Charles Sultan1, 2 , Laura Gaspari1, 2, 3 and Françoise Paris1, 2
(1)
Unité d’Endocrinologie-Gynécologie Pédiatriques, Departement de Pédiatrie, Hôpital Arnaud-de-Villeneuve, CHU Montpellier et Université Montpellier1, Montpellier, France
(2)
Service d’Hormonologie (Développement et Reproduction), Hôpital Lapeyronie, CHU Montpellier, Montpellier, France
(3)
Service de Pédiatrie, Hôpital Caremeau, CHU Nîmes, Nîmes, France
Charles Sultan
Email: c-sultan@chu-montpellier.fr
Keywords
HyperandrogenismAdolescentPCOSNCCAHIdiopathic hirsutism
4.1 Introduction
Androgen excess during puberty produces a variety of clinical signs and symptoms that must be appropriately recognized, evaluated, and treated. Acne, hirsutism, and obesity are outward signs of androgen excess, and they therefore must be considered as more than cosmetic concerns. The body image component of sexual identity and peer interactions are critical for the evolving personality. Timely medical intervention may prevent health sequelae and contribute to psychological well-being.
4.2 Definition
Hyperandrogenism (HA) must be considered in an adolescent with [1]:
· Severe acne
· Hirsutism
· Menstrual irregularities
· Abdominal obesity
· Masculinization of the body habitus
· Clitoromegaly
The management of an adolescent girl with HA has three main goals:
1.
2.
3.
4.3 Causes of Hyperandrogenism in Adolescent Girls
In the peripubertal period, HA may be due to the following (Fig. 4.1, Table 4.1):
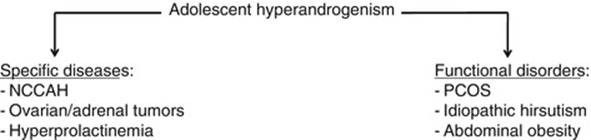
Fig. 4.1
Diagnostic approach to adolescent hyperandrogenism
Table 4.1
Causes of adolescent hyperandrogenism
|
1. Polycystic ovarian syndrome |
|
2. Idiopathic hirsutism |
|
3. Nonclassical congenital adrenal hyperplasia |
|
4. Obesity |
|
5. Transient/idiopathic hyperandrogenism |
|
6. Adrenal: ovarian tumors |
|
7. Hyperprolactinemia |
|
8. Drugs |
· Ovarian disorders, such as PCOS, hyperthecosis, ovarian tumors, and enzymatic defects such as 17-keto-reductase deficiency
· Adrenal disorders, such as NCCAH, Cushing’s disease, or adrenal tumor
· A mixed origin, such as hyperprolactinemia, stress, anorexia nervosa, and elite sport
· A peripheral origin, such as obesity or idiopathic hirsutism
For the last 15 years, we have managed a cohort of 178 adolescent girls with HA in our pediatric endocrinology clinic. The causes of HA were as follows: PCOS (34 %), NCCAH (15 %), abdominal obesity (10 %), idiopathic hirsutism (9 %), elite sport (10 %), anorexia nervosa (6 %), transitory HA (11 %), 46,XY disorder of sex development (46,XY-DSD) (3 %), hyperprolactinemia (2 %), and endocrine tumors (1 %).
4.3.1 PCOS During Puberty
The long-term sequelae of PCOS are well known and continue to present challenges for endocrinologists and gynecologists, who need to make early diagnoses (in the pubertal period) so that these teenagers can be promptly treated both symptomatically and prophylactically. The striking trend toward adolescent obesity should reinforce our responsibilities. Menstrual irregularities in adolescents in the early postmenarcheal years can be an early sign of PCOS. In obese adolescents who subsequently develop glucose intolerance, there is an overall clinical impression that PCOS has become a prevalent cause of hyperandrogenism and menstrual disorders.
There is currently no consensual definition of adolescent PCOS [2]. We propose to define PCOS in the adolescent as the combination of four of the following criteria comprising the PCOS diagnosis (Fig. 4.2):

Fig. 4.2
Pathophysiology of PCOS
· Clinical HA: persistent and severe acne and hirsutism (Ferriman score >10)
· Oligo- or amenorrhea persisting 2 years postmenarche
· Biochemical evidence of HA: T >50 ng/ml, along with dysovulation (LH/FSH ≥2)
· Insulin resistance and hyperinsulinemia: visceral adiposity, acanthosis nigricans, and impaired glucose tolerance
· Polycystic ovarian morphology on ultrasound
There are several clinical expressions of PCOS during adolescence [3]:
· Postmenarcheal PCOS, the most common expression.
· Premenarcheal PCOS.
· Familial PCOS.
· PCOS that occurs in adolescents previously diagnosed with central precocious puberty (CPP).
· PCOS that occurs in adolescents previously diagnosed with intrauterine growth retardation (IUGR) and/or precocious pubarche.
· Early metabolic expression: hyperinsulinism and insulin resistance are present in early puberty.
· In certain elite sports, we have observed PCOS-like symptoms in a significant percentage of adolescent athletes (50 % vs 22 % in the control group) [4].
We propose screening for PCOS in all adolescents with oligo- or amenorrhea that persists 2 years after menarche, with particular attention given to those girls presenting obesity and a history of IUGR, premature pubarche, CPP, or familial history of PCOS.
Diagnosis of PCOS should be based on several criteria (Fig. 4.2):
1.
2.
3.
4.
The aims of treatment are to regulate menses and improve androgenic concerns as well as lifestyle issues. The treatment is based on the following:
· Lifestyle intervention and weight loss, both of which have been found to be beneficial in many areas.
· Antiandrogens (cyproterone acetate, Androcur*: 50 mg/day, day 1–day 20) and natural estrogens (Provames*: 2 mg/day, day 1–day 20).
· Oral contraceptive pills (OCP), if contraception is needed.
· Insulin sensitizers (metformin: 500 mg × 3/day) have been proven useful for regulating menses, inducing ovulation, and normalizing weight [5].
4.3.2 Non-classical CAH
Individuals with non-classical CAH (NCCAH) typically present in late childhood, adolescence, or adulthood with signs and symptoms of excessive androgen production. The prevalence of NCCAH ranges from 0.1 to 0.26 %, but it occurs much more frequently among Ashkenazi Jews (prevalence 1–2 %).
Many women with NCCAH are relatively fertile, but the success rate of women seeking pregnancy is in the range of 60–70 %. This heightened risk of subfertility may be due to ovulatory dysfunction, inadequate endometrial maturation, or impaired embryo implantation secondary to the elevated progesterone levels.
The diagnosis NCCAH is sometimes difficult. Random 17-OH progesterone measurements may show values within the normal range [6]. The gold standard today therefore remains the ACTH stimulation test, which should identify 17-OH progesterone >1,500 ng/dl at the end of the test.
Genetic testing is helpful for diagnosis, especially to identify those individuals with compound heterozygous mutations, and for genetic counseling. Since two thirds of NCCAH women show compound heterozygosity, the predicted incidence is 1 out of 360.
The molecular genetic investigation of individuals with NCCAH has shown that the most common finding is compound heterozygous mutations with a different mutation on each allele:
· Seventy percent of NCCAH: Val 281 Leu (50–82 % loss of 21-OHase).
· Other missense mutations: P30L, P4535, and R339H.
· The phenotype reflects the residual activity of the milder mutation.
Many patients with NCCAH are asymptomatic and thus are not in need of treatment [7].
The symptomatic patients are often prepubertal girls with premature pubarche, girls with accelerated growth velocity and bone age, and adolescents with hirsutism (60 % of cases), oligomenorrhea (53 %), and persistent acne (30 %).
The aims of treatment for NCCAH in adolescents and young women are the following:
· Regularization of the menstrual cycle
· Prevention of progressive hirsutism (acne)
· Improved fertility
NCCAH management includes:
· OCP alone, which is useful in oligomenorrheic, hyperandrogenic adolescents and women not seeking fertility
· Antiandrogens
· Glucocorticoids
4.3.3 Idiopathic Hirsutism
Idiopathic hirsutism (IH) is defined by evidence of clinical HA contrasting with normal androgen levels and no menstrual dysfunction [8]. IH is considered as a hypersensitivity to androgens (short CAG repeat lengths on the androgen receptor in target cells). The current diagnosis of IH should be one of exclusion.
Its prevalence ranges between 10 and 15 % in certain ethnic groups (e.g., of Mediterranean origin).
4.3.4 Obesity
Several studies have suggested that abdominal obesity is linked to HA in peripubertal girls. In addition, peripubertal obesity has been associated with variable degrees of insulin resistance. Compensatory hyperinsulinemia can then increase ovarian and/or adrenal androgen production and lower SHBG, both of which increase free plasma T concentration [9, 10].
In some girls, HA impairs the sensitivity of the GhRH pulse to negative feedback, leading to a persistently rapid GnRH pulse and elevated LH, which maintain or worsen HA.
4.4 Patient Evaluation
The first visit begins with a thorough medical history and careful physical examination. Certain clinical symptoms should draw the clinician’s attention toward serious disease, such as:
· Rapidly progressing hirsutism
· Symptoms of hypercorticism
· Galactorrhea
In most situations, the symptoms of hyperandrogenism are mild, such as hirsutism and acne.
The laboratory investigations are limited to evaluation of plasma T, 17-OH progesterone, and basal plasma LH and FSH; in some situations, however, investigation should include an ACTH stimulation test and/or genetic analysis, along with pelvic US [11, 12].
4.5 Conclusions
1.
2.
3.
References
1.
Hacivelioglu S, Gungor AN, Gencer M, Uysal A, Hizli D, Koc E, Cosar E (2013) Acne severity and the Global Acne Grading System in polycystic ovary syndrome. Int J Gynaecol Obstet 123:33–36PubMedCrossRef
2.
Diamanti-Kandarakis E (2010) PCOS in adolescents. Best practice & research. Clin Obstet Gynaecol 24:173–183
3.
Horn M, Geraci SA (2013) Polycystic ovary syndrome in adolescents: (women’s health series). South Med J 106:570–576PubMedCrossRef
4.
Coste O, Paris F, Galtier F, Letois F, Maimoun L, Sultan C (2011) Polycystic ovary-like syndrome in adolescent competitive swimmers. Fertil Steril 96:1037–1042PubMedCrossRef
5.
Palomba S, Materazzo C, Falbo A, Orio F, La Sala GB, Sultan C (2014) Metformin, oral contraceptives or both to manage oligo-amenorrhea in adolescents with polycystic ovary syndrome? A clinical review. Gynecol Endocrinol 30:335–340PubMedCrossRef
6.
Ghizzoni L, Cappa M, Vottero A, Ubertini G, Carta D, Di Iorgi N, Gasco V, Marchesi M, Raggi V, Ibba A, Napoli F, Massimi A, Maghnie M, Loche S, Porzio O (2011) Relationship of CYP21A2 genotype and serum 17-hydroxyprogesterone and cortisol levels in a large cohort of Italian children with premature pubarche. Eur J Endocrinol 165:307–314PubMedCrossRef
7.
Witchel SF (2013) Non-classic congenital adrenal hyperplasia. Steroids 78:747–750PubMedCrossRef
8.
Azziz R, Carmina E, Sawaya ME (2000) Idiopathic hirsutism. Endocr Rev 21:347–362PubMed
9.
Knudsen KL, Blank SK, Burt Solorzano C, Patrie JT, Chang RJ, Caprio S, Marshall JC, McCartney CR (2010) Hyperandrogenemia in obese peripubertal girls: correlates and potential etiological determinants. Obesity (Silver Spring) 18:2118–2124CrossRef
10.
McCartney CR, Prendergast KA, Chhabra S, Eagleson CA, Yoo R, Chang RJ, Foster CM, Marshall JC (2006) The association of obesity and hyperandrogenemia during the pubertal transition in girls: obesity as a potential factor in the genesis of postpubertal hyperandrogenism. J Clin Endocrinol Metab 91:1714–1722PubMedCrossRef
11.
Dennedy MC, Smith D, O'Shea D, McKenna TJ (2010) Investigation of patients with atypical or severe hyperandrogenaemia including androgen-secreting ovarian teratoma. Eur J Endocrinol 162:213–220PubMedCrossRef
12.
Franks S (2012) The investigation and management of hirsutism. J Fam Plann Reprod Health Care 38:182–186PubMedCrossRef