George K. Creatsas1 and Maria Creatsas1
(1)
2nd Department of Obstetrics and Gynecology, University of Athens-Aretaieio Hospital, 76 Vas Sofias Ave., Athens, 11528, Greece
George K. Creatsas (Corresponding author)
Email: geocre@aretaieio.uoa.gr
Maria Creatsas
Email: geocre@aretaieio.uoa.gr
A significant number of adolescents present menstrual irregularities during the first 2 gynecological years. The absence of menses is defined as amenorrhea and is classified as primary or secondary. Primary amenorrhea (PA) is the absence of menstruation in 16-year-old girls with developed secondary characteristics or in 14-year-old girls with no presence of secondary characteristics. Secondary amenorrhea is defined as the absence of menstrual period, for 6 months or more, in women who had previously normal or irregular menses [1–4, 11].
The classification of PA, in relation to the etiology of the disease, includes the uterovaginal aplasia or congenital uterovaginal anomalies with obstruction, endocrine disorders, chromosomal anomalies, as well as stress and psychological problems [5–7].
Uterovaginal anomalies with obstruction needs immediate repair following excision or/and reconstruction of the obstructive area (vaginal diaphragm or imperforate hymen).
Endocrine disorders presented with PA include cases of congenital adrenal hyperplasia, hypothalamic or pituitary amenorrhea, the premature ovarian failure, and the polycystic ovarian syndrome (PCOS) [8, 9].
PA due to chromosomal anomalies includes cases of gonadal dysgenesis, hermaphroditism, etc. (Fig.1.1) [1, 2]. Gonadal dysgenesis (streak gonads) may be present either with normal XX and XY karyotypes or abnormal karyotypes. The Turner syndrome (45X0) is usually diagnosed in early childhood because of the well-known phenotypic characteristics (short stature, webbed neck, and low hairline), and therefore many patients do not present for assessment of PA.
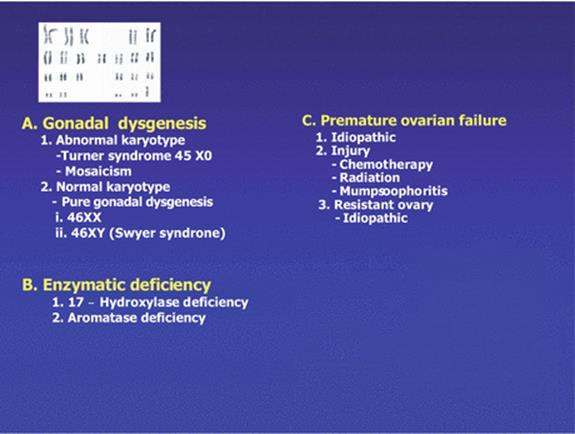
Fig. 1.1
Primary hypogonadism ([2], modified)
Stress and psychological problems are common causes of PA in young girls including cases of athletic amenorrhea.
Another classification, including the relative incidence of PA causes, is presented in Table 1.1 [1–3, 5, 10–14].
Table 1.1
Classification and incidence of PA cases
|
• No breast development and low follicle-stimulating hormone (FSH) (30 % of PA cases) – Constitutional delay (10 %) – Prolactinomas (5 %) – Kallmann syndrome (2 %) – Other central nervous system lesions (3 %) – Stress, weight loss, and anorexia (3 %) – PCOS (3 %) – Congenital adrenal hyperplasia (3 %) – Other reasons (1 %) |
|
• No breast development: high FSH (40 % of PA cases) – 46 XX (15 %) – 46 XY (5 %) – Abnormal (20 %) |
|
• Breast development (30 % of PA) – Mullerian agenesis (10 %) – Androgen insensitivity (9 %) – Vaginal septum (2 %) – Imperforate hymen (1 %) – Constitutional delay (8 %) |
Delayed puberty (DP) is the absence of onset of puberty by >2 SD, later than the average age of menarche. DP is also the absence of menstruation in 13–14-year-old girls who have no secondary sexual characteristic development. The causes of DP are (1) general: constitutional delay of growth and puberty, underweight, and other chronic diseases; (2) gonadal origin (hypergonadotropic hypogonadism): prodromal premature ovarian failure—karyotypically normal, Turner’s syndrome, and pure gonadal dysgenesis; (3) autoimmune oophoritis; (4) 17,20-desmolase deficiency; (5) radiation or chemotherapy; (6) FSH receptor mutation; (7) galactosemia; (8) congenital hypogonadotropic hypogonadism; (9) gonadotropin deficiency; and (10) hypothalamic/pituitary lesions [3, 5, 11–14].
Patient’s evaluation includes information taken by the clinical history, gynecological and physical examination, X-rays, ultrasonography (US), the hormonal profile of the patient, and rarely endoscopic evaluation (Fig. 1.2).
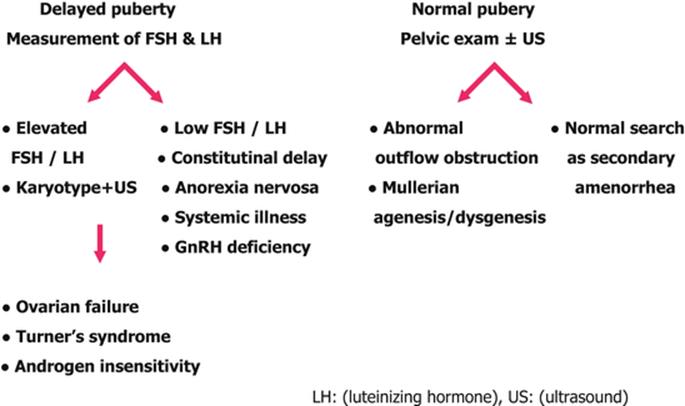
Fig. 1.2
Approach to adolescent PA [3, 4, 11, 13]
1.1 Case Presentations
1.
2.
3.
4.
5.
6.
7.
8.
Each patient should be individually treated, avoiding unnecessary tests and overtreatment. In cases presented with obstruction of the genital route immediate surgery is advised. If hormonal treatment is scheduled, the low-dose, new-generation 17β-estradiol COCs are recommended. Explanation, reassurance, and emotional support are necessary tools for the management of the disease, as in many cases treatment is advisable for a long period of time.
References
1.
ASRM Practice Committee (2008) Current evaluation of amenorrhea. Fertil Steril 90:S219–S225
2.
American Society for Reproductive Medicine (ASRM) (2006) The practice committee of the ASRM. Fertil Steril 86(Suppl 4):S148–S155
3.
Creatsas G, Deligeoroglou E, Christopoulos P (2010) Creation of a neovagina after Creatsas modification of Williams vaginoplasty for the treatment of 200 patients with Mayer – Rokitansky – Kyster – Hauser syndrome. Fertil Steril 94(5):1848–1852PubMedCrossRef
4.
Diaz A, Laufer MR, Breech LL (2006) Menstruation in girls and adolescents: using the menstrual cycle as a vital sign. Pediatrics 118(5):2245–2250PubMedCrossRef
5.
Deligeoroglou E, Tsimaris P (2010) Menstrual disturbances in puberty. Best Pract Res Clin Obstet Gynaecol 24(2):157–171PubMedCrossRef
6.
Hickey M, Balen A (2003) Menstrual disorders in adolescence: investigation and management. Hum Reprod Update 9(5):493–504PubMedCrossRef
7.
Patel SS, Bamigboye V (2007) Hyperprolactinaemia. J Obstet Gynaecol 9(5):493–504
8.
Deligeoroglou E, Tsimaris P, Deliveliotou A, Christopoulos P, Creatsas G (2006) Μenstrual disorders during adolescence. Pediatr Endocrinol Rev 3(Suppl 1):150–159PubMed
9.
Slap GB (2003) Menstrual disorders in adolescence. Best Pract Res Clin Obstet Gynaecol 17(1):75–92PubMedCrossRef
10.
Creatsas G (1996) Hormone replacement therapy in gonadal dysgenesis cases. Gynecol Endocrinol 10:13–14CrossRef
11.
Creatsas G, Deligeoroglou E, Cardamakis E, Aravantinos D (1994) XY pure gonadal (testicular) dysgenesis: brief report of a familiar case. Adolesc Pediatr Gynecol 7:34–37CrossRef
12.
Creatsas G, Salakos N, Averkiou M, Miras K, Aravantinos D (1992) Endocrinological profile of oligomenorrheic strenuously exercising adolescents. Int J Gynecol 38:215–221CrossRef
13.
Deligeoroglou E, Athanasopoulos N, Tsimaris P, Dimopoulos KD, Vrachnis N, Creatsas G (2010) Evaluation and management of adolescent amenorrhea. Ann NY Acad Sci 1205:23–32PubMedCrossRef
14.
Deligeoroglou E, Karountzos V, Creatsas G (2013) Abnormal uterine bleeding and dysfunctional uterine bleeding in pediatric and adolescent gynecology. Gynecol Endocrinol 29(1):74–78PubMedCrossRef
© Springer International Publishing Switzerland 2014