Liselotte Mettler1 , George M. Ogweno2, Rebekka Schnödewind1 and Ibrahim Alkatout1
(1)
Department of Gynecology and Obstetrics, University Hospitals Schleswig-Holstein, Campus Kiel, Arnold-Heller Strasse 3, House 24, 24105 Kiel, Germany
(2)
Gynecologist, Nairobi, Kenya
Liselotte Mettler
Email: endo-office@email.uni-kiel.de
Email: profmettler@gmx.de
URL: http://www.endo-kiel.de
Keywords
LaparoscopyFibroidMyomectomyInfertility
10.1 Introduction
Despite extensive research on the factors involved in the initiation and growth of uterine leiomyomas, the precise causes of these tumors still remain unknown. Chromosomal abnormalities have been found in 40–50 % of uterine leiomyomas [1]. Intrinsic abnormalities of the myometrium, congenitally elevated myometrial estrogen receptors (ER), hormonal changes, or a response to ischemic injury during menstruation may possibly be responsible for the initiation of genetic changes found in these neoplasms [2]. After these changes have developed, they are further influenced by ovarian steroids (promoters) and growth factors (effectors) [3].
The degree to which uterine fibroids contribute to infertility is controversial. It has been estimated that uterine myomas are associated with infertility in 5–10 % of cases by a number of mechanisms [4]. The role of fibroids in infertility was evaluated indirectly by fertility performance after myomectomy. The effect of submucosal, intramural, and subserosal uterine fibroids was also investigated on the reproductive outcome of assisted reproduction treatments (ART) [5]. It is well accepted that the anatomical location of the fibroid is an important factor, with submucosal, intramural, and subserosal fibroids, in decreasing order of importance, being a cause of infertility [6]. Submucosal myoma (SMM) or intramural myoma (IMM) may cause dysfunctional uterine contractility that may interfere with sperm migration, ovum transport, or nidation. Occluded tubes can be caused by intramural fibroids that can hinder the transport of gametes or the migration of spermatozoa. Submucous fibroids can hinder implantation and nidation of the embryo [7].
The benefits of the laparoscopic approach in gynecological surgery are well recognized [8]. Compared with conventional open surgery, it is associated with smaller incisions and better cosmetic results regarding wound healing, less tissue trauma, less blood loss, less postoperative pain, shorter duration of stay in hospital, faster recovery due to early ambulation with an earlier return to work, and subsequent resumption of full activity (Figs. 10.1and 10.2). The major concern about laparoscopic myomectomy (LM) is suboptimal tissue apposition during repair of myometrial defects leading to uterine rupture in subsequent pregnancies. However, if the myometrial repair is performed with the same degree of care as it would be at open myomectomy, there appears to be no reason why the rate of uterine rupture should be higher after LM [9]. This gives more credit to the use of laparoscopically assisted myomectomy (LAM) in selected difficult cases but very little credit if any to the use of the conventional approach. Robotic technology for myomectomy gives even more precise adaption and suturing possibilities but certainly does not increase dampers or side effects. Aspects of LM and pregnancy outcome are discussed in this chapter, not, however, the impact of submucous fibroids or the hysteroscopic approach.
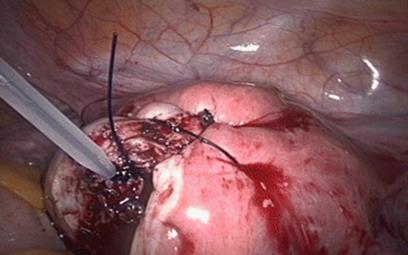
Fig. 10.1
Intraoperative closure after myomectomy with inverted absorbable monofilament suture
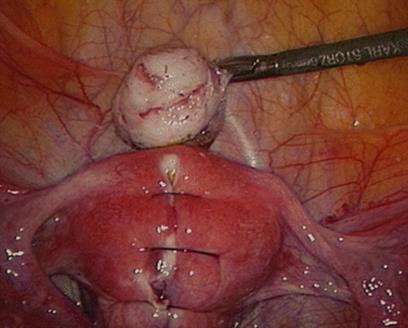
Fig. 10.2
Reconstructed uterine wall and enucleated myoma before morcellation and extraction
10.2 Material and Methods
Laparoscopic myomectomy was performed in patients with symptoms such as disturbed menstrual bleeding, pelvic pain, and infertility.
The laparoscopic enucleation of fibroids always followed the same pattern:
1.
2.
3.
4.
5.
6.
The hysteroscopic enucleation of a submucous fibroid is performed by filling the uterine cavity with Purisole® and then in a continuous movement slicing the fibroid into pieces (electroresection) and retracting the pieces through the cervix. Bleedings can be controlled by pressure release and coagulation with the roller ball or with the cutting loop.
10.2.1 Questionnaire for Patient Data
A questionnaire was sent to 392 patients with fertility problems who were treated by laparoscopy or hysteroscopy at the Department of Obstetrics and Gynaecology, University Hospitals Schleswig-Holstein, Campus Kiel. One hundred and fifty-four patients (40 %) returned the questionnaire that posed questions concerning myomectomies, endometriosis resection, ovarian cyst enucleation, and adhesiolysis.
Patients were evaluated as follows:
· Group A = all patients (n = 392)
· Group B = patients who answered the questionnaire (n = 154)
· Group C = patients from group B who became pregnant (n = 78)
10.3 Results
Of the 392 patients who underwent laparoscopic surgery for fertility problems in our department in 2008/2009, in 129 cases (32 %) myomas (fibroids) were the indication for surgery. Of these 129 patients, in 56 cases (14.3 %) myomas were the only indication for infertility. In 44 cases (11.2 %) myomas appeared together with another disease: in 20 cases (5.1 %) with other genital abnormalities, in 18 cases (4.6 %) with tubal pathology, in 3 cases (0.8 %) with endometriosis, and in 3 cases (0.8 %) with ovarian cysts. The combined appearance of myomas with more than one other genital disturbance was found in 29 patients (7.5 %).
10.3.1 Frequency of the Different Myoma Localizations
Figures 10.3, 10.4, and 10.5 show the frequency of myomas within the whole evaluation. Multiple sites often occurred and this resulted in a higher incidence (n = 140). The location of fibroids were evaluated as diffuse (within the uterine wall), submucous, intramural, subserous, and submucous as well as at multiple locations. Primarily a deep, diffuse myomatosis was found in 60 % of patients in group A, in 62 % of patients in group B, and in 59 % of patients in group C. Submucous fibroids occupied second position in group A (16 %) and subserous fibroids occupied second position in group B (19 %) and group C (21 %). Third position was occupied by subserous fibroids in group A (13 %) and by submucous fibroids in group B (12 %) and group C (14 %). In all three groups, intramural fibroids were the most rarely found: group A (11 %), group B (8 %), and group C (7 %) (Table 10.1).
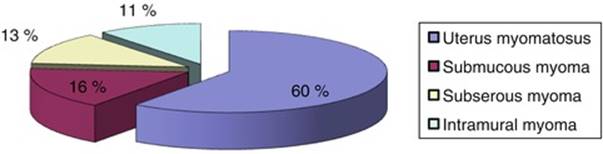
Fig. 10.3
Localization of myomas in the 392 patients (group A)
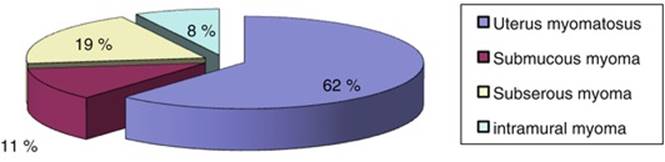
Fig. 10.4
Localization of myomas in the group which answered the questionnaire (group B)
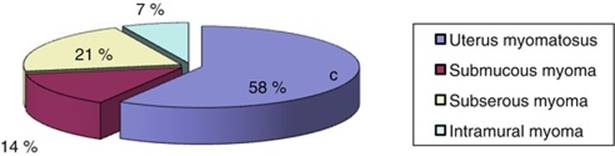
Fig. 10.5
Localization of myomas in the group which became pregnant (group C)
Table 10.1
Frequency of myoma locations in the individual groups, A, B, and C
|
Location |
Group A (all patients) |
Group B (patients who answered the questionnaire) |
Group C (patients who became pregnant) |
|
Combined subserous-intramural |
84 |
32 |
17 |
|
Submucous |
23 |
6 |
4 |
|
Subserous |
18 |
10 |
6 |
|
Intramural |
15 |
4 |
2 |
|
Total |
140 |
52 |
29 |
10.3.2 Side Effects and Symptoms
The following side effects were observed in descending frequency: bleeding abnormalities (33.3 %), tubal patency, degree 1–2 (23 %), adhesions (22 %), and intramural tubal occlusions (15 %).
In 122 patients a laparoscopic myoma enucleation was performed. In 61 % of patients the myomas were situated subserous-intramural, in 18 % submucous, in 13 % subserous, and in 8 % intramural. In 33 patients adhesiolysis was necessary prior to the myomectomy.
Figure 10.6 shows the procedures performed on the 392 patients who underwent laparoscopic surgery for infertility in 2008/2009.
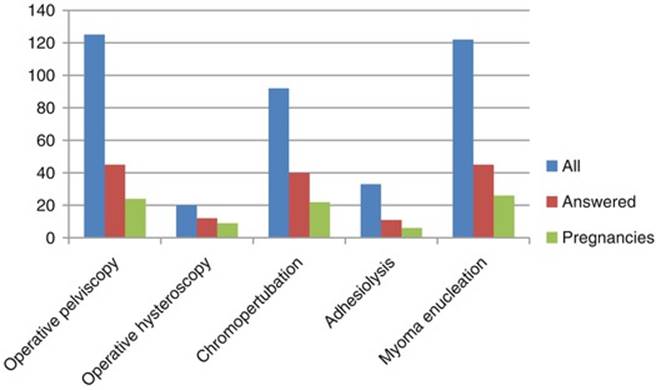
Fig. 10.6
Laparoscopic surgical procedures performed for infertility according to groups A, B, and C
10.3.3 Additional Previous Therapy for Fibroids
Figure 10.7 shows clearly that pregnancy rates increased after pretreatment and surgery.
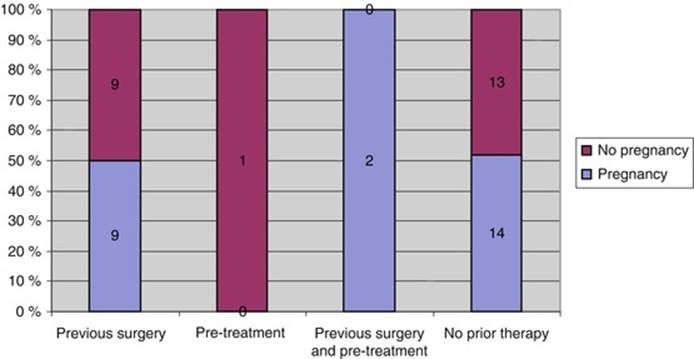
Fig. 10.7
Influence of surgery and pretreatment on pregnancy rates of patients with myomas
10.3.4 Pregnancies and Deliveries
The average age of the evaluated patients was 34.6 years. Different pregnancy rates resulted depending on the localization of the fibroids. The lowest pregnancy rate was achieved after intramural fibroid resection. The resection of intramural-subserous fibroids resulted in a good pregnancy and delivery rate, and the highest pregnancy rate was achieved after submucous fibroid resection (Figs. 10.8 and 10.9).
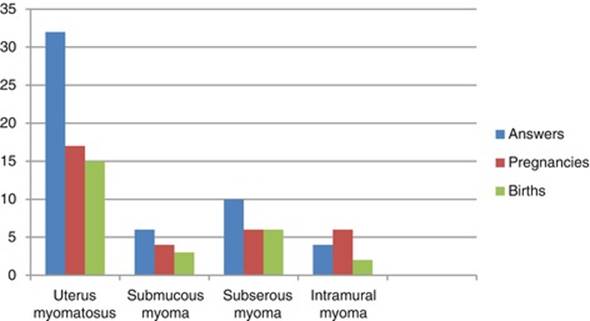
Fig. 10.8
Number of pregnancies and deliveries according to localization of myoma with display of answers
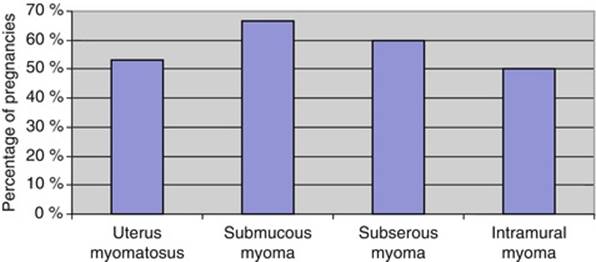
Fig. 10.9
Number of pregnancies according to myoma localization
10.3.5 Mode of Delivery
Eleven of the 129 myomectomy patients underwent a cesarean section. Of these 129 patients, only 25 suffered from myomas alone; all others had multiple morbidities. The 14 pregnancies (56 %) which resulted in this group of 25 led to 12 deliveries (48 %), 5 (42 %) of which were spontaneous and 7 (58 %) cesarean sections. In the group of patients who underwent myomectomy for fertility problems, we had a pregnancy rate of 53 % (n = 17) and a delivery rate of 47 % (n = 15).
10.3.6 Complications
Four complications occurred in the group of myomectomy patients at or after delivery: bladder descensus after delivery, placenta accrete, one uterine rupture, and one emergency cesarean section due to imminent asphyxia of the baby.
10.4 Discussion
Recent advances in endoscopic surgical techniques and the increased sophistication of surgical instruments have offered new operative methods and techniques for the gynecologic surgeon [10]. Recent years have witnessed a marked increase in the number of gynecological endoscopic procedures performed, mainly as a result of technological improvements in instrumentation. Laparoscopy has become an integral part of gynecologic surgery for the diagnosis and treatment of abdominal and pelvic disorders of the female reproductive organs. Endoscopic reproductive surgery intended to improve fertility may include surgery on the uterus, ovaries, pelvic peritoneum, and fallopian tubes.
10.4.1 Laparoscopic Myomectomy and Pregnancy Outcome
Uterine leiomyomas are the most common benign tumors of the female reproductive tract and affect 30–40 % of reproductive-age women. Although they are seldom the sole cause of infertility, myomas have been linked to fetal wastage and premature delivery. Several elements indicate that myomas are responsible for infertility. For example, the pregnancy rate is lower in patients with myomas, and in cases of medically assisted procreation, the implantation rate is lower in patients presenting with interstitial myomas. There is other indirect evidence supporting a negative impact, including lengthy infertility before surgery (unexplained by other factors) and rapid conception after myomectomy [11]. Approximately 50 % of women who have not previously conceived become pregnant after myomectomy [12]. Because medically treated fibroids tend to grow back or recur, most fibroids that cause symptoms are managed surgically (Table 10.2).
Table 10.2
Treatment modalities for uterine leiomyomas
|
Surgical treatment |
Nonsurgical treatment |
Hormonal treatment |
|
Hysterectomy (laparoscopy or laparotomy) |
Myoma embolization |
Gonadotropin-releasing hormone agonists |
|
Abdominal myomectomy |
Magnetic resonance-guided focused ultrasound surgery |
Others (mifepristone, danazol, gestrinone, raloxifene, levonorgestrel-releasing intrauterine system) |
|
Laparoscopic myomectomy (LM) |
||
|
Laparoscopic-assisted myomectomy (LAM) |
||
|
Vaginal myomectomy (VM) |
||
|
Laparoscopic-assisted vaginal myomectomy (LAVM) |
||
|
Hysteroscopic myomectomy |
||
|
Interstitial laser photocoagulation |
||
|
Laparoscopic cryomyolysis |
||
|
Interstitial magnetic resonance imaging-guided thermo-ablation |
||
|
Interstitial magnetic resonance imaging-guided cryotherapy |
||
|
Laparoscopic uterine artery occlusion |
Depending on their number and their location, myomas with mostly intracavitary development should be dealt with by hysteroscopy. Interstitial and subserosal myomas can be operated either by laparotomy or by laparoscopy. Technological advancements in endoscopic instrumentation, equipment, and the surgeon’s expertise have led to an ever-increasing number of informed women choosing the advantages of the new and innovative techniques utilizing hysteroscopy and laparoscopy. Laparoscopy is most often employed in women that are diagnosed early when their fibroids are small and more suited to laparoscopic removal. However, new surgical devices called oscillators allow the safe and efficient removal of fibroid tumors much larger than could have been accomplished in the past. It is imperative to know the size, location, and number of uterine myomas. This is especially important in a laparoscopic approach to myomectomy as tactile feedback is diminished [13].
As fertility preservation is one of the primary goals of myomectomy, the marked reduction of adhesion formation by laparoscopic myomectomy (LM) gives it a distinct advantage over laparotomy. The incidence of adhesions following laparotomic myomectomy and laparoscopic myomectomy is nearly 100 and 36–67 %, respectively [14]. These adhesions can adversely affect fertility, cause pain and small bowel obstructions, and increase the risk of ectopic pregnancy.
Dubuisson et al. studied the risk of adhesions after LM [15]. A second-look procedure was performed in 45 of 271 LM patients. Additional laparoscopic procedures were performed at the time of LM in 19 patients (42.2 %). The overall postoperative adhesion rate was 35.6 %, with 16.7 % of myomectomy sites affected. Most importantly, the adnexal adhesion rate was 24.4 % with 11.1 % bilaterally. In patients without associated laparoscopic procedures, the adhesion rates were even lower, with an overall adhesion rate of 26.9 % and an adnexal adhesion rate of only 11.5 %, none of which was bilateral. Other factors that are related with the increase in the risk of adhesions are depth (intramural and submucosal), posterior location, and suturing.
The factors responsible for prolonged surgical times in LM are the need to morcellate large or multiple fibroids for removal through the trocar and suture repair of the myometrium. Laparoscopically assisted myomectomy (LAM) where myoma enucleation is done laparoscopically or through a 5 cm Pfannenstiel minilaparotomy, following which the uterus could be exteriorized for palpation and multilayered open suturing done, has also been described [16]. This technique combines the advantages of increased exposure, visibility, and magnification provided by the laparoscope (especially for evaluation of the posterior cul-de-sac and under the ovaries) with the ease of adequate uterine repair and removal of specimen that is associated with minilaparotomy.
LAM is a safe alternative to LM and is less difficult and less time consuming. This technique can be used for large (greater than 8 cm), multiple, or deep intramural myomas. Using a combination of laparoscopy and a 2–4 cm abdominal incision, the uterine defect can be closed in three layers to reduce the risk of uterine dehiscence, fistula, and adhesion formation. Women who desire future fertility and require myomectomy for an intramural myoma may benefit from LAM to ensure proper closure of the myometrial incision. Cesarean delivery is recommended in patients who have deep intramural or multiple myomas even if the endometrial cavity is not entered. One of the concerns regarding LM has been adequate reconstruction and healing of the uterine defect with subsequent ability for the uterus to withstand the elements associated with pregnancy and labor.
Concerns have been raised regarding complications of pregnancy after LM, such as uterine dehiscence or rupture. This latter complication is rare and has been reported in women who conceive after both laparotomic myomectomy and laparoscopic myomectomy. Its real incidence remains unknown, as several reports investigating the follow-up of myomectomy failed to document any case of uterine dehiscence. Events leading to uterine scar dehiscence in subsequent pregnancies are thought to include suboptimal suturing of the uterine incision and/or impaired wound healing from extensive use of coagulation or any tissue-destroying modality. This may contribute to adjacent myometrial necrosis, thereby impairing surgical wound healing. At laparotomy, closure of the excision site is usually accomplished by a multilayered suture. With operative laparoscopy, suturing can be cumbersome and tedious, and restoration of the uterine wall integrity to an equivalent manner may be difficult.
There are no data suggesting that any one suturing technique is superior in minimizing this risk – whether continuous or interrupted sutures are placed, whether the knots are tied intracorporally or extracorporally, or whether the suturing is done by hand or a suturing device. Sutures with shorter half-lives or ones that may lose strength in the presence of infection (e.g., chronic) should most likely not be used. All in all, careful closure of the uterine incision with minimal coagulation is most critical [17]. Few cases of dehiscence following LM have been reported to have occurred during the third trimester of pregnancy [18].
Fibroids may also increase the rate of pregnancy complications during the second and third trimesters [19]. Adhesions form in >90 % of abdominal myomectomy cases. The incidence is highest with posterior uterine incisions and lower with fundal or anterior incisions. The laparoscopic approach may reduce this complication but definitive evidence is still lacking [20].
In any case, LM should be performed cautiously. Excess thermal damage should be avoided and adequate uterine repair must be assured using multiple-layer suturing.
Aside from the dehiscence case reports, few studies have evaluated the pregnancy rate after LM [14, 21–26]. Their results are summarized in Table 10.3.
Table 10.3
Pregnancy outcome after laparoscopic myomectomy
|
Author |
No. of patients |
Average number of myomas removed |
Average size of myomas (cm) |
No. of pregnancies achieved |
|
Hasson et al. [14] |
56 |
144 total |
range 3–16 |
15 |
|
Dubuisson et al. [22] |
21 |
2 |
6.2 |
7 |
|
Stringer et al. (1996) |
5 |
2 |
3.6 |
5 |
|
Seinera et al. [24] |
54 |
1 |
4.2 |
5 |
|
Darai et al. [25] |
143 |
1.5 |
5.4 |
19 |
|
Nezhat et al. [21] |
115 |
3 |
5.9 |
42 |
|
Dessolle et al. [26] |
88 |
1.7 (range 1–4) |
6.2 (range 3–11) |
42 |
Additionally, few studies [27, 28] have evaluated the effect of uterine fibroids on the pregnancy rate after assisted reproductive treatment (ART). Eldar-Geva et al. compared 106 ART cycles in patients with uterine fibroids with 318 ART cycles in age-matched patients without fibroids and concluded that implantation and pregnancy rates were significantly lower in patients with intramural or submucosal fibroids, even those with no deformation of the uterine cavity [27]. Stovall et al. showed that even after patients with submucosal fibroids are excluded, the presence of fibroids reduces the efficacy of ART [28]. Therefore, if women with unexplained infertility have a better chance of conception after myomectomy and if the main factors in treatment success are patient age and duration of infertility, this conservative operation should not be postponed for too long.
Although the indications for laparotomy and for laparoscopic surgery for myomectomy are completely different, the fertility results observed after each of these techniques are comparable. Excellent pregnancy rates are obtained for those infertile patients with no other associated factor to explain their infertility. After IVF, implantation rates are better in patients without interstitial myoma. Consequently, the goal of the myomectomy will essentially be to optimize the results of ART, rather than to hope for a spontaneous pregnancy.
10.4.2 Complications
Basically, lacerations at laparoscopic entry by Veress needle and trocar insertion as well as secondary lesions caused by different instruments may occur as vascular, bowel, bladder, ureter, or other organ lesions. They are, unfortunately, more frequent than injuries caused by the procedure itself.
At our department in Kiel in the years 1987–1991, Mecke et al. evaluated 5,035 laparoscopies and found a complication rate of 2 % [29]. In another retrospective study, Kolmorgen investigated laparoscopic complications in preoperated patients compared to patients without previous surgeries and observed a complication rate of 2.15 % among the preoperated patients compared to 1 % in patients without previous surgeries [30]. Myoma enucleations per se do not carry any higher surgical risk whether performed by laparoscopy or laparotomy [31].
10.5 Conclusions
Advances in endoscopic surgery have revolutionized our approach to gynecological surgery. Most fertility operations can be easily and effectively performed laparoscopically. The variety of conditions indicative of surgery demonstrates the importance of maintaining good surgical skills in the practice of reproductive medicine so that patients can be offered the most appropriate treatment. It appears that endoscopic surgery for infertility patients, when performed by an experienced endoscopist, is efficacious and can produce as good as or even better results than conventional procedures. Correct case selection and optimal tissue apposition with good and meticulous laparoscopic suturing are vital and the key to the success of LM. Results so far are encouraging in terms of fertility outcome after laparoscopic myomectomy (LM) in patients in whom myomata are associated with the presence of unexplained infertility.
References
1.
Ligon AH, Morton CC (2000) Genetics of uterine leiomyomata. Genes Chromosomes Cancer 28:235–245PubMedCrossRef
2.
Rein MS (2000) Advances in uterine leiomyoma research: the progesterone hypothesis. Environ Health Perspect 108(suppl 5):791–793PubMedCrossRef
3.
Rein MS, Barbieri RL, Friedman AJ (1995) Progesterone: a critical role in the pathogenesis of uterine myomas. Am J Obstet Gynecol 172:14–18PubMedCrossRef
4.
The Practice Committee of the American Society for Reproductive Medicine (2004) Myomas and reproductive function. Fertil Steril 82(Suppl 1):S111–S116
5.
Rackow BW, Arici A (2005) Fibroids and in-vitro fertilization: which comes first? Curr Opin Obstet Gynecol 17:225–231PubMedCrossRef
6.
Bajekal N, Li TC (2000) Fibroids, infertility and pregnancy wastage. Hum Reprod Update 6:614–620PubMedCrossRef
7.
Vollenhoven BJ, Lawrence AS, Hely DL (1990) Uterine fibroids: a clinical review. Br J Obstet Gynaecol 97:285–298PubMedCrossRef
8.
Dubuisson JB, Chapron C (1996) Laparoscopic myomectomy today. A good technique when correctly indicated. Hum Reprod 11:934–935PubMedCrossRef
9.
Kumakiri J, Takeuchi H, Kitade M et al (2005) Pregnancy and delivery after laparoscopic myomectomy. J Minim Invasive Gynecol 12:241–246PubMedCrossRef
10.
Nezhat C, Winer WK, Cooper JD, Nezhat F, Nezhat C (1989) Endoscopic infertility surgery. J Reprod Med 34(2):127–134PubMed
11.
Rosenfeld DL (1986) Abdominal myomectomy for otherwise unexplained infertility. Fertil Steril 46:328–330PubMed
12.
Verkauf BS (1992) Myomectomy for fertility enhancement and preservation. Fertil Steril 58:1–15PubMed
13.
Berker B et al (2005) Role of laparoscopic surgery in infertility. Middle East Fertil Soc J 10(2):97
14.
Hasson HM, Rotman C, Rana N (1992) Laparoscopic myomectomy. Obstet Gynecol 80:884–888PubMed
15.
Dubuisson JB, Fauconnier A, Chapron C, Krieker G, Norgaard C (1998) Second look after laparoscopic myomectomy. Hum Reprod 13:2102–2106PubMedCrossRef
16.
Nezhat C, Nezhat F, Bess O et al (1994) Laparoscopically assisted myomectomy: a report of a new technique in 57 cases. Int J Fertil 39:34–44
17.
Fisherman G, Jurema M (2005) Myomas and myomectomy. J Minim Invasive Gynecol 12:443–456CrossRef
18.
Pelosi MA, Pelosi MA (1997) Spontaneous uterine rupture at 33 weeks subsequent to previous superficial laparoscopic myomectomy. Am J Obstet Gynecol 177:1547–1549PubMedCrossRef
19.
Ouyang DW, Economy KE, Norwitz ER (2006) Obstetric complications of fibroids. Obstet Gynecol Clin North Am 33:153–169PubMedCrossRef
20.
Hurst BS, Matthews ML, Marshburn PB (2005) Laparoscopic myomectomy for symptomatic uterine myomas. Fertil Steril 83:1–23PubMedCrossRef
21.
Nezhat CH, Nezhat F, Roemisch M, Seidman DS, Tazuke SI, Nezhat CR (1999) Pregnancy following laparoscopic myomectomy: preliminary results. Hum Reprod 14:1219–1221PubMedCrossRef
22.
Dubuisson JB, Chapron C, Chavet X (1996) Fertility after laparoscopic myomectomy of large intramural myomas: preliminary results. Hum Reprod 11:518–522PubMedCrossRef
23.
Stringer NH, Strassner HT (1996) Pregnancy in five patients after laparoscopic myomectomy with the harmonic scalpel. J Gynecol Surg 12:129–133CrossRef
24.
Seinera P, Arisio R, Decko A (1997) Laparoscopic myomectomy: indications, surgical technique and complications. Hum Reprod 12:1927–1930PubMedCrossRef
25.
Darai E, Dechaud H, Benifla JL (1997) Fertility after laparoscopic myomectomy: preliminary results. Hum Reprod 12:1931–1934PubMedCrossRef
26.
Dessolle L, Soriano D, Poncelet C, Benifla JL, Madelenat P, Darai E (2001) Determinants of pregnancy rate and obstetric outcome after laparoscopic myomectomy for infertility. Fertil Steril 76:370–374PubMedCrossRef
27.
Eldar-Geva T, Meagher S, Healy DL, MacLachlan V, Breheny S, Wood C (1998) Effect of intramural, subserosal, and submucosal uterine fibroids on the outcome of assisted reproductive technology treatment. Fertil Steril 70:687–691PubMedCrossRef
28.
Stovall DW, Parrish SB, Van Voorish BJ, Hahn SJ, Sparks AET, Syrop CH (1998) Uterine leiomyomata reduce the efficacy of assisted reproduction cycles: results of a matched follow-up study. Hum Reprod 13:192–197PubMedCrossRef
29.
Mecke H, Heuchmer R, Lehmann-Willenbrock E (1996) Komplikationen bei 5000 Pelviskopien an der Universitätsfrauenklinik Kiel. Geburtshilfe Frauenheilkd 56:449–452PubMedCrossRef
30.
Kolmorgen K (1998) Laparoscopy complications in previously operated patients. Zentralbl Gynakol 120:191–194PubMed
31.
Mettler L (2006) Manual for laparoscopic and hysteroscopic gynecological surgery. Jaypee Brothers Medical Publishers (P) Ltd, New DelhiCrossRef