Suryakanth R. Gurudu, MD, FACG, FASGE
![]() What percentage of primary gastrointestinal tumors originate in the small bowel?
What percentage of primary gastrointestinal tumors originate in the small bowel?
Less than 5%.
![]() What clinical conditions are associated with an increased risk of small bowel tumors?
What clinical conditions are associated with an increased risk of small bowel tumors?
• Crohn’s disease of the small intestine (adenocarcinoma)
• Familial adenomatous polyposis (adenoma and adenocarcinoma, particularly periampullary)
• Celiac sprue (lymphoma and adenocarcinoma)
• AIDS (non-Hodgkin’s lymphoma and Kaposi’s sarcoma)
• Neurofibromatosis (leiomyoma and adenocarcinoma)
• Ileal conduit or ileocystoplasty (adenocarcinoma)
• Ileostomy after colectomy (adenocarcinoma at ileocutaneous junction)
• Immunoproliferative small intestine disease (non-Hodgkin’s lymphoma)
• Nodular lymphoid hyperplasia (non-Hodgkin’s lymphoma)
![]() What is the most common benign small bowel tumor?
What is the most common benign small bowel tumor?
Adenoma. Followed in descending order by leiomyoma, Brunner’s gland hamartoma, and lipoma. As in the colon, adenomas of the small bowel are considered premalignant.
![]() What is the most common malignant small bowel tumor?
What is the most common malignant small bowel tumor?
Adenocarcinoma. Followed in descending order by carcinoid, lymphoma, and leiomyosarcoma.
![]() What is the most common presentation of malignant periampullary tumors?
What is the most common presentation of malignant periampullary tumors?
Jaundice is seen in up to 80% of cases.
![]() What is the most common clinical presentation of benign small bowel tumors?
What is the most common clinical presentation of benign small bowel tumors?
While most remain asymptomatic, mechanical small bowel obstruction, usually related to luminal constriction or intussusception, is the most common clinical presentation.
![]() What nongastrointestinal malignancy has the highest rate of metastasis to the small bowel?
What nongastrointestinal malignancy has the highest rate of metastasis to the small bowel?
Melanoma.
![]() Which benign small bowel tumor has the highest propensity for malignant change?
Which benign small bowel tumor has the highest propensity for malignant change?
Villous adenoma. They are often sessile, located in the second portion of the duodenum and 40%–45% have undergone malignant degeneration at the time of diagnosis.
![]() What is the most common cause of intussusception in adults?
What is the most common cause of intussusception in adults?
Benign small bowel tumors. Lipomas are the leading cause.
![]() Where are lipomas of the small intestine most often located?
Where are lipomas of the small intestine most often located?
Ileum.
![]() What is the initial therapy of choice for small bowel adenomas?
What is the initial therapy of choice for small bowel adenomas?
Endoscopic mucosal resection (EMR) is safe and effective; however, the presence of a villous adenoma or the presence of malignant changes on biopsy warrants surgical resection. The size and sessile nature of most villous adenomas make complete resection by endoscopic methods almost impossible. High rates of cancerous transformation also make surgery a preferred option.
![]() What is the most appropriate treatment of small bowel adenomas that cannot be resected endoscopically?
What is the most appropriate treatment of small bowel adenomas that cannot be resected endoscopically?
Laparotomy with segmental resection.
![]() What symptoms are most commonly produced by duodenal villous adenomas?
What symptoms are most commonly produced by duodenal villous adenomas?
Most symptomatic duodenal villous adenomas are 3 cm or more in diameter. The usual clinical presentations include partial gastric outlet obstruction, pancreatitis, bleeding, and obstructive jaundice.
![]() What is the leading cause of cancer death in patients who have undergone proctocolectomy for familial adenomatous polyposis?
What is the leading cause of cancer death in patients who have undergone proctocolectomy for familial adenomatous polyposis?
Adenocarcinoma of the proximal small bowel.
![]() True/False: Endoscopic surveillance of the upper gastrointestinal tract is indicated in individuals with familial adenomatous polyposis.
True/False: Endoscopic surveillance of the upper gastrointestinal tract is indicated in individuals with familial adenomatous polyposis.
True.
![]() What is the diagnostic test of choice in the evaluation of patients with a suspected small bowel tumor?
What is the diagnostic test of choice in the evaluation of patients with a suspected small bowel tumor?
CT or MR enterography; particularly in patients with obstructive symptoms. Capsule endoscopy and balloon-assisted enteroscopy may play a complementary role in the evaluation.
![]() Which benign small bowel tumor has the highest predilection for severe gastrointestinal bleeding?
Which benign small bowel tumor has the highest predilection for severe gastrointestinal bleeding?
Gastrointestinal stromal tumor (GIST). As these tumors grow, they can undergo necrosis and bleeding which is sometimes severe.
![]() What radiographic or endoscopic feature is commonly seen in GIST?
What radiographic or endoscopic feature is commonly seen in GIST?
Central ulceration of the lesion may be seen as umbilication on barium radiograph or endoscopy.
![]() What is the cell of origin of a GIST?
What is the cell of origin of a GIST?
The interstitial cell of Cajal, an intestinal pacemaker cell.
![]() What is the most common location for a GIST?
What is the most common location for a GIST?
Stomach followed by small bowel.
![]() What endoscopic ultrasound (EUS) findings are suggestive of a benign natural history of a GIST?
What endoscopic ultrasound (EUS) findings are suggestive of a benign natural history of a GIST?
Regular margins, tumor size less than 3 cm, and a homogeneous echogenicity pattern. Presence of cystic spaces and irregular margins predict malignant potential.
![]() What is the therapeutic agent of choice for unresectable or metastatic GIST?
What is the therapeutic agent of choice for unresectable or metastatic GIST?
Imatinib.
![]() True/False: Peutz–Jeghers syndrome affects the small bowel.
True/False: Peutz–Jeghers syndrome affects the small bowel.
True. Patients with this syndrome develop hamartomatous polyps throughout the gut. These polyps are especially common in the jejunum. Malignant degeneration can occur but is rare.
![]() Which small bowel malignancy has the slowest rate of growth and metastasis?
Which small bowel malignancy has the slowest rate of growth and metastasis?
Carcinoid. The average time from onset of symptoms to death from metastases is 9 years.
![]() What organs are most frequently involved by metastases from small bowel carcinoid tumors?
What organs are most frequently involved by metastases from small bowel carcinoid tumors?
Liver, bone (especially bones of the orbit and the eye itself), female breast, and ovary.
![]() How do small bowel carcinoid tumors lead to intestinal ischemia?
How do small bowel carcinoid tumors lead to intestinal ischemia?
Spread of disease into mesenteric and celiac lymph nodes produces encasement of the mesenteric artery causing ischemia and eventually small bowel infarction. This is a surprisingly frequent cause of death with small bowel carcinoids.
![]() Malignant carcinoids are most commonly found in which portion of the small bowel?
Malignant carcinoids are most commonly found in which portion of the small bowel?
Forty-four percent of all gastrointestinal carcinoids arise in the small bowel. The ileum is the most frequent location for gastrointestinal carcinoids.
![]() What is the most important factor that influences whether a carcinoid tumor is metastatic?
What is the most important factor that influences whether a carcinoid tumor is metastatic?
Size of the primary lesion. Metastasis is found in only 6% of tumors less than 1 cm in diameter. Conversely, tumors over 2 cm have metastases in over 80% of cases.
![]() What is the surgery of choice for an appendiceal carcinoid tumor more than 2 cm in size?
What is the surgery of choice for an appendiceal carcinoid tumor more than 2 cm in size?
Right hemicolectomy is appropriate for tumor size more than 2 cm, extension into muscularis propria, or evidence of lymph node metastasis. Appendectomy alone is adequate for tumor size <2 cm in size. Appendiceal carcinoids are often found incidentally at the time of appendectomy and have the best prognosis of all types of carcinoids.
![]() True/False: Small bowel carcinoids commonly present with gastrointestinal bleeding.
True/False: Small bowel carcinoids commonly present with gastrointestinal bleeding.
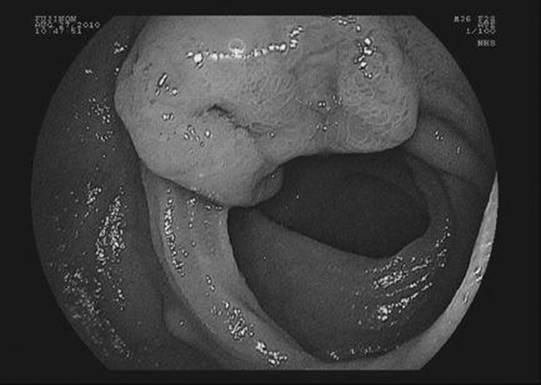
Figure 23-1 See also color plate.
False. Gastrointestinal bleeding from ulcerated tumors as shown in the figure is uncommon. Intermittent obstructive symptoms are more common. Presentation with the carcinoid syndrome is rare.
![]() What are the most common symptoms of carcinoid syndrome?
What are the most common symptoms of carcinoid syndrome?
Flushing, diarrhea, and abdominal pain. Asthma, pellagra, and cardiac valvular lesions are uncommon.
![]() When do patients with small bowel carcinoid tumors develop the carcinoid syndrome?
When do patients with small bowel carcinoid tumors develop the carcinoid syndrome?
Typically only when hepatic metastasis is present. Even with hepatic lesions, 30%–50% of patients with carcinoid tumors do not develop the carcinoid syndrome.
![]() What laboratory test can be used to diagnose carcinoid syndrome?
What laboratory test can be used to diagnose carcinoid syndrome?
Urinary 5-hydroxyindoleacetic acid (HIAA) level. Levels greater than 20 mg in 24 hours are diagnostic.
![]() When do 5-HIAA levels elevate in carcinoid tumors?
When do 5-HIAA levels elevate in carcinoid tumors?
5-HIAA is cleared by the liver after the first-pass from the primary tumor. Thus, it is not elevated until hepatic metastases are extensive.
![]() What serotonin-containing foods should be avoided when collecting urine for 24-hour 5-HIAA?
What serotonin-containing foods should be avoided when collecting urine for 24-hour 5-HIAA?
Walnuts, bananas, pecans, butternuts, pineapples, and tomatoes.
![]() What nuclear medicine scans can be used to diagnose carcinoid tumor?
What nuclear medicine scans can be used to diagnose carcinoid tumor?
123I-labeled Tyr3-octreotide (TOCT, a somatostatin analog) or 123I-labeled metaiodobenzylguanidine. These scans take advantage of the large number of somatostatin receptors expressed by most carcinoid tumors.
![]() True/False: Small bowel carcinoid tumors are almost always solitary.
True/False: Small bowel carcinoid tumors are almost always solitary.

Figure 23-2 See also color plate.
False. Multicentric carcinoid tumors, as shown in the Figure 23-2, are seen in up to 33%.
![]() What medical therapy is available for treating the symptoms of carcinoid syndrome?
What medical therapy is available for treating the symptoms of carcinoid syndrome?
Octreotide, a synthetic somatostatin analog, injected subcutaneously in doses of 50–250 µg BID-TID. Symptoms improve in more than 90% of patients; however, disease progression is not altered. If effective, a long-acting depot form may be substituted.
![]() What can be done to prevent carcinoid crisis caused by invasive procedures?
What can be done to prevent carcinoid crisis caused by invasive procedures?
The use of octreotide before invasive procedures is an important step to prevent carcinoid crisis in patients with known carcinoid syndrome. A bolus dose of 250–500 µg should be given subcutaneously 1 to 2 hours before the surgery and followed by an infusion of 50–200 µg/hour during the surgery.
![]() Weight loss is usually most severe in what type of malignant small bowel tumor?
Weight loss is usually most severe in what type of malignant small bowel tumor?
Lymphoma.
![]() What small bowel lymphoma is seen exclusively in underdeveloped countries?
What small bowel lymphoma is seen exclusively in underdeveloped countries?
Immunoproliferative small intestinal disease (IPSID), also known as alpha-chain disease and Mediterranean lymphoma. Microbial colonization of the small bowel is of major etiologic significance in IPSID.
![]() What small bowel tumor should be suspected in a patient with long-standing celiac disease who develops a relapse of symptoms despite strict adherence to a gluten-free diet?
What small bowel tumor should be suspected in a patient with long-standing celiac disease who develops a relapse of symptoms despite strict adherence to a gluten-free diet?
Intestinal lymphoma, which occurs in 7%–12% of patients with long-standing celiac disease. The cells of this secondary lymphoma are of T-cell origin.
![]() What cell type is present in the majority of primary gastrointestinal lymphomas?
What cell type is present in the majority of primary gastrointestinal lymphomas?
B-cell.
![]() List the criteria for the diagnosis of a primary gastrointestinal lymphoma.
List the criteria for the diagnosis of a primary gastrointestinal lymphoma.
• Absence of palpable peripheral lymphadenopathy on initial presentation
• Absence of mediastinal lymphadenopathy on chest radiography
• A normal peripheral blood smear
• At laparotomy, involvement of only the gut and regional lymphadenopathy
• Absence of liver and spleen involvement except by direct spread from a contiguous focus
• • • SUGGESTED READINGS • • •
Oberg K. Gastrointestinal Carcinoid Tumors (Gastrointestinal Neuroendocrine Tumors) and the Carcinoid Syndrome. In: Feldman LS, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran’s Gastrointestinal and Liver disease. Philadelphia, PA: Elsevier; 2010:475-490.
Paski SC, Semrad CE. Small Bowel Tumors. Gastrointest Endosc Clin N Am. 2009;19(3):461-479.