Siddharth A. Wartak and Heather L. Gornik
Lower extremity peripheral artery disease (PAD) is a marker of systemic atherosclerosis and has been estimated to affect approximately 8 to 12 million Americans.1 PAD is associated with functional and quality of life (QOL) impairment, increased risk of progressive limb ischemia, and increased risk of cardiovascular ischemic events (i.e., myocardial infarction [MI] and stroke) and mortality. Although screening for PAD is simple, easy, and inexpensive using the ankle–brachial index (ABI), PAD remains an underdiagnosed and undertreated health condition. Treatment of the PAD patient requires attention to leg symptoms and functional capacity as well as aggressive cardiovascular risk reduction therapies.
DEFINITION
Atherosclerotic peripheral vascular disease includes a diverse group of disorders that lead to progressive stenosis, occlusion, or aneurysmal dilation of the aorta and its noncoronary branch arteries, including the carotid and vertebral, upper extremity, visceral, and lower extremity arterial branches. According to the American Heart Association, PAD is the preferred clinical term used to describe disease of the arteries of the arms and legs. This chapter focuses on lower extremity PAD, although it is recognized that upper extremity PAD, especially subclavian artery stenosis, can be an important clinical disorder that may lead to discrepant blood pressures in the arms, arm claudication, or vertebral–subclavian or coronary–subclavian steal phenomena. In addition, while lower extremity PAD may uncommonly be caused by nonatherosclerotic disease (e.g., large vessel vasculitis, arterial entrapment syndromes, fibromuscular dysplasia), this chapter focuses on lower extremity PAD due to atherosclerotic vascular disease, the most common cause.
EPIDEMIOLOGY AND RISK FACTORS
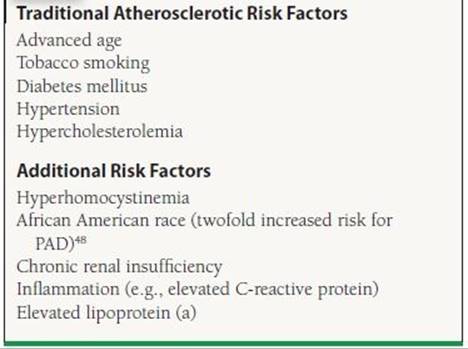
The prevalence of PAD increases with age, and the disease affects men and women nearly equally, up to 29% of the elderly population in a general medical practice.2,3 Risk factors for PAD are similar to those of coronary artery disease. They can be categorized as hereditary or acquired. The most important risk factors for PAD are advanced age, diabetes mellitus, and tobacco use. Additional risk factors for PAD are shown in Table 50.1.
TABLE
50.1 Risk Factors for Lower Extremity PAD
PAD IS A MARKER OF INCREASED CARDIOVASCULAR RISK
PAD is a marker for extensive systemic atherosclerosis and high cardiovascular risk. It has been estimated that among patients with symptomatic PAD (claudication) the 5-year mortality is as high as 30% with an additional 20% suffering a nonfatal MI or stroke.4 In published case series of PAD patients, 60% to 80% have significant coronary artery disease in at least one vessel on angiography5,6 and up to 25% of patients will have significant internal carotid artery stenosis 7,8 In the recent REACH registry, 21% of patients with PAD suffered an MI, a stroke, cardiovascular death, or hospitalization within 1 year of follow-up as compared to 15% of patients with established coronary artery disease.9
A low ABI has been shown in multiple studies to be an independent predictor of mortality.10,11 Patients with ABI of <0.90 are twice as likely to have a history of MI, angina, and heart failure than patients with an ABI of >1.0.12,13 An abnormal ABI also provides complimentary information to Framingham risk score (FRS) and increases cardiovascular risk prediction. A low ABI (≤0.90) was associated with approximately twice the 10-year total mortality, cardiovascular mortality, and major coronary event rate compared to the overall rate in each FRS category.14 In the recently published German Epidemiological Trial on Ankle-Brachial Index (GET ABI), an abnormal ABI for both symptomatic and asymptomatic patients was associated with increased risk of major cardiovascular events.15
NATURAL HISTORY OF PAD
Less than 5% of patients with stable claudication will require amputation;4 however, the annual risk increases dramatically to 30% to 40% among those with critical limb ischemia (CLI).16 It has been demonstrated that patients with PAD have significant function and QOL impairment. The QOL impairment among PAD patients is similar to that of patients with congestive heart failure or recent MI.17Objective evidence of clinical depression is twice as common among patients with PAD.18 PAD leads to functional impairment with decreased walking distance and speed in patients with claudication and even among patients with atypical leg symptoms.19 Such functional impairment can diminish a patient’s abilities to work, exercise regularly, and participate in recreational activities.
SYMPTOMS AND SIGNS OF PAD
The classic symptom of lower extremity PAD is claudication, which is derived from Latin and meaning to limp. Claudication is defined as recurrent burning, aching, fatigue, or heaviness in the leg muscles that is provoked with a predictable level of exercise and that resolves with a predictable duration of rest (generally <10 minutes). The Rose claudication questionnaire is a simple screening tool for claudication that can be used in clinical practice by asking the patient two simple questions: “Do you get pain in either leg when you walk?” and “Does the pain go away when you stop walking?” If the answer to both questions is yes, the likelihood of PAD is >95%.20 Claudication must be distinguished from other potential diagnoses, including pseudoclaudication due to lumbar canal stenosis that can present with buttock, back, and thigh pain with both exertion and prolonged standing. While claudication is an important symptom of PAD, it is important to recognize that the majority of patients with PAD do not present with classic intermittent claudication (Fig. 50.1). The majority of patients with PAD will exhibit leg discomforts that do not meet the definition of claudication (atypical leg symptoms), while others remain completely asymptomatic and are identified only through measures such as the ABI.
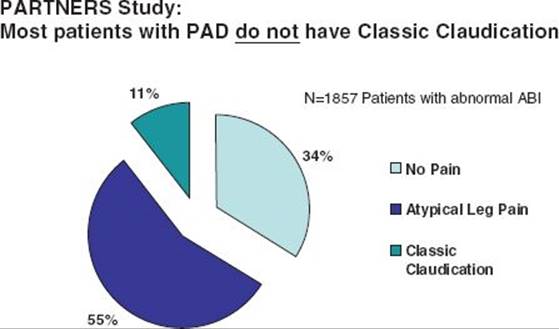
FIGURE 50.1 Clinical presentation of lower extremity PAD in the stable patient. In these data from the PARTNERS study, the majority of patients identified to have an abnormal ABI on a screening examination were either asymptomatic or had leg symptoms atypical for claudication. Only 11% in this study had classic intermittent claudication. These findings emphasize the variable clinical presentation of PAD and the need to incorporate modalities beyond screening for claudication (such as the ABI) to diagnose this disease. (Adapted from Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286(11):1317–1324.)
Acute Limb Ischemia and Critical Limb Ischemia
There are two severe clinical presentations of lower extremity PAD that must be clinically recognized in a timely fashion. Acute limb ischemia, characterized by the “6Ps” of pain, paresthesias, pallor, pulselessness, paralysis, and poikilothermia (or “polar”), is a vascular emergency due to thrombotic arterial occlusion that requires urgent revascularization with thrombolytic therapy and/or thrombectomy. CLI is a more common severe clinical presentation of PAD. CLI is defined as objectively proven PAD plus ischemic rest pain, nonhealing ulceration, or gangrene that has been present for at least 2 weeks.21The most important risk factors for development of CLI among patients with stable PAD are diabetes mellitus and ongoing tobacco use, but older patient age (>65 years), lower baseline ABI, and hyperlipidemia also increase risk.21 CLI is vascular urgency that requires expedient evaluation for revascularization. Patients with CLI are at a very high risk of a major cardiovascular event in the year following diagnosis, including death, and careful assessment of cardiovascular risk factor control and symptoms is important in this population.
Physical Examination Findings in Peripheral Arterial Disease
A comprehensive history and vascular examination is key for diagnosis and appropriate management of PAD. The comprehensive physical examination in the PAD patient should include measurement of blood pressure in bilateral arms (to screen for subclavian stenosis/upper extremity PAD); assessment of the carotid, upper extremity, and lower extremity (femoral, popliteal, dorsalis pedis [DP], posterior tibial) pulses; and assessment of the abdominal aorta. Using standardized definitions, pulses are graded on a scale from 0 to 3 with 2 = normal pulse, 1 = diminished pulse, 0 = nonpalpable pulse, and 3 = abnormally bounding or aneurysmal pulse.16 If no pulse is palpable, Doppler examination using a handheld continuous-wave device should be performed. An absent posterior tibial pulse has high specificity for diagnosis of PAD. Abnormalities of the DP pulse are less specific due to a high prevalence of anomalous or absent DP arteries in healthy patients. In addition to pulse deficits, other physical examination findings consistent with lower extremity PAD include vascular bruits (heard over femoral or popliteal arteries), hair loss, nail hypertrophy, and rapid elevation pallor or dependent rubor of the leg. Socks must be removed at every visit to carefully inspect the feet for evidence of tissue loss (i.e., ulcers or gangrene) as well as for signs of concomitant foot pathology, such as peripheral neuropathy or excessive callous formation.
DIAGNOSTIC TESTING FOR PAD
Ankle–Brachial Index
The ABI is the ratio of ankle systolic pressure to brachial systolic pressure and is determined by measuring systolic blood pressures in bilateral brachial arteries and at bilateral DP and posterior tibial arteries using a handheld Doppler device. Calculation of the ABI is shown in Figure 50.2. Interpretation guidelines for the ABI are shown in Table 50.2. The range of normal values for an ABI is 1.0 to 1.4. A normal resting ABI does not always rule out PAD. If the ABI is borderline (e.g., 0.91 to 0.99) or normal and the clinical suspicion of PAD is high, repeat ABI after treadmill exercise should be performed. An ABI may fall by 20% or more in patients with significant PAD after exercise. This is especially true among patients with aortoiliac disease (“inflow disease”).

Figure 50.2 Calculation of the ABI. The ABI is the ratio of blood flow in the legs to the arms. The ankle blood pressure for each limb is the higher of the DP and posterior tibial artery pressures. For both the right and left ABI calculation, the higher of the two arm blood pressures is used for the denominator. (From Cleveland Clinic Foundation, with permission.)
TABLE
50.2 Interpretation of the ABIa
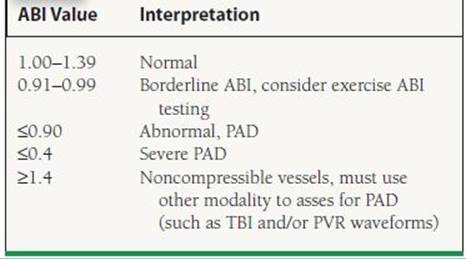
aABI values are interpreted according to the 2011 update of the American College of Cardiology Foundation/American Heart Association Guideline for the management of Patients with Peripheral Artery Disease. Rooke TW, et al. J Am Coll Cardiol. 2011;58(19):2020–2045.
It should also be emphasized that an ABI of >1.4 is not normal and suggests noncompressible vessels either from vascular calcification (“medial calcinosis”) or from inability to compress arteries due to obesity. This is commonly seen among patients with diabetes and chronic kidney disease. A high or falsely elevated ABI has been shown to confer increased cardiovascular risk in epidemiologic studies.10,14In clinical practice, an ABI > 1.4 cannot be interpreted and thus cannot confirm or rule out the diagnosis of PAD without another diagnostic test, such as pulse volume recordings (PVRs), the toe–brachial index (TBI), or an imaging modality.
Imaging Studies for PAD
Beyond the ABI, segmental leg pressures with PVRs or Doppler tracings may be used to localize disease by anatomic segments (e.g., aortoiliac disease, femoropopliteal disease, infrapopliteal disease). Transcutaneous oximetry may be helpful to determine tissue perfusion and limb viability in the setting of CLI and ulceration. In some cases, imaging modalities may be indicated to more definitively define anatomy and establish severity of disease. Diagnostic modalities for PAD are shown in Table 50.3. In general, imaging studies are most appropriately reserved for selected patients with PAD, such as for revascularization planning or for postprocedural graft or stent surveillance or for cases in which the diagnosis of PAD or the nature of disease is uncertain. For example, these imaging studies are particularly important for evaluation of nonatherosclerotic causes of PAD (e.g., arterial aneurysm, fibromuscular dysplasia, entrapment syndromes, and vasculitis). Imaging studies may also be indicated to establish the diagnosis of PAD in the setting of noncompressible vessels (i.e., ABI > 1.4).
TABLE
50.3 Diagnostic Modalities for PAD
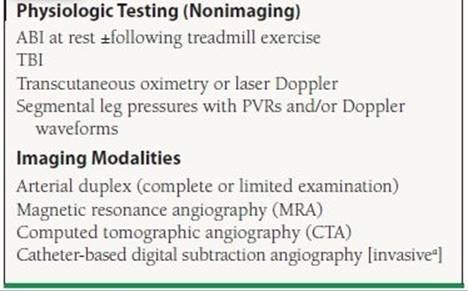
aAngiography is generally reserved for cases in which revascularization is anticipated or noninvasive testing is inadequate to comprehensively evaluate the patient.
MANAGEMENT OF PAD: A THREE-PRONGED APPROACH
The comprehensive care of the PAD patient must address three important aspects: protection of the feet and prevention of limb loss, prevention of cardiovascular events, and improvement of functional capacity and QOL (Fig. 50.3).
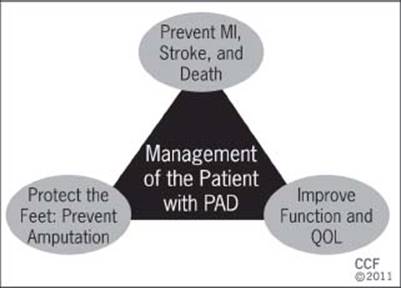
FIGURE 50.3 The three-pronged approach to PAD care. Comprehensive care of the PAD patient must include all three aspects of care. (From Cleveland Clinic Foundation, with permission.)
Foot Care and Ulcer Prevention
The feet of the PAD patient must be examined at every office visit. The importance of meticulous foot and nail care should be reviewed regularly, including the need for regular foot self-inspection, moisturization of the feet, and use of appropriate footwear. Patients should be educated regarding the symptoms and signs of CLI and advised to seek medical attention should these develop. Patients should be referred for podiatric care when indicated, and the use of diabetic footwear and orthotic devices should be considered for patients with diabetes mellitus, foot deformities, or excessive callous formation.
Prevention of Cardiovascular Events
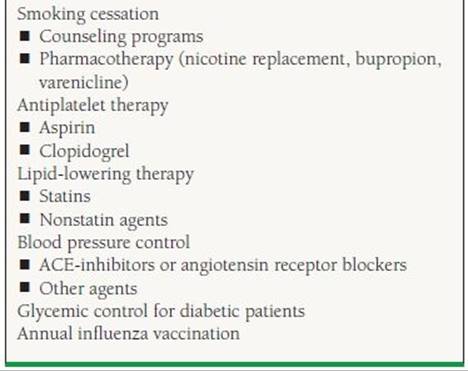
Therapies to prevent MI and stroke are crucial for every patient with PAD, including those without known atherosclerotic carotid or coronary artery disease. While there are little data regarding the benefits of CV risk reduction therapies among asymptomatic patients with an abnormal ABI, the same therapies are generally recommended for these PAD patients. Elements of a risk reduction program for the PAD patient are shown in Table 50.4 and discussed in detailed in both the American College of Cardiology/American Heart Association (ACC/AHA) and the Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC-II) guidelines.16,21,21a Cardiovascular risk reduction therapies are underprescribed among patients with PAD and in comparison to those with coronary artery disease.22,23
TABLE
50.4 Therapies to Prevent Cardiovascular Events Among Patients with PAD
Smoking Cessation
It is well established that smoking cessation decreases the risk of MI, stroke, and malignancy and improves survival. Among patients with PAD, smoking cessation has been shown (in epidemiologic studies) to lower the risk of amputation, need for revascularization, and bypass graft failure and to improve overall survival.24–27 Asking patients about their smoking status at every visit and counseling them to quit is the first step in the management of PAD. Pharmacotherapy for smoking cessation such as nicotine replacement, bupropion, and varenicline should be considered and offered. The use of varenicline, a partial α4β nicotinic acetylcholine receptor agonist, has shown to be effective in smokers with cardiovascular disease, including PAD.28 Referring patients to a formal smoking cessation program, when available, may be helpful.
Antiplatelet Agents
Clinical trials and meta-analyses have shown that antiplatelet medications like aspirin are efficacious in secondary prevention for coronary artery disease and carotid disease. Antiplatelet therapy reduces the incidence of major vascular events among symptomatic PAD patients by approximately 25% as shown in a large meta-analysis.29 Based upon these data, both the ACC/AHA and TASC II PAD guidelines recommend antiplatelet therapy with either aspirin or clopidogrel for patients with PAD.16,21,21a However, the optimal agent and dose of antiplatelet therapy for patients with PAD have not been definitively established. Data from the prevention of progression of arterial disease and diabetes (POPADAD) trial and Aspirin for Asymptomatic Atherosclerosis (AAA) trial demonstrated a lack of benefit of low-dose aspirin (100 mg/d) for prevention of cardiovascular events among patients with asymptomatic PAD and borderline abnormal ABI.30,31 The CLIPS trial demonstrated a significant benefit of aspirin 100 mg/d versus placebo among patients with symptomatic or asymptomatic PAD with mean ABI = 0.63, although this study was stopped early due to poor recruitment and had some methodologic flaws.32 A recently published meta-analysis of trials of aspirin for symptomatic and asymptomatic PAD patients has shown a need for additional studies to confirm the benefit of aspirin for CV risk reduction in PAD patients.33When clopidogrel was compared with aspirin among high-risk patients with atherosclerotic vascular disease in the CAPRIE study (Clopidogrel versus Aspirin in Patients at Risk of Ischemic Events),33 there was a small but incremental benefit of clopidogrel, particularly among the subgroup of symptomatic PAD patients.34 A focused update of the 2005 ACC/AHA PAD guidelines has been published that addresses these new antiplatelet data.21a Antiplatelet therapy with either aspirin or clopidogrel is recommended for patients with lower extremity PAD for reduction of cardiovascular events.21a Given a lack of compelling efficacy data, dual antiplatelet therapy is not recommended for PAD patients unless there is another compelling indication such as recent acute coronary syndrome or coronary stenting.35
Warfarin
Warfarin in combination with antiplatelet medication was compared with antiplatelet medication alone in PAD patients in the WAVE trial (Warfarin Antiplatelet Vascular Evaluation). The combination was not more beneficial but was associated with an increased risk of significantly life-threatening bleeding.36 Based upon these data, warfarin is not recommended unless there is another compelling indication for its use (e.g., venous thromboembolism or atrial fibrillation).16,21a
Lipid-Lowering Therapy
All patients with PAD should be treated with an HMG coenzyme-A reductase inhibitor (statin), unless there is a compelling contraindication. The Heart Protection Study randomized high-risk and relatively normocholesterolemic patients (total cholesterol ≥135 mg/dL) to simvastatin and placebo, including 4,588 patients with lower extremity PAD.37 Statins were associated with a 13% reduction in all-cause mortality, 17% reduction in cardiovascular mortality, and 24% reduction in first major vascular event.37 Among the subset of PAD patients, randomization to simvastatin was associated with a 20% reduction in noncoronary revascularization procedures.38 Statin therapy has been shown to improve claudication symptoms and slowed the rate of functional decline among patients with PAD.39,40 The 2005 ACC/AHA PAD guidelines recommend statin therapy to a goal low-density lipoprotein (LDL) cholesterol < 100 mg/dL for PAD patients (Class I, level of evidence [LOE] B) with an option to target cholesterol to <70 mg/dL for very high risk patients (Class IIa, LOE B). For PAD patients with low highdensity lipoprotein (HDL) cholesterol and/or significantly elevated triglycerides, additional lipid-lowering agents (e.g., niacin and fibrates) may be considered, but generally as adjunctive therapy to statins.
Blood Pressure Control
Current practice guidelines recommend antihypertensive therapy for hypertensive PAD patients to achieve a goal of <140/90 mm Hg for nondiabetic patients or of <130/80 mm Hg for PAD patients with concomitant diabetes mellitus or chronic renal disease.16 Clinical trials have further established the benefit of more intensive blood pressure control, particularly with the angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers. The HOPE trial included 4,046 patients with symptomatic PAD among its population of patients with atherosclerotic vascular disease or diabetes and other risk factors and compared ramipril verses placebo for CV risk reduction among relatively normotensive patients. The trial showed a 22% reduction in major CV events among patients randomized to ramipril.41The ONTARGET trial established a role for angiotensin receptor blockers (telmisartan) as an alternative to ACE inhibitors in the management of CV risk in patients with atherosclerotic vascular disease, including PAD.42 In this study, the combination of ramipril plus telmisartan showed no incremental benefit and increased the risk of significant adverse events including hypotension and hyperkalemia compared to the individual therapies. Intensive blood pressure control among diabetic patients with PAD is particularly important. The ABCD trial compared intensive blood pressure control to standard therapy among diabetic patients using nisoldipine or enalapril. In this trial, intensive BP control essentially eliminated the inverse relationship of ABI and adverse cardiovascular events43 (Fig. 50.4).
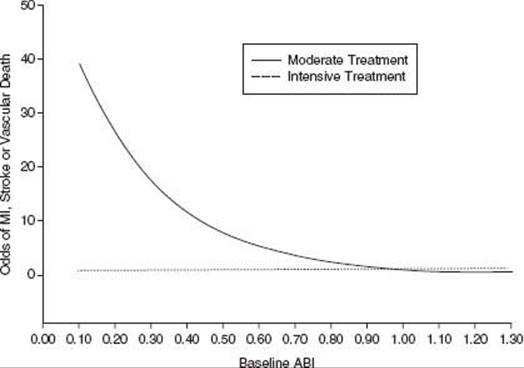
FIGURE 50.4 Intensive blood pressure control reduces risk of cardiovascular events among diabetic patients with PAD: Data from the ABCD trial. Intensive blood pressure control with nisoldipine or enalapril (dashed line) essentially eliminated the relationship of reduced ABI and risk of a major cardiovascular event that was seen in the standard therapy arm (solid line). (Reproduced from Mehler PS, Coll JR, Estacio R, et al. Intensive blood pressure control reduces the risk of cardiovascular events in patients with peripheral arterial disease and type 2 diabetes. Circulation. 2003;107(5):753–756, with permission.)
Beta-Blockers and PAD
Beta-blockers are important medications for PAD patients with prior MI, arrhythmias, and congestive heart failure as well as to prevent cardiovascular events among those undergoing major noncardiac surgery. They may also be used as a first- or second-line agent for blood pressure control. Historically, physicians were taught that beta-blockers may worsen claudication. It has recently been established that beta-blockers can be safely prescribed to patients with symptomatic or asymptomatic PAD. In a recently published meta-analysis of 11 randomized controlled trials, beta-blocker therapy did not worsen claudication in patients with PAD and had no significant effect on pain-free walking distance compared with placebo.44
Glycemic Control in Diabetic Patients with PAD
Epidemiologic data have demonstrated an increased risk of lower extremity amputation among diabetic patients with PAD with poor glycemic control and higher HgB A1C levels.45 Intensive glycemic control has been shown to reduce the incidence of microvascular events among diabetic patients, but its role in prevention of macrovascular (cardiovascular) events is less established and somewhat controversial.46–50
It is recommended that diabetic patients with PAD be managed according to the American Diabetes Association (ADA)/ACC/AHA guidelines for glycemic control and the prevention of cardiovascular events51 (Table 50.5). Diabetic patients with PAD are at increased risk for development of CLI and patient education and meticulous foot care are particularly important in this population of patients.
TABLE
50.5 Key Recommendations from the American Diabetes Association/American College of Cardiology/American Heart Association (ADA/ACC/AHA) Guidelines for Glycemic Control and Prevention of Cardiovascular Events
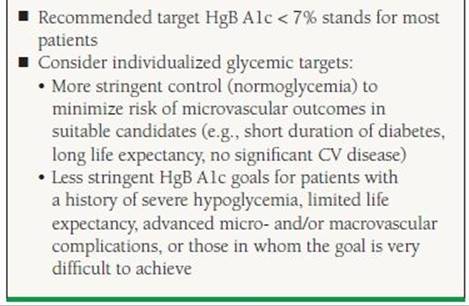
Skyler JS, et al. Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA Diabetes Trials: a position statement of the American Diabetes Association and a Scientific Statement of the American College of Cardiology Foundation and the American Heart Association. J Am Coll Cardiol. 2009;53(3):298–304, with permission from Elsevier.
Therapies to Improve Function and Quality of Life
There are multiple treatments available for improvement of functional capacity and leg symptoms among patients with PAD including exercise training (supervised or unsupervised), pharmacotherapy (cilostazol), and revascularization (surgical or endovascular).
Supervised Exercise Rehabilitation for PAD
Supervised exercise rehabilitation is one of the most effective therapies for PAD but unfortunately is not widely available due to a lack of reimbursement by third-party payers. PAD rehabilitation programs generally consists of supervised exercise with training sessions focused on increasing intervals of treadmill walking with alternating periods of rest when the patient experiences moderately intense claudication. Optimal programs are continued for at least 12 weeks and meet for 30 to 45 minutes at a time at least three times weekly.16 PAD exercise rehabilitation programs have been shown to increase distance to claudication onset by up to 180% along with improvements in exercise performance, physical functioning, and QOL.52 PAD rehabilitation has been shown to be highly cost-effective treatment when compared to catheter-based revascularization53 and has been recommended as a first-line therapy by both major mulitisocietal consensus practice guidelines16,21 as Class I, LOE A.16,21 The efficacy of home-based or unsupervised exercise (walking) programs for PAD has not been as well established, although certainly all patients with PAD with or without claudication should be encouraged to begin a walking program.
Pharmacotherapy for PAD
In the United States, there are two FDA-approved medications for treatment of claudication (pentoxifylline and cilostazol). There are a number of investigational agents that have been and continued to be studied, including recent efforts exploring the use of angiogenic factors and stem cell therapy for the treatment of PAD patients. However, it should be noted that there have been no new agents FDA approved for treatment of claudication since cilostazol in 1999. Pharmacotherapy for claudication is a major area of unmet medical need. Recently, some medications that prevent cardiovascular events among PAD patients, such as statins and ACE inhibitors, have also been shown to have potential benefit in terms of claudication symptoms and walking performance.39,54 A number of nutraceutical agents have been studied for claudication with limited success. The amino acid L-carnitine (especially its propionyl-L-carnitine form) has shown some promise.55
Cilostazol Cilostazol is a phosphodiesterase type III inhibitor. It increases cyclic AMP levels, inhibits platelet aggregation and smooth muscle cell proliferation, and has a weak vasodilator effect. In clinical trials, cilostazol has been shown to increase the maximal walk distance by 50.7% as compared to 24.3% for placebo.56 The use of cilostazol to prevent coronary and superficial femoral artery stent restenosis is an ongoing area of research.57,58 The standard dose of cilostazol is 100 mg twice a day. Dosage reduction should be implemented in the presence of drugs such as ketoconazole and omeprazole due to potential interactions (50 mg tablets also available). The most common side effects of cilostazol are diarrhea, palpitations/arrhythmias, and headache. Cilostazol is contraindicated in patients with congestive heart failure of any severity and carries a black box warning for this patient population. A trial of cilostazol therapy for claudication is given a Class I (LOE A) indication for patients with lifestyle-limiting claudication in the 2005 ACC/AHA PAD guidelines.16
Pentoxifyline Pentoxifyline is a methylxanthine derivative with mechanism of action felt to be related to improvement of blood viscosity. Though there is a long-standing history of its use among patients with claudication, it is not highly efficacious, and it should be used only as a pharmacotherapy option for patients intolerant of cilostazol or those with a contraindication (e.g., congestive heart failure or left ventricular dysfunction).
Revascularization of PAD
A complete discussion of revascularization for PAD patients is beyond the scope of this chapter. The spectrum of PAD symptom severity and indications for revascularization are shown in Figure 50.5. Revascularization is clearly indicated for the patient with acute limb ischemia or chronic limb ischemia. Among claudicants, revascularization should be considered for the patient with significant (i.e., lifestyle- or vocationally limiting) symptoms after a trial of exercise and/or pharmacologic therapy or in cases where there is highly favorable anatomy of endovascular therapy (such as aortoiliac occlusive disease). Revascularization is never indicated as prophylactic therapy in an asymptomatic patient with a low ABI.16 There are very few data to support endovascular therapy over medical therapy and/or supervised exercise training to improve functional outcomes and QOL in patients with intermittent claudication. In the recently published CLEVER trial, among patients with aortoiliac occlusive disease, both supervised exercise therapy and endovascular stenting improved functional outcomes in patients with claudication.59
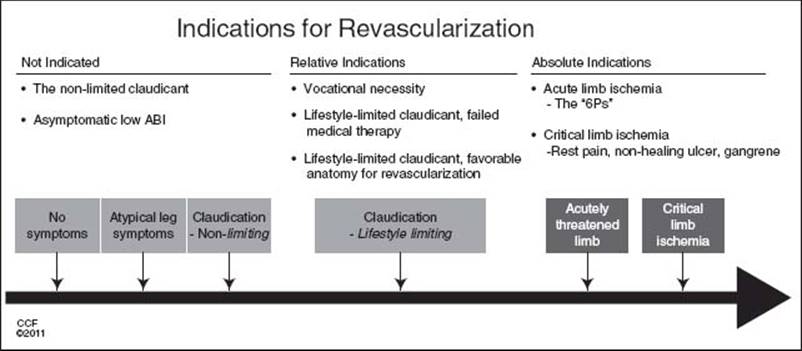
FIGURE 50.5 Indications for revascularization. Most patients with PAD can be managed with medical therapy. Acute and CLI are definite indications for lower extremity revascularization, either endovascular or surgical. In addition, revascularization may be considered for a severely limited PAD patient with stable claudication, particularly if a trial of medical therapy has failed or is unavailable or if the patient has aortoiliac disease that is readily amenable to endovascular treatment. (From Cleveland Clinic Foundation, with permission.)
While open bypass surgery may be necessary in some cases of severe PAD, endovascular therapy has emerged as a first-line approach to revascularization in cases with favorable anatomy, particularly aortoiliac occlusive disease. Endovascular therapy offers the advantage of less severe procedural complications and shorter recovery compared to lower extremity bypass surgery. The durability of endovascular versus surgical revascularization depends upon a number of factors, including anatomic location of disease (aortoiliac disease having better long-term patency outcomes than revascularization procedures below the inguinal ligament) as well as technical factors such as balloon angioplasty alone versus angioplasty with stenting and choice of surgical conduit (autogenous vein vs. prosthetic). Autogenous vein conduit is associated with improved long-term patency compared with prosthetic grafts.
EDUCATION ABOUT PAD
Increasing awareness about PAD among the public, patients, and health care providers is important. More than 70% of primary care providers in the PARTNERS (PAD Awareness, Risk, and Treatment study) study whose patients were screened were previously unaware of the presence of PAD.2 In addition, in a recent survey of United States households, individuals were far less familiar with PAD than they were with relatively uncommon diseases such as Lou Gehrig’s disease or cystic fibrosis.60 There are many tools available to educate patients about PAD. One excellent source of patient information booklets and fact sheets, as well as health care provider resources, is the PAD Coalition (www.padcoalition. org). Most recently, multispecialty performance measures for providers who care for patients with PAD have been published.61 Performance measures include evaluating patients at risk for PAD with the ABI, smoking cessation counseling, prescribing antiplatelet and lipid-lowering therapies, and referring for supervised exercise training for PAD patients with claudication.37
ACKNOWLEDGMENT
The authors thank Ms. Mariam Khan for her assistance in preparation of this manuscript.
REFERENCES
1. Selvin E, Erlinger TP. Prevalence of and risk factors for peripheral arterial disease in the United States: results from the National Health and Nutrition Examination Survey, 1999–2000. Circulation. 2004;110(6):738–743.
2. Hirsch AT, et al. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286(11):1317–1324.
3. Hiatt WR. Medical treatment of peripheral arterial disease and claudication. N Engl J Med. 2001;344(21):1608–1621.
4. Weitz JI, et al. Diagnosis and treatment of chronic arterial insufficiency of the lower extremities: a critical review. Circulation. 1996;94(11):3026–3049.
5. Valentine RJ, et al. Coronary artery disease is highly prevalent among patients with premature peripheral vascular disease. J Vasc Surg. 1994;19(4):668–674.
6. McFalls EO, et al. Coronary-artery revascularization before elective major vascular surgery. N Engl J Med. 2004;351(27):2795–2804.
7. Klop RB, Eikelboom BC, Taks AC. Screening of the internal carotid arteries in patients with peripheral vascular disease by colour-flow duplex scanning. Eur J Vasc Surg. 1991;5(1):41–45.
8. Cheng SW, et al. Screening for asymptomatic carotid stenosis in patients with peripheral vascular disease: a prospective study and risk factor analysis. Cardiovasc Surg. 1999;7(3):303–309.
9. Steg PG, et al. One-year cardiovascular event rates in outpatients with atherothrombosis. JAMA. 2007;297(11):1197–1206.
10. Resnick HE, et al. Relationship of high and low ankle brachial index to all-cause and cardiovascular disease mortality: the Strong Heart Study. Circulation. 2004;109(6):733–739.
11. McKenna M, Wolfson S, Kuller L. The ratio of ankle and arm arterial pressure as an independent predictor of mortality. Atherosclerosis. 1991;87(2–3):119–128.
12. Newman AB, et al. Ankle-arm index as a marker of atherosclerosis in the Cardiovascular Health Study. Cardiovascular Heart Study (CHS) Collaborative Research Group. Circulation. 1993;88(3):837–845.
13. Zheng ZJ, et al. Associations of ankle-brachial index with clinical coronary heart disease, stroke and preclinical carotid and popliteal atherosclerosis: the Atherosclerosis Risk in Communities (ARIC) Study. Atherosclerosis. 1997;131(1):115–125.
14. Fowkes FG, et al. Ankle brachial index combined with Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA. 2008;300(2):197–208.
15. Diehm C, et al. Mortality and vascular morbidity in older adults with asymptomatic versus symptomatic peripheral artery disease. Circulation. 2009;120(21):2053–2061.
16. Hirsch AT, et al. ACC/AHA 2005 guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): executive summary a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. J Am Coll Cardiol. 2006;47(6):1239–1312.
17. Schneider JR, et al. Functional health and well-being in patients with severe atherosclerotic peripheral vascular occlusive disease. Ann Vasc Surg. 1993;7(5):419–428.
18. Arseven A, et al. Peripheral arterial disease and depressed mood in older men and women. Vasc Med. 2001;6(4): 229–234.
19. McDermott MM, et al. The ankle brachial index is associated with leg function and physical activity: the Walking and Leg Circulation Study. Ann Intern Med. 2002;136(12):873–883.
20. Rose GA. The diagnosis of ischaemic heart pain and intermittent claudication in field surveys. Bull World Health Organ. 1962;27:645–658.
21. Norgren L, et al. Inter-society consensus for the management of peripheral arterial disease. Int Angiol. 2007;26(2):81–157.
21a. Rooke TW, et al. 2011. American College of Cardiology Foundation/American Heart Association Focused Update of the Guideline for the Management of Patients with Peripheral Artery Disease. J Am Coll Cardiol. 2011;58(19):2020–2045.
22. Pande RL, et al. Secondary prevention and mortality in peripheral artery disease: National Health and Nutrition Examination Study, 1999 to 2004. Circulation. 2011;124(1):17–23.
23. Selvin E, Hirsch AT. Contemporary risk factor control and walking dysfunction in individuals with peripheral arterial disease: NHANES 1999–2004. Atherosclerosis. 2008;201(2):425–433.
24. Lassila R, Lepantalo M. Cigarette smoking and the outcome after lower limb arterial surgery. Acta Chir Scand. 1988;154(11–12): 635–640.
25. Jonason T, Bergstrom R. Cessation of smoking in patients with intermittent claudication. Effects on the risk of peripheral vascular complications, myocardial infarction and mortality. Acta Med Scand. 1987;221(3):253–260.
26. Willigendael EM, et al. Smoking and the patency of lower extremity bypass grafts: a meta-analysis. J Vasc Surg. 2005; 42(1):67–74.
27. Faulkner KW, House AK, Castleden WM. The effect of cessation of smoking on the accumulative survival rates of patients with symptomatic peripheral vascular disease. Med J Aust. 1983;1(5):217–219.
28. Rigotti NA, et al. Efficacy and safety of varenicline for smoking cessation in patients with cardiovascular disease: a randomized trial. Circulation. 2010;121(2):221–229.
29. AntithromboticTrialists’Collaboration. Collaborative metaanalysis of randomised trials of antiplatelet therapy for prevention of death, myocardial infarction, and stroke in high risk patients. BMJ. 2002;324(7329):71–86.
30. Belch J, et al. The prevention of progression of arterial disease and diabetes (POPADAD) trial: factorial randomised placebo controlled trial of aspirin and antioxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ. 2008;337:a1840.
31. Fowkes FG, et al. Aspirin for prevention of cardiovascular events in a general population screened for a low ankle brachial index: a randomized controlled trial. JAMA. 2010;303(9):841–848.
32. Catalano M, Born G, Peto R. Prevention of serious vascular events by aspirin amongst patients with peripheral arterial disease: randomized, double-blind trial. J Intern Med. 2007;261(3):276–284.
33. Berger JS, et al. Aspirin for the prevention of cardiovascular events in patients with peripheral artery disease: a meta-analysis of randomized trials. JAMA. 2009;301(18):1909–1919.
34. CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). Lancet. 1996;348(9038):1329–1339.
35. Cacoub PP, et al. Patients with peripheral arterial disease in the CHARISMA trial. Eur Heart J. 2009;30(2):192–201.
36. Anand S, et al. Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med. 2007;357(3):217–227.
37. Heart Protection Study Collaborative Group. MRC/BHF Heart Protection Study of cholesterol lowering with simvastatin in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360(9326):7–22.
38. Heart Protection Study Collaborative Group. Randomized trial of the effects of cholesterol-lowering with simvastatin on peripheral vascular and other major vascular outcomes in 20,536 people with peripheral arterial disease and other high-risk conditions. J Vasc Surg.2007;45(4):645–654; discussion 653–654.
39. Mohler ER III, Hiatt WR, Creager MA. Cholesterol reduction with atorvastatin improves walking distance in patients with peripheral arterial disease. Circulation. 2003;108(12):1481–1486.
40. Giri J, et al. Statin use and functional decline in patients with and without peripheral arterial disease. J Am Coll Cardiol. 2006;47(5):998–1004.
41. Yusuf S, et al. Effects of an angiotensin-converting-enzyme inhibitor, ramipril, on cardiovascular events in high-risk patients. The Heart Outcomes Prevention Evaluation Study Investigators. N Engl J Med. 2000;342(3):145–153.
42. Dominiak M. Commentary to the article: ONTARGET Investigators, Yusuf S, Teo KK, Pogue J, et al. Telmisartan, ramipril, or both in patients at high risk for vascular events. N Engl J Med. 2008;358:1547–59. Kardiol Pol. 2008;66(6):705–706; discussion 707.
43. Mehler PS, et al. Intensive blood pressure control reduces the risk of cardiovascular events in patients with peripheral arterial disease and type 2 diabetes. Circulation. 2003;107(5):753–756.
44. Radack K, Deck C. Beta-adrenergic blocker therapy does not worsen intermittent claudication in subjects with peripheral arterial disease. A meta-analysis of randomized controlled trials. Arch Intern Med. 1991;151(9):1769–1776.
45. Resnick HE, et al. Incidence of lower-extremity amputation in American Indians: the Strong Heart Study. Diabetes Care. 2004;27(8):1885–1891.
46. Nathan DM, et al. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N Engl J Med. 2005;353(25):2643–2653.
47. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352(9131):837–853.
48. Dormandy JA, et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised controlled trial. Lancet. 2005;366(9493):1279–1289.
49. Patel A, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560–2572.
50. Gerstein HC, et al. Effects of intensive glucose lowering in type 2 diabetes. N Engl J Med. 2008;358(24):2545–2559.
51. Skyler JS, et al. Intensive glycemic control and the prevention of cardiovascular events: implications of the ACCORD, ADVANCE, and VA Diabetes Trials: a position statement of the American Diabetes Association and a Scientific Statement of the American College of Cardiology Foundation and the American Heart Association. J Am Coll Cardiol. 2009;53(3):298–304.
52. Gardner AW, Poehlman ET. Exercise rehabilitation programs for the treatment of claudication pain. A meta-analysis. JAMA. 1995;274(12):975–980.
53. Treesak C, et al. Cost-effectiveness of exercise training to improve claudication symptoms in patients with peripheral arterial disease. Vasc Med. 2004;9(4):279–285.
54. Ahimastos AA, et al. Brief communication: ramipril markedly improves walking ability in patients with peripheral arterial disease: a randomized trial. Ann Intern Med. 2006;144(9):660–664.
55. Hiatt WR. Carnitine and peripheral arterial disease. Ann N Y Acad Sci. 2004;1033:92–98.
56. Pande RL, et al. A pooled analysis of the durability and predictors of treatment response of cilostazol in patients with intermittent claudication. Vasc Med. 2010;15(3):181–188.
57. Douglas JS Jr, et al. Coronary stent restenosis in patients treated with cilostazol. Circulation. 2005;112(18):2826–2832.
58. Soga Y, et al. Efficacy of cilostazol after endovascular therapy for femoropopliteal artery disease in patients with intermittent claudication. J Am Coll Cardiol. 2009;53(1):48–53.
59. Murphy TP, Cutlip DE, Regensteiner JG, et al. Supervised exercise versus primary stenting for claudication resulting from aortoiliac peripheral artery disease: six-month outcomes from the claudication: exercise versus endoluminal revascularization (CLEVER) study. Circulation. 2012;125(1):130–139.
60. Hirsch AT, et al. Gaps in public knowledge of peripheral arterial disease: the first national PAD public awareness survey. Circulation, 2007;116(18):2086–2094.
61. Olin JW, et al. ACCF/AHA/ACR/SCAI/SIR/SVM/SVN/SVS 2010 performance measures for adults with peripheral artery disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on performance measures, the American College of Radiology, the Society for Cardiac Angiography and Interventions, the Society for Interventional Radiology, the Society for Vascular Medicine, the Society for Vascular Nursing, and the Society for Vascular Surgery (Writing Committee to Develop Clinical Performance Measures for Peripheral Artery Disease). Circulation. 2010;122(24):2583–2618.
QUESTIONS AND ANSWERS
Questions
1. A 66-year-old man comes to see you for evaluation of severe bilateral buttock and thigh discomfort with exertion. He is a current tobacco smoker and underwent coronary artery bypass grafting (CABG) 5 years ago. He has had long-standing difficulties with low back pain, and he carries a diagnosis of mild lumbar canal stenosis. Your medical assistant measures ABIs in the office: right leg ankle–brachial index (ABI) = 1.01 and left leg ABI = 1.02. What is the most appropriate next step?
a. MRI of the lumbar spine
b. Computed tomographic angiography (CTA) of the aorta and lower extremities
c. Duplex arterial studies
d. Repeat ABIs after treadmill exercise
e. Measure toe–brachial indices (TBIs) bilaterally
2. A 68-year-old man with a history of uncontrolled diabetes mellitus, hypertension, and advanced chronic kidney disease requiring hemodialysis is referred to you for evaluation of a nonhealing ulcer of the left heal. All of the following are the appropriate next steps except:
a. Sharp debridement of the ulcer
b. Probe the ulcer
c. Plain radiograph of the foot to rule out osteomyelitis
d. Perform ABI with pulse volume recording (PVR) tracing
e. Check metabolic panel, lipids, and HbA1c
2. The ABI is done on the above patient. His right ABI is 1.54 and left ABI is 0.63. How would you interpret this test? Each of the following is true except:
a. ABI is not reliable as the patient has non-compressible arteries.
b. ABI is suggestive of calcified vessel and cannot be interpreted.
c. Right ABI is normal. Left ABI is abnormal.
d. Right ABI is not diagnostic in this patient and he will need other testing.
e. Measuring the TBI will be helpful.
3. A 58-year-old woman with long-standing bilateral calf claudication, which has been medically managed, reports progression of pain in her right calf and foot with less and less exertion. She also has intense burning in her right foot, occurring at night. These symptoms have developed over the past 4 weeks. The patient says she can help her right foot burning at night by dangling the foot over the side of the bed. What is the most likely diagnosis?
a. Phlegmasia cerulea dolens from proximal deep vein thrombosis
b. Restless leg syndrome
c. Critical limb ischemia (CLI)
d. Acute arterial embolism
e. Painful peripheral neuropathy
4. A 72-year-old man with multiple cardiovascular risk factors (former smoker, diabetes mellitus, hypertension, hyperlipidemia) presents with pain in calves after walking for two blocks. After resting for 5 minutes, he can resume his walk. His ABI in the right leg is 0.78 and left leg is 0.83. His medications are aspirin 162 mg/d, lisinopril, pioglitazone, and simvastatin. His blood pressure is 130/80 mm Hg, HbA1c of 7.2, and LDL is 66 mg/dL. Which of the following is the next step?
a. Refer to supervised exercise rehabilitation program and prescribe a trial of cilostazol.
b. Clopidogrel should be added.
c. Warfarin should be added if the risk of bleeding is acceptable.
d. Schedule arteriography and anticipated bilateral superficial femoral artery stenting.
e. The patient should be started on insulin therapy.
5. A 68-year-old woman is diagnosed with peripheral artery disease (PAD) on routine screening with ABI. She is a former heavy smoker who suffers from hypertension, congestive heart failure with mildly reduced left ventricular function, and hyperlipidemia. The right leg ABI is 0.88 and the left leg ABI is 0.82. She is currently taking aspirin, metoprolol, lisinopril, and atorvastatin. She has recently quit smoking after receiving the report of her ABIs. She was started on cilostazol by her primary care physician. She visits you for a second opinion. Which of the following is the most appropriate next step?
a. The patient should be warned of the side effects of cilostazol, including postural hypotension and constipation.
b. Cilostazol is a reasonable FDA-approved option for medical treatment of PAD and should be continued.
c. Schedule the patient for lower extremity angiogram and possible percutaneous revascularization.
d. Stop cilostazol but continue remainder of medical regimen.
e. Tell the patient to continue cilostazol as it may prevent cardiovascular events.
6. A 72-year-old man with known PAD and a history of prior tobacco use and diabetes mellitus is admitted for intense right calf and foot pain and progressive gangrene of his right great toe for the last month. Right leg ABI is 0.33 and left leg ABI is 0.73. What is the next best step in managing his symptoms?
a. Begin intravenous heparin followed by coumadin.
b. Toe amputation
c. Add cilostazol to the medical regimen.
d. Arterial duplex or CTA examination
e. Arterial flow pump
7. A 26-year-old woman and avid cyclist complains of increasing fatigue in her left thigh after bicycling for <1 hour and has to slow down. Symptoms resolve within minutes of slowing down or stopping. She has never smoked tobacco and has no chronic medical conditions and otherwise feels well. Her resting vascular examination is normal. What is the most likely vascular diagnosis?
a. Atherosclerotic PAD
b. Coarctation of aorta
c. Neurologic claudication
d. External iliac endofibrosis
e. Vasculitis
Answers
1. Answer D: This patient has multiple risk factors for PAD. While his symptoms may be consistent with intermittent claudication (particularly aortoiliac occlusive disease), lumbar canal stenosis could also be contributing (pseudoclaudication). Normal ABIs at rest do not rule out a diagnosis of PAD. In this case, repeat ABIs after treadmill exercise are indicated to establish the diagnosis. In the setting of PAD, the postexercise ABIs would be expected to significantly fall. Duplex ultrasound and CTA are not needed to diagnose PAD but may be useful if revascularization is planned. The MRI of the spine could be performed to evaluate the severity of spinal stenosis if the patient does not have significant fall in ABIs with exercise and reproduction of symptoms. TBIs are most helpful to diagnose PAD when ABIs are not interpretable due to noncompressible vessels (i.e., resting ABI > 1.4).
2. Answer A: This patient has multiple PAD risk factors and it is important to first assess the circulation and severity of PAD. Vascular physiologic testing including the ABI with PVR tracings or Doppler waveforms should be obtained to rule out ischemia as a contributor to this nonhealing wound. Debriding the ulcer with compromised perfusion can lead to poor wound healing and increased risk of infection and amputation and should not be done until PAD status is known. Gently probing the ulcer to assess its depth should be done routinely in the evaluation of a wound. In this case, circulation should be first restored either by angioplasty or by bypass surgery before surgical debridement of ischemic ulcer. A plain radiograph may be helpful to assess for osteomyelitis in this chronic wound. Assessment of control cardiovascular risk factors is an important component of PAD care.
3. Answer C: The ABI of the right leg is not interpretable due to noncompressible vessels and is not normal. A noncompressible ABI (>1.4) has been associated with increased cardiovascular risk and a majority of these patients have significant PAD. The left leg ABI is abnormal and consistent with significant PAD, although partially noncompressible vessels can also lead to overestimation of ankle pressure and underestimation of severity of disease in diabetic patients, and it is possible that disease may be more severe than the ABI indicates. In all patients with noncompressible vessels by ABI, the TBI should be measured to establish the diagnosis of PAD. In this case, segmental PVR tracings or Doppler waveforms, including tracings at the ankle, metatarsal, and digits would be helpful along with TBIs.
4. Answer C: This patient has known PAD that has progressed to the point of ischemic rest pain and CLI. The history of pain worsening with limb elevation and improved with dependency (i.e., dangling the foot over the side of the bed) is very typical for severe PAD/CLI. In this patient, repeat ABI measurement and expedient evaluation for revascularization are indicated.
5. Answer A: Supervised exercise training is the most cost-effective first-line treatment for management of claudication in the PAD patient. A trial of pharmacotherapy with cilostazol is also reasonable and recommended by the PAD guidelines (ref. ACC/AHA PAD Hirsch 2005). This approach would be first-line therapy with revascularization indicated (particularly for suspected SFA disease) only after medical therapy has failed. There is little evidence to support dual antiplatelet therapy for the PAD patient without concomitant coronary artery disease or stenting, and anticoagulation with warfarin is not superior to aspirin alone and has higher associated bleeding risk. This patient has reasonable diabetes mellitus control (by HgB A1c) on oral medication and thus insulin is not indicated.
6. Answer D: This patient has asymptomatic PAD but also has congestive heart failure and impaired LV systolic function. Cilostazol is approved for use in symptomatic patients to improve symptoms in patients with lower extremity claudication. It is contraindicated in this patient with CHF and LV dysfunction and is also not indicated given her lack of symptoms. There is no evidence that cilostazol improves cardiovascular outcomes among PAD patients. The most common side effects of cilostazol are headache, diarrhea, and palpitations. There is no role for revascularization in this asymptomatic patient with mildly reduced ankle–brachial indices.
7. Answer D: Not all patients with PAD are candidates for revascularization. In this patient, additional imaging is required given his CLI and to assess candidacy for revascularization. Arterial duplex or CTA of the extremities may be useful to diagnose anatomic location and degree of stenotic/occlusive lesions in the legs. Angioplasty or bypass of the proximal arteries (femoral, popliteal, and tibial) alone may not be helpful if the distal runoff is compromised and an imaging study can be used to further assess candidacy for revascularization. While the patient may ultimately require toe amputation, degree of ischemia and candidacy for revascularization must be considered first. Cilostazol is not known to be beneficial for treatment of CLI. An arterial flow pump may be an option for treating CLI and ischemic wound in patients who are not candidates for intervention.
8. Answer D: Atherosclerotic PAD is unlikely in this young woman with no risk factors. In such cases, it is important to think of alternative diagnoses. External iliac artery endofibrosis has been reported most commonly in bicyclists and leads to arterial narrowing and claudication or leg weakness, often at a high workload. This diagnosis should always be considered in a young athlete with claudication, especially a bicyclist. This entity has been traditionally treated with open surgery but can also be managed by endovascular means. Aortic coarctation and vasculitis are unlikely based on the given history and the normal vascular examination. Arterial physiological testing (i.e., ABI at rest and after treadmill exercise reproduces symptoms) and imaging studies can help to make this diagnosis.