Matthew Cavender and Stephen G. Ellis
Despite tremendous advances in the care of patients with heart disease seen over the past 30 years, coronary artery disease remains the leading cause of mortality and morbidity in the world.1 With an international population that is increasingly affected by hypertension, diabetes, and obesity, the incidence of coronary artery disease will continue to affect large proportions of the world’s population.2Advances in the medical treatment of patients with coronary artery disease have improved outcomes over this period of time; however, the use of revascularization to prevent mortality, improve anginal symptoms, and increase exercise capacity remains a fundamental component in management in patients with ischemic heart disease.3-5
Revascularization strategies were initially limited to surgical procedures such as coronary artery bypass grafting (CABG). This paradigm began to shift in 1977 when Andreas Gruentzig performed the first percutaneous transluminal coronary angioplasty (PTCA) that successfully increased coronary blood flow previously limited by coronary atherosclerosis. Initial attempts at percutaneous revascularization were hindered by high rates of acute closure and restenosis of the treated lesions.6 With the development of more potent antiplatelet agents such as thienopyridines and the increased use of coronary stents (percutaneous coronary intervention [PCI]), these limitations have been reduced such that PCI is now the predominant form of coronary revascularization in the United States.7
As such, PCI has been the focus of some of the most important clinical trials in cardiology that have shaped clinical practice and defined the algorithms established in the American College of Cardiology/American Heart Association (ACC/AHA) guidelines.3-5 The current format of the cardiovascular board exam focuses approximately 25% of the content on the management of patients with coronary artery disease and acute myocardial infarction (MI). Revascularization strategies are an important component in the management of these problems. The constant evolution in both the management of patients with ischemic heart disease and the use of PCI makes it challenging to present from the perspective of the Cardiology Board exam, which is based mostly on the most current ACC/AHA guidelines, and thus lags current practice by a few years. In this chapter, we focus briefly on the techniques and complications of PCI while devoting increased attention to the ACC/AHA guidelines and major clinical trials evaluating the role of PCI in the management of patients with ischemic heart disease.
INDICATIONS AND APPROPRIATENESS OF PCI
ST-Elevation Myocardial Infarction
It is now well established that ST-elevation myocardial infarction (STEMI) occurs when an atherosclerotic plaque ruptures or erodes leading to thrombosis in an epicardial coronary artery. Initial attempts at restoring coronary flow utilized medications with fibrinolytic capabilities designed to breakdown the coronary thrombosis. These therapies, tested in numerous clinical trials (GUSTO, GISSI, ISIS-2, FTT), clearly showed that patients treated with reperfusion therapy had improved survival as compared to those patients treated with conservative management.8-11 Fibrinolytic therapy was hindered by its relatively high rates of intracranial hemorrhage leading to the search for improved revascularization techniques.12
Initial attempts to treat STEMI with percutaneous therapies were limited to balloon angioplasty (PTCA). Studies comparing primary PTCA to fibrinolytic therapy demonstrated less recurrent ischemia, reinfarction, reocclusion, and strokes in patients treated with primary PTCA. While the long-term mortality benefit of primary PTCA was not consistent in the various studies (GUSTO-2B, PAMI), a metaanalysis by Keeley et al. showed a 23% relative reduction in mortality (7% in PTCA vs. 9% in fibrinolytic; p = 0.0002) for PTCA compared to thrombolysis.13,14 Since these trials were conducted, additional therapies such as coronary stenting (which prevents acute vessel closure) and aspiration thrombectomy (removes clot from the coronary artery) have been developed and found to be beneficial in patients with STEMI.15 Studies have shown that the use of coronary stents in STEMI is more effective than PTCA alone in increasing postintervention lumen size and decreasing the risk of acute vessel closure, subsequent ischemic events, and repeat target vessels revascularization (GRAMI, FRESCO, stent-PAMI).16-18 There have been no studies demonstrating a survival benefit for stents compared to PTCA alone.
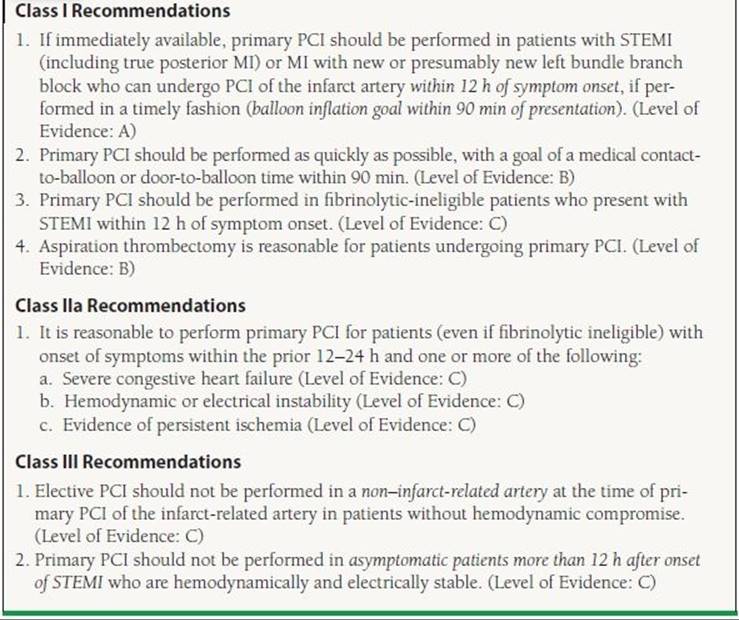
The superiority of PCI as compared to fibrinolytic therapy is reflected in the current ACC/AHA guidelines that support the use of primary PCI in patients with STEMI or chest pain and a new left bundle branch block in situations where it can be performed in a timely manner (door to balloon time of <90 minutes). The timing of symptom onset is an important component of the decision to pursue percutaneous revascularization. For patients with symptom onset within 12 hours of presentation, primary PCI is given a Class I indication. Patients with the onset of symptoms within 12 to 24 hours who have severe congestive heart failure, hemodynamic/electrical instability, or evidence of persistent ischemia (i.e., continued chest pain) are also candidates for percutaneous revascularization (Class IIa recommendation). Asymptomatic patients who present more than 12 hours after the onset of symptoms should not be treated with percutaneous revascularization (Class III recommendation) (Table 47.1).
TABLE
47.1 Recommendations for the Use of PCI in Patients with STEMI
Modified from the ACC/AHA guidelines: King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209; Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175; Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
PCI in Cardiogenic Shock
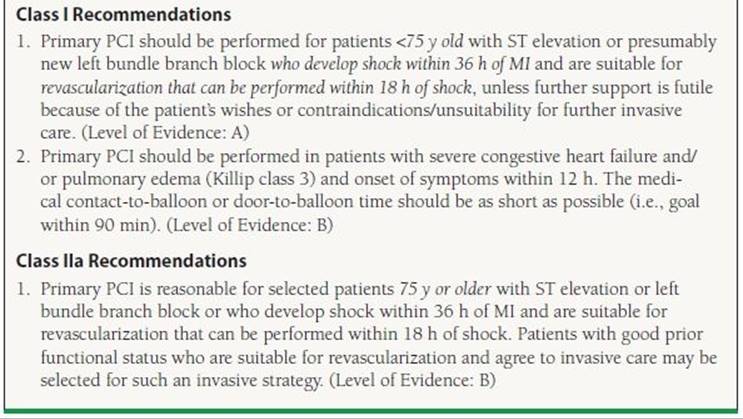
Approximately 5% of patients with STEMI have a significant decrease in cardiac output resulting in end-organ malperfusion. This condition, known as cardiogenic shock, is defined clinically by the presence of a systolic blood pressure <90 mm Hg lasting for more than 30 minutes (in the absence of hypovolemia) or vasopressors required to achieve a systolic blood pressure ≥90 mm Hg combined with a reduced cardiac index (1.8 L/min/m2) and evidence of an elevated left ventricular filling pressure (i.e., pulmonary capillary wedge pressure >18 mm Hg).19 Patients who develop cardiogenic shock are at increased risk of death with mortality rates ranging from 30% to 50%.20 The SHOCK trial was a landmark trial that serves as the basis for the current ACC/AHA recommendations for the treatment of patients in cardiogenic shock. This trial showed that revascularization performed within 36 hours from symptom onset was superior to initial medical stabilization with a lower mortality rates at 6 months (50% with PTCA vs. 63% with initial medical therapy, p = 0.027).21
Subset analysis from the SHOCK trial showed that patients ≥75 years old did not have the same benefit from revascularization raising questions as to whether patient revascularization should be pursued in the elderly. While subsequent observational and post hoc analysis have provided support for the use of revascularization in the elderly, this ambivalence is reflected in the current ACC/AHA guidelines (Table 47.2).22
TABLE
47.2 Recommendations for the Use of PCI in Patients with Cardiogenic Shock
Modified from the ACC/AHA guidelines: King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209; Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175; Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
Role of PCI in Patients Treated with Fibrinolytics
Not all hospitals are equipped with catheterization laboratories capable of performing emergent PCI in the setting of STEMI. As a result, some patients with STEMI may be treated with fibrinolytic therapy if transfer to a PCI hospital cannot be performed in a timely manner. Attempts to combine lower dose fibrinolytic therapies with PCI have largely been unsuccessful in improving outcomes. The FINESSE trial (Facilitated Intervention with Enhanced Reperfusion Speed to Stop Events) randomized patients with STEMI to facilitated PCI (half-dose fibrinolytics + abciximab), abciximab-facilitated PCI, or primary PCI.23 At 90 days, there was no difference in the primary endpoint (composite of death from all causes, ventricular fibrillation occurring more than 48 hours after randomization, cardiogenic shock, and congestive heart failure during the first 90 days after randomization). Based on this study, facilitated PCI (fibrinolytics as an intentional prelude to primary PCI) should not be performed.
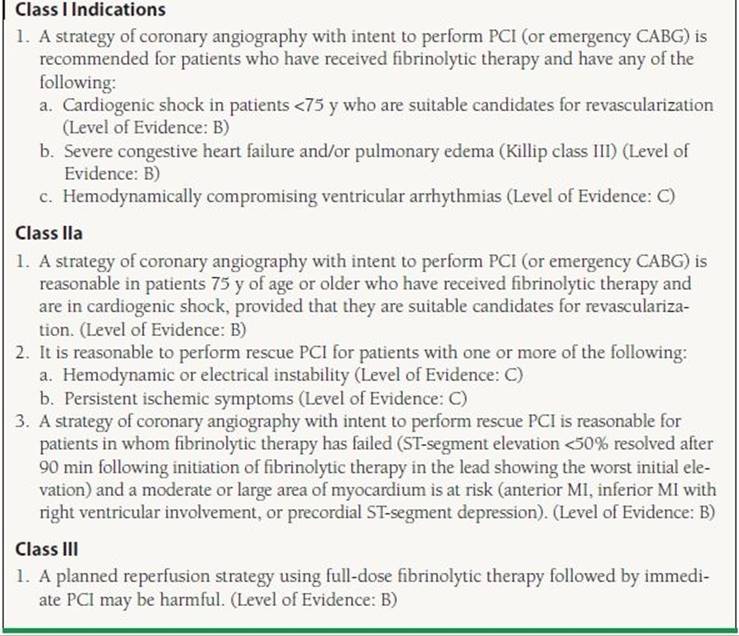
The lack of benefit for facilitated PCI does not imply that PCI does not have a role in the management of patients treated with fibrinolytic therapy. Up to 25% of patients treated with fibrinolytics will not achieve coronary reperfusion.24 Identifying this subset is important since patients with a patent infarct–related artery have improved clinical outcomes as compared to patients in which reperfusion is not successful. Continued chest pain and persistent ST elevations are typically considered markers of failed reperfusion; however, prior studies have found that approximately half of patients with persistent chest pain and ST elevations will actually have a patent infarct artery.24Despite this limitation, persistent ST elevation of >50% remains an indication for rescue PCI (PCI performed after failed fibrinolysis) due to the large benefit of rescue PCI shown in the REACT trial. The REACT trial randomized patients who did not have a >50% reduction in ST elevation to conservative therapy, repeat thrombolysis, or rescue PCI. At 6 months, patients treated with rescue PCI were significantly more likely to be free from death, reinfarction, stroke, or severe heart failure (adjusted hazard ratios of 0.43; p = 0.001 for rescue PCI vs. repeated thrombolysis).25 In addition to the ECG requirement, ACC/AHA guidelines also support immediate PCI following the administration of fibrinolytic therapy for patients with recurrent MI (Class I indication), moderate or severe ischemia (Class I indication), cardiogenic shock/hemodynamic instability (Class I indication), LVEF <40% (Class IIa indication), and serious ventricular arrhythmias (Class IIa indication) (Table 47.3).
TABLE
47.3 Recommendations for PCI After Failed Fibrinolysis (Rescue PCI)
Modified from the ACC/AHA guidelines: King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209; Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175; Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
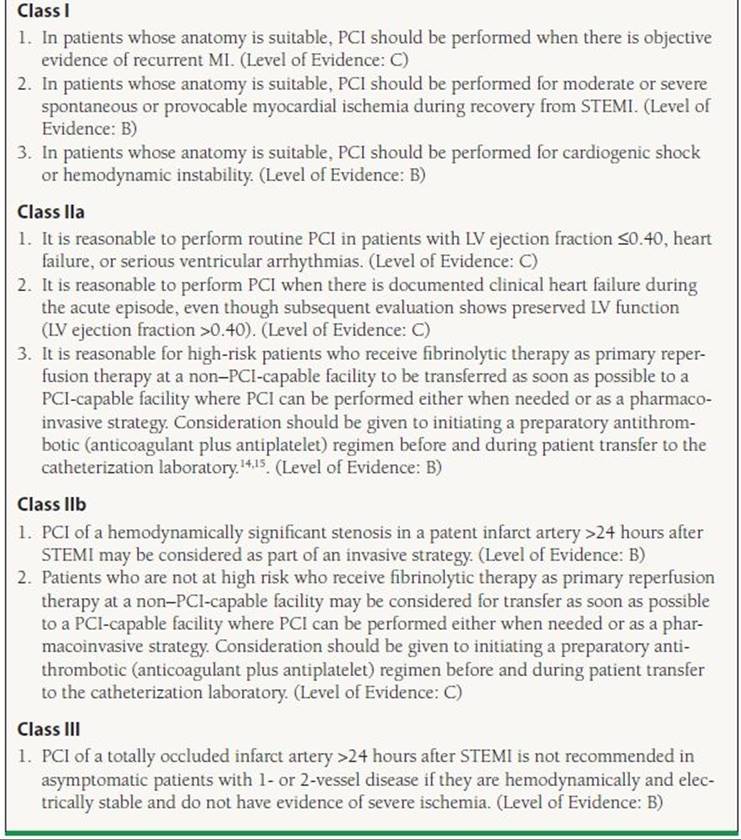
Patients should be transferred to a hospital with PCI capabilities after the administration of fibrinolytics due to the numerous potential indications for PCI. In patients with successful fibrinolysis who are asymptomatic, earlier trials that predated the routine use of clopidogrel and GP IIb/IIIa inhibitors showed no evidence that immediate PCI of the infarct-related artery provided any further reduction in death, reinfarction, or myocardial salvage (SWIFT and TIMI II). Other trials such as SIAM III, GARCIA-1, and CAPITAL-AMI showed significant reduction in mortality and ischemic events in those who underwent immediate PCI after successful fibrinolysis. A larger, definitive trial has also provided evidence of benefit. The TRANSFER-AMI study randomized patients to either standard treatment (including rescue PCI) or immediate transfer to another hospital for PCI within 6 hours after fibrinolysis.26 At 30 days, there was a significant decrease in the number of patients with death, reinfarction, recurrent ischemia, new or worsening congestive heart tailure, or cardiogenic shock (relative risk with early PCI, 0.64; p = 0.004).This has been further clarified with results of a meta-analysis by D’Souza et al., which showed that an early invasive PCI strategy following administration of fibrinolytic therapy results in a 53% reduction (odds ratio 0.47 [95% confidence interval (CI), 0.32-0.68, p <0.0001]) in a combined endpoint of 30-day mortality, reinfarction, and ischemia. The majority of the difference was in a significant reduction in both reinfarction and recurrent ischemia that 30-day mortality and major bleeding rates between strategies were not significantly different.27 While not yet reflected in the ACC/AHA guidelines, many providers now advocate routine angiography following the administration of fibrinolytic therapy; however, the optimal timing of PCI following the administration of fibrinolytic therapy remains unknown (Table 47.4).
TABLE
47.4 Recommendations for PCI After Successful Fibrinolysis or for Patients Not Undergoing Primary Reperfusion
Modified from the ACC/AHA guidelines: King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209; Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175; Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
Unstable Angina/Non–ST-Elevation Myocardial Infarction
The proportion of patients with high-risk unstable angina or non–ST-elevation acute coronary syndrome (NSTEMI) is increasing in the United States.28 Current ACC/AHA guidelines assume that patients with UA/NSTEMI are already on intensive medical therapy including aspirin, thienopyridine, antithrombotic (heparin, bivalirudin, etc.) beta-blockers, and statins. The role of revascularization in this population has been the focus of much attention and numerous clinical trials, including TIMI-IIIB, VANQWISH, FRISC II, TACTICS TIMI-18, RITA-3, and ICTUS. While there has been differences in the conclusions drawn from these studies, the bulk of the trials and a large meta-analysis support the use of an early invasive revascularization strategy (performance of diagnostic angiography with intent to perform revascularization within 48 hours of presentation).29 In patients with refractory angina or hemodynamic/electrical instability, revascularization should be performed in a semiemergent manner.30
While the early invasive strategy is preferred for patients who are suitable candidates for revascularization, the largest benefit comes from revascularization in patients considered to be high risk. Numerous risk prediction models, including the GRACE and PURSUIT risk scores, have been developed in order to guide the decision to refer to revascularization. The most well validated and widely used of these risk scores is the TIMI Risk Score that assigns patients one point for each of the following risk factors: age >65, known coronary artery disease (lesion >50%), three of more risk factors of coronary artery disease (tobacco abuse, family history, diabetes, hypertension, hyperlipidemia), aspirin use within 7 days, positive cardiac biomarkers, ST changes of >1 mm, and two or more episodes of chest pain within the past 24 hours. Patients with greater than two risk factors derive benefit from an early invasive strategy31 (Table 47.5).
TABLE
47.5 Risk Stratification in UA/NSTEMI
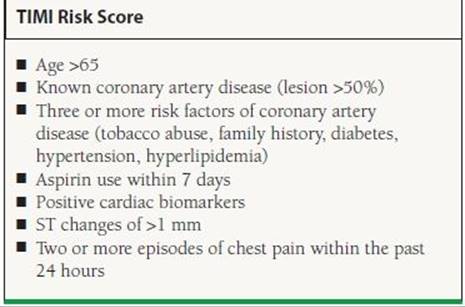
Adapted from Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. JAMA. 2000;284:835–842.
In patients who are stable, an initial conservative strategy may be considered even in high-risk patients if preferred by either patients or their physicians. While the guidelines support early catheterization for patients, this does not imply that all patients with UA/NSTEMI warrant revascularization. Revascularization is not indicated in patients with—one- to two-vessel CAD with either no symptoms or symptoms that are unlikely to be due to myocardial ischemia. In addition, revascularization is contraindicated in patients without high risk features who have only a small area of at-risk myocardium, lesions that have a low likelihood of revascularization, high risk of procedure-related morbidity/mortality, and stenosis of <50% or patients with left main CAD who are candidates for CABG (Table 47.6).
TABLE
47.6 Recommendations for PCI in Patients with UA/NSTEMI
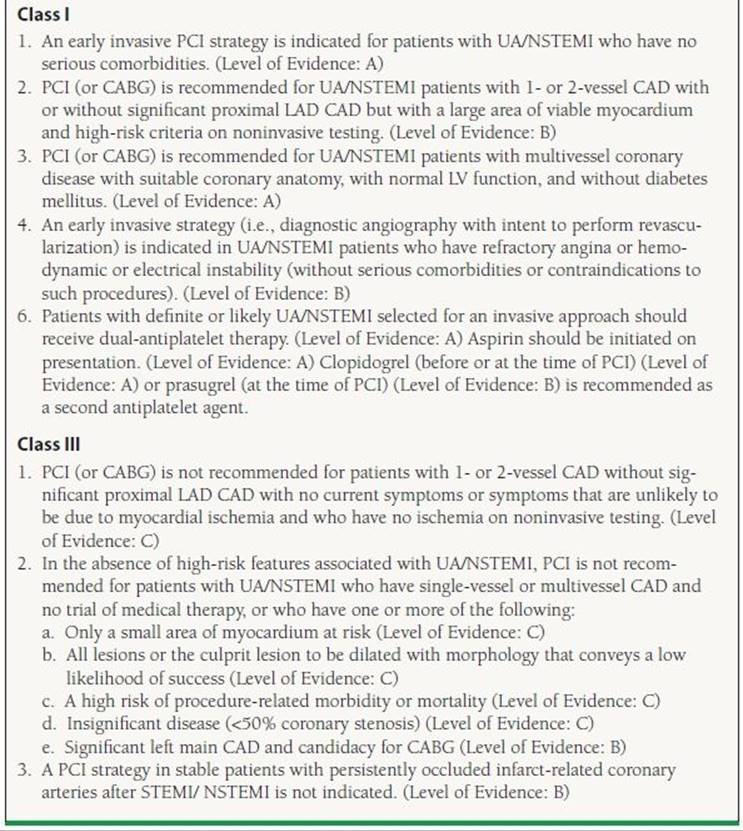
Modified from the ACC/AHA guidelines: King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209; Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175; Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
Stable Angina
Percutaneous revascularization was first utilized in patients with severe, chronic angina. In the current era, symptom relief from chronic stable angina remains the most frequent indication for revascularization. The decision to pursue medical therapy or revascularization is a highly individualized decision based on patient characteristics, symptoms, lifestyle, and preferences. The severity of angina is typically classified on the Canadian Cardiovascular Society Functional Classification of Angina Pectoris scale32 (Table 47.7).
TABLE
47.7 Canadian Cardiovascular Society Angina Pectoris Scale
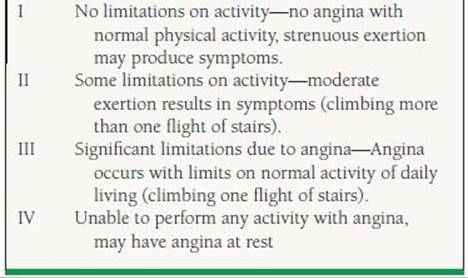
From Campeau L. Letter: grading of angina pectoris. Circulation. 1976;54:522–523, with permission from Wolters Kluwer Health.
There is a significant amount of clinical trial data comparing outcomes in patients treated with medical therapy versus revascularization. Numerous clinical trials and observational studies have been conducted in an attempt to understand the patient populations most likely to benefit from PCI. The RITA-II trial (Second Randomized Intervention Treatment of Angina) randomized 1,018 patients with angina to either PTCA (only 8% received stents) or medical therapy.33 After 2.7 years, death or definite MI occurred in 6.3% of patients treated with PCI, whereas these endpoints occurred in 3.3% of patients with medical care (p = 0.02). The difference between the two groups was primarily due to seven periprocedural nonfatal MIs in the revascularization group (which are of questionable significance). Revascularization did result in significant improvement in angina. There was a 16.5% absolute excess of moderate/severe angina in the patients treated with medical therapy. In addition, patients treated with revascularization have longer exercise times on the Bruce protocol. By 7 years, the incidence of death or MI was comparable in both groups.34
The ACIP trial (Asymptomatic Cardiac Ischemia Pilot) evaluated a slightly different population.35 Five hundred and fifty-eight patients with evidence of ischemia who underwent angiography and were found to have coronary artery disease amenable to revascularization were randomized with angina-guided medical therapy, ischemia-guided medical therapy, or revascularization with CABG or PTCA. After 2 years, the total mortality was 6.6% in the angina-guided group, 4.4% in the ischemia-guided group, and 1.1% in those receiving revascularization. These data suggested a benefit from initial revascularization compared to medical therapy in patients with demonstrable ischemia.
The most recent trial of medical therapy versus revascularization trial in patients with stable coronary artery disease was the COURAGE study (Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation).36This trial randomized 2,287 patients with coronary artery disease and evidence of ischemia to either PCI with optimal medical therapy (PCI group) or initial optimal medical therapy. Approximately one out of every three patients initially treated with medical therapy had a revascularization at some point during the follow-up period. After a median follow-up of 4.6 years, there was no difference in either all-cause mortality or nonfatal MI between the two groups. Relief from angina was significantly improved in patients treated with revascularization plus optimal medical therapy. This difference was attenuated over time possibly due to the significant number of patients in the initial medical therapy arm who eventually underwent revascularization. On the basis of this study, patients with stable angina can be treated initially with a trial of medical therapy with revascularization reserved for those patients with persistent angina.
It is possible that the use of functional assessment of coronary artery stenosis using either fractional flow reserve or stress imaging may provide an appropriate way of risk stratifying those patients most likely to benefit from revascularization instead of initial medical management. For example, a substudy of the COURAGE trial showed that patients with a >5% reduction in the amount of ischemia had improved outcomes, and PCI was more effective than medical therapy in reducing myocardial ischemia.37 This provides support for the use of ischemia-guided PCI; however, it remains unclear whether reduction of ischemia with PCI will improve clinical outcomes in patients with stable coronary artery disease.
The continuing improvements in outcomes with revascularization and the individuality of each patient’s symptoms and coronary anatomy make definitive conclusions about generalized patient populations challenging. It is apparent that patients with chronic stable angina have more effective relief of angina with percutaneous revascularization; however, it is likely that there is no difference between the two strategies in regard to the risk of MI, death, or need for future PCI and/or CABG. Patients with more severe angina and demonstrable ischemia on stress testing have a greater benefit in regard to relief of angina, while the effect on mortality remains debatable. As a result, a strategy of initial medical management in this population is both safe and effective.
Appropriateness criteria have been developed by the ACC/AHA to help guide the decision on which patients are likely to have the greatest benefit from revascularization.38 These criteria were developed largely from expert opinions based on the limited data available and the clinical experience of those involved in formulating the guidelines. For the purposes of the boards, these criteria do not need to be committed to memory but are a useful reference for making decisions regarding the decision to pursue revascularization. Factors considered in the development of the appropriateness criteria for revascularization include the location and extent of the coronary disease, severity of symptoms, extent of ischemia on stress testing, and use of medical therapy. Those patients with increased severity of coronary artery disease, larger area of ischemia, and more severe symptoms are those patients most likely to benefit from revascularization therapy. In contrast, those patients with minimal symptoms, small areas of ischemia, and less extensive coronary artery disease are those who are most likely to benefit from medical therapy with aspirin, antianginal medication (nitrates, beta-blockers, calcium channel blockers), and statins. Revascularization is also often considered in patients with ischemic heart disease prior to planned surgery. There is no evidence that prophylactic revascularization improves outcomes as compared to medical therapy with aspirin, beta-blockers, and statins. As a result, revascularization should only be considered for patients if they meet an indication for revascularization irrespective of their planned surgery.39
The revascularization options for patients with stable angina include both CABG and PCI. The landmark BARI (Bypass Angioplasty Revascularization Investigation) trial randomized 1,829 patients with multivessel coronary artery disease (patients with left main disease were excluded) to either PTCA (prior to the use of stents) or CABG. There was no difference in survival between the two groups at 5 years; however, post hoc analysis showed that patients with diabetes had a 15% absolute reduction in mortality when undergoing CABG.40 Based on the results of BARI, surgical therapy has historically been the preferred method of revascularization in patients with diabetes or three-vessel coronary artery disease.
The SYNTAX (Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery) trial was designed to provide contemporary data to guide the type of revascularization for patients with severe coronary artery disease.41 This contemporary trial differed from the BARI trial by including patients with left main disease and/or three-vessel coronary artery disease and randomizing them to either CABG or complete revascularization with drug-eluting stents. In addition, the SYNTAX trial utilized a team approach that included both an interventional cardiologist and a cardiac surgeon to determine whether patients were a candidate for both percutaneous revascularization and CABG. This team calculated a SYNTAX score which takes into account calcification, tortuosity, and length for every stenosis >50% found in vessels more than 1.5 mm in diameter. The SYNTAX score, if used by trained personnel, can be a reproducible score that allows for direct comparison of the severity of coronary artery disease between patients (SYNTAX score <22 = low risk, 23 to 32 = intermediate risk, ≥33 = high risk). In the 4,337 patients randomized, there was no difference in all-cause mortality, stroke, or MI at 1 year between the two groups (PCI 7.7% vs. CABG 7.6%, p = 0.99); however, the primary endpoint that added repeat revascularization to the three other endpoints occurred more frequently in the patients treated with PCI (17.8% vs. 12.4%, p = 0.002). Post hoc analysis at 4 years showed that patients treated with CABG had lower cardiovascular mortality when compared to patients treated with PCI (4.3% vs. 7.6%, p = 0.004) although the validity of this finding is uncertain given the difference in the numbers of patients lost to follow-up seen between the two arms (CABG arm had more patients lost to follow-up). These results largely coincided with smaller randomized clinical trials that evaluated PCI with bare metal stents to CABG which suggested that there is no mortality benefit provided by PCI over CABG [ARTS-I (Arterial Revascularization Therapies Study Part I), MASS-II (Medicine, Angioplasty, or Surgery Study for Multivessel Coronary Artery Disease), ERACI-II (Argentine Randomized Study of Coronary Angioplasty with Stenting versus Coronary Bypass Surgery in Patients with Multiple Vessel Disease), and AWESOME (Angina with Extremely Serious Operative Mortality Evaluation)]. Patients with more severe coronary artery disease are likely to see lower rates of repeat revascularization after CABG; however, those patients with isolated left main disease and/or low SYNTAX score have improved outcomes with percutaneous revascularization.
In summary, CABG has previously been the preferred method of revascularization for patients with three-vessel coronary artery disease and LV dysfunction, left main disease, or diabetes and multivessel disease. With the potential exception of patients with diabetes, there has been no definitive mortality difference between the two types of revascularization. Patients undergoing CABG are at increased risk of perioperative stroke, while patients undergoing PCI are at increased risk of restenosis and the need for repeat revascularization. Drug-eluting stents have been successful in decreasing the rates of restenosis allowing for the percutaneous revascularization of the left main artery and patients with three-vessel coronary artery disease; however, the use of drug-eluting stents remains associated with higher rates of repeat revascularization. CABG provides the most enduring revascularization for patients with the most extensive coronary artery disease (SYNTAX > 22) (Table 47.8).
TABLE
47.8 ACC/AHA Appropriateness Criteria for the Selection Of PCI or CABG in Patients with Severe Coronary Artery Disease
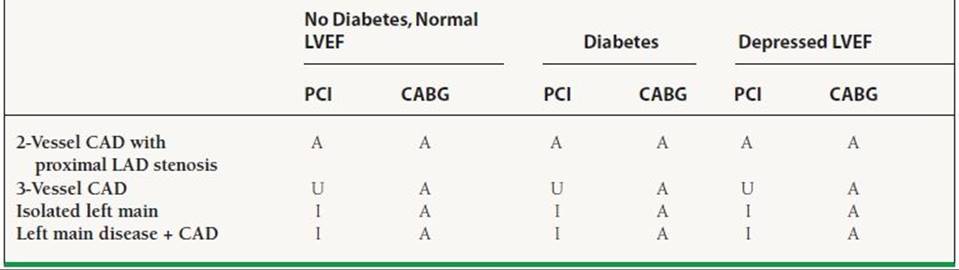
A, Appropriate; U, Appropriateness uncertain; I, Inappropriate.
Modified from Patel MR, Dehmer GJ, Hirshfeld JW, et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: a report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2009;53:530–553..
Patients Who Are Undergoing PCI Post-CABG
Patients who undergo CABG are still at risk of ischemia due to either graft occlusion or the progression of disease in the native vessels. Considering that repeat CABG carries a higher risk (approximately two times the risk of mortality in an otherwise low-risk patient), a post-CABG patient with recurrent ischemia may require PCI procedures to the grafts or the native vessels. The timing of ischemia following CABG offers insight into the etiology of the ischemia and the appropriateness for PCI in the management of this population. Ischemia within 30 days (very early ischemia) is usually secondary to graft failure from thrombosis or native vessel disease that was not supplied by the coronary bypass grafts. Ischemia occurring 30 days to 1 year following CABG is usually secondary to perianastomotic graft stenosis (early ischemia). Ischemia occurring >1 year after CABG (late ischemia) is usually secondary to disease progression in the grafts and/or native coronary vessels. PCI may be used to recanalize thrombosed vessels, dilate anastomotic points, or balloon or stent native vessels or grafts. It is important to keep in mind that the choice of PCI versus redo CABG in patients with recurrent ischemia depends on multiple factors including the potential graft conduits (arterial vs. venous), the number of grafts required and how many are occluded, the location of recurrent disease (in native vessels vs. grafts), LV function, and associated comorbidities.
ADJUNCT THERAPY FOR PCI
Antiplatelet Therapies
Aspirin/Thienopyridines
Early efforts at coronary stenting were hindered by high rates of stent thrombosis following PCI. Aspirin and thienopyridine have become the standard antiplatelet regimen used after PCI to prevent stent thrombosis after the conclusion of the STARS trial (Stent Anticoagulation Restonosis Study).42 The STARS trial randomized 1,653 patients with recent stent implantation to aspirin only, aspirin plus ticlopidine, or aspirin plus warfarin. At 30 days, only 0.5% of patients treated with aspirin and ticlopidine had the primary endpoint (death, MI, revascularization of the target lesion, and angiographically evident stent thrombosis) that was significantly less than both aspirin alone (3.6%) and aspirin plus warfarin (2.6%). The use of ticlopidine in clinical care was hindered by its side effect profile that included both neutropenia and thrombotic thrombocytopenic purpura. As a result, clopidogrel, which has a lower incidence of these side effects, has become the most used thienopyridine.43 The efficacy of clopidogrel in patients treated with PCI has been tested and shown to be effective in multiple studies. The CREDO (Clopidogrel for the Reduction of Events during Observation) trial randomized 2,116 patients undergoing PCI with bare metal stenting to either clopidogrel load with continued therapy for 1 year or clopidogrel after PCI with continued therapy for 28 days. Those patients treated with long-term clopidogrel had a 27% relative risk reduction in death, MI, or stroke at 1 year.44
Prasugrel is a new thienopyridine that has a faster onset and more potent antiplatelet effects than clopidogrel.45 It was approved for use in patients with acute coronary syndrome based on the results of the TRITON TIMI-38 trial.46 TRITON randomized 13,608 patients with acute coronary syndrome undergoing PCI to standard therapy with clopidogrel (300-mg loading dose and long-term treatment with 75 mg/d) or prasugrel (60-mg loading dose and long-term treatment with 10 mg/d). After a follow-up that ranged between 6 and 15 months, cardiovascular mortality, nonfatal MI, and nonfatal stroke were significantly lower in the group treated with prasugrel (hazard ratio for prasugrel vs. clopidogrel, 0.81; p < 0.001). There were some significant safety concerns that have limited the widespread adoption of this agent. Patients treated with prasugrel had a significant increase in bleeding (hazard ratio, 1.32; 95% CI, 1.03 to 1.68; p = 0.03) and patients with prior transient ischemic attack/cerebral vascular accident (TIA/CVA) had worse outcomes when treated with prasugrel. Also, patients older than 75 years and <60 kg did not appear to benefit from increased platelet inhibition. Based on this subgroup analysis, prasugrel is contraindicated in patients with prior TIA/CVA, age >75 years old, or <60 kg due to the increased bleeding risk.
Ticagrelor is a newly approved antiplatelet agent that is a direct and reversible inhibitor of the P2Y12 receptor. The half-life of the drug is 12 hours and as a result is given twice daily. The largest study of ticagrelor is the Study of Platelet Inhibition and Patient Outcomes (PLATO).47 The PLATO study randomized 18,624 patients with ACS to either ticagrelor (180-mg loading dose and then 90 mg twice daily) or clopidogrel (300- to 600-mg loading dose and then 75 mg daily). After 12 months, death from vascular causes, MI, or stroke was less common in the patients treated with ticagrelor (HR 0.84, p < 0.001).48While the overall outcomes favored ticagrelor, there are some safety concerns. Among patients not undergoing CABG, bleeding rates were higher in patients treated with ticagrelor (4.5% vs. 3.8%, p = 0.03). In addition, a post hoc analysis demonstrated that patients randomized from the United States had worse outcomes with ticagrelor.49 It is unclear whether this is due to statistical chance or that patients in the United States were more likely to be on higher doses of aspirin. In summary, ticagrelor is an agent with antiplatelet effects that are reversible and have a short half-life. Given the potential interaction between high-dose aspirin and outcomes, ticagrelor should only be used in conjunction with low doses of aspirin.
The dosing and duration of dual antiplatelet therapy (DAPT) have changed over time. Current guidelines recommend that patients not already taking daily chronic aspirin therapy should be given 300 to 325 mg of aspirin before the PCI with long-term therapy at a dose between 75 mg and 325 mg/d. Further insight into the most appropriated aspirin dose has been provided with the CURRENT OASIS-7 trial. This trial randomized patients with ACS treated with an early invasive strategy in a two-by-two factorial design to low- versus high-dose aspirin and low- versus high-dose clopidgrel.50 At 30 days, there was no difference in the primary endpoint of cardiovascular death, MI, or stroke. Given the higher bleeding rates seen with higher doses of aspirin, it is reasonable to treat patients with the lowest available aspirin dose.51 Current ACC/AHA guidelines do not yet reflect the results of this trial. Despite concurrent thienopyridine, aspirin remains necessary for patients treated with PCI. Among patients with aspirin sensitivity, desensitization can be considered; however, thienopyridines alone are more frequently utilized.
The duration of clopidogrel treatment after PCI is also subject to some debate. Originally, it was recommended that patients treated with bare metal stent be treated for at least 4 weeks, while patients treated with drug-eluting stents be treated for 3 to 6 months depending on the type of stent. Over time, it became apparent that there was a small but significant incidence of late stent thrombosis in patients treated with drug-eluting stents.52 This was attributed to the lack of endothelialization caused by the medications on the stent designed to inhibit restenosis. Current guidelines support the use of DAPT for at least 12 months; however, there will be no definitive answer regarding the optimal duration of DAPT therapy until the completion of the ongoing DAPT Study (Dual Antiplatelet Therapy Study).53 This trial is enrolling patients treated with drug-eluting stents who will then be treated for 12 months with DAPT. After 12 months, patients will be randomized to either placebo (thereby completing DAPT) or an additional 18 months of DAPT (long- term DAPT). Scheduled for completion in December 2013, this trial will provide evidence that will be helpful in determining whether long-term DAPT past 1 year is necessary (Table 47.9).
TABLE
47.9 Recommendations for Adjunctive Antiplatelet Therapies in PCI
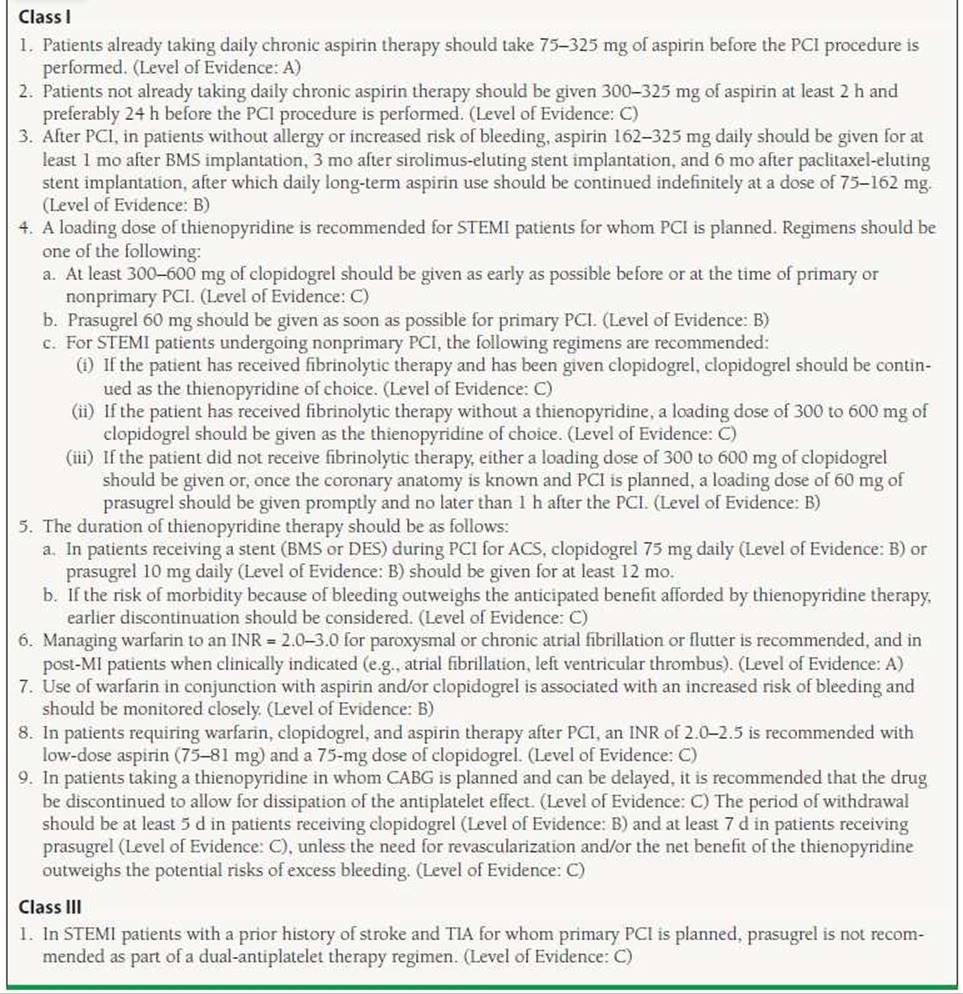
Adapted from the ACC/AHA guidelines: King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209; Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175; Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
Glycoprotein Ilb/IIIa Inhibitors
Thrombosis of the coronary artery is mediated by platelet aggregation and linkage via glycoprotein IIb/IIIa (GP IIb/IIIa) receptors. Commercially available GP IIb/IIIa inhibitors (abciximab, eptifibatide, and tirofiban) prevent platelet aggregation by blocking fibrinogen from binding to these receptors.54 Abciximab is a chimeric monoclonal antibody that binds nonspecifically to the GP IIb/IIIa receptor causing an irreversible inhibition. Eptifibatide is a cyclic heptapeptide with a lysine–glycine–aspartic acid (KGD) sequence that binds selectively to the GP IIb/IIIa receptor. Tirofiban hydrochloride is a nonpeptide derivative of tyrosine that binds selectively to the GP IIb/IIIa receptor. While these agents have similar actions, they differ in their modes of action, costs, and indications for use.
The majority of evidence for the efficacy of GP IIb/IIIa inhibitors was derived in anera that predated the routine use of DAPT. As a result, there are little data from the modern era in which GP IIb/IIIa inhibitors have been found to be effective. The EARLY-ACS (Early GP IIb/IIIa Inhibition in Non–ST-Segment Elevation Acute Coronary Syndrome) study randomized 9,492 patients with high-risk NSTEMI (had two or more of the following features: ischemic changes on electrocardiography, elevated cardiac biomarkers, and age >60 years) to either early, routine administration of eptifibatide or early administration of placebo with delayed, provisional administration of eptifibatide.55 Only 39% of the patients in the delayed/provisional arm received eptifibatide, yet there was no difference in the primary endpoint of all-cause mortality, MI, recurrent ischemia requiring urgent revascularization, or thrombotic bailout at 96 hours (9.3% in early treatment group versus 10% in delayed treatment group; odds ratio 0.92; 95% CI 0.80 to 1.06; p = 0.23). These data correspond with recent contemporary clinical trials such as ON-TIME2 (no significant difference in death, recurrent MI, or urgent target vessel revascularization at 30 days in highdose tirofiban group), HORIZONS-AMI (major bleeding and adverse events were higher in the group randomized to GP IIb/IIIa as compared to bivalirudin), FINESSE (no benefit with prehospital abciximab before primary PCI, either by itself or in combination with fibrinolytic therapy), and a meta-analysis (22 trials in patients undergoing elective PCI with DAPT who received GP IIb/IIIa inhibitors) that showed no effect of GP IIb/IIIa inhibitors in mortality.23,56–58 Based on these results, ACC/AHA guidelines conclude that the use of GP IIb/IIIa inhibitors before primary PCI is of uncertain benefit. Therefore, the use of GP IIb/IIIa inhibitors can be considered in selective cases such as in patients with significant thrombus or those in whom DAPT has not been initiated; however, the routine use of GP IIb/IIIa inhibitors is not recommended (Table 47.10).
TABLE
47.10 Recommendations for the Use of GP IIb/IIIa
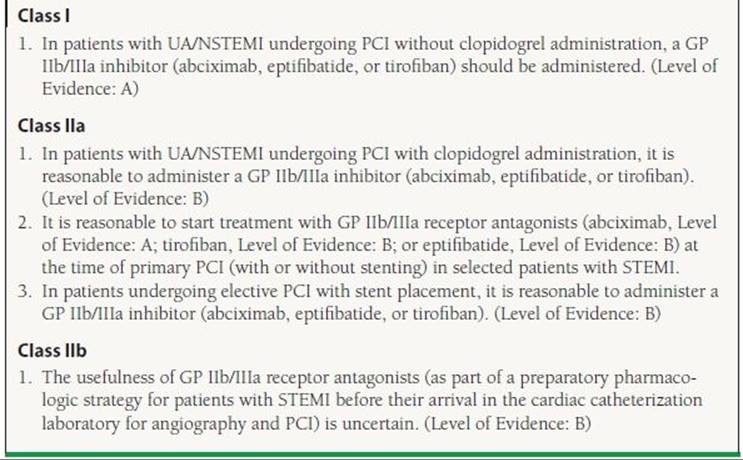
Adapted from the ACC/AHA guidelines: King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guidel0069ne update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol. 2008;51:172–209; Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175; Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
Antithrombin Therapies
Heparin Agents
Antithrombotic agents block the coagulation cascade and are necessary when performing coronary interventions in order to prevent coronary artery thrombosis. Unfractionated heparin (UFH) was the first agent utilized for this purpose. High doses of heparin with intravenous boluses of 100 IU/kg to maintain an activated clotting time (ACT) of 250 to 350 seconds have been used in the past. With improved interventional technology and accumulation of clinical experience, it has been possible to reduce the dose of intravenous UFH to 60 IU/kg plus an infusion of 12 IU/kg/h with a goal PTT of 50 to 70 (ACT of 200 to 250 seconds) in an attempt to reduce bleeding complications.59 It is necessary to monitor the degree of anticoagulation because heparin binds strongly to plasma proteins resulting in unpredictable levels of antithrombotic effects.
Enoxaparin is a low-molecular-weight heparin that inhibits factor Xa. Administration of enoxaparin gives more consistent plasma levels resulting in a more predictable degree on anticoagulation and does not require routine monitoring. The lack of routine monitoring caused some concern among interventionalists leading to low utilization rates while performing PCI. Due to the evidence of its effectiveness in patients with acute coronary syndromes, it is increasingly utilized in clinical practice (especially for patients with NSTEMI).60 For patients undergoing PCI, 1 mg of enoxaparin per kilogram should be administered subcutaneously twice a day before angiography. If the most recent subcutaneous dose has been given more than 8 hours earlier, an intravenous bolus of an additional 0.3 mg/kg should be given. An additional intravenous bolus of 0.75 mg/kg should be administered before PCI if the most recent subcutaneous dose has been >16 hours prior. Both approaches appear to be safe and efficacious in patients with ACS, although a concern remains about increased bleeding rates with LMWH use. Additionally, UFH is effectively reversed with protamine, whereas LMWH is only partially reversed. Currently there is no evidence to support a preference for LMWH over UFH.
Bivalirudin
Bivalirudin is a direct thrombin inhibitor and has been suggested as a replacement for UFH because it causes significantly less bleeding when compared with heparin alone in stable patients undergoing PCI, NSTEMI, and STEMI. The ACUITY trial randomized 13,819 patients to UFH or enoxaparin plus a GP IIb/IIIa inhibitor, bivalirudin plus a GP IIb/IIIa inhibitor, or bivalirudin alone.59 There was no difference in a composite endpoint of death, MI, and unplanned revascularization for ischemia between patients treated with bivalirudin and UFH or enoxaparin plus a GP IIb/IIIa inhibitor (7.8% and 7.3%, respectively; p = 0.32). Patients treated with bivalirudin had significantly lower rates of major bleeding (3.0% vs. 5.7%; p < 0.001). Similar results in patients with STEMI undergoing PCI were shown in the HORIZONS-AMI trial.57 The reduction in hemorrhagic complications, cost savings, and ease of administration have established bivalirudin plus provisional GP IIb/IIIa inhibition as an attractive antithrombotic strategy for patients undergoing elective or urgent PCI.
COMPLICATIONS
Improved equipment and increased operator experience have improved PCI outcomes and decreased the risk of complications. In the early days of interventional cardiology, cardiac surgery backup was required given the high rates of acute vessel closure; however, PCI is now routinely performed without cardiac surgery backup. Despite these improvements, complications including cath lab deaths are still seen. The latest statistics from a national quality improvement database report an overall unadjusted mortality rate for PCI of 1.3%.61 The risk of mortality varies depending on the characteristics of the patients: older patients, women, and patients with diabetes having increased risk associated with PCI.62 The mortality rate also varies depending on the indication with the mortality rate of elective PCI being 0.4% to 0.7% while the mortality rate of ST-elevation MI is 4.8%. In order to better quantify risk, PCI risk scores have been developed by investigators from the NCDR CathPCI database and Mayo Clinic that are able to provide some idea of preprocedural risk61,63 (Table 47.11).
TABLE
47.11 Predictors of Mortality in Patients Undergoing PCI Used in Risk Prediction Models
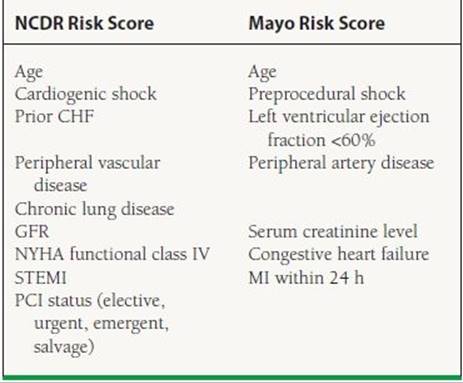
Adapted from Peterson ED, Dai D, DeLong ER, et al. Contemporary mortality risk prediction for percutaneous coronary intervention: results from 588,398 procedures in the National Cardiovascular Data Registry. J Am Coll Cardiol. 2010;55:1923–1932; Singh M, Rihal CS, Lennon RJ, et al. Bedside estimation of risk from percutaneous coronary intervention: the new Mayo Clinic risk scores. Mayo Clin Proc. 2007;82:701–708.
Renal Failure
Invasive procedures utilizing contrast dye are associated with the development of renal dysfunction, known as contrast-induced nephropathy (CIN). CIN is most commonly defined as a rise in creatinine by >0.5 mg/dL or a 25% increase from the baseline creatinine. CIN is typically classically described as nonoliguric renal dysfunction; however, oliguria can occur in patients with CIN. The pathophysiology of CIN is not well understood but vasoconstriction and injury to the renal tubules have been proposed as possible explanations.
The incidence of CIN is variable but averages around 12%.64 This risk is dependent upon both patient and procedural characteristics (Table 47.12). Advanced age, large volumes of contrast dye, cardiogenic shock, and advanced chronic kidney disease have been found to be some of the strongest predictors.65 The increase in creatinine seen with CIN typically is not seen until 48 hours after angiography, peaks at 5 days postcatheterization, and returns to h1 by days 7 to 10. Patients with CIN typically do not require hemodialysis (incidence is <1%), although the risk of hemodialysis is increased among patients who are at highest risk of developing CIN and receive large amounts of contrast dye.
TABLE
47.12 Risk Factors for the Development of CIN
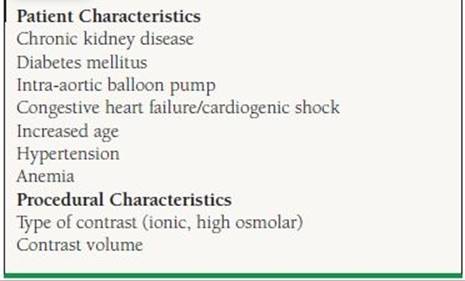
Modified from Pannu N, Wiebe N, Tonelli M. Prophylaxis strategies for contrast-induced nephropathy. JAMA. 2006;295:2765–2779.
The development of CIN is associated with increased hospital length of stay and is a predictor of long-term mortality in patients undergoing primary PCI. As such, there has been considerable effort placed in exploring strategies to reduce the incidence of CIN. To date, hydration prior to catheterization is the only therapy with convincing evidence of efficacy. There has been some indication that N-acetylcysteine (Muco-myst) may provide benefit; however, the studies examining its use have provided contradictory results. In addition, the majority of these studies have been limited with one or more significant limitations such as small sample size, inadequate controls, etc.65 The ACT trial (Acetylcysteine for Contrast-Induced Nephropathy Trial) provides strong evidence against its efficacy. In this study, 2,308 patients were randomized to N-acetylcysteine or placebo and there were no differences in the incidence of CIN or serum creatinine elevation seen between the two groups.66 As such, N-acetylcysteine is not recommended for routine use in the prevention of CIN. In patients at high risk of developing CIN, attempts should be made to provide adequate hydration prior to catheterization and minimize the amount of contrast dye used during the procedures. There is some evidence that selection of contrast material may alter the rate of CIN (see below).
Bleeding
Bleeding is a common complication from PCI that is associated with increased patient discomfort, length of stay, cost, and risk of mortality (both short and long term).67 While the mechanism linking bleeding with an increased risk of mortality is not well understood, it has been identified in multiple studies.68,69 The mechanisms for the association of bleeding complications with mortality are likely multifactorial and include the physiology effects of hemorrhage, decreased medication use/adherence after bleeding events, deleterious effects of anemia/red blood cell transfusions, and the increased comorbidities seen in patients who develop bleeding complications.70–72 Regardless of the etiology, the OASIS-5 and HORIZONS-AMI trials evaluating therapies for the treatment of acute coronary syndrome found that mortality could be decreased through a reduction in the incidence of bleeding. As such, the development of strategies that reduce the incidence of bleeding may improve the outcomes of patients undergoing PCI. The increased emphasis on comparing bleeding risk among PCI strategies and techniques has also led to the development of a standardized bleeding definition that should improve the ability to perform comparative effectiveness research.73,74
The incidence of bleeding varies depending on the patient population being studied and the definition used for bleeding. Registries following patients with NSTEMI have found bleeding rates as high as 9% to 12%, while patients undergoing elective PCI have considerably lower risk of bleeding. This illustrates that the characteristics of both the patient and the procedural determine the risk of bleeding. Female sex, baseline anemia, renal dysfunction, diabetes, and the use of GP IIb/IIIa inhibitors, large sheaths, femoral access and intra-aortic balloon pumps have been consistently identified as risk factors associated with increased bleeding complications (Table 47.13).
TABLE
47.13 Factors Associated with Bleeding in Selected Non–St-Elevation ACS
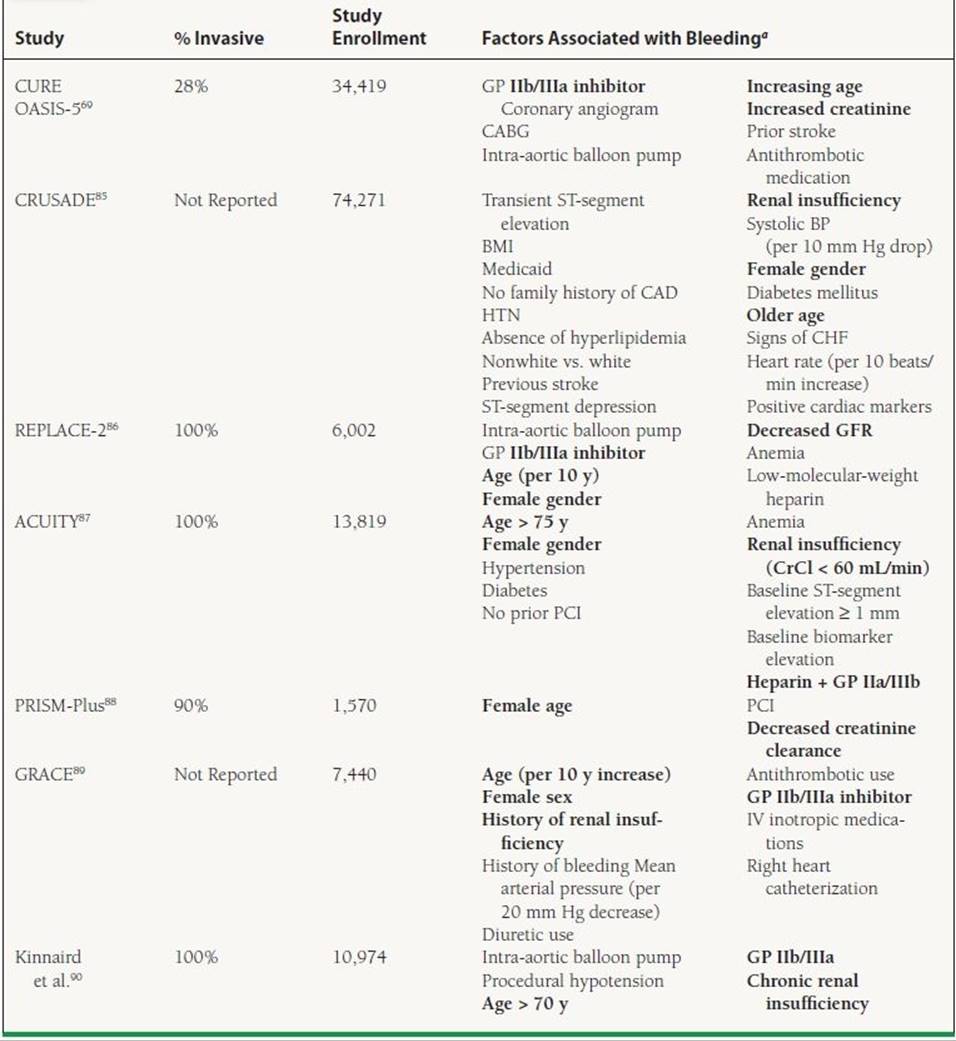
aPatient characteristics in bold are those found consistently through the majority of studies.
Modified from Cavender MA, Rao SV Ohman EM. Major bleeding: management and risk reduction in acute coronary syndromes. Exp Opin Pharmacother. 2008;9:1869–1883.
The majority of early bleeding events are related to vascular access and hemostasis. Over time, the risk of vascular access complications decrease and gastrointestinal bleeding in the setting of chronic antithrombotic therapy becomes the predominant etiology of blood loss.45 Strategies for reducing bleeding, termed by some as bleeding avoidance strategies, thus far have been predominately focused on reducing early bleeding through optimization of procedural pharmacology and procedural techniques. For example, bivalirudin has been found both in the ACUITY trial (NSTEMI) and HORIZONS-AMI to reduce bleeding rates of bleeding.57, 59HORIZONS-AMI compared three pharmacologic strategies in patients with ST-elevation ACS: heparin plus GP IIb/IIIa inhibitor, bivalirudin plus GP IIb/IIIa inhibitor, and bivalirudin alone. Patients treated with bivalirudin alone had a 24% lower incidence of major bleeding and combined adverse clinical events (combination of major bleeding or major adverse cardiovascular events—death, reinfarction, target-vessel revascularization for ischemia, and stroke) at 30 days.57 Further pharmacologic modifications such as utilization of lower levels of anticoagulation with heparin, decreasing the utilization and/or duration of therapy with GP IIb/IIIa inhibitors, and long-term maintenance on low-dose aspirin instead of full strength may be useful in decreasing bleeding complications.67 Finally, utilizing procedural techniques such as radial artery access and smaller sheath sizes that are associated with lower rates of bleeding provide additional benefit.
PERIPROCEDURAL MYOCARDIAL INFARCTION
There is no standard, universally accepted definition of a periprocedural MI used in clinical studies. The definition has varied over time but most studies now define it as a rise in CK-MB and/or troponin >3x the upper limit h1.75,76This definition is widely used despite the fact that there is a poor correlation between troponin elevations and adverse clinical outcomes. This is likely due to the fact that troponin elevations are more sensitive for myocardial damage allowing the detection of myocyte death that is not even detectable on cardiac MRI.77 Patients who develop a rise in cardiobiomarkers that does not meet the definition for periprocedural MI (1 to 3 x the upper limit of h1 [ULN]) are considered to have periprocedural myonecrosis that has not been closely correlated with adverse outcomes. No criteria have been developed for periprocedural MI in the setting of cardiac biomarkers that were increasing prior to the start of the procedure. Patients with biomarkers that are already elevated (but are stable or declining) prior to the start of the procedure are considered to have a periprocedural MI when the biomarkers increase by >20% from the preprocedural level.
Chest pain following PCI is common and occurs in up to 40% of all patients. The majority of these patients do not develop evidence of periprocedural MI. Observational studies of post-PCI patients have found that the development of Q waves or CK-MB >3 x ULN increases the risk of adverse outcomes and serious PCI-related complications (distal embolization, dissection, side branch occlusion, stent thrombosis). As a result, some have suggested that periprocedural MIs are simply a reflection of patient comorbidities such as atherosclerotic burden and the complexity of the PCI. This has been illustrated by intravascular ultrasound studies that correlated the degree of atherosclerosis with the development of periprocedural MI. As such, efforts including the use of embolic protection devices when performing PCI in saphenous vein grafts (that frequently have significant atherosclerotic/thrombotic burden) have shown the ability to reduce the incidence of periprocedural MI.
In practice, the debate over the prognostic implications of periprocedural MI and its impact on therapy have kept many providers from routinely checking biomarkers following PCI. Patients who have chest pain following PCI should have cardiac biomarkers checked as significant increases in combination with persistent pain and/or ECG changes may require repeat angiography or treatment with GP IIb/IIIa inhibitors.
TECHNICAL ASPECTS OF ANGIOGRAPHY AND PCI
Covering all the technical aspects of angiography and PCI in detail is beyond the scope of this book and the boards. The following sections attempt to cover the topics that may be seen on the general cardiology board exam.
Access
Catheterization originally was performed through a method known as the Sones technique that involved a cut-down of the brachial artery. As the indications for catheterization grew, accessing the vasculature through the femoral artery was found to be less invasive and associated with lower risks to the patient. Femoral access replaced the Sones technique as the predominant method of catheterization over the past 20 years.78 Advances in catheter design and improvements in technique have made the routine use of catheterization via the radial artery feasible in routine clinical practice. Data from the NCDR CathPCI database have shown that radial artery catheterization is associated with lower odds of bleeding complications at the expense of increased radiation exposure. While there is a learning curve associated with the adoption of catheterization from the radial artery, increased patient satisfaction and lower rates of vascular complications such as bleeding have increased its acceptance into clinical practice.
Catheters
Catheters commonly used to enter the left coronary circulation are Judkins left (JL) catheters and Amplatz left (AL) catheters. The JL catheter has a double curve with the length of the segment (in centimeters) between the first and second curves that determines the size of the catheter (JL 3.5, 4, 5, or 6 cm). The AL catheter has a preshaped half-circle with a tip extending out of the curve and perpendicular to it, giving the catheter three curves. AL catheters come in three sizes (0.5, 0.75, and 1 cm) based on the diameter of the half-circle/secondary curve. The increasing use of radial artery catheterization has resulted in the development of new catheters, such as the Jacky and Tiger catheters, specifically designed for accessing the coronary arteries through the arm. These catheters have a double bend similar to the AL catheters but differ in the design of the tip. The Jacky (tip which points slightly outward) and Tiger catheter (straight tip) are able to engage both the left and right coronary artery by advancing the catheter into the aortic root and then manipulating the catheter into the different coronary ostia.
During catheterization from the femoral artery, the JL4 is typically used as a starting catheter as it will be successful in engaging the left coronary artery in the majority of patients. Patients with a large aortic root, tortuous aorta, or large body habitus may require a larger catheter (JL5, JL6). Coronary artery anomalies may require the use of different catheters. For example, when the left main artery is located superiorly, a smaller JL catheter (JL3.5) or AL catheter is frequently used. Inferior origins of the left main may require a multipurpose catheter that has a downward tip. Short left main arteries or separate ostia for the left anterior descending (LAD) and left circumflex are more easily accessed using AL catheters. The LAD artery can be cannu- lated in these circumstances by clocking and advancing the catheter while the left circumflex artery can be accessed by counterclocking the catheter. The most common catheters used to enter the right coronary artery are the Judkins right (JR) catheters, 3DRC, and Amplatz right (AR). These catheters can also be used to access saphenous vein grafts and the subclavian artery.
Contrast Material
Coronary angiography utilizes contrast agents that allow for the visualization of the coronary vasculature. Currently available contrast agents contain iodine that more readily absorbs x-rays as compared to the surrounding tissue. This differential absorption of radiation results in the ability of the contrast agents to provide contrast and visualization of the coronary arteries. Contrast agents are divided based on osmolality (high, low, isosmolar) (Table 47.14). The majority of contrast agents used in current practice are low osmolar or isosmolar because high-osmolar agents have been found to have more hypotension, myocardial depression, heart failure, and electrical abh1ities (bradycardia, QRS and QT-interval prolongation, ventricular fibrillation).
TABLE
47.14 Summary of the Various Types of Contrast Agents Used in Coronary Angiography
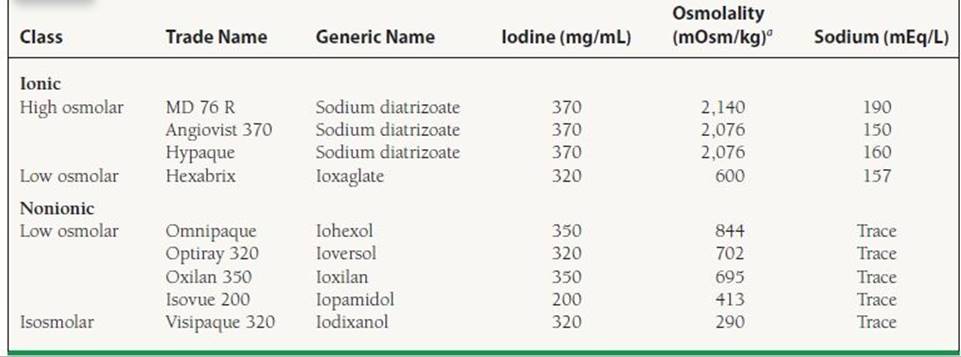
aBlood osmolality is 275 mOsmol/L.
Adapted from Askari AT, et al., eds. Introductory guide to cardiac catheterization. Philadelphia, PA: Lippincott Williams & Wilkins.
Prior ACC/AHA guidelines recommended the use of isosmolar contrast agents (i.e., iodixanol) in patients with chronic kidney disease. This was based upon the RECOVER trial that randomized 300 patients with a creatinine clearance <60 mL/min to either a low osmolar contrast agent (ioxaglate) or an isosmolar agent (iodixanol). The primary endpoint was CIN, defined as an increase in serum creatinine by 25% or >0.5 mg/dL. Patients treated with iodixanol had significantly lower rates of CIN (7.9%) than patients treated with ioxaglate (17.0%; p = 0.021).79 These recommendations have since been modified after the publication of the CARE study. This study randomized 482 patients with a creatinine clearance between 20 and 59 mL/min to iopamidol and iodixanol. Rates of CIN (defined as increase in serum creatinine ≥0.5) were similar in the two groups (4.4% after iopamidol and 6.7% after iodixanol) suggesting no difference between the agents.80 The lack of benefit with low osmolar agents was further supported with a subsequent meta-analysis.81 This analysis included 16 randomized controlled trials and 2,763 patients and did not find isosmolar agents to be protective against CIN when compared to all low osmolar agents except ioxaglate and iohexol. As such, current ACC/AHA guidelines have been modified to state that patients with chronic kidney disease can be treated with either an isosmolar contrast agent or a low osmolar contrast agent other than ioxaglate or iohexol.
Stents
Initial attempts at percutaneous revascularization with angioplasty were hindered by a high-rate acute vessel closure requiring cardiac surgery (often due to dissection). In 1993, the FDA approved the Gianturco–Roubin stent, making it the first coronary stents approved for routine clinical use.6Since that time, coronary artery stenting has undergone many advances and now serves as the predominant form of coronary revascularization. Initial stents were hindered by the proliferation of smooth muscle at the site of injury (known as restenosis). In response to this restenosis, stents coated with antiproliferative agents such as sirolimus, paclitaxel, everolimus, and zotarolimus were developed. As compared to bare metal stents, drug-eluting stents (DESs) greatly reduce the risk of in-stent restenosis and target lesion revascularization.
Some observational studies have suggested that drug-eluting stents have a mortality benefit.82 A mortality benefit has not been demonstrated in randomized data and is likely due to unmeasured differences in the two groups.83Given the concern over stent thrombosis and the requirement that patients who receive DES be treated with DAPT for up to a year, it is important to understand the patient populations who benefit most from drug-eluting stent implantation. Patients with diabetes, small vessel diameter (<3.0 mm), and long lesion length (>30 mm) are those patients who have consistently been shown to have the highest rate of restenosis and derive the most benefit from treatment with drug-eluting stents.84
ACKNOWLEDGMENTS
The authors would like to thank Soundos Moualla and Brendan Duffy, authors of this chapter in previous editions of the book, for their contributions and prior work.
REFERENCES
1. Roger VL, Go AS, Lloyd-Jones DM, et al. Heart disease and stroke statistics—2011 update: a report from the American Heart Association. Circulation. 2011;123:e18–e209.
2. Cavender MA, Nicholls SJ, Lincoff AM. Strategies for the development of new PPAR agonists in diabetes. Eur J Cardiovasc Prev Rehabil. 2010;17(suppl 1):S32–S37.
3. King SB III, Smith SC Jr, Hirshfeld JW Jr, et al. 2007 focused update of the ACC/AHA/SCAI 2005 guideline update for percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Practice guidelines. J Am Coll Cardiol.. 2008;51:172–209.
4. Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation. 2006;113:156–175.
5. Kushner FG, Hand M, Smith SC Jr, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2009;54:2205–2241.
6. Roubin GS. Coronary stenting: the first 10 years. Eurolntervention. 2006;2:40–44.
7. Epstein AJ, Polsky D, Yang F, et al. Coronary revascularization trends in the United States, 2001–2008. JAMA. 2011;305:1769–1776.
8. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. The GUSTO investigators. N Engl J Med. 1993;329:673–682.
9. Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto Miocardico (GISSI). Lancet. 1986;1:397–402.
10. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collaborative Group. Lancet. 1988;2: 349–360.
11. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Fibrinolytic Therapy Trialists'(FTT) Collaborative Group. Lancet.1994;343:311–322.
12. Gore JM, Granger CB, Simoons ML, et al. Stroke after thrombolysis. Mortality and functional outcomes in the GUSTO- I trial. Global Use of Strategies to Open Occluded Coronary Arteries. Circulation. 1995;92:2811–2818.
13. A clinical trial comparing primary coronary angioplasty with tissue plasminogen activator for acute myocardial infarction. The Global Use of Strategies to Open Occluded Coronary Arteries in Acute Coronary Syndromes (GUSTO IIb) Angioplasty Substudy Investigators. N Engl J Med. 1997;336:1621–1628.
14. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet. 2003;361:13–20.
15. Sardella G, Mancone M, Bucciarelli-Ducci C, et al. Thrombus aspiration during primary percutaneous coronary intervention improves myocardial reperfusion and reduces infarct size: the EXPIRA (thrombectomy with export catheter in infarct-related artery during primary percutaneous coronary intervention) prospective, randomized trial. J Am Coll Cardiol. 2009;53: 309–315.
16. Rodriguez A, Bernardi V Fernandez M, et al. In-hospital and late results of coronary stents versus conventional balloon angioplasty in acute myocardial infarction (GRAMI trial). Gianturco-Roubin in Acute Myocardial Infarction. Am J Cardiol. 1998;81:1286–1291.
17. Antoniucci D, Santoro GM, Bolognese L, et al. A clinical trial comparing primary stenting of the infarct-related artery with optimal primary angioplasty for acute myocardial infarction: results from the Florence Randomized Elective Stenting in Acute Coronary Occlusions (FRESCO) trial. J Am Coll Cardiol. 1998;31:1234–1239.
18. Stone GW Brodie BR, Griffin JJ, et al. Prospective, multicenter study of the safety and feasibility of primary stenting in acute myocardial infarction: in-hospital and 30-day results of the PAMI stent pilot trial. Primary Angioplasty in Myocardial Infarction Stent Pilot Trial Investigators. J Am Coll Cardiol.1998;31:23–30.
19. Reynolds HR, Hochman JS. Cardiogenic shock: current concepts and improving outcomes. Circulation. 2008;117:686–697.
20. Goldberg RJ, Spencer FA, Gore JM, et al. Thirty-year trends (1975 to 2005) in the magnitude of, management of, and hospital death rates associated with cardiogenic shock in patients with acute myocardial infarction: a population-based perspective. Circulation.2009;119:1211–1219.
21. Hochman JS, Sleeper LA, Webb JG, et al. Early Revascularization in acute myocardial infarction complicated by cardiogenic shock. SHOCK Investigators. Should We Emergently Revas- cularize Occluded Coronaries for Cardiogenic Shock. N Engl J Med. 1999;341:625–634.
22. Alexander KP, Newby LK, Armstrong PW et al. Acute coronary care in the elderly, part II: ST-segment-elevation myocardial infarction: a scientific statement for healthcare professionals from the American Heart Association Council on Clinical Cardiology: in collaboration with the Society of Geriatric Cardiology. Circulation. 2007;115:2570–2589.
23. Ellis SG, Tendera M, de Belder MA, et al. Facilitated PCI in patients with ST-elevation myocardial infarction. N Engl J Med. 2008;358:2205–2217.
24. Califf RM, O’Neil W Stack RS, et al. Failure of simple clinical measurements to predict perfusion status after intravenous thrombolysis. Ann Intern Med. 1988;108:658–662.
25. Gershlick AH, Stephens-Lloyd A, Hughes S, et al. Rescue angioplasty after failed thrombolytic therapy for acute myocardial infarction. N Engl J Med. 2005;353:2758–2768.
26. Cantor WJ, Fitchett D, Borgundvaag B, et al. Routine early angioplasty after fibrinolysis for acute myocardial infarction. N Engl J Med. 2009;360:2705–2718.
27. D’Souza SP, Mamas MA, Fraser DG, Fath-Ordoubadi F. Routine early coronary angioplasty versus ischaemia-guided angioplasty after thrombolysis in acute ST-elevation myocardial infarction: a meta-analysis. Eur Heart J. 2011;32:972–982.
28. Roe MT, Messenger JC, Weintraub WS, et al. Treatments, trends, and outcomes of acute myocardial infarction and percutaneous coronary intervention. J Am Coll Cardiol. 2010;56:254–263.
29. Bavry AA, Kumbhani DJ, Rassi AN, et al. Benefit of early invasive therapy in acute coronary syndromes: a meta-analysis of contemporary randomized clinical trials. J Am Coll Cardiol. 2006;48:1319–1325.
30. Mehta SR, Granger CB, Boden WE, et al. Early versus delayed invasive intervention in acute coronary syndromes. N Engl J Med. 2009;360:2165–2175.
31. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision making. JAMA. 2000;284:835–842.
32. Campeau L. Letter: Grading of angina pectoris. Circulation. 1976;54:522–523.
33. Coronary angioplasty versus medical therapy for angina: the second Randomised Intervention Treatment of Angina (RITA- 2) trial. RITA-2 trial participants. Lancet. 1997;350:461–468.
34. Henderson RA, Pocock SJ, Clayton TC, et al. Seven-year outcome in the RITA-2 trial: coronary angioplasty versus medical therapy. J Am Coll Cardiol. 2003;42:1161–1170.
35. Davies RF, Goldberg AD, Forman S, et al. Asymptomatic Cardiac Ischemia Pilot (ACIP) study two-year follow-up: outcomes of patients randomized to initial strategies of medical therapy versus revascularization. Circulation. 1997;95:2037–2043.
36. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356:1503–1516.
37. Shaw LJ, Berman DS, Maron DJ, et al. Optimal medical therapy with or without percutaneous coronary intervention to reduce ischemic burden: results from the Clinical Outcomes Utilizing Revascularization and Aggressive Drug Evaluation (COURAGE) trial nuclear substudy. Circulation.2008;117:1283–1291.
38. Patel MR, Dehmer GJ, Hirshfeld JW et al. ACCF/SCAI/STS/AATS/AHA/ASNC 2009 Appropriateness Criteria for Coronary Revascularization: a report by the American College of Cardiology Foundation Appropriateness Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, and the American Society of Nuclear Cardiology Endorsed by the American Society of Echocardiography, the Heart Failure Society of America, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2009;53:530–553.
39. Poldermans D, Hoeks SE, Feringa HH. Pre-operative risk assessment and risk reduction before surgery. J Am Coll Cardiol. 2008;51:1913–1924.
40. The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med. 1996;335:217–225.
41. Serruys PW, Morice MC, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961–972.
42. Leon MB, Baim DS, Popma JJ, et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. Stent Anticoagulation Restenosis Study Investigators. N Engl J Med. 1998;339:1665–1671.
43. Savi P, Herbert JM. Clopidogrel and ticlopidine: P2Y12 adenosine diphosphate-receptor antagonists for the prevention of atherothrombosis. Semin Thromb Hemost. 2005;31:174–183.
44. Steinhubl SR, Berger PB, Mann JT, 3rd, et al. Early and sustained dual oral antiplatelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA. 2002;288:2411–2420.
45. Cavender MA, Rao SV. Bleeding associated with current therapies for acute coronary syndrome: what are the mechanisms? J Thromb Thrombolysis. 2010;30:332–339.
46. Wiviott SD, Braunwald E, McCabe CH, et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2007;357:2001–2015.
47. James S, Akerblom A, Cannon CP, et al. Comparison of ticagrelor, the first reversible oral P2Y(12) receptor antagonist, with clopidogrel in patients with acute coronary syndromes: Rationale, design, and baseline characteristics of the PLATelet inhibition and patient Outcomes (PLATO) trial. Am Heart J.2009;157:599–605.
48. Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med. 2009;361:1045–1057.
49. Gaglia MA, Jr., Waksman R. Overview of the 2010 Food and Drug Administration Cardiovascular and Renal Drugs Advisory Committee meeting regarding ticagrelor. Circulation. 2011;123:451–456.
50. Mehta SR, Bassand JP, Chrolavicius S, et al. Dose comparisons of clopidogrel and aspirin in acute coronary syndromes. N Engl J Med. 2010;363:930–942.
51. Campbell CL, Smyth S, Montalescot G, et al. Aspirin dose for the prevention of cardiovascular disease: a systematic review. JAMA. 2007;297:2018–2024.
52. Harrington RA, Califf RM. Late ischemic events after clopidogrel cessation following drug-eluting stenting should we be worried? J Am Coll Cardiol. 2006;48:2592–2595.
53. Mauri L, Kereiakes DJ, Normand SL, et al. Rationale and design of the dual antiplatelet therapy study, a prospective, multicenter, randomized, double-blind trial to assess the effectiveness and safety of 12 versus 30 months of dual antiplatelet therapy in subjects undergoing percutaneous coronary intervention with either drug- eluting stent or bare metal stent placement for the treatment of coronary artery lesions. Am Heart J. 2010;160:1035–1041, 41e1.
54. Bhatt DL, Topol EJ. Current role of platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes. JAMA. 2000;284:1549–1558.
55. Giugliano RP, White JA, Bode C, et al. Early versus delayed, provisional eptifibatide in acute coronary syndromes. N Engl J Med. 2009;360:2176–2190.
56. Winchester DE, Wen X, Brearley WD, et al. Efficacy and safety of glycoprotein IIb/IIIa inhibitors during elective coronary revascularization: a meta-analysis of randomized trials performed in the era of stents and thienopyridines. J Am Coll Cardiol. 2011;57:1190–1199.
57. Stone GW, Witzenbichler B, Guagliumi G, et al. Bivalirudin during primary PCI in acute myocardial infarction. N Engl J Med. 2008;358:2218–2230.
58. Van’t Hof AW, Ten Berg J, Heestermans T, et al. Prehospital initiation of tirofiban in patients with ST-elevation myocardial infarction undergoing primary angioplasty (On-TIME 2): a multicentre, double-blind, randomised controlled trial. Lancet. 2008;372:537–546.
59. Stone GW, McLaurin BT, Cox DA, et al. Bivalirudin for patients with acute coronary syndromes. N Engl J Med. 2006;355:2203–2216.
60. Ferguson JJ, Califf RM, Antman EM, et al. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. JAMA.2004;292:45–54.
61. Peterson ED, Dai D, DeLong ER, et al. Contemporary mortality risk prediction for percutaneous coronary intervention: results from 588,398 procedures in the National Cardiovascular Data Registry. J Am Coll Cardiol. 2010;55:1923–1932.
62. Singh M, Rihal CS, Selzer F, et al. Validation of Mayo Clinic risk adjustment model for in-hospital complications after percutaneous coronary interventions, using the National Heart, Lung, and Blood Institute dynamic registry. J Am Coll Cardiol. 2003;42:1722–1728.
63. Singh M, Rihal CS, Lennon RJ, et al. Bedside estimation of risk from percutaneous coronary intervention: the new Mayo Clinic risk scores. Mayo Clin Proc. 2007;82:701–708.
64. Rihal CS, Textor SC, Grill DE, et al. Incidence and prognostic importance of acute renal failure after percutaneous coronary intervention. Circulation. 2002;105:2259–2264.
65. Pannu N, Wiebe N, Tonelli M. Prophylaxis strategies for contrast-induced nephropathy. JAMA. 2006;295:2765–2779.
66. ACT Investigators. Acetylcysteine for Prevention of Renal Outcomes in Patients Undergoing Coronary and Peripheral Vascular Angiography: Main Results From the Randomized Acetylcysteine for Contrast-Induced Nephropathy Trial (ACT). Circulation. 2011;124:1250–1259.
67. Cavender MA, Rao SV, Ohman EM. Major bleeding: management and risk reduction in acute coronary syndromes. Exp Opin Pharmacother. 2008;9:1869–1883.
68. Rao SV O’Grady K, Pieper KS, et al. Impact of bleeding severity on clinical outcomes among patients with acute coronary syndromes. Am J Cardiol. 2005;96:1200–1206.
69. Eikelboom JW, Mehta SR, Anand SS, et al. Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation. 2006;114:774–782.
70. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA. 2004;292:1555–1562.
71. Wang TY, Xiao L, Alexander KP, et al. Antiplatelet therapy use after discharge among acute myocardial infarction patients with in-hospital bleeding. Circulation. 2008;118:2139–2145.
72. Spencer FA, Moscucci M, Granger CB, et al. Does comorbidity account for the excess mortality in patients with major bleeding in acute myocardial infarction? Circulation. 2007;116:2793–2801.
73. Mehran R, Rao SV, Bhatt DL, et al. Standardized bleeding definitions for cardiovascular clinical trials: a consensus report from the bleeding academic research consortium. Circulation. 2011;123:2736–2747.
74. Steg PG, Huber K, Andreotti F, et al. Bleeding in acute coronary syndromes and percutaneous coronary interventions: position paper by the Working Group on Thrombosis of the European Society of Cardiology. Eur Heart J. 2011;32:1854–1864.
75. Cannon CP, Battler A, Brindis RG, et al. American College of Cardiology key data elements and definitions for measuring the clinical management and outcomes of patients with acute coronary syndromes. A report of the American College of Cardiology Task Force on Clinical Data Standards (Acute Coronary Syndromes Writing Committee). J Am Coll Cardiol. 2001;38:2114–2130.
76. Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. Eur Heart J. 2007;28:2525–2538.
77. Locca D, Bucciarelli-Ducci C, Ferrante G, et al. New universal definition of myocardial infarction applicable after complex percutaneous coronary interventions? JACC Cardiovasc Interv. 2010;3:950–958.
78. Rao SV, Ou FS, Wang TY, et al. Trends in the prevalence and outcomes of radial and femoral approaches to percutaneous coronary intervention: a report from the National Cardiovascular Data Registry. JACC Cardiovasc Interv. 2008;1:379–386.
79. Jo SH, Youn TJ, Koo BK, et al. Renal toxicity evaluation and comparison between visipaque (iodixanol) and hexabrix (ioxaglate) in patients with renal insufficiency undergoing coronary angiography: the RECOVER study: a randomized controlled trial. J Am Coll Cardiol.2006;48:924–930.
80. Solomon RJ, Natarajan MK, Doucet S, et al. Cardiac Angiography in Renally Impaired Patients (CARE) study: a randomized double-blind trial of contrast-induced nephropathy in patients with chronic kidney disease. Circulation. 2007;115:3189–3196.
81. Reed M, Meier P, Tamhane UU, et al. The relative renal safety of iodixanol compared with low-osmolar contrast media: a meta-analysis of randomized controlled trials. JACC Cardiovascular Interv. 2009;2:645–654.
82. Douglas PS, Brennan JM, Anstrom KJ, et al. Clinical effectiveness of coronary stents in elderly persons: results from 262,700 Medicare patients in the American College of Cardiology-National Cardiovascular Data Registry. J Am Coll Cardiol. 2009;53:1629–1641.
83. Kirtane AJ, Gupta A, Iyengar S, et al. Safety and efficacy of drug-eluting and bare metal stents: comprehensive meta-analysis of randomized trials and observational studies. Circulation. 2009;119:3198–3206.
84. Stone GW, Parise H, Witzenbichler B, et al. Selection criteria for drug-eluting versus bare-metal stents and the impact of routine angiographic follow-up: 2-year insights from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) trial. J Am Coll Cardiol. 2010;56:1597–1604.
85. Yang X, Alexander KP, Chen AY, et al. The implications of blood transfusions for patients with non-ST-segment elevation acute coronary syndromes: results from the CRUSADE National Quality Improvement Initiative. J Am Coll Cardiol. 2005;46:1490–1495.
86. Nikolsky E, Mehran R, Dangas G, et al. Development and validation of a prognostic risk score for major bleeding in patients undergoing percutaneous coronary intervention via the femoral approach. Eur Heart J. 2007;28:1936–1945.
87. Manoukian SV, Feit F, Mehran R, et al. Impact of major bleeding on 30-day mortality and clinical outcomes in patients with acute coronary syndromes: an analysis from the ACUITY Trial. J Am Coll Cardiol. 2007;49:1362–1368.
88. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non-Q-wave myocardial infarction. Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators. N Engl J Med.1998;338:1488–1497.
89. Moscucci M, Fox KA, Cannon CP, et al. Predictors of major bleeding in acute coronary syndromes: the Global Registry of Acute Coronary Events (GRACE). Eur Heart J. 2003;24:1815–1823.
90. Kinnaird TD, Stabile E, Mintz GS, et al. Incidence, predictors, and prognostic implications of bleeding and blood transfusion following percutaneous coronary interventions. Am J Cardiol. 2003;92:930–935.
QUESTIONS AND ANSWERS
Questions
1. A 73-year-old man underwent percutaneous coronary intervention (PCI) after a non–ST-elevation myocardial infarction (NSTEMI). He was pretreated with 325 mg of aspirin and 600 mg of clopidogrel, plus bivalirudin during the intervention. A DES is deployed into the mid-left anterior descending (LAD). Following the procedure, which of the following antiplatelet regimens is most appropriate?
a. Continue 325 mg aspirin and 75 mg clopidogrel for 12 months.
b. Continue 81 mg aspirin for life and clopidogrel 75 mg for 6 months.
c. Continue 81 mg aspirin for life and clopidogrel for at least 12 months.
d. Continue 81 mg aspirin for 12 months and clopidogrel 75 mg for 6 months.
2. A 62-year-old woman with stable angina has presented for elective PCI to a known focal stenosis in a moderate-sized first diagonal branch. She is not taking medications and has a severe allergy to shellfish (hives), and she also reports an allergy to aspirin although she cannot specify the reaction. Which of the following statements regarding patient management is correct?
a. Administer 100 mg hydrocortisone IV, 50 mg diphenhydramine (Benadryl) IV, and 600 mg clopidogrel orally before the procedure, and then proceed with the scheduled intervention.
b. Administer 40 mg methylprednisolone IV, 50 mg diphenhydramine (Benadryl) IV, 600 mg clopidogrel orally, and proceed with the scheduled intervention.
c. Administer 100 mg hydrocortisone IV, 50 mg diphenhydramine (Benadryl) IV, 325 mg aspirin, and 300 mg clopidogrel orally before the procedure, and then proceed with the scheduled intervention.
d. Consult an allergy specialist and postpone the intervention.
3. A 50-year-old man presents to the emergency room (ER) about 100 minutes after the onset of chest pain. The pain is substernal, radiates to the left arm, and is associated with vomiting and diaphoresis. On examination, the patient is tachycardic with a heart rate of 104 and hypertensive with blood pressure of 150/88. An electrocardiogram showed 3 mm ST elevation in the anterior and lateral leads. Symptoms were not relieved with sublingual nitroglycerin or beta-blocker therapy. An IV nitroglycerin drip was titrated to control the patient’s symptoms. The closest interventional cardiology center is 120 minutes away. The patient has asked about the therapeutic options at this point. What can you tell him about the various therapeutic modalities?
a. Primary PCI is recommended over thrombolytics because PCI has short-term mortality benefit, reduced reinfarction risk, and reduced risk of stroke, regardless of duration of symptoms and time required to PTCA.
b. Thrombolysis followed by transfer to center with PCI capabilities
c. Half-dose thrombolysis should be recommended; then the patient should be transferred for PCI.
d. Thrombolysis. Transfer to center with PCI capabilities if chest pain and ECG changes do not resolve within 3 hours.
4. A 62-year-old woman, with ongoing tobacco abuse, diabetes, hypertension, and hyperlipidemia, presents to the ER with a 2-day history of intermittent chest pain. On examination, she is tachycardic with a heart rate of 101 beats/min (bpm) and hypertensive with a blood pressure of 160/100 mm Hg. The patient does not have any signs of heart failure. An electrocardiogram showed 2-mm depression in V2–V6. The patient is started on heparin and given IV metoprolol and nitroglycerin. In addition, she was started on an eptifibatide infusion. The patient remained asymptomatic until her coronary angiogram. The left heart catheterization showed 90% stenosis in the proximal third of the LAD and 80% stenosis in the proximal RCA, with 70% disease in the middle circumflex artery. The best plan of treatment for this patient is:
a. Complete revascularization with multivessel PCI
b. Referral for three-vessel CABG
c. PCI to the LAD with staged intervention to the RCA and LCx
d. Medical management with no PCI or CABG
5. A previously healthy 78-year-old male presents to the emergency department (ED) complaining of chest pain and shortness of breath. His initial blood pressure is 79/40 and his heart rate is 117 bpm. His initial ECG shows 3 mm ST elevations in V1–V4and his chest x-ray is notable for pulmonary edema. What is the next best treatment option?
a. Medically stabilize with IV diuretics and antithrombotic agents. Consider revascularization once medically stabilized.
b. Fibrinolytic therapy
c. Urgent angiography with goal to provide revascularization therapy
d. Intubate and place Swan Ganz catheter to help determine etiology of illness. Place intra-aortic balloon pump if the patient appears to have cardiogenic shock with low cardiac index and elevated pulmonary capillary wedge pressure.
6. A 56-year-old female with hypertension, obesity, obstructive sleep apnea, and fibromyalgia is undergoing angiography for chest pain. She describes her chest pain as stabbing in nature. It occurs mostly when performing housework or in periods of increased stress. It is not associated with shortness of breath. Her primary care physician evaluated her with a nuclear stress test that showed no evidence of ischemia; however, she continued to have this discomfort. The patient was scheduled for angiography to provide a definitive workup for her persistent chest pain. Angiography was notable for a 60% stenosis in the left circumflex artery and mild diffuse coronary artery disease in the LAD artery and right coronary artery. The most appropriate management is:
a. Medical therapy with aspirin and statin as there is no indication for revascularization.
b. Begin secondary prevention medications and schedule repeat stress test in 1 year.
c. PCI to the left circumflex
d. Perform FFR of the left circumflex.
7. An 85-year-old female with a creatinine of 1.6 is undergoing angiography after a positive stress test. Which of the following interventions reduces her risk of contrast-induced nephropathy (CIN)?
a. Admission the night before catheterization for N-acetylcysteine and sodium bicarbonate infusion
b. Biplane angiography and iodixanol contrast
c. Hydration with h1 saline prior to the catheterization
d. Discontinuation of lisinopril 1 week prior to angiography
8. A 67-year-old male with diabetes and hypertension presents with three episodes of chest pain at rest over the past 24 hours. He is currently chest pain–free. His home medications include aspirin, lisinopril, and simvastatin. He continues to abuse tobacco. His first set of cardiac biomarkers is notable for a troponin of 0.94 and a CK-MB of 54. The next step in the management of this patient is:
a. Give 325 mg of aspirin and 600 mg of clopidogrel and begin infusion of eptifibatide and heparin. Schedule angiography as soon as possible (urgent, not emergent).
b. Give 325 mg of aspirin and 600 mg of clopidogrel and begin infusion of heparin. Schedule stress test once cardiac enzymes begin to decline.
c. Give 325 mg of aspirin and 600 mg of clopidogrel and begin infusion of heparin. Schedule angiography as soon as possible (urgent, not emergent).
d. Give 325 mg of aspirin and 600 mg of clopidogrel and begin infusion of eptifibatide and heparin. Schedule stress test once cardiac enzymes begin to decline.
9. Which of following is not a relative contraindication for the use of prasugrel in patients with acute coronary syndrome undergoing PCI?
a. Weight <60 kg
b. Previous TIA/CVA
c. Creatinine clearance <30
d. Age ≥75
10. Which is following statements is false regarding the indications for routine PCI immediately following administration of fibrinolytic therapy for patients with ST-elevation myocardial infarction (STEMI)?
a. Patients with hemodynamic instability following fibrinolytic therapy should undergo rescue PCI.
b. Patients with sustained, unstable ventricular tachycardia following fibrinolytic therapy should undergo rescue PCI.
c. Patients with <50% resolution of ST-segment elevation 30 minutes after fibrinolytic therapy should undergo rescue PCI.
d. Patients with <50% resolution of ST-segment elevation 90 minutes after fibrinolytic therapy should undergo rescue PCI.
Answers
1. Answer C: There is no indication for high-dose aspirin therapy following PCI based on the CURRENT OASIS-7 trial. Patients with prior PCI should continue on low-dose aspirin for the remainder of their lifetime. The length of time in which clopidogrel is necessary is currently unknown. Prior recommendations suggested that 3 to 6 months (depending on the type of stent) of thienopyridine therapy was sufficient; however, there was a small but potentially devastating risk of late-stent thrombosis. Given this risk of stent thrombosis, thienopyridines are recommended for at least 1 year. Patients at low risk of bleeding can continue therapy past 1 year, but the optimal length of therapy will not be known until the completion of the ongoing DAPT trial.
2. Answer D: Consult an allergy specialist and postpone the intervention. Manifestations of aspirin sensitivity such as exacerbations of respiratory tract disease and urticaria can occur in up to 10% and 0.2% of the general population, respectively. An urgent intervention could be undertaken with the pharmacologic therapy described in the second option. However, an elective intervention should be postponed, awaiting appropriate workup and desensitization. There is little or no experience with aspirin desensitization in patients with aspirin-induced anaphylaxis. Potent platelet inhibitors, such as prasugrel and clopidogrel, can be used in patients with aspirin allergy.
3. Answer B: Current American College of Cardiology/American Heart Association (ACC/AHA) guidelines for management of patients with STEMI are dependent on the duration of symptoms, mortality risk of the STEMI, the risk of bleeding, and the difference between time to PCI and time to thrombolytics. PCI is recommended over thrombolysis when experienced operators restore blood flow in <90 minutes. The patient in this question is relatively young, with a large STEMI that has a high mortality risk. He has been having symptoms for 80 minutes and requires 120 minutes or more to have perfusion established with PCI. He is hemodynamically stable. Delayed treatment affects outcome negatively, whether treatment is PCI or thrombolytics. Thrombolysis is highly effective in restoring coronary flow in STEMI, particularly when the patient has presented within 3 hours of symptoms. Data from the National Registry of MI showed increased mortality when PCI is delayed beyond 2 hours. Hence, this patient will likely have better outcome if he receives thrombolysis. Following thrombolysis, he should be transferred to a center with PCI capabilities for angiography.
4. Answer B: The patient is diabetic with multivessel coronary artery disease. CABG has been shown to provide a survival benefit over PTCA according to the BARI trial. However, in the PCI era, one could recommend PCI with stenting in patients with low/immediate SYNTAX score because there was no survival benefit of CABG over PCI shown in the SYNTAX trial. Patients treated with PCI are more likely to require further revascularization and more antianginal medications; hence, the current appropriateness criteria for PCI give CABG an appropriate rating, while PCI is given an indeterminate rating.
5. Answer C: The patient is clearly in cardiogenic shock due to a large anterior myocardial infarction (MI). Placement of a Swan Ganz catheter would only delay definitive therapy with revascularization. The SHOCK trial showed that patients with cardiogenic shock benefit from emergent revascularization when compared to initial medical stabilization and therapy. While the SHOCK trial did not show definite benefit for patients older than 75 years, there is no reason to suggest that a previously well 78-year-old patient would not derive similar benefit. Observational studies of elderly patients undergoing revascularization for cardiogenic shock have suggested no increased harm in this population.
6. Answer D: The patient has a moderately severe stenosis in the left circumflex. While her symptoms are somewhat atypical, women are less likely to have classic stable angina. The normal stress test is reassuring; however, direct measurement of the physiologic significance of the stenosis is a useful tool. The FAME trial showed that deferring intervention in patients with an FFR of >0.80 is safe and reduces the utilization of PCI. The use of FFR-guided PCI in patients such as this reduces the use of unnecessary PCI while utilizing PCI in those patients with lesions resulting in limitation of coronary perfusion. Based on the results of the COURAGE trial, it is not unreasonable to pursue medical therapy (Choice A); however, the patient should be started on an antianginal therapy such as calcium channel blocker, nitrate, etc. PCI to the left circumflex is not indicated given her atypical symptoms without some evidence of physiologic significance (i.e., stress test, FFR, IVUS).
7. Answer C: The only strategy proven to reduce CIN is adequate hydration prior to angiography. Iodixanol, an isosmolar/nonionic contrast dye, has some evidence that it reduces CIN; however, when compared to iopamidol, a low osmolar/nonionic contrast dye, there was no difference in CIN. W-acetylcysteine has not been shown in large studies to reduce CIN when compared to simple hydration. While angiotensin-converting enzyme inhibitors should be discontinued if CIN develops, there is no evidence that discontinuing these medications will prevent CIN.
8. Answer D: His TIMI risk score is 5 (age >65, three or more risk factors for CAD, two or more episodes of chest pain, aspirin use within 7 days, and positive cardiac bio-markers). Patients with TIMI risk score >2 benefit from an early invasive revascularization strategy. Based on the EARLY-ACS trial, there is no indication for glycoprotein IIb/IIIa inhibitors (GP IIb/IIIa inhibitors) at this time. GP IIb/IIIa inhibitors can be safely reserved for provisional use in the cath lab if necessary or in patients who have not had thienopyridine pretreatment.
9. Answer C: The TRITON TIMI-38 trial showed that patients with ACS undergoing PCI who were randomized to prasugrel had a 19% reduction in death, nonfatal MI, or nonfatal stroke when compared to patients randomized to clopidogrel. However, patients with age ≥75 years, weight <60 kg, or a previous TIA/CVA had less efficacy and more bleeding events. As a result, prasugrel is contraindicated in these patient populations.
10. Answer C: ST-segment resolution is a frequently used but relatively poor marker of the success of fibrinolytic therapy. Patients who are otherwise stable but have persistent ST-segment elevations on electrocardiograms taken immediately after the administration of fibrinolytics should be monitored and not proceed with rescue PCI as long as they do not develop hemodynamic or electrical instability. If ST segments have seen >50% resolution after 90 minutes, rescue PCI should be performed.