John S. McDonald, MD
Biing-Jaw Chen, MD
Wing-Fai Kwan, MD
Analgesia is the loss or modulation of pain perception. It can be (1) local and affect only a small area of the body, (2) regional and affect a larger portion of the body, or (3) systemic. Analgesia is achieved by the use of hypnosis (suggestion), systemic medication, regional agents, or inhalational agents.
Anesthesia is the total loss of sensory perception and may include loss of consciousness. It is induced by various agents and techniques. In obstetrics, regional anesthesia is accomplished with local anesthetic techniques (epidural, spinal) and general anesthesia with systemic medication and endotracheal intubation.
The terms analgesia and anesthesia are sometimes confused in common usage. Analgesia denotes those states in which only modulation of pain perception is involved. Anesthesia denotes those states in which mental awareness and perception of other sensations are lost. Attempts have been made to divide anesthesia into various components, including analgesia, amnesia, relaxation, and loss of reflex response to pain. Analgesia can be regarded as a component of anesthesia if viewed in this way.
The use of techniques and medications to provide pain relief in obstetrics requires an expert understanding of their effects to ensure the safety of both mother and fetus.
ANATOMY OF PAIN
It may be academic to argue that pain should be defined as the parturient’s response to the stimuli of labor, because agreement on a definition of pain has eluded scholars for centuries.
Nevertheless, it should be appreciated that the “pain response” is a response of the total personality and cannot be dissected systematically and scientifically. Physicians are obligated to provide a comfortable or at least a tolerable labor and delivery. Many patients are tense and apprehensive at the onset of labor, although they may have little or no discomfort. The physician must be knowledgeable of the options for pain relief and respond to the patient’s needs and wishes.
The evolution of pain in the first stage of labor originally was described as involving spinal segments T11 and T12. Subsequent research has determined that segments T10–L1 are involved. Discomfort is associated with ischemia of the uterus during contraction as well as dilatation and effacement of the cervix. Sensory pathways that convey nociceptive impulses of the first stage of labor include the uterine plexus, the inferior hypogastric plexus, the middle hypogastric plexus, the superior hypogastric plexus, the lumbar and lower thoracic sympathetic chain, and the T10–L1 spinal segments.
Pain in the second stage of labor also is produced by distention of the vagina and perineum. Sensory pathways from these areas are conveyed by branches of the pudendal nerve via the dorsal nerve of the clitoris, the labial nerves, and the inferior hemorrhoidal nerves. These are the major sensory branches to the perineum and are conveyed along nerve roots S2, S3, and S4. Nevertheless, other nerves, such as the ilioinguinal nerves, the genital branches of the genitofemoral nerves, and the perineal branches of the posterior femoral cutaneous nerves, may play a role in perineal innervation.
Although the major portion of the perineum is innervated by the 3 major branches of the pudendal nerve, innervation by the other nerves mentioned may be important in some patients. The type of pain reported may be an ache in the back or loins (referred pain, perhaps from the cervix), a cramp in the uterus (due to fundal contraction), or a “bursting” or “splitting” sensation in the lower vaginal canal or pudendum (due to dilatation of the cervix and vagina).
Dystocia, which usually is painful, may be due to feto-pelvic disproportion; tetanic, prolonged, or dysrhythmic uterine contractions; intrapartum infection; or many other causes.
SAFETY OF OBSTETRIC ANESTHESIA
Substantial advances in the quality and safety of obstetric anesthesia have been made in the past 3 decades. Outdated techniques, such as “twilight sleep” and mask anesthesia, have been recognized as ineffective or unsafe and have been replaced by epidural infusion of narcotic/local anesthesia mixtures and patient-controlled analgesia during labor and postoperatively. When required, general anesthesia is provided using short-acting drugs with well-known fetal effects, and careful attention is focused on airway management.
Maternal mortality relating to anesthesia has been reduced 10-fold since the 1950s, largely because of an enhanced appreciation of special maternal risks associated with anesthesia. The overall anesthesia-related death rate in the United States now is as low as 1.0 per million live births, a 5-fold decline in the last decade. Regional anesthesia now is more commonly performed for caesarean delivery, fewer births occur in hospitals performing fewer than 500 deliveries per year, and having both in-house anesthesia and obstetric physician coverage is more common. Historically, women have a higher chance of dying under general anesthesia than regional anesthesia during caesarean deliveries. During the 1970s and 1980s, the case fatality rate for general anesthesia during caesarean delivery was 32.3 per million and the rate for regional anesthesia was 1.9 per million. Thus 17 women died under general anesthesia for every 1 who died from regional anesthesia. By the 1990s, that ratio dropped to 6 to 1. In the 2000s, the case fatality rate for general anesthesia during caesarean delivery has decreased to 6.5 per million and case fatality rate for regional anesthesia has slightly increased to 3.8. The relative risk of general compared with regional anesthesia fell to 1.7. General anesthesia now seems just as safe as a spinal or epidural for caesarean delivery. The decline in deaths under general anesthesia could be attributed to better anesthetic monitoring, better management of difficult airway-failed intubation, and expertise with laryngeal airway mask and other airways devices. Difficulty with intubation, aspiration, and hypoxemia leading to cardiopulmonary arrest are the leading causes of anesthesia-related maternal death under general anesthesia. And the leading causes of anesthesia-related maternal death from regional anesthesia are high spinal or epidural block, respiratory failure, and drug reaction.
Another point of concern is that the overall maternal mortality (not related specifically to anesthesia) has increased in the United States since 1985. This increase in maternal mortality is most pronounced in older parturients (older than 35 years), particularly in black parturients. Cardiomyopathy, hypertension, obesity, and hemorrhage are the principal etiologies associated with these rising mortality rates and are important factors for the anesthesiologist to consider.
TECHNIQUES OF ANALGESIA WITHOUT THE USE OF DRUGS
Psychophysical Methods
Three distinct psychologic techniques have been developed as a means of facilitating the birth process and making it a positive emotional experience: “natural childbirth,” psycho-prophylaxis, and hypnosis. So-called natural childbirth was developed by Grantly Dick-Read in the early 1930s and popularized in his book Childbirth Without Fear. Dick-Read’s approach emphasized the reduction of tension to induce relaxation. The psychoprophylactic technique was developed by Velvovski, who published the results of his work from Russia in 1950. In Russia in the mid-1950s, it became evident that obstetric psychoprophylaxis was a useful substitute for poorly administered or dangerously conducted anesthesia for labor and delivery. This method was later introduced in France by Lamaze. Hypnosis for pain relief has achieved periodic spurts of popularity since the early 1800s and depends on the power of suggestion.
Many obstetricians argue that psychoprophylaxis can largely eliminate the pain of childbirth by diminishing cortical appreciation of pain impulses rather than by depressing cortical function, as occurs with drug-induced analgesia. Relaxation, suggestion, concentration, and motivation are factors that overlap other methods of preparation for childbirth. Some of them are closely related to hypnosis.
These techniques can significantly reduce anxiety, tension, and fear. They provide the parturient with a valuable understanding of the physiologic changes that occur during labor and delivery. In addition, they provide an opportunity for closer understanding and communication between the patient and her mate, who may be an important source of comfort to her during the stressful process of childbirth. If psychophysical techniques do no more than this, they deserve the obstetrician’s support.
Studies undertaken to assess the effectiveness of psychophysical techniques have reported widely divergent results, with effectiveness ranging from as low as 10–20% to as high as 70–80%. The overall benefit is best judged by the parturient herself, with validation by the observations of attendants. As is no doubt true in other aspects of medical practice in which emotional overlay and subjective reporting play a role in the evaluation of specific types of therapy, the personality and level of enthusiasm of the doctor can strongly influence the patient’s reactions to a given therapy. Practitioners who are skeptical of psychophysical techniques cannot expect to accomplish very much using them.
None of these psychophysical techniques should be forced on a patient, even by a skillful provider. The patient must not be made to feel that she will fail if she does not choose to complete her labor and delivery without analgesic medication. It must be made clear to the patient from the outset that she is expected to ask for help if she feels she wants or needs it. All things considered, psychophysical techniques should be viewed as adjuncts to other analgesic methods rather than substitutes for them.
The effectiveness of hypnosis is partially due to the well-known, although incompletely understood, mechanisms by which emotional and other central processes can influence a person’s overall responses to the pain experience. Verbal suggestion and somatosensory stimulation may help to alleviate discomfort associated with the first stage of labor. In addition, hypnotic states may provide apparent analgesia and amnesia for distressing, anxiety-provoking experiences. Finally, hypnotic techniques may substantially improve the parturient’s outlook and behavior by reducing fear and apprehension. However, certain practical points with regard to hypnosis must be considered because the time needed to establish a suitable relationship between physician and patient often is more than can be made available in the course of a busy medical practice.
ANALGESIC, AMNESTIC, & ANESTHETIC AGENTS
General Comments & Precautions
1. If the patient is prepared psychologically for her experience, she will require less medication. Anticipate and dispel her fears during the antenatal period and in early labor. Never promise a painless labor.
2. Individualize the treatment of every patient, because each one reacts differently. Unfavorable reactions to any drug can occur.
3. Know the drug you intend to administer. Be familiar with its limitations, dangers, and contraindications as well as its advantages.
4. All analgesics given to the mother will cross the placenta. Systemic medications produce higher maternal and fetal blood levels than regionally administered drugs. Many drugs have central nervous system depressant effects. Although they may have the desired effect on the mother, they also may exert a mild to severe depressant effect on the fetus or newborn.
The ideal drug will have an optimal beneficial effect on the mother and a minimal depressant effect on the offspring. None of the presently available narcotic and sedative medications used in obstetrics has selective maternal effects. The regional administration of local anesthetics accomplished this goal to a large extent because the low maternal serum levels that are produced expose the fetus to insignificant quantities of drugs.
Pharmacologic Aspects
A. Route of Administration
Systemic techniques of analgesia and anesthesia include both oral and parenteral routes of administration. Parenteral administration includes subcutaneous, intramuscular, and intravenous injection. Sedatives, tranquilizers, and analgesics usually are given by intramuscular injection. In some cases, the intravenous route is preferred.
The advantages of intravenous administration are (1) avoidance of variable rates of uptake due to poor vascular supply in fat or muscle; (2) prompt onset of effect; (3) titration of effect, avoiding the “peak effect” of an intramuscular bolus; and (4) smaller effective doses because of earlier onset of action.
The disadvantages of intravenous injection are inadvertent arterial injection and the depressant effect of over-dosage, but the advantage of smaller dosage outweighs the disadvantages.
Always administer the lowest concentration and the smallest dose to obtain the desired effect.
B. Physical and Chemical Factors
Anesthetics penetrate body cells by passing through the lipid membrane boundary. This membrane is not permeable to charged (ionized) drugs but is permeable to unionized forms of drugs. Much of the total drug transfer is dependent on the degree of lipid solubility, so local anesthetics are characterized by aromatic rings that are lipophilic, and all are lipid-soluble. The intermediate amine radical of a local anesthetic is a weak base that in aqueous solutions exists partly as undissociated free base and partly as dissociated cation. Figure 24–1 shows the equilibrium for such an existence and the Henderson-Hasselbalch equation, with which the proportion of the anesthetic in the charged and uncharged forms can be determined. The ratio of the cation to the base form of the drug is important, because the base form is responsible for penetration and tissue diffusion of the local anesthetic, whereas the cation form is responsible for local analgesia when the drug contacts the site of action within the sodium channel on the axolemma.
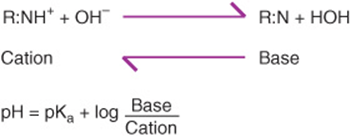
Figure 24–1. Local anesthetics are weak bases coexisting as undissociated free base and dissociated cation. Their proportion can be calculated by means of the Henderson-Hasselbalch equation.
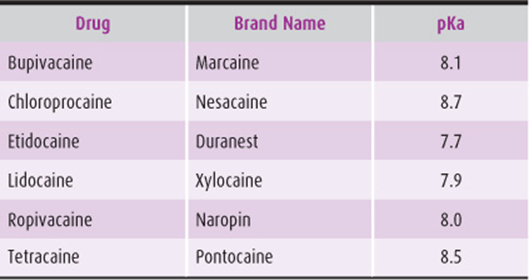
The pKa of a drug is the pH at which equal proportions of the free base and cation form occur. Most local anesthetics used in obstetric analgesia have pKa values ranging from 7.7–9.1 (Table 24–1). Because the pH of maternal blood is equal to or greater than 7.4, the pKa of local anesthetics is so close that significant changes in maternal and fetal acid–base balance may result in fluxes in the base versus the cation forms of the drug. For example, a rising pH shifts a given amount of local anesthetic cation to the base form; conversely, a fall in pH generates more of the cationic form.
Table 24–1. pKa values of the more commonly used local anesthetics.
Physical factors are important in drug transfer. Drugs with a molecular weight (MW) under 600 cross the placenta without difficulty, whereas those with MW over 1000 do not. A molecule such as digoxin (MW 780.95) crosses the ovine placenta very poorly. Molecular weights of most local anesthetics are in the 200–300 range. From the physical aspect, most local anesthetics cross the maternal–fetal barrier by simple diffusion according to the principles of Fick’s law (Fig. 24–2), which states that the rate of diffusion of a drug depends on the concentration gradient of the drug between the maternal and fetal compartments and the relationship of the thickness and total surface available for transfer.
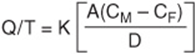
Figure 24–2. Fick’s law. A, surface area available for drug transfer; CM, maternal drug concentration; CF, fetal drug concentration; D, membrane thickness; K, diffusion constant of the drug; Q/T, rate of diffusion.
C. Placental Transfer
Factors other than the physical or chemical properties of a drug may affect its transfer across the placenta. These factors include the rate and route of drug administration and the distribution, metabolism, and excretion of the drug by the mother and fetus. Fick’s law may appear to be a simple method of determining drug transfer, but other complexities exist: differential blood flow on either side of the placenta, volume of maternal and fetal blood, and various shunts in the intervillous space that are important determinants of the final amount of drug a fetus may receive. Certain maternal disorders, such as hypertensive cardiovascular disease, diabetes, and preeclampsia-eclampsia, may alter placental blood flow and in some way affect the extent of drug distribution.
As the placenta matures, the thickness of the epithelial trophoblastic layer progressively decreases. This reduction may cause the thickness of the tissue layers between the maternal and fetal compartments to decrease 10-fold (from as much as 25 μm in early gestation to 2 μm at term in some species). As gestation progresses, the surface area of the placenta also increases. At term, these changes in physical structure tend to favor improved transfer of drugs across the placenta.
Placental transfer is affected by the pH of the blood on both sides of the placenta. The pH of the blood on the fetal side of the placenta normally is 0.1–0.2 U lower than that on the maternal side. Therefore, passage of drug to the fetal unit results in a tendency for more of the drug to exist in the ionized state. Because the maternal–fetal equilibrium is established only between the unionized fraction of the drug on either side of the barrier, this physiologic differential will expedite maternal–fetal transfer of drug. With more drug in the ionized form in the fetal unit, the new equilibrium that arises results in a greater total (ionized plus unionized) drug load in the fetus. Because the pKavalues of commonly used local anesthetics are closer to the maternal blood pH, these agents tend to accumulate on the fetal side of the placenta. This also is true of other basic drugs such as morphine, meperidine, and propranolol. Further decreases in the fetal pH lead to additional drug entrapment in the fetus. For acidic drugs (eg, thiopental) the shift in total drug concentration is in the opposite direction, that is, toward the maternal side of the placenta.
In summary, the rate of transfer of a drug is governed mainly by (1) lipid solubility, (2) degree of drug ionization, (3) placental blood flow, (4) molecular weight, (5) placental metabolism, and (6) protein binding.
D. Fetal Distribution
After a drug deposited in the maternal compartment passes through the maternal–fetal barrier, the drug must reach the fetus and undergo distribution (Fig. 24–3). The response of the fetus and newborn depends on drug concentration in vessel-rich organs, such as the brain, heart, and liver. Drugs transferred from the maternal to the fetal compartment of the placenta are then diluted before distribution to the various fetal vital organs. Approximately 85% of the blood in the umbilical vein, which passes from the placenta to the fetus, passes through the fetal liver and then into the inferior vena cava. The remainder bypasses the liver and enters the vena cava primarily via the ductus venosus. An admixture of blood coming from the lower extremities, the abdominal viscera, the upper extremities, and the thorax further reduces the drug concentration. Blood from the right atrium shunts from right to left through the foramen ovale into the left atrium, resulting in a final concentration on the left side of the heart that is only slightly lower than that in the vena cava.
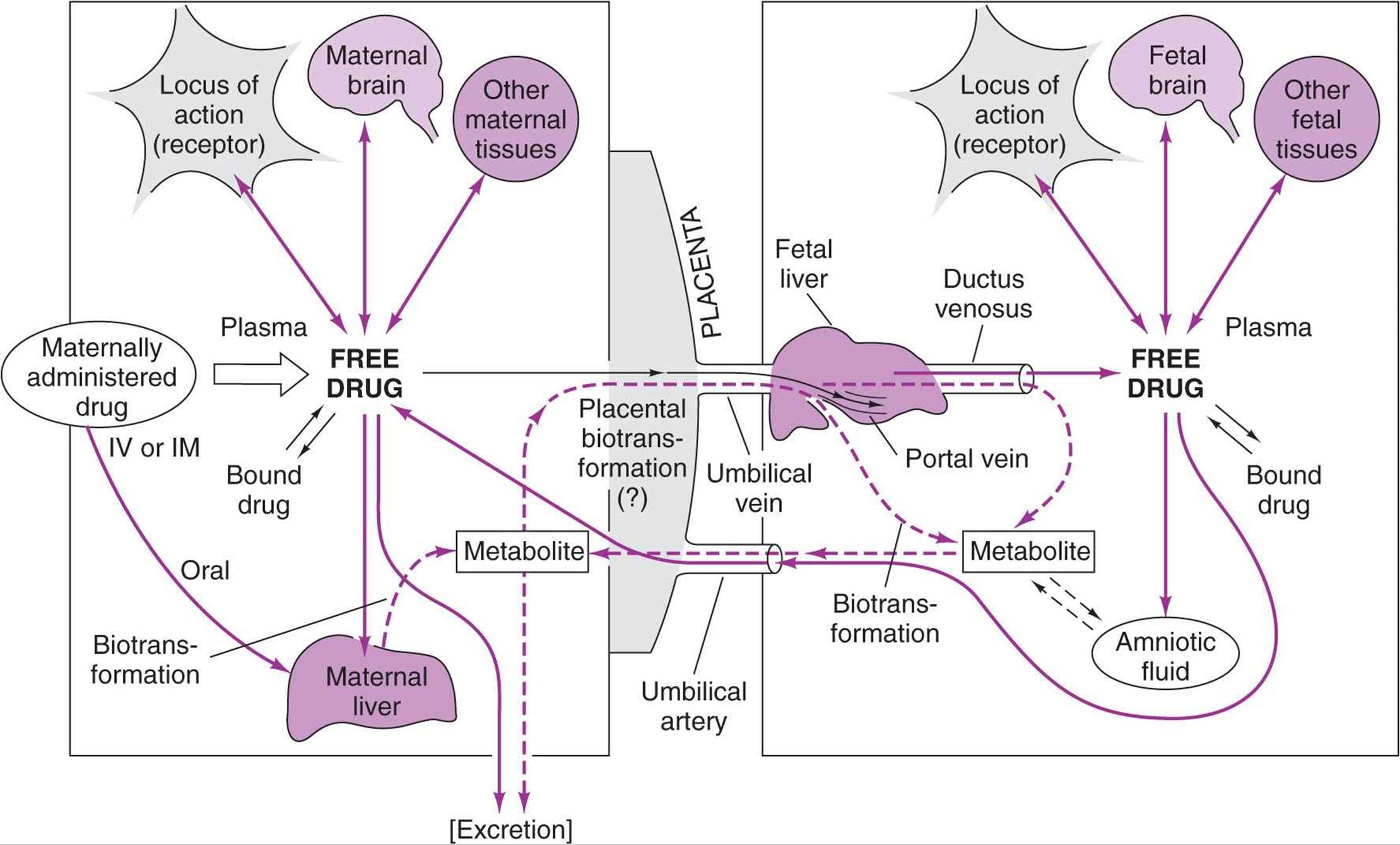
Figure 24–3. Relationship between maternal and fetal compartments and distribution of drugs between them. Drug is passed from the maternal compartment, via the placenta (a partial barrier), to the fetal compartment, where the principles of drug dynamics (ie, distribution, biotransformation, and excretion) determine the eventual specific organ tissue levels. One purely mechanical barrier exists between the maternal and fetal compartments, which attains importance in the late first and second stages of labor—the umbilical cord, which is susceptible to partial and total occlusion.
The amount of drug ultimately reaching a vital organ is related to that organ’s blood supply. Because the central nervous system is the most highly vascularized fetal organ, it receives the greatest amount of drug. Once the drug reaches the fetal liver, it may either be bound to protein or metabolized.
The uptake of drug by fetal tissues can be very rapid after either intravenous or epidural administration. Measurable concentrations of local anesthetics have been found in fetal tissues as early as 1–2 minutes after injection. Lipid solubility of a drug is important in developing concentrations in certain organs with high lipid content, such as the adrenal, ovary, liver, and brain.
Drug metabolism and excretion are the final features of the fetal distribution picture. The fetal liver is able to metabolize drugs and numerous substrates as early as the second trimester, an ability that improves to term. Narcotics and sedatives are metabolized much more slowly by the fetal liver, producing a prolonged effect of these drugs in the newborn who is exposed in utero. Finally, the ability of the fetus to excrete drugs is also reduced by reduced renal function.
Systemic Analgesics & Anesthetics
A. Sedatives (Hypnotics)
The principal use of sedative–hypnotic drugs is to produce drowsiness. For many years, these drugs were the only ones available to reduce anxiety and induce drowsiness. The latent phase of the first stage of labor can be managed by either psychologic support alone or utilization of sedative–hypnotic compounds. Psychologic support may be complemented by the use of sedatives. When properly used, these drugs induce tranquility and an enhanced feeling of well-being. They are poor analgesics and do not raise the pain threshold appreciably in conscious subjects. Amnesia does not occur. Labor may be slowed by large doses of sedatives, especially when given too early in the first stage.
The use of barbiturates alone for obstetric analgesia is not common practice and should be discouraged. The required dosage is dangerous to the fetus, which is extremely sensitive to central nervous system depression by these drugs. Periodic apnea and even abolition of all movements outlast the effects of the barbiturates on the mother.
B. Tranquilizers & Amnestics
These drugs are used principally to relieve apprehension and anxiety and to produce a calm state. Additionally, they may potentiate the effects of other sedatives. An analgesic-potentiating effect is often claimed for this group of agents but has not been definitely demonstrated. Hydroxyzine and diazepam are popular tranquilizer–amnestics. Scopolamine, which was widely popular in obstetrics in the past, produces no analgesia but has a mild sedative and marked amnestic effect. Scopolamine is no longer used because the amnesia produced is excessive and prolonged. Diazepam should be avoided during labor because it has a long chemical half-life, which is even more prolonged in the neonate. Diazepam readily crosses the placenta and is found in significant concentrations in fetal plasma. At present, diazepam is not recommended if the neonate is premature because of the threat of kernicterus. Other potential side effects related to the use of diazepam are fetal hypotonia, hypothermia, and a loss of beat-to-beat variability in the fetal heart rate.
One of the controversies over diazepam concerns the content of sodium benzoate and benzoic acid buffers. Both compounds are potent uncouplers of the bilirubin–albumin complex, and some investigators have suggested that the neonate may be more susceptible to kernicterus because of an increase level of free circulating bilirubin. However, because injectable diazepam is effective in the treatment of human newborn seizure disorders, opiate withdrawal, and tetanus and because it is regarded as a useful adjunct in obstetric analgesia, a study was undertaken in animals in which comparable quantities of sodium benzoate were injected to determine whether significant amounts of bilirubin would be made available to the circulation. Midazolam, a short-acting water-soluble benzodiazepine, appears to be devoid of the neonatal effects seen with diazepam and is more rapidly cleared. In small doses it could conceivably become a useful anxiolytic for the laboring patient. Midazolam is 3–4 times more potent than diazepam, and there is a brief delay in the onset of its sedative effect after intravenous injection. Doses should be kept below 0.075 mg/kg to avoid excessive anterograde amnesia.
C. Narcotic Analgesics
Systemic analgesic drugs (including narcotics) are commonly used in the first stage of labor because they produce both a state of analgesia and mood elevation. The favored drugs are codeine 60 mg intramuscularly or meperidine 50–100 mg intramuscularly or 25–50 mg (titrated) intravenously. The combination of morphine and scopolamine was once popular for its “twilight sleep” effect but is rarely used now. Common undesirable effects of this combination of drugs are nausea and vomiting, cough suppression, intestinal stasis, and diminution in frequency, intensity, and duration of uterine contractions in the early first stage of labor. Also, amnesia is excessive for these patients.
Morphine is not used in active laboring patients because of the excessive respiratory depression seen in the neonate compared with equipotent doses of other narcotics. Fetuses who are of young gestational age, are small for dates, or have undergone trauma or long labor are more susceptible to narcosis.
Fentanyl is a popular synthetic narcotic that has been used in obstetrics in both the systemic and epidural compartments. Its use in the epidural compartment has met with good success when combined with small quantities and low concentrations of bupivacaine. Data supporting its use come from both Europe and the United States.
Sufentanil is a derivative of fentanyl with increased potency and lipophilicity. It is widely used for intrathecal and epidural analgesia during labor. Potential adverse effects of sufentanil include possible placental deposition and neonatal respiratory depression. Adding intrathecal or epidural sufentanil to bupivacaine improves labor analgesia with faster onset and longer duration compared with bupivacaine alone. The usual dose is 3–5 μg intrathecally and 10–15 μg epidurally.
Remifentanil is a newer ultra short-acting synthetic opioid with rapid onset (approximately 1 minute) after intravenous administration. It is rapidly metabolized by nonspecific blood and tissue esterases, not depending on renal or hepatic function, and hence it does not accumulate in the fetus. This rapid onset and elimination facilitate its effective and safe use during labor. Remifentanil has been administered as intravenous analgesia for labor using a variety of methods, including baseline infusion, PCA boluses (with or without baseline infusion), and target-controlled infusions.
Butorphanol (Stadol) is a synthetic parenteral analgesic that has agonist and antagonist of opioid properties. It is 5 times as potent as morphine and 40 times as potent as meperidine. The typical doses are 1–2 mg intravenously or intramuscularly every 3–4 hours. Onset of analgesia is within a few minutes after intravenous injection. There is less respiratory depression compared with an equivalent dose of morphine due to ceiling effect from its agonist-antagonist properties. This property makes butorphanol particularly useful for labor analgesia, when respiratory depression of the fetus/neonate is a concern.
Nalbuphine (Nubain) is a mixed agonist/antagonist opioid similar to butorphanol commonly used for parenteral labor analgesia. Its potency is equivalent to that of morphine on a milligram basis. The onset of action after intravenous injection is 2–3 minutes with duration of 5–6 hours. The usual dose is 10–20 mg intravenously every 4–6 hours. It is metabolized predominantly by the liver and excreted by the kidney.
D. Thiobarbiturate
Intravenous anesthetics such as thiopental and thiamylal are widely used in general surgery. However, less than 4 minutes after a thiobarbiturate is injected into the mother’s vein, the concentrations of the drug in the fetal and maternal blood will be equal. The mother will lose consciousness and airway protective reflexes with a thiopental dose of 1.5–2 mg/kg; therefore, it should be used only in association with general endotracheal anesthesia. Thiopental doses of 3–4 mg/kg are used for induction of general anesthesia.
E. Propofol
Propofol is a newer induction agent that was introduced into practice in the United States in the early 1990s. As an induction agent, it is similar to the barbiturates in mild cardiac depression and loss of peripheral vasomotor tone. It offers the advantages of rapid clearance, short duration of action, antiemetic properties, and reduced risk of airway reactivity. It is an ideal agent for induction of general anesthesia at a dose of 2 mg/kg in parturients. It also can be used in 10- to 20-mg increments during surgery under regional block to treat nausea and vomiting. Neonatal Apgar scores and umbilical gases are similar after induction with propofol or barbiturates.
F. Etomidate
Etomidate is an intravenous induction agent that has been used in obstetric anesthesia since 1979. It produces a rapid onset of anesthesia with minimal cardiorespiratory effects. This property makes it ideal for parturients who are hemodynamically unstable or who would not tolerate hemodynamic aberrations well. With an induction dose of 0.2–0.3 mg/kg, etomidate undergoes a rapid hydrolysis that leads to quick recovery. Etomidate crosses the placenta rapidly; however, large variations in the UV/MV (umbilical vein: maternal vein) ratio (0.04–0.5) have been reported. Etomidate may cause pain at the injection site and involuntary muscle movements in some patients.
G. Ketamine
The phencyclidine derivative ketamine produces anesthesia by a dissociative interruption of afferent pathways from cortical perception. It has become a useful and widely used adjunctive agent in obstetrics because maternal cardiovascular status and uterine blood flow are well maintained. Effective maternal analgesia results from low doses of 0.25–0.5 mg/kg but without loss of consciousness or protective reflexes. The margin of safety is narrow, however, so it should be used only by physicians able to easily secure and protect the airway if loss of consciousness occurs. For caesarean delivery, general anesthetic induction can be produced with 1–2 mg/kg intravenously. Ketamine stimulates the cardiovascular system to maintain heart rate, blood pressure, and cardiac output. It is useful in the setting of major blood loss, when rapid induction of general anesthesia is required. However, it has significant hallucinogenic effects that limit its utility in obstetrics.
H. Inhalation Anesthetics
Inhaled anesthetics are administered as a component of general anesthesia. In the past, inhaled anesthetics were given during labor in subanesthetic concentrations to treat contraction pain, but they are no longer used for this indication. The mask administration of these gases to the conscious laboring patient can result in airway obstruction, aspiration, and hypoxia. Also, the vaporized gases would unacceptably contaminate the labor room environment because effectively scavenging of exhaust gases from the room is not possible. Finally, of all the presently used volatile anesthetics, only nitrous oxide has analgesic properties at subanesthetic concentrations.
The most commonly used inhaled anesthetics in pregnancy are nitrous oxide, sevoflurane, desflurane, and isoflurane. These drugs all readily cross the placenta and produce significant blood concentrations in the fetus. During the brief exposure to maternally administered anesthetic gases, the fetus is not adversely affected. Fetal cardiac output is slightly reduced by these drugs, but critical organ blood flow is unaffected, and fetal acid–base status is unchanged. Exposure to minimum alveolar concentrations of anesthetic gases for more than 15 minutes is associated with reduced Apgar scores, but other parameters of fetal and newborn well-being are unimpaired.
The term parturient is more sensitive to the anesthetic effects of all inhaled anesthetics, presumably as a result of elevated progesterone levels. This increased sensitivity of 20–30% compared with nonpregnant subjects places the patient at increased risk for obtundation and aspiration; therefore, these drugs should not be administered without preparation for endotracheal intubation. Volatile agents except N2O produce uterine relaxation, and high concentrations should be avoided during delivery to prevent uterine atony and postpartum hemorrhage. At low concentrations (<1%), they produce amnesia, and their tocolytic effects are easily counteracted by standard infusions of oxytocin (Pitocin).
REGIONAL ANESTHESIA
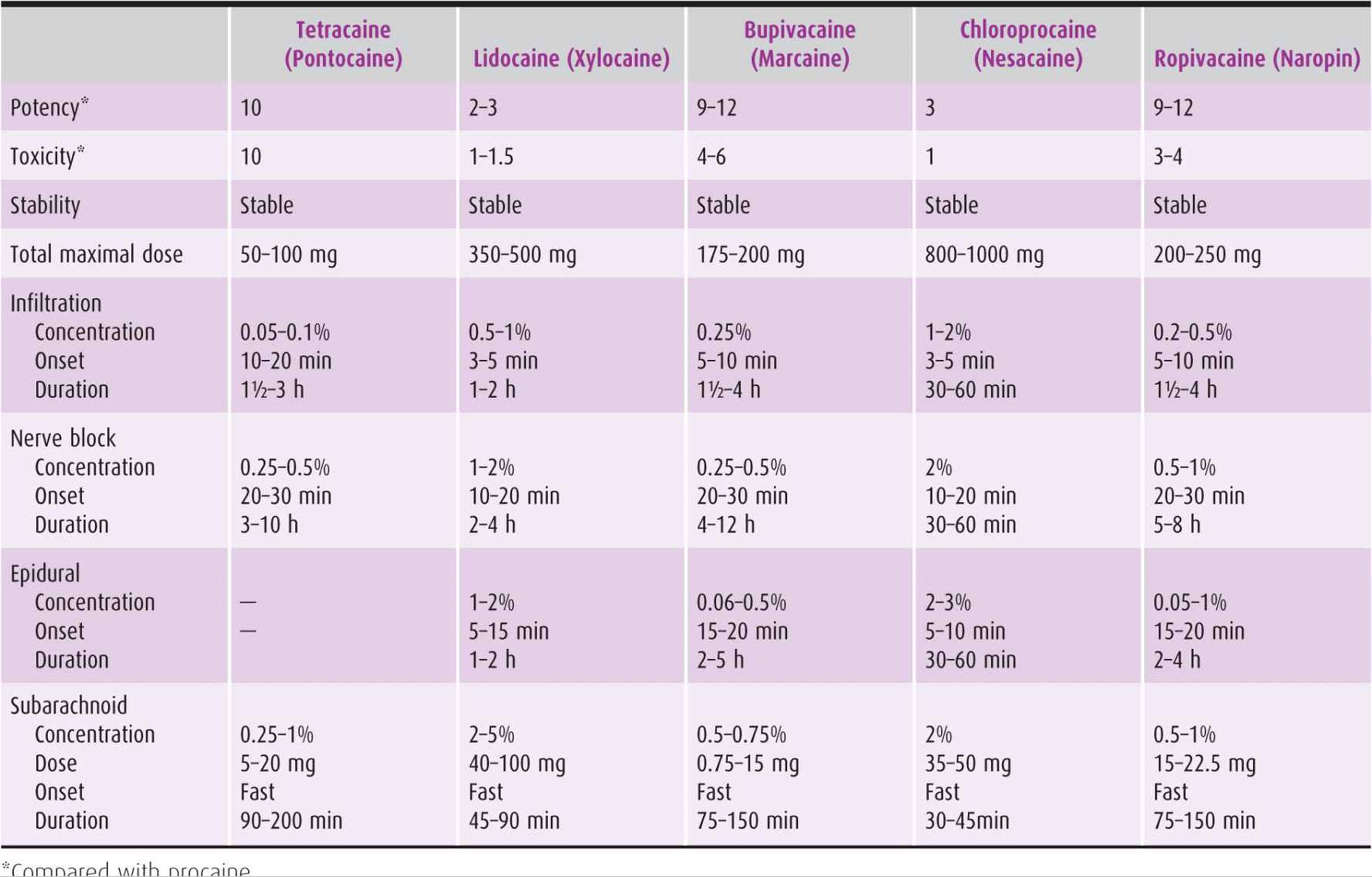
Regional anesthesia is achieved by injection of a local anesthetic (Table 24–2) around the nerves that pass from spinal segments to the peripheral nerves responsible for sensory innervation of a portion of the body. More recently, narcotics have been added to local anesthetics to improve analgesia and reduce some side effects of local anesthetics. Regional nerve blocks used in obstetrics include the following: (1) lumbar epidural and caudal epidural block, (2) subarachnoid (spinal) block, (3) combined spinal epidural block, and (4) pudendal block.
Table 24–2. Drugs used for local anesthesia.
Infiltration of a local anesthetic drug and pudendal block analgesia carry minimal risks. The hazards increase with the amount of drug used. The safety and suitability of regional anesthesia depend on proper selection of the drug and the patient and the obstetrician–gynecologist’s knowledge, experience, and expertise in the diagnosis and treatment of possible complications. Major conductive anesthesia and general anesthesia in obstetrics require specialized knowledge and expertise in conjunction with close maternal and fetal monitoring. This field of expertise has developed as a subspecialty within anesthesia, reflecting the need for specialized understanding of the obstetric patient and her response and of the fetal responses to anesthesia.
Patient Selection
Regional anesthesia is appropriate for labor analgesia, caesarean delivery, and other obstetric operative procedures (eg, postpartum tubal ligation, cervical cerclage). Most patients prefer to remain awake; however, occasionally a choice is made to provide general anesthesia.
The anesthesiologist will assess the patient to determine the relative risks of general versus regional anesthesia. For example, some forms of valvular heart disease may contraindicate regional block, and general anesthesia may be considered more appropriate. Other contraindications to regional anesthesia include infection, coagulopathy, hypovolemia, progressive neurologic disease, and patient refusal.
Patient Preparation
The woman who is well informed and has a good rapport with her physician generally is a calm and cooperative candidate for regional or general anesthesia. The patient and her partner should be well informed early in her pregnancy of the options for labor anesthesia as well as for caesarean section if that circumstance arises. The anesthesiologist can be involved early in pregnancy if the patient has special concerns about anesthesia (family history of anesthetic risk, previous back surgery, coagulation problems). Some hospitals have obstetric anesthesia preassessment clinics that deal with these patient concerns.
Local Anesthetic Agents
A local anesthetic drug blocks the action potential of nerves when their axons are exposed to the medication. Local anesthetic agents act by modifying the ionic permeability of the cell membrane to stabilize its resting potential. The smaller the nerve fiber, the more sensitive it is to local anesthetics because the susceptibility of individual nerve fibers is inversely proportional to the cross-sectional diameter of the fibers. Hence, with regional anesthesia, the patient’s perception of light touch, pain, and temperature and her capacity for vasomotor control are obtunded sooner and with a smaller concentration of the drug than is the perception of pressure or the function of motor nerves to striated muscles. The exception to this rule is the sensitivity of autonomic nerve fibers that are blocked by the lowest concentration of local anesthetic despite their being larger than some sensory nerves.
Only anesthetic drugs that are completely reversible and nonirritating and cause minimal toxicity are clinically acceptable. Other desirable properties of regional anesthetic agents include rapidity of onset, predictability of duration, and ease of sterilization. Table 24–2 summarizes the local anesthetics commonly used in obstetrics and gynecology together with their uses and doses.
All local anesthetics have certain undesirable dose-related side effects when absorbed systemically. All these drugs are capable of stimulating the central nervous system and may cause bradycardia, hypertension, or respiratory stimulation at the medullary level. Moreover, they may produce anxiety, excitement, or convulsions at the cortical or subcortical level. This response stimulates grand mal seizures because it is followed by depression, loss of vasomotor control, hypotension, respiratory depression, and coma. Such an episode of indirect cardiovascular depression often is accentuated by a direct vasodilatory and myocardial depressant effect. The latter is comparable to the action of quinidine. This effect explains why lidocaine is useful for treatment of certain cardiac arrhythmias.
Chloroprocaine is an ester derivative that was popular in 1970s primarily because of its rapid onset and short duration of action and its low toxicity to the fetus. It is metabolized by plasma cholinesterase and therefore does not demand liver enzyme degradation, as do the more complex and longer acting amide derivatives. Chloroprocaine has a half-life of 21 seconds in adult blood and 43 seconds in neonatal blood. Direct toxic effects on the fetus are minimized because fewer drugs are available for transfer in the maternal compartment.
The potency of chloroprocaine is comparable to that of lidocaine and mepivacaine, and the drug is 3 times more potent than procaine. Its average onset of action ranges from 6–12 minutes and persists for 30–60 minutes, depending on the amount used. Chloroprocaine is often used for urgent caesarean delivery when epidural catheter is already placed to avoid general anesthesia.
Bupivacaine, the amide local anesthetic, is related to lido-caine and mepivacaine but has some very different physico-chemical properties. It has a much higher lipid solubility, a higher degree of binding to maternal plasma protein, and a much longer duration of action. More than with other local anesthetics, the concentration of bupivacaine can be reduced to produce sensory block with minimal motor block. Because injection of bupivacaine for labor pain relief now is mostly in the form of continuous small-volume and minimal concentration administration via a pump mechanism, the complications previously of concern, such as hypotension and convulsions, are now rare.
A word of caution is needed regarding the administration of bupivacaine for caesarean delivery. This drug has been implicated in certain cardiovascular catastrophes associated with initial drug injection, such as cardiac arrests that were refractory to full and appropriate resuscitative attempts. Although these catastrophes are rare, the practitioner is well advised to inject no more than 5 mL of the drug at any one time, to wait 4–5 minutes, then to repeat the procedure until the desired volume has been delivered. The maximum concentration of bupivacaine now allowed by the Food and Drug Administration (FDA) for obstetric epidural anesthesia is 0.5%. The dose of more than 3 mg/kg is considered a toxic dose now. The safety of bupivacaine can be enhanced by giving it in fractional doses (eg, 5 mL every 5 minutes).
Ropivacaine is a newer amide local anesthetic introduced into the United States in the mid-1990s. It is less lipid-soluble than bupivacaine, and initial studies suggested that it produced less motor blockade and was less cardiotoxic than its homologue bupivacaine. Later studies have been less convincing in documenting improved efficacy and safety, but ropivacaine has replaced bupivacaine in some institutions. There is ongoing study of the safety and efficacy of levobupivacaine, the levorotatory isomer of bupivacaine, which may also prove less cardiotoxic than its racemic parent molecule. Both of these newer amide local anesthetics are used in doses and concentrations similar to those of bupivacaine.
Local Infiltration Analgesia
Local tissue infiltration of dilute solutions of anesthetic drugs generally yields satisfactory results because the target is the fine nerve fibers. Nevertheless, one must keep in mind the dangers of systemic toxicity when large areas are anesthetized or when reinjection is required. It is good practice, therefore, to calculate in advance the milligrams of drug and volume of solution that may be required to keep the total dosage below the accepted toxic dose.
Infiltration in or near an area of inflammation is contra-indicated. Injections into these zones may be followed by rapid systemic absorption of the drug as a result of increased vascularity of the inflamed tissues. Moreover, the injection may introduce or aggravate infection.
Regional Analgesia Techniques
A. Lumbar Epidural Block
This analgesic technique is well suited to obstetric anesthesia. Either bolus injections or continuous infusion of local anesthetics is used for labor, vaginal delivery, or caesarean surgery. Narcotics are added to supplement the quality of the block.
After the patient is evaluated, an epidural block can be placed once labor is established. Drug dosages can be adjusted as circumstances change. The catheter can be used for surgery and postoperative analgesia if necessary. The second stage of labor is prolonged by epidural anesthesia; however, the duration of the first stage is unaffected. The use of outlet forceps is increased, but fetal outcome is not adversely affected by epidural block.
The epidural block technique must be exact, and inadvertent massive (high) spinal anesthesia occasionally occurs. Other undesirable reactions include the rapid absorption syndrome (hypotension, bradycardia, hallucinations, and convulsions), postpartum backache, and paresthesias. Epidural block should eradicate pain between T10 and L1 for the first stage of labor and between T10 and S5 for the second stage of labor.
The procedure is as follows. Inject 3 mL of a 1.5% aqueous solution of lidocaine or similar agent into the catheter as a test dose. If spinal anesthesia does not result after 5–10 minutes, inject an additional 5 mL. Inject 10 mL of the anesthetic solution in total to slowly accomplish an adequate degree and suitable level of anesthesia. Once the block is established, a continuous infusion of 10–12 mL/h will maintain the block for labor. Bupivacaine 0.125–0.25% is most often used for an epidural block, with fentanyl 2–5 μg/mL in the epidural mixture.
The mother is nursed in a wedged or lateral position to prevent aortocaval compression. The sympathectomy produced by the block predisposes the patient to venous pooling and reduced venous return. Maternal blood pressure must be measured frequently when the epidural is in effect.
B. Caudal Block
Caudal anesthesia (Fig. 24–4) is an epidural block approached through the caudal space. It can provide selective sacral block for the second stage of labor; however, it is rarely used now because of complications specific to the obstetric patient. The descent of the fetal head against the perineum, in addition to the sacral edema at term, obscures the landmarks of the sacral hiatus. This makes the caudal procedure technically challenging, and reports of transfixing the rectum and fetal skull puncture with the epidural needle have led many anesthesiologists to avoid this technique. Lumbar epidural anesthesia is considered a safer alternative.
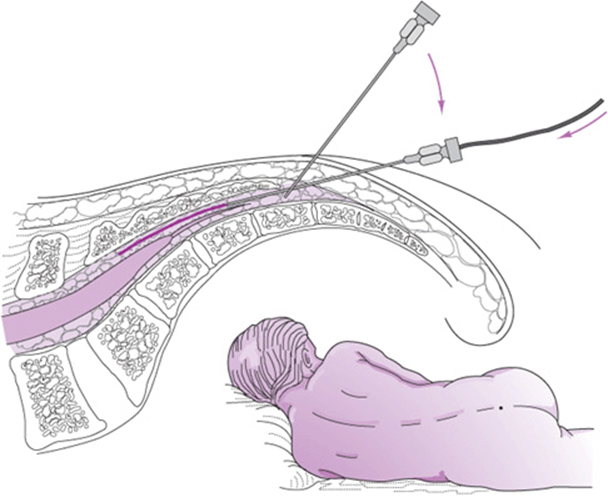
Figure 24–4. Caudal catheter in place for continuous caudal anesthesia.
C. Spinal Anesthesia
Spinal anesthesia currently is the anesthetic of choice for caesarean delivery. Spinal anesthesia can be performed more quickly than epidural anesthesia and provides ideal operating conditions, including dense sensory and motor block. The onset of sympathectomy is more abrupt than with epidural block, so care must be taken to ensure that the patient is adequately preloaded with 1.5–2 L of saline solution before performing the technique. Spinal anesthesia is used less commonly these days to alleviate the pain of delivery and the third stage of labor. The advantages of spinal anesthesia are that the mother remains conscious to witness delivery, no inhalation anesthetics or analgesic drugs are required, the technique is not difficult, and good relaxation of the pelvic floor and lower birth canal is achieved. Prompt anesthesia is achieved within 5–10 minutes. The dosage of spinal anesthetic is small. Complications are rare and easy to treat. However, spinal headache occurs in 1–2% of patients.
D. Combined Spinal–Epidural Analgesia
The use of combined spinal–epidural anesthesia (CSE) became popular in the mid 1990s as an alternative to epidural anesthesia for labor. A small dose of local anesthetic and narcotic (2.5 mg bupivacaine and 25 μg fentanyl) is injected through a spinal needle, which is introduced through the epidural needle and advanced into the intrathecal space. The spinal needle is withdrawn and the epidural catheter placed for later use. The spinal medication produces immediate pain relief and minimal motor block and may allow ambulation. Later in labor, the epidural catheter is used for continuous infusion of epidural solution, similar to that described for standard epidural anesthesia in labor.
Detractors of CSE argue that the technique may increase the incidence of post–lumbar puncture headache and that ambulation even after low-dose spinal injection is unsafe for both mother and baby. Finally, because the technique is technically cumbersome, it may be associated with higher complication rates, although the studies did not support this statement.
The most serious consequence of spinal or epidural anesthesia is maternal mortality. Maternal deaths associated with use of 0.75% bupivacaine for caesarean delivery and labor were reported in the late 1980s, prompting the FDA to outlaw the use of this drug in obstetrics. These deaths were attributed to venous uptake of the drug and immediate and lasting myocardial depression from the local anesthetic, which did not respond to appropriate cardiac resuscitative efforts. Today maternal mortality associated with regional anesthesia is lower, primarily because bolus dosing of high concentrations of local anesthesia is no longer performed.
Most side effects of spinal or epidural anesthesia are secondary to block of the sympathetic nerve fibers that accompany the anterior roots of the spinal thoracic and upper lumbar nerves (thoracolumbar outflow). Thus many physiologic regulating mechanisms are disturbed. The blood pressure falls as a result of loss of arterial resistance and venous pooling—assuming no compensation is made by change of the patient’s position (eg, Trendelenburg position). If high thoracic dermatomes (T1–T5) are blocked, alteration of the cardiac sympathetic innervation slows the heart rate and reduces cardiac contractility. Epinephrine secretion by the adrenal medulla is depressed. Concomitantly, the unopposed parasympathetic effect of cardiac slowing alters vagal stimulations. As a result of these and related changes, shock follows promptly, especially in hypotensive or hypovolemic patients. Moreover, a precipitous fall in the blood pressure of the arteriosclerotic hypertensive patient is inevitable.
Fluids, oxygen therapy for adequate tissue perfusion, shock position to encourage venous return, and pressor drugs given intravenously are recommended.
In the past, postdural puncture headache (PDPH) due to leakage of cerebrospinal fluid through the needle hole in the dura was an early postoperative complication in up to 15% of patients. Small-caliber needles (25F) decrease the incidence of headache to 8–10%. With the introduction of pencil-point Whitaker and Sprotte spinal needles, the incidence of PDPH has been reduced to 1–2%. Therapy for PDPH includes recumbent position, hydration, sedation, and, in severe cases, epidural injection of 10–20 mL of the patient’s fresh blood to “seal” the defect.
Rarely, spinal or epidural anesthesia caused nerve injury and transient or permanent hypesthesia or paresthesia. Excessive drug concentration, sensitivity, or infection may have been responsible for some of these complications. The incidence of serious complications of spinal or epidural anesthesia is considerably lower than that of cardiac arrest during general anesthesia.
E. Paracervical Block
Paracervical block is no longer considered a safe technique for the obstetric patient. In the past, paracervical anesthesia was used to relieve the pain of the first stage of labor. Pudendal block was required for pain during the second stage of labor. Sensory nerve fibers from the uterus fuse bilaterally at the 4–6 o’clock and 6–8 o’clock positions around the cervix in the region of the cervical–vaginal junction. Ordinarily, when 5–10 mL of 1% lidocaine or its equivalent is injected into these areas, interruption of the sensory input from the cervix and uterus promptly follows.
Many now consider paracervical block to be contraindicated in obstetrics because of the potential adverse fetal effects. Many reports in the literature place the incidence of fetal bradycardia at 8–18%. However, recent work with accurate fetal heart rate monitoring associated with continuous uterine contraction patterns suggests that the incidence is closer to 20–25%. Some researchers have attempted to investigate the significance of the bradycardia. One explanation is that an acid–base disturbance in the fetus does not occur unless the bradycardia lasts longer than 10 minutes and that neonatal depression is rare unless associated with delivery during the period of bradycardia. There seems to be little difference in the incidence and severity of fetal bradycardia by paracervical block between complicated and uncomplicated patients. Other disadvantages of paracervical block include maternal trauma and bleeding, fetal trauma and direct injection, inadvertent intravascular injection with convulsions, and short duration of the block.
F. Pudendal Nerve Block
Pudendal block has been one of the most popular of all nerve block techniques in obstetrics. The infant is not depressed, and blood loss is minimal. The technique is simplified by the fact that the pudendal nerve approaches the spine of the ischium on its course to innervate the perineum. Injection of 10 mL of 1% lidocaine on each side will achieve analgesia for 30–45 minutes approximately 50% of the time.
Both the transvaginal and transcutaneous methods are useful for administering a pudendal block. The transvaginal technique has important practical advantages over the trans-cutaneous technique. The “Iowa trumpet” needle guide can be used, and the operator’s finger should be placed at the end of the needle guide to palpate the sacrospinous ligament, which runs in the same direction and is just anterior to the pudendal nerve and artery. Appreciating the sensation of the needle puncturing the ligament usually is difficult. This facet of the technique (no definite end point) may make it difficult for the inexperienced clinician to perform. Aspiration of the syringe for possible inadvertent entry into the pudendal artery should be accomplished, and, if no blood is returned, 10 mL of local anesthetic solution should be injected in a fanlike fashion on the right and left sides. The successful performance of the pudendal block requires injection of the drug at least 10–12 minutes before episiotomy. Often in clinical practice, pudendal block is performed within 4–5 minutes of episiotomy, so the local anesthetic may not have adequate time to take effect.
1. Advantages and disadvantages—Advantages of pudendal nerve block are its safety, ease of administration, and rapidity of onset of effect. Disadvantages include maternal trauma, bleeding, and infection; rare maternal convulsions due to drug sensitivity; occasional complete or partial failure; and regional discomfort during administration.
The pudendal perineal block, like any other nerve block, demands some technical experience and knowledge of the innervation of the lower birth canal. Nevertheless, in spite of a well-placed bilateral block, skip areas of perineal analgesia may be noted. The possible reason is that although the pudendal nerve of S2–S4 derivation does contribute to the majority of fibers for sensory innervation to the perineum, other sensory fibers also are involved. For example, the inferior hemorrhoidal nerve may have an origin independent from that of the sacral nerve and therefore will not be a component branch of the pudendal nerve. In this case, it must be infiltrated separately. In addition, the posterior femoral cutaneous nerve (S1–S3) origin may contribute an important perineal branch to the anterior fourchette bilaterally. In instances in which this nerve plays a major role in innervation, it must be blocked separately by local skin infiltration.
Two other nerves contribute to the sensory innervation of the perineum: the ilioinguinal nerve, of L1 origin, and the genital branch of the genitofemoral nerve, of L1 and L2 origin. Both of these nerves sweep superficially over the mons pubis to innervate the skin over the symphysis of the mons pubis and the labium majus. Occasionally, these nerves must also be separately infiltrated to provide optimal perineal analgesic effect. Thus it should be apparent that a simple bilateral pudendal nerve block may not be effective in many cases. For maximum analgesic effectiveness, in addition to a bilateral pudendal block, superficial infiltration of the skin from the symphysis medially to a point halfway between the ischial spines may be necessary. Thus a true perineal block may be regarded as a regional technique.
Either lumbar epidural or caudal epidural block should eradicate pain between the T10 and S5 levels for the second stage. All of these nerves are denervated because they all are derived from L1–S5 segments.
2. Procedure (Fig. 24–5)
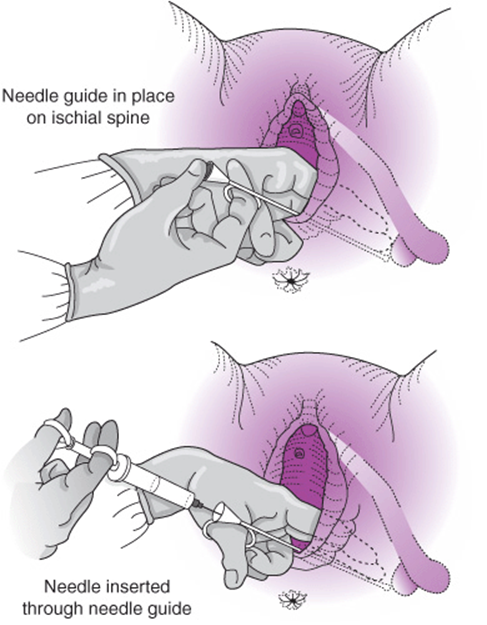
Figure 24–5. Use of needle guide (“Iowa trumpet”) in pudendal anesthetic block. (Reproduced, with permission, from Benson RC. Handbook of Obstetrics & Gynecology. 8th ed. Los Altos, CA: Lange; 1983.)
1. Palpate the ischial spines vaginally. Slowly advance the needle guide toward each spine. After placement is achieved, the needle is advanced through the guide to penetrate approximately 0.5 cm. Aspirate, and if the needle is not in a vessel, deposit 5 mL below each spine. This blocks the right and left pudendal nerves. Refill the syringe when necessary, and proceed in a similar manner to anesthetize the other areas specified. Keep the needle moving while injecting and avoid the sensitive vaginal mucosa and periosteum.
2. Withdraw the needle and guide approximately 2 cm and redirect toward an ischial tuberosity. Inject 3 mL near the center of each tuberosity to anesthetize the inferior hemorrhoidal and lateral femoral cutaneous nerves.
3. Withdraw the needle and guide almost entirely and then slowly advance toward the symphysis pubica almost to the clitoris, keeping approximately 2 cm lateral to the labial fold and approximately 1–2 cm beneath the skin. Injection of 5 mL of lidocaine on each side beneath the symphysis will block the ilioinguinal and genitocrural nerves.
If the procedure explained is carefully and skillfully done, only slight discomfort will be felt during the injections. Prompt flaccid relaxation and good anesthesia for 30–60 minutes can be expected. A summary of anesthetic approaches in labor is shown in Figure 24–6.
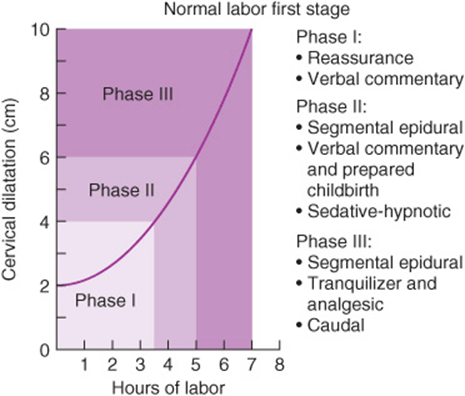
Figure 24–6. First-stage management in a primipara can be divided into 3 phases. Phase I (early labor) should be managed by simple reassurance and verbal commentary if the patient has received adequate antepartum education. An epidural may be performed once labor is well established. Phase II can be handled by a segmental epidural block, continued reassurance, a sedative–hypnotic drug, a narcotic, or a tranquilizer. Phase III, the accentuated phase of labor, can be handled by segmental epidural block, a combination tranquilizer and analgesic, or a caudal epidural block. However, use of reassurance and verbal commentary in conjunction with prepared childbirth methods may be adequate for some patients to tolerate the discomfort of phase III labor.
Prevention & Treatment of Local Anesthetic Overdosage
The correct dose of any local anesthetic is the smallest quantity of drug in the greatest dilution that will provide adequate analgesia. The pregnant patient is more likely to have an intravascular drug injection because of venous distention in the epidural space and may be more susceptible to the toxic effects of local anesthetics (Table 24–3). Injection of the drug into a highly vascularized area will result in more rapid systemic absorption than, for example, injection into the skin. To prevent too-rapid absorption, the operator can add epinephrine to produce local vasoconstriction and prolong the anesthetic. A final concentration of 1:200,000 is desirable, especially when a toxic amount is approached. Epinephrine is contraindicated in patients with increased cardiac irritability of medical or drug origin.
Table 24–3. Toxic doses of local anesthetics commonly used in obstetrics.
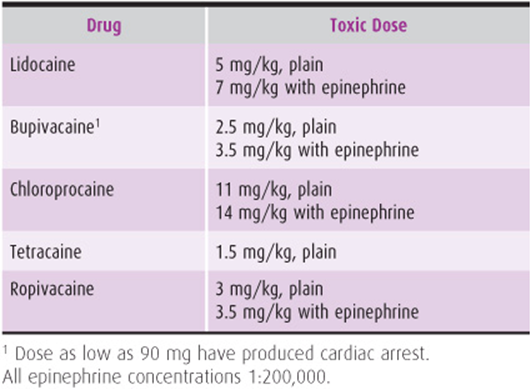
Treatment of local anesthetic overdosage manifested by central nervous system toxicity (a convulsion) is generally achieved effectively and without incident. However, the clinician must be aware of certain basic principles. These include the recognition of prodromal signs of a central nervous system toxic reaction and immediate treatment as required. A toxic central nervous system reaction to local anesthetics consists of ringing in the ears, diplopia, perioral numbness, and deep, slurred speech. An adequate airway must be maintained, and the patient should receive 100% oxygen, with respiratory assistance if necessary. Protection of the patient’s airway and immediate injection of thiopental 50 mg or midazolam 1–2 mg usually stop the convulsion immediately. Succinylcholine was recommended in the past, but it is a potent neuromuscular relaxant that requires placement of an endotracheal tube with positive-pressure ventilation. Studies have indicated that cellular metabolism is greatly increased during convulsive episodes so that a definite increase in cellular oxygenation occurs—hence the use of a depressant selective for the hypothalamus and thalamus because these sites are the foci of irritation.
Local anesthetics-induced cardiotoxicity, especially by bupivacaine, is serious consequence when local anesthetic overdosage happens. The treatment of this complication is usually difficult, and the patient may suffer from arrhythmias (ventricular tachycardia) to even cardiac arrest. Intralipid intravenous infusion is recommended for bupivacaine-induced cardiotoxicity. Current guidelines suggest that 20% lipid emulsion initially be administered as a bolus of 1.5 mL/kg over 1 minute. After completion of the bolus, a continuous infusion of 0.25 mL/kg/min should be started. If the patient does not respond to the initial bolus, 1 to 2 additional boluses may be administered. The rate of the infusion may be increased to 0.5 mL/kg if there is persistent hypotension. The infusion should be continued until 10 min after the patient regains hemodynamic stability. An upper limit of 10 mL/kg is the recommended upper limit for administration in 30 minutes. Any patient that has had local anesthetic toxicity should be monitored for 12 hours after the event, as recurrence of cardiovascular instability has been shown to occur even after lipid administration.
ANESTHESIA FOR CAESAREAN DELIVERY
With few exceptions, all caesarean deliveries in the United States are performed with spinal, epidural, or general anesthesia. Maternal and neonatal outcomes are good when these techniques are performed effectively. In 1982, more than half of the caesarean births in the United States were performed under general anesthesia. By 1998, the rate had dropped to less than 10% of all caesarean births. Spinal anesthesia has become more common than epidural anesthesia for caesarean delivery in the past few years, primarily as a result of the introduction of newer spinal needles that prevent post–lumbar puncture headaches. Although the majority of anesthesia-related maternal mortality is associated with caesarean birth, the rate has continued to decline dramatically over the last few decades and now is less than 1.5 anesthesia-related deaths per million live births in the United States.
Regional Analgesia
A. Lumbar Epidural Block
Lumbar epidural blockade can be used for caesarean analgesia and adequate analgesia for operative delivery. As mentioned in the discussion of regional anesthesia, the major hazard of the regional analgesic technique is blockade of sympathetic fibers and a decrease in vascular resistance, along with venous pooling and hypotension. However, this can be greatly alleviated by elevating the patient’s right hip to prevent compression of the vena cava by the gravid uterus when the patient is lying on the operating table. In addition, the anesthesiologist can rotate the operating table 15–20 degrees to the left to rotate the uterus away from the vena cava.
An epidural catheter can be placed immediately before surgery, or a catheter used to provide pain relief for labor can be reinjected for the surgery. After the catheter is suitably placed and taped in position, the patient should be rotated slightly out of the supine position to remove the hazard of vena cava occlusion when local anesthetic is injected as a test dose. Lidocaine 2% with epinephrine 1:200,000 can be used, or lidocaine 2% without epinephrine can be used if cardiovascular instability is present. Bupivacaine 0.5% or mepivacaine 1.5% with or without epinephrine (as described for lidocaine) also can be used. The total dosage for the therapeutic test is approximately 3 mL, which is an adequate amount to ascertain whether or not inadvertent subarachnoid injection of the drug has occurred. Incremental injections of 5 mL are then titrated to produce a T4–T6 sensory level. Usually a total volume of 18–20 mL of local anesthetic is required.
The blood pressure is monitored every 5 minutes and the dermatome levels examined every 5 minutes for the first 20 minutes to ascertain the height and density of the analgesic block. Usually a waiting period of only 15–20 minutes is needed for adequate analgesic block for incision. During this time, the patient’s abdomen is surgically scrubbed and prepared and the patient draped for caesarean delivery. If a brief episode of hypotension occurs, the patient is given a rapid infusion of lactated Ringer’s solution. In addition, the uterus must be shifted away from the vena cava. If these measures are not sufficient to relieve a brief episode of hypotension, 5–10 mg of ephedrine or 50–100 μg of phenylephrine can be administered intravenously for a mild vasopressor effect.
B. Subarachnoid Block
Spinal block is now the most common anesthesia used for elective caesarean delivery in the United States. The advantages are immediate onset of analgesia, so no waiting period is needed for the block to become effective, and the absence of drug transmission from the maternal to the fetal compartment because the anesthetic is deposited in the subarachnoid space in such small quantities. In addition, subarachnoid block may be a simpler technique to perform because the end point is definite—the identification of fluid from the subarachnoid space. The disadvantages are a more profound and rapid onset of hypotension and more frequent nausea and vomiting due either to unopposed parasympathetic stimulation of the gastrointestinal tract or to hypotension. Subarachnoid block usually is achieved via the paramedian or midline technique, details of which are beyond the scope of this text. The agents most commonly used for subarachnoid analgesia are lidocaine 5% (50–75 mg) and bupivacaine 10–12.5 mg. As with the lumbar epidural technique, the patient is prehydrated with 500–1000 mL of lactated Ringer’s solution.
After the technical aspects of the procedure have been completed, the patient is placed in the supine position with the uterus displaced to the left as described. If hypotension occurs, the uterus should be pushed farther to the left to improve return of blood from the lower extremities into the circulation and increase right atrial pressure and thus cardiac output, and a bolus of Ringer’s lactate should be given. If these measures are not successful, the patient should receive ephedrine 5–10 mg or phenylephrine 50–100 μg intravenously to sustain a mild vasopressor effect. During a period of hypotension, the mother should receive oxygen by mask to increase oxygen delivery to the uteroplacental bed. Newer spinal needles are associated with a low incidence (1–2%) of spinal headache (PDPH). As a result, spinal anesthesia is becoming more popular for elective caesarean surgery.
C. Combined Spinal-Epidural Anesthesia
The combination of spinal and epidural technique (CSE) has increased in popularity and may provide rapid and effective anesthesia for caesarean delivery. Advantages of CSE include the rapid onset of surgical anesthesia with a smaller spinal dose and ability to extend the duration by activation of epidural anesthesia. The use of smaller local anesthetic dose may decrease the incidence of maternal hypotension, which can be significantly detrimental both to the mother and the fetus.
General Anesthesia
General anesthesia is indicated for caesarean delivery when regional techniques cannot be used because of coagulopathy, infection, hypovolemia, or urgency. Some patients prefer to be “put to sleep” and refuse regional techniques.
Ideally, general anesthesia for caesarean delivery should cause the mother to be unconscious, feel no pain, and have no unpleasant memories of the procedure; the fetus should not be jeopardized, with minimal depression and intact reflex irritability.
General anesthesia for caesarean delivery is substantially modified from the typical nonobstetric technique. A rapid sequence technique is used with cricoid pressure to prevent aspiration, with recognition that the risks for the term obstetric patient include (1) full stomach (and aspiration), (2) difficulty with laryngoscopy and intubation, and (3) rapid desaturation if intubation is unsuccessful.
A. Patient Preparation
Preoperative medication usually is not required when the patient is brought to the caesarean section room. Alert the patient preoperatively that she may have a lucid “window” during the operative procedure when she experiences pain or hears voices. Explain that the condition results from the need to maintain a light analgesic state in order to protect the fetus from large doses of drugs. The patient should be prepared with 30 mL of nonparticulate antacid to offset gastric acidity. The patient is given 100% oxygen with a close-fitting mask for 3 minutes before induction.
B. Procedure
When the surgeon is ready to make the incision, thiopental 2.5 mg/kg should be injected intravenously and cricoid pressure exerted by an assistant. Immediately, succinylcholine 120–140 mg intravenously should be administered, and intubation and inflation of the cuff performed. Intubation is confirmed by auscultation and monitoring end-tidal CO2 before the cricoid pressure is released and the incision made. After 6–8 breaths of 100% oxygen, the patient should be given nitrous oxide 50% with oxygen 50% until delivery of the fetus. Low concentrations of halothane or isoflurane (0.5%) will reduce the incidence of awareness. Intermediate-acting muscle relaxants maintain paralysis. An attempt must be made to keep the induction-to-delivery time under 10 minutes. Five minutes is required for redistribution of barbiturate back across the placenta into the maternal compartment. After delivery of the fetus, the nitrous oxide concentration can be increased to 70% if oxygen saturation is more than 98% and intravenous narcotics and benzodiazepines injected for supplemental anesthesia.
The patient should be fully awakened and on her side before extubation. Postoperative analgesia can be provided by patient-controlled administration of morphine or meperidine.
With this approach, good neonatal outcomes are anticipated if induction-to-delivery times and uterine entry-to-delivery times are kept to a minimum.
Local Anesthesia
Local infiltration anesthesia as a primary technique for caesarean delivery is very rarely used. When used, local anesthesia is performed to provide supplemental anesthesia in patients with inadequate epidural or spinal blockade. However, there may be situations when regional or general anesthesia is not immediately available, and caesarean delivery under local anesthesia may be necessary for fetal indications (eg, prolonged fetal bradycardia during the first stage of labor). The general nerve supply of the abdominal wall is composed of 6 of the lowest thoracic nerves, the ilioinguinal and the iliohypogastric nerves bilaterally. The 3 primary nerves that make up the sensory input from the abdomen all end as anterior cutaneous nerves in the abdominal wall. For emergent caesarean delivery, one can use 1% lidocaine in a 10-mL syringe with a 3.5-inch 25-gauge spinal needle injected just under the skin from the umbilicus to near symphysis pubis. If the knife follows this line during incision, the patient will not feel pain. Then, the subcutaneous, muscle and rectal sheath layers are injected as the abdomen is opened. This is the most rapid method for analgesia and delivery by caesarean section and may be a choice in cases in which anesthesia is not available or possible for a period of time. The major disadvantages of local infiltration are the potential for systemic toxicity and technical difficulties in providing adequate anesthesia for surgery, but it can be life-saving for the fetus when immediate delivery is needed for fetal indications.
ANESTHESIA FOR SPECIAL OBSTETRICAL CIRCUMSTANCES
Multiple Gestations
A. Psychoanalgesia
The psychoprophylactic technique helps to prepare the patient for the intrapartum experience. When the labor progresses normally, psychoanalgesia can effectively reduce apprehension and enhance the pleasurable aspects of childbirth. It also may prepare the patient for an understanding of some of the complications of multiple gestations (uterine inertia in the first stage of labor, uterine atony in the third stage, and possible need for caesarean delivery) and reduce the total amount of drugs required for analgesia.
B. Pudendal Nerve Block
Pudendal nerve block usually is reserved for cases in which epidural block is not available. Analgesia is more limited and does not provide as effective analgesia should version or breech extractions of the second twin be required.
C. Epidural Block
This technique is useful as a first-stage analgesic method, but only a segmental type should be used (T10–L2) to prevent the increased hazard of hypotension secondary to a combined large-segment sympathetic block and vena cava occlusion. Ideal management entails the use of lumbar epidural block for the first stage of labor and low caudal block for the late second stage of labor. Epidural anesthesia does not affect fetal outcome with twin delivery but has the advantage of enabling the obstetrician to intervene more easily if the second twin presents abnormally. The need for a general anesthetic can be avoided if an epidural is in place and a caesarean section is required urgently for delivery of the second twin.
D. Spinal Block
The low subarachnoid block is rarely used at the end of the second stage for crowning, delivery, and episiotomy. A low spinal block does not provide a sufficiently high block for caesarean section should it be required urgently (eg, in malpresentation or cord prolapse of the second twin). Therefore, an epidural anesthetic is always preferable for the labor and delivery of multiple births.
E. Inhalation Analgesics
Nitrous oxide is the only inhalation anesthetic that is analgesic at low concentrations. Experience is needed to use nitrous oxide safely because the pregnant patient is sensitive to the drug’s anesthetic effects and she can easily become obtunded. Loss of airway reflexes and aspiration are causes of maternal mortality.
General endotracheal anesthesia can be used for caesarean delivery of twins. Neonatal depression is more likely if the induction-to-delivery time is long (>8 minutes), especially if the uterine incision-to-delivery time also is prolonged (>3 minutes).
Midforceps Delivery
Midforceps delivery is rarely used in current practice given the limited number of practitioners skilled in the technique. Midforceps delivery generally involves both rotation and traction. Therefore, the anesthetic regimen must provide relaxation as well as analgesia for the perineum, lower vagina, and upper birth canal. In order for the obstetrician to perform the procedures necessary for delivery, optimal conditions must be provided so that maternal and fetal trauma can be minimized. Regional analgesia with a lumbar, caudal, epidural, or subarachnoid block is preferred because these blocks provide analgesia and optimal relaxation.
The Trapped Head
On the rare occasion when breech delivery is complicated by a trapped head, the application of forceps or other manipulations may be required urgently. If an epidural block is in place, no further analgesia will be required; however, if one is not in place, immediate anesthesia and pelvic relaxation will be required to facilitate rapid delivery and minimize trauma. The best technique for this purpose is general anesthesia with halothane after suitable protection of the patient from the hazards of aspiration. Protection should include use of antacid 30 mL orally and adequate oxygenation, followed by thiopental 200 mg intravenously, succinylcholine 80–100 mg intravenously, and rapid intubation with cricoid pressure. Another approach described in the literature is administration of 50–100 μg intravenous nitroglycerin to relax the lower uterine segment.
Preeclampsia–Eclampsia
This syndrome is classically described as the proteinuric hypertension. However, it can affect multiple organ systems and be associated with other variants, the most notable being HELLP syndrome, the constellation of hemolysis, elevated liver enzymes and low platelet count. Preeclampsia–eclampsia accounts for approximately 20% of maternal deaths per year in the United States. The primary pathologic characteristic of this disease process is generalized arterial spasm and endothelial dysfunction. As gestation lengthens, there is a tendency toward a fluid shift from the vascular to the extravascular compartment with resultant hypovolemia—in spite of an expanded extracellular fluid space.
It is estimated that nearly 50% of eclamptic patients who die have myocardial hemorrhages or areas of focal necrosis. Major disorders of central nervous system function probably are caused by cerebral vasospasm. Optimal anesthetic management of these patients during the intrapartum period must include a careful preanesthetic evaluation of the cardiovascular and central nervous systems.
The physiologic changes of severe preeclampsia–eclampsia are exaggerated by regional block as a result of restricted intravascular volume, which may lead to considerable depression of blood pressure. Small subgroups of these patients suffer from reduced cardiac output (compared with normal pregnancy), decreased intravascular fluid space, and marked increases in SVR. Patients with severe hemodynamic changes may require direct monitoring of pulmonary artery and wedge pressures to manage labor and the effects of epidural anesthesia. Uterine blood flow is increased with epidural block because of the favorable reduction of SVR, as long as central filling pressures and mean arterial pressure are well maintained.
Regional and general anesthesia is used in the management of preeclamptic patients. Contraindications to regional anesthesia include coagulopathy and urgency for delivery in the setting of nonreassuring fetal testing. The latter may mitigate against taking excessive time for placing a spinal or epidural if the baby requires immediate delivery.
Epidural anesthesia may be preferred to spinal anesthesia in cases of severe hypertension. The more graduated onset of sympathetic block with this technique is thought to produce less hypotension than would occur with spinal block. However, recent evidence suggests that adequate volume preloading of these patients, who by definition are depleted intravascularly, results in similar hemodynamic responses to both regional techniques. More study is required to confirm these findings. However, spinal and epidural anesthesia now usually is encouraged for the management of preeclamptic patients. Obstetricians have become aware that epidural anesthesia is a valuable adjunct in the management of hypertension as a result of the pain relief as well as the vasodilation produced by epidural block. In the past, epidural anesthesia was avoided because of an exaggerated concern over hypotension; now epidural anesthesia is encouraged if the patient’s volume status is well managed and if coagulopathy does not complicate the clinical picture.
Hemorrhage and Shock
Intrapartum obstetric emergencies demand immediate diagnosis and therapy for a favorable outcome for the mother and fetus. Placenta previa and abruptio placentae can be accompanied by serious maternal hemorrhage. Aggressive obstetric management may be indicated, but superior anesthetic management will play a major role in reducing maternal and fetal morbidity and mortality rates. The primary threat to the mother is blood loss, which reduces her effective circulating blood volume and her oxygenation potential. Similarly, the chief hazard to the fetus is diminished uteroplacental perfusion secondary to maternal hypovolemia and hypotension. The perinatal mortality rate associated with placenta previa and abruptio placentae ranges from 15–20% in some studies and up to 50–100% in other studies. The overall morbidity and mortality rates for both the fetus and the mother depend on the gestational age and health of the fetus, the extent of the hemorrhage, and the therapy given.
Good anesthetic management demands early consultation. Reliable intravenous lines should be established early. In addition, recommendations for treatment and control of shock must be formulated. Prompt caesarean delivery often is indicated. Ketamine can support blood pressure for induction. A modified nitrous oxide–oxygen relaxant method of general anesthesia will provide improved oxygenation for both the mother and the fetus and will have a minimal effect on maternal blood pressure. As surgery progresses, it may be necessary to administer large volumes of warm blood, intravenous fluids, or even vasopressors when imperative. Regional block is contraindicated in the presence of hypovolemia.
Umbilical Cord Prolapse
Umbilical cord prolapse is an acute obstetric emergency that is a critical threat to the fetus. Often, because of confusion, irrational behavior by the medical staff may threaten the mother’s life. For example, a haphazard rapid induction of anesthesia without attention to many of the essential safety details may be attempted. Naturally, prolapse of the umbilical cord is incompatible with fetal survival unless the fetal presenting part is elevated at once and maintained in that position to avoid compression of the cord. There then should be adequate time for methodical, safe induction of anesthesia. General anesthesia is induced as soon as the abdomen is prepped and draped. In the rush of the emergency situation, the anesthesiologist must remain meticulous in his or her assessment and management of the mother’s airway. A failed intubation and its consequent cardiorespiratory arrest constitute the leading cause of anesthetic maternal mortality.
Breech Delivery
Epidural anesthesia can be used for the labor patient with a breech presentation. The need for breech extraction is not increased by the use of epidural anesthesia, and a functioning epidural may prevent the need for general anesthesia should an emergency arise at delivery.
If an epidural block is not in place at the time of delivery, the anesthesiologist must be prepared to proceed with an immediate endotracheal general anesthesia if the after-coming fetal head becomes trapped. Drugs, monitors, and anesthetic equipment must be prepared in anticipation of such an event.
Because vaginal breech delivery is associated with an increased risk of perinatal mortality in singleton pregnancies, excellent communication and cooperation between the obstetrician and the anesthesiologist is greatly needed to succeed in an atraumatic delivery. Instead of vaginal delivery, most obstetricians perform caesarean delivery for singleton fetuses in breech presentation now.
Emergency Caesarean Section
General anesthesia is the technique most suitable for the urgent cesarean delivery. It entails placement of an endotracheal tube with an inflated cuff to protect the patient from aspiration of gastric contents into the lung after administration of adequate barbiturate and a muscle relaxant to facilitate endotracheal intubation. Several safety measures must be taken. (1) Give 30 mL of a nonparticulate antacid (sodium citrate) within 15 minutes of induction. (2) Accomplish denitrogenation with 100% oxygen by tight-fitting mask. (3) Inject thiopental 2.5 mg/kg intravenously. (4) Apply cricoid pressure. (5) Give succinylcholine 100–120 mg intravenously. (6) Intubate the trachea and inflate the cuff. (7) Give 6–8 deep breaths of 100% oxygen. (8) Continue to administer nitrous oxide 50% with oxygen 50%, half minimum alveolar concentration (MAC) of volatile agents, and maintain relaxation with muscle relaxants. (9) Supplement with short-acting narcotics and midazolam after the baby is delivered.
These steps should be instituted rapidly and with effective communication between the anesthesiologist and the obstetrician, who should be scrubbed and prepared to make the incision. With this technique, anesthesia can be induced and the fetus delivered within 30 minutes from the time caesarean section is ordered. To prevent vena cava occlusion from the gravid uterus, a wedge should be placed under the patient’s right hip or the operating table rotated slightly to the left.
ANESTHESIA FOR NONOBSTETRIC COMPLICATIONS
Anesthesiologists use the following classification system developed by the American Society of Anesthesiologists (ASA). It is used in both emergency and nonemergent situations to record physical status and to ascertain that proper materials are available for the anticipated procedure.
Class 1: No organic, physiologic, biochemical, or psychiatric disturbance
Class 2: Mild to moderate systemic disturbance that may or may not be related to the reason for surgery, eg, heart disease that only slightly limits physical activity, essential hypertension, anemia, extremes of age, obesity, chronic bronchitis)
Class 3: Severe systemic disturbance that may or may not be related to the reason for surgery (eg, heart disease that limits activity, poorly controlled hypertension, diabetes mellitus with vascular complications, chronic pulmonary disease that limits activity)
Class 4: Severe systemic disturbance that is life-threatening with or without surgery (eg, congestive heart failure, crescendo angina pectoris, advanced pulmonary, renal, and hepatic dysfunction)
Class 5: Moribund patient who has little chance of survival but is submitted to surgery as a last resort (resuscitative effort) (eg, uncontrolled hemorrhage as from a ruptured abdominal aneurysm, cerebral trauma, pulmonary embolus)
Emergency operation (E): Any patient in whom an emergency operation is required (eg, otherwise healthy 30-year-old woman who requires dilatation and curettage for moderate but persistent hemorrhage [ASA class 1E])
Hypertension
Pre-existing hypertensive cardiovascular disease in a pregnant woman should be differentiated from preeclampsia–eclampsia. Unlike the latter, the manifestations of hypertensive disease usually are present before week 20 of pregnancy and persist after delivery. The untreated disease by itself presents a serious challenge to the obstetrician and increases maternal and fetal risk. Chronic hypertension does not specifically contraindicate any of the anesthetic options, but the anesthesiologist must assess and manage abnormalities of volume and vascular resistance to prevent hypotension. Systemic analgesia with sedatives and tranquilizers may be selected for first-stage pain relief, but a hazard still remains.
Heart Disease
Pregnancy superimposed on heart disease presents serious problems in anesthetic management. Patients with functional class I or II rheumatic or congenital heart disease usually fare well throughout pregnancy. Except for patients with fixed cardiac output (moderate to severe aortic stenosis or mitral stenosis), regional analgesia epidural block provides ideal management of first- and second-stage pain relief. This avoids undesirable intrapartum problems such as anxiety, tachycardia, increased cardiac output, and the Valsalva maneuver. The lumbar epidural catheter can be activated for first-stage analgesia with sensory levels of T10 through L2 segments. With the restricted epidural technique, wide variations in blood pressure usually will be avoided and adequate analgesia provided.
Patients with valvular heart disease must be thoroughly assessed before onset of labor so that the anesthesiologist can determine the risks of regional block, tolerance to volume loading, and sympathectomy and determine the need for invasive monitoring. These patients require thorough physical examination, electrocardiography, echocardiography, and Doppler assessment of valve areas and left ventricular function.
Patients with stenotic lesions may not tolerate fluid loading or sympathetic block. Epidural narcotic anesthesia does not provide complete analgesia for labor but may be an appropriate choice if the patient does not tolerate the autonomic effects of local anesthetics. Patients with regurgitant valve lesions generally do well with this afterload reduction of epidural local anesthesia. Central monitoring of preload is indicated with severe lesions.
Marfan’s syndrome and ischemic heart disease require early and aggressive management of labor pain to prevent hypertension and tachycardia. Early lumbar epidural anesthesia with narcotic/local anesthetic mixtures is recommended.
Diabetes Mellitus
Diabetes presents unique problems in anesthetic management because of the hazard to the fetus. The patient with diabetes requires a detailed regimen of antepartum care that extends through the intrapartum and the neonatal period. Moreover, hypotension presents an anesthetic hazard in situations of reduced fetal reserve common to diabetes. The latent phase of labor is best managed with psychological support, mild sedatives, or tranquilizers. The latter part of the first stage can be managed with small intravenous doses of narcotics or epidural block. If labor continues without signs of fetal distress and analgesia for the second stage is desired, either local or pudendal block or epidural or saddle block is appropriate. If a patient is allowed to undergo the stress of labor but fetal decompensation is evident, operative delivery must be performed at once, with emphasis on preventing hypotension. Careful regional block can be used if time permits. If time does not permit placement of a regional block, emergency general endotracheal anesthesia is indicated. Blood glucose levels should be measured intraoperatively because the unconscious patient cannot report hypoglycemia.
Gastrointestinal Difficulties
Gastrointestinal nonstriated muscle has diminished tone and motility during pregnancy. Some medical gastrointestinal difficulties present special problems in management during the intrapartum period. Peptic ulcer often improves during pregnancy, but in some cases the disease worsens in the last trimester and causes serious problems during labor and the immediate postpartum period. Ulcer perforation and hematemesis are rare in labor. Nonetheless, good management of analgesia during delivery is necessary to decrease anxiety and apprehension.
Ulcerative colitis may worsen during pregnancy. Perinatal and maternal mortality rates are not increased because symptomatic management usually is adequate. Regional ileitis may become more severe during pregnancy.
Chronic pancreatitis may be reactivated during pregnancy. Acute pancreatitis occasionally occurs in the third trimester. The significant laboratory values are elevated serum amylase and reduced serum calcium levels, along with typical symptoms of epigastric pain and nausea and vomiting.
Sympathetic blocking techniques are not contraindicated for anesthetic management of the first and second stages of labor in these gastrointestinal disorders that may coincide with pregnancy. It is clinically desirable to alleviate anxiety and apprehension in the first stage of labor because tension may exacerbate the disease process. Therefore, a tranquilizer–narcotic combination early in the first stage of labor should be considered and then lumbar epidural block for first- and second-stage management. Subarachnoid block can be administered to manage the second stage of labor successfully, with use of a true saddle block obtunding chiefly the sacral fibers.
Psychiatric Disorders
Most patients approaching delivery look on the experience as one of the happiest times of their lives. However, some patients undergo severe emotional stress during the third trimester and as delivery nears.
The obstetrician and the anesthesiologist should talk openly with a psychiatric patient about the problems of labor and delivery management and offer suggestions for management of discomfort so that she will have minimal emotional stress. The ideal technique is the combined use of lumbar epidural block for the first stage and lumbar or caudal epidural block for the second stage. It is best to carefully point out to the patient the reasons for choosing the technique and to review the technical points of the procedure so that she will not be alarmed when the block is attempted. These techniques are preferred because they afford early and continuous analgesia during labor and delivery.
TREATMENT OF COMPLICATIONS OF ANESTHETICS
Resuscitation of the Mother
Anesthesia is responsible for 10% of maternal mortality. The most common cause of maternal death is failure to intubate the trachea at induction of general anesthesia. Less frequently, maternal death results from inadvertent intravascular injection of local anesthetic (toxic reaction) or inadvertent intrathecal injection of anesthetic (total spinal).
When faced with maternal cardiovascular collapse, full cardiopulmonary resuscitation (CPR) is indicated:
1. Establish a patent airway.
2. Aspirate mucus, blood, and vomitus with a tracheal suction apparatus. Use a laryngoscope for direct visualization of air passages and intubate the trachea.
3. Administer oxygen by artificial respiration if respirations are absent or weak. If high spinal anesthesia has occurred, continue to ventilate the patient until paralysis of the diaphragm has dissipated.
4. Give vasopressors intravenously (ephedrine 10–20 mg). Place the patient in the wedged supine position with the feet elevated and give transfusions of plasma, plasma expanders, and blood for traumatic or hemorrhagic shock.
5. Specifically treat cardiac arrhythmias in accordance with advanced cardiac life support (ACLS) recommendations.
6. Provide external cardiac massage in the absence of adequate rhythm and blood pressure.
7. Consider immediate caesarean delivery to salvage fetus and improve venous return if the patient does not immediately respond to efforts.
Full cardiopulmonary arrest can be averted if the prodromal symptoms are recognized and treated immediately. A total spinal block is recognized by excessive and dense sensory and motor block to a test injection of local anesthesia through the epidural catheter. Further injections are avoided, and the patient’s blood pressure is supported with fluid, positioning, and vasopressors.
An intravascular injection of local anesthetic is recognized early by symptoms of drowsiness, agitation, tinnitus, perioral tingling, bradycardia, and mild hypotension. The patient should be immediately given 100% oxygen and a small dose of diazepam (5 mg), midazolam (1 mg), or thiopental (50 mg). Further treatment may not be needed. The patient must be watched closely and the epidural catheter removed.
Aya AGM, Mangin R, Vialles N, Ferrer JM, Robert C, Ripart J, de La Coussaye JE. Patients with severe preeclampsia experience less hypotension during spinal anesthesia for elective cesarean delivery than healthy parturients: A prospective cohort comparison. Anesth Analg 2003;97:867–872. PMID: 12933418.
Bucklin BA, Hawkins JL, Anderson JR, et al. Obstetric anesthesia workforce survey: Twenty-year update. Anesthesiology 2005;103:645–653. PMID: 16129992.
Hawkins JL, Chang J, Palmer SK, Charles P, Callaghan WM. Anesthesia-related maternal mortality in the United States: 1979–2002. Obstet Gynecol 2011;117:69–74. PMID: 21173646.
MacKay AP, Berg CJ, Atrash HK. Pregnancy-related mortality from preeclampsia and eclampsia. Obstet Gynecol 2001;97: 533–538. PMID: 11275024.
Mhyre JM. What’s new in obstetric anesthesia in 2009? An update on maternal patient safety. Anesth Analg 2010;111:1480–1487. PMID: 20861422.
Practice guidelines for obstetric anesthesia: An updated report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Anesthesiology 2007;106:843–863. PMID: 17413923.
Toledo P. The role of lipid emulsion during advanced cardiac life support for local anesthetic toxicity. Int J Obest Anesth 2011;20:60–63. PMID: 21112763.
Visalyaputra S, Rodanant O, Somboonviboon W, Tantivitayatan K, Thienthong S, Saengchote W. Spinal versus epidural anesthesia for cesarean delivery in severe preeclampsia: A prospective randomized, multicenter study. Anesth Analg 2005;101:862–868. PMID: 16116005.
Weinberg GL. Lipid infusion therapy: Translation to clinical practice. Anesth Analg 2008;106:1340–1342. PMID: 18420841.
Wong CA, Scavone BM, Peaceman AM, et al. The risk of cesarean delivery with neuraxial analgesia given early versus late in labor. N Engl J Med 2005;352:655–665. PMID: 15716559.