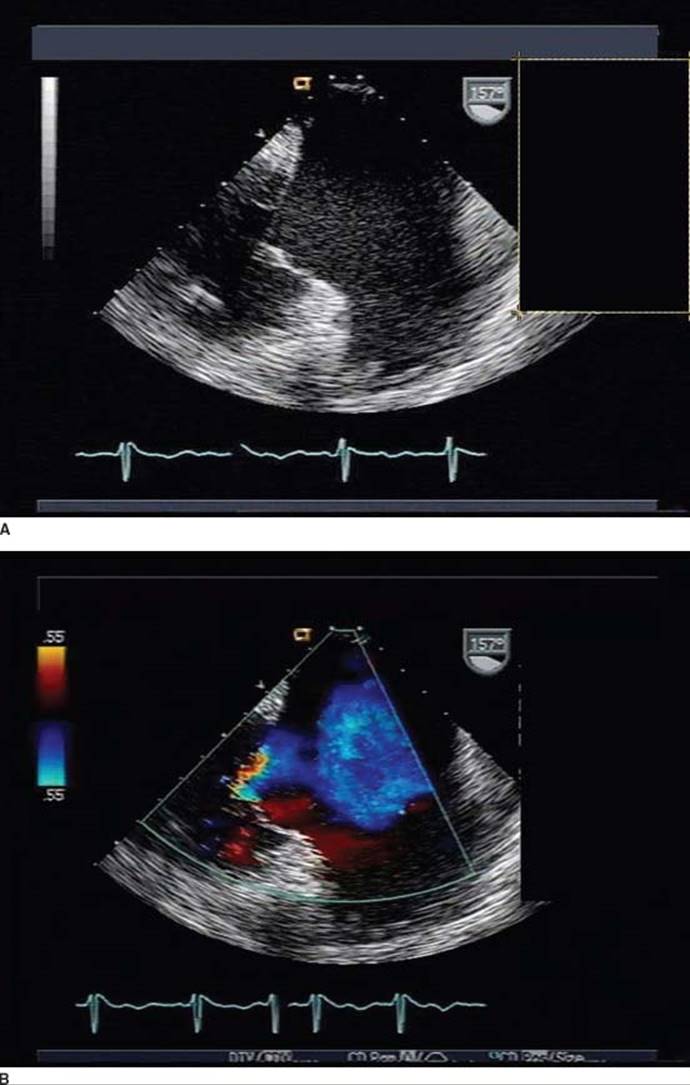
FIGURE 34.19 Midesophageal diastolic 2-D image (A) and color flow image (B) in a patient with severe rheumatic tricuspid stenosis, showing the diastolic doming, leaflet thickening, and restricted motion. The severely enlarged right atrium is shown. The patient was under evaluation for reoperation, with recurrence of right and left heart failure after three previous mitral valve operations.
Surgical correction is the mainstay of therapy, and this is clinically successful primarily when combined with mitral and/or aortic valve surgery. Correcting the tricuspid valve without fixing the left-sided problems may lead to pulmonary congestion and edema. Open or balloon valvotomy, especially to relieve the fusion at the commissure between the anterior and septal leaflets and between the posterior and septal leaflets, can relieve the stenosis, but the clinical results are often poor because of persistence of TR. Often tricuspid valve replacement, usually with a bioprosthesis, is necessary to treat the patient with significant TS–TR adequately.
REFERENCES
1. Bonow RO, Carabello BA, Chatterjee K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol. 2006;48:e1–e148.
2. Freed LA, Levy D, Levine RA, et al. Prevalence and clinical outcome of mitral-valve prolapse. N Engl J Med. 1999;341:1–7.
3. Avierinos JF, Gersh BJ, Melton LJ III, et al. Natural history of asymptomatic mitral valve prolapse in the community. Circulation. 2002;106:1355–1361.
4. Enriquez-Sarano M, Avierinos JF, Messika-Zeitoun D, et al. Quantitative determinants of the outcome of asymptomatic mitral regurgitation. N Engl J Med. 2005;352:875–883.
5. Bonow RO, Carabello BA, Chatterjee K, et al. 2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Valvular Heart Disease). J Am Coll Cardiol. 2008;52:e1–e142.
6. Wilson W Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116:1736–1754.
7. Cosgrove DM, Stewart WJ. Mitral valvuloplasty. Curr Probl Cardiol. 1989;14:359–415.
8. Stewart WJ, Currie PJ, Salcedo EE, et al. Evaluation of mitral leaflet motion by echocardiography and jet direction by Doppler color flow mapping to determine the mechanisms of mitral regurgitation. J Am Coll Cardiol. 1992;20:1353–1361.
9. Zoghbi WA, Enriquez-Sarano M, Foster E, et al. Recommendations for evaluation of the severity of native valvular regurgitation with two-dimensional and Doppler echocardiography. J Am Soc Echocardiogr. 2003;16:777–802.
10. Pu M, Vandervoort PM, Griffin BP, et al. Quantification of mitral regurgitation by the proximal convergence method using transesophageal echocardiography. Clinical validation of a geometric correction for proximal flow constraint. Circulation. 1995;92:2169–2177.
11. Pu M, Griffin BP, Vandervoort PM, et al. The value of assessing pulmonary venous flow velocity for predicting severity of mitral regurgitation: a quantitative assessment integrating left ventricular function. J Am Soc Echocardiogr. 1999;12:736–743.
12. Grigioni F, Enriquez-Sarano M, Ling LH, et al. Sudden death in mitral regurgitation due to flail leaflet. J Am Coll Cardiol. 1999;34:2078–2085.
13. Stewart WJ. Myocardial factor for timing of surgery in asymptomatic patients with mitral regurgitation. Am Heart J. 2003;146:5–8.
14. Leung DY, Griffin BP, Stewart WJ, et al. Left ventricular function after valve repair for chronic mitral regurgitation: predictive value of preoperative assessment of contractile reserve by exercise echocardiography. J Am Coll Cardiol. 1996;28(5):1198–1205.
15. Abascal VM, Wilkins GT, O’Shea JP, et al. Prediction of successful outcome in 130 patients undergoing percutaneous balloon mitral valvotomy. Circulation. 1990;82:448–456.
QUESTIONS AND ANSWERS
Questions
1. Mitral valve regurgitation is not associated with which of the following?
a. Heart failure
b. Atrial fibrillation (AF)
c. Stroke
d. Pulmonary hypertension
e. Increased pulse pressure
2. What is the effect of successful mitral regurgitation (MR) repair on left ventricular ejection fraction (LVEF)?
a. Stays the same
b. Goes up
c. Goes down
3. What level of instantaneous regurgitant orifice area (ROA) is the criterion for severe (4+) MR?
a. >60 mL
b. >0.4 cm2
c. >200 mL/s
d. >400 mm2
e. >0.6 cm2
4. What is the most common etiology of tricuspid regurgitation (TR)?
a. Rheumatic disease
b. Prolapse or flail
c. Trauma
d. Carcinoid
e. Left-sided heart failure
5. A 55-year-old man has posterior mitral valve prolapse (MVP) that was detected on a recent physical exam. His MR is anteriorly directed and his ROA measures 0.5 cm2 on proximal convergence method. He has an LVEF of 50%, normal pulmonary artery pressures, and can run 3 miles every other day without difficulty. He has never experienced AF to his knowledge. His left ventricular (LV) end systolic dimension is 4.2 cm and his LV end diastolic dimension is 6 cm. His left atrial diameter is 4.5 cm. What do you recommend now?
a. Watchful waiting with repeat echocardiogram in a year
b. Mitral valve replacement (MVR) with a bioprosthesis given his age
c. MVR with a mechanical valve given his age
d. Mitral valve repair within the next few months
e. Afterload reduction with an angiotensin-converting enzyme (ACE) inhibitor and careful monitoring of his LV function
6. A 70-year-old woman with long-standing mitral stenosis (MS) comes to see you. She claims that she is perfectly fine and can do all her activities of daily living. Her family who accompany her suggest that she has gradually reduced her activities and is now house bound. The valve is heavily calcified and her mean gradient across it is 6 mm Hg by echocardiography. There is 2+ MR. The pulmonary artery pressure is 50 mm Hg systolic. Her other valves are thickened but not stenotic. She has 3+ TR. She has long-standing AF that is rate controlled. She is taking coumadin, digoxin, and a beta-blocker. The next step in her evaluation is:
a. Start furosemide to reduce her filling pressures.
b. Do a stress echocardiogram to assess her functional capacity and change in valve gradients, regurgitation, and pulmonary pressures with stress.
c. Recommend cardiac catheterization to measure her intracardiac pressures invasively.
d. Perform transesophageal echocardiography (TEE) to better assess her MS.
e. Recommend balloon valvuloplasty now to improve her valve gradients.
7. A 45-year-old woman presents with increasing weight gain and abdominal fullness for a number of months. She sustained a motor vehicle accident about 6 months ago and had a major injury to her chest. She had made a reasonable recovery but is now limited. On examination, she is in normal sinus rhythm. Her venous pressure wave is prominent and elevated. She has a Grade 3/6 systolic murmur at the right sternal border. She has abdominal distention with hepatomegaly. She has 3+ pitting edema bilaterally. The most likely cause of her problems is:
a. Carcinoid syndrome with resultant severe TR
b. Right heart failure from respiratory insufficiency following her traumatic injury to the chest
c. Constrictive pericarditis consequent on her chest injury
d. Ischemic injury to the right coronary artery and ruptured papillary muscle to the tricuspid valve
e. Traumatic chordal rupture of tricuspid valve leaflet with severe TR
8. The following is true about tricuspid stenosis:
a. It often occurs as an isolated lesion independent of other valve involvement.
b. Balloon valvuloplasty is the treatment of choice in most situations.
c. If mitral valve disease is present, tricuspid stenosis is usually evident before mitral valve disease is manifest.
d. Is often accompanied by severe TR.
e. Often an audible opening snap (OS) is present over the tricuspid valve.
9. A 55-year-old woman has severe symptomatic MS and has a valve area of 0.8 cm2. She has 2+ MR, moderate aortic regurgitation (AR), and a splittability score of 11. She had an open commissurotomy in the past. Which of the following statements is most likely to be correct?
a. She should not undergo mitral balloon valvuloplasty as the degree of MR and splittability score are absolute contraindications to the procedure.
b. You tell her that balloon mitral valvuloplasty is unlikely to be successful because of her prior commissurotomy.
c. You tell her that balloon mitral valvuloplasty may be attempted but she is unlikely to have an optimal result based on her splittability score and her prior commissurotomy but may provide symptomatic relief.
d. You recommend watchful waiting as she will likely improve with an exercise program.
e. You tell her that her only option is MVR and that this will be a low-risk procedure with estimated mortality of <1%.
10. Which of the following statements with regard to MVP is true?
a. It is more common in women than in men.
b. It is best diagnosed from the apical four-chamber echocardiographic image plane.
c. Men are more likely to have significant complications including surgery on the mitral valve than women.
d. Leaflet thickening when present has no adverse effect.
e. Most patients with MVP will eventually progress to severe MR and need for surgery.
Answers
1. Answer E: AR is associated with increased pulse pressure due to the excess run-off of flow back into the LV in diastole. Prior to end-stage MR with secondary abnormalities, the cardiac output and forward stroke volume are normal. Arterial pressure is usually normal, and pulse pressure is normal. All the other choices are in some circumstances associated with MR, including the development of left atrial thrombi, often from concomitant AF, leading to systemic embolization.
2. Answer C: In a study by Leung et al.13 of 139 patients with isolated MR and no evidence of coronary artery disease, of whom 74 underwent uncomplicated valve repair, MR repair was associated with decreased LVEF and end-diastolic volume. However, end-systolic volume was preserved. This can be understood as relief of the chronic state of increased chronic excess stroke volume present when the MR is causing redundant mitral valve inflow, over LV outflow. In other words, chronic MR is often associated with an ejection fraction that overestimates true myocardial function.
3. Answer B: The following cut points have been established for severe MR when using proximal isovelocity surface area (PISA) to calculate instantaneous ROA:
<0.19 cm2 is mild
0.2 to 0.29 cm2 is moderate
0.3 to 0.39 cm2 is moderately severe
>0.4 cm2 is severe
4. Answer E: The most common etiology of TR is left-sided heart disease.
5. Answer D: He has severe MR with ROA > 0.5 cm2. He now has LV dysfunction as his LVEF is 50%. This should be at least 60% in someone with severe MR and normal LV function and is a Class I indication for surgical intervention. Mitral valve repair is favored over MVR in the treatment of MR when feasible as long-term outcomes are generally better and LV function is more likely to be preserved postoperatively with repair. Waiting further in this man may only cause his contractile function to deteriorate further. There is no evidence that afterload reduction or any other medical therapy will alter the natural history of MR. Either a mechanical or bioprosthetic valve might be reasonable choices in this individual if repair were not feasible.
6. Answer B: This lady has mixed MS and regurgitation and significant pulmonary hypertension. She has a heavily calcified mitral valve with moderate mitral gradients. The first thing to establish with her is how severely limited she is and whether the mitral valve is contributing to this. A stress echocardiogram will allow her functional capacity and her hemodynamic changes on exercise be determined. In some patients with mixed mitral valve disease, the MR may worsen on exercise and lead to a significant increase in the pulmonary artery pressures. TEE is useful in evaluating MR but planimetry of the mitral valve is often difficult with TEE. Cardiac catheterization is very useful in evaluating the hemodynamics of mitral valve disease but will not give an assessment as to how limited the patient is. This is crucial for decision making as to the best options for her.
7. Answer E: Traumatic injury to the tricuspid valve may occur following a motor vehicle accident and can present insidiously with severe TR and right heart failure. Surgical repair is usually feasible and curative.
8. Answer D: Tricuspid stenosis is relatively uncommon and is almost always seen in the setting of significant rheumatic mitral valve disease. It usually manifests late often with accompanying significant TR. Balloon valvuloplasty is feasible in some instances but is rarely considered because of concomitant severe TR.
9. Answer C: Balloon valvuloplasty is not contraindicated based on either the splittability score or a history of prior commissurotomy or 2+ MR. The results are less likely to be optimal in this situation but may afford symptomatic relief. It is unlikely that her symptoms will improve with exercise as she has critical MS. MVR will have a >1% risk given her prior surgical procedure.
10. Answer C: MVP is equally prevalent in men and women but men are more likely to have complications such as endocarditis and significant MR. In most patients, mitral prolapse is a benign condition and does not require surgery. Mitral valve thickening of > 5 mm— classic mitral prolapse- is more likely to have a complicated course. Mitral prolapse is best detected and diagnosed on the long-axis views and not the apical four-chamber echocardiographic view because the saddle shape of the mitral annulus may lead to apparent but factitious prolapse on the apical four-chamber view.