Bruce Hugman1
(1)
Uppsala Monitoring Centre, Uppsala, Sweden
Bruce Hugman
Email: brucehugman@hotmail.com
Introduction
In this chapter we review the detailed issues, questions and skills in risk communication relevant to medicines for all patients and then focus on challenges of communication with regard to a small selection of medicines for women: anti-convulsant drugs in pregnancy, oral contraceptives, HPV vaccination and Hormone Replacement Therapy (HRT).
The Basics of Risk Communication
Chapter 18 opened with the statement: The purpose of risk communication in clinical practice is to inform and protect; to support wise, balanced and rational decisions that match patients’ wishes and needs. At its heart is risk assessment from the best evidence available and risk management with the purpose of anticipating known or potential risks and taking measures to reduce or avoid them. In everyday life, we know that the risk of domestic fires is high; we manage those risks with smoke-detectors, sprinklers, fire-extinguishers, evacuation plans, escape routes and training and rehearsal. The principles of these activities and the communications associated with them apply to all aspects of life, from oil-rigs to natural disasters, from driving to rock-climbing (Hugman 2013a).
In clinical practice, once a diagnosis has been agreed, the process of risk assessment and risk management begins as the options are discussed:
· What are the risks of the condition?
· What are the risks of no treatment?
· What options for treatment are available?
· What are the benefits and risks of the options available?
· What measures can be taken to avoid or reduce the risks?
Once a treatment has been proposed, its benefits and risks require further discussion before a final choice is agreed. Then further information is necessary about the specific therapy and managing its risks.
MedicineNet.com is an excellent source of intermediate advice for patients and the public, providing up-to-date, simple, well-structured information based on FDA guidance and package inserts. It is one resource among many for patients who want to research the options for themselves, but also provides a fine template for doctors to base their risk communication on.
Once a diagnosis has been made and agreed, all patients should have, and many will actively want to have, the following information about their treatment options:
· What is the drug used for?
· How should the drug be taken?
· What should you do if you miss a dose?
· What are the drug’s side effects?
· What substances interact with the drug?
· What should you expect the drug to do?
· How should the drug be stored?
· Should you use a generic version of the drug?
· What laboratory tests or other observations should be done to monitor the effects of the drug? (Ogbru 2009)
This begins the active process of risk assessment (what are the risks?) and risk management (what action can be taken to reduce risks to the absolute minimum?) This is a stage at which physicians and pharmacists must remember that matters that are familiar and routine to them may not be understood by patients at all. Every element of communication needs to be checked, at least by using ‘teach back,’ that is by asking patients to repeat what they believe they’ve been told (‘Can you just tell me how you're going to take this medicine?’ ‘What will you do if you have any symptoms of side effects?’) Asking, ‘Do you understand?’ is risky, because many people, not wishing to appear foolish or inattentive, will answer, ‘Yes’ whether they understand or not. Those who are illiterate or semi-literate often have very sophisticated strategies for disguising their problems and may understand much less than they appear to.
To make the risk communication aspects of these question clear, here’s an expanded and annotated version of the basic list from MedicineNet:
· What underlies the disease or condition?
· While many conditions will be attributable to specific causes (infection, accident, for example), many others will have their roots in other risk factors and broader causes such as lifestyle issues (diet, exercise, smoking, and so on), working conditions, psychological state of mind, the demands, pressures and risks of women’s lives, and many more. General health, prevention and healing may all be dependent on factors well beyond the presenting problem (injury from intimate partner violence or child abuse being amongst the most blatant), many of them discussed in the previous chapter. Diagnosis and risk communication need a very wide angle of view to embrace consideration of these broad issues and risks
· What is the drug used for?
· Many patients leave their consultation without a clear grasp of their condition and its causes and what their medicine is for; one risk here is that they will simply treat the symptoms without understanding how they came about and what might be done to reduce the chances of recurrence. (Some studies suggest that, unknown to their prescribers, up to one third of patients may not fulfill their prescriptions at all (LaMendola2012), implying strongly that communication with some patients has failed in all its purposes.) A simple example is common and troublesome vaginal candidiasis. Knowledge of the nature of the organism, possible reasons for its emergence as a problem, and what promotes or inhibits its growth is essential, alongside the rationale for topical treatment of symptoms and/or oral or topical anti-fungal treatment of the yeast itself.
· How does the drug work?
· Not all patients will need or want such an explanation, but there are times when some understanding is essential. The most obvious example is that of antibiotics where the risks of inappropriate or incomplete use are considerable for individuals and populations who don't understand how they work. Women need to have some grasp of how OCs and other forms of contraception work in their bodies if they are to have optimum control of their fertility and avoid such risks as there are. Taking pills or using devices whose functions are not understood leads to risks of imperfect or non-compliant use.
· How should the drug be taken?
· This not as simple as it sounds:
· ‘Three times a day after meals’ may be unhelpful for people who do not have three meals a day, or for whom ‘meal’ means significant eating like an evening meal, or whose eating patterns are irregular or, for shift-workers, take place during the night (where pictograms are used, a rising sun usually marks the first dose of the day)
· ‘After food’ may not be helpful if the minimum amount of food is not specified (an apple, a snack, a glass of milk, a full meal?) and the reason for ensuring protective stomach contents is not explained
· Patients may not understand the rationale for the spacing of doses, that is, commonly, to ensure a reasonably constant level of the drug or drug-effect in the body. If that is explained, then some of the risks of ignorance and potential non-adherence are reduced. Cost-related non-adherence is a risk, especially for elderly or depressed patients (Briesacher et al. 2007)
· Whether tablets are to be chewed, swallowed whole or dissolved sub-lingually, how to use a nebuliser effectively are among issues that need careful attention; demonstration of devices is usually essential
· Information about route needs to be explicit and clear, especially with maybe unfamiliar forms such as pessaries where a degree of embarrassment may interfere with clear communication (patients have been known to swallow pessaries; mothers have put liquid oral antibiotics into their children’s infected ears (Boodman 2011))
· There can be serious problems with regard to dosage forms: some patients have difficulty with large tablets; tablet-splitting can be troublesome and may result in inaccurate dosing. Common expressions such as ‘teaspoonful’ are liable to variable interpretation and are dangerous. Liquid medicines always need to be accompanied by a model spoon or a calibrated cup or syringe.
· What should you do if you miss a dose?
· Very few patients are perfectly adherent and they need specific guidance as to what they should do when doses are missed. Adherence, especially in chronic diseases and with multiple medications, is a major issue (see below). Pill-boxes, electronic reminders, medication calendars, dated blister-packs, and other methods are important ways of reducing the risk of forgetfulness or confusion.
· Very few doctors or pharmacists have any idea what happens to most patients once they have left the clinic or the shop, particularly with regard to adherence (see prescription fulfillment above). Best practice suggests some way of maintaining contact with patients through methods such as return visits, phone calls or electronic reminders and for providing opportunities for self-reporting (Royal College of General Practitioners2009). (The evidence about patient adherence is shocking, especially in chronic conditions (WHO 2003; Brown and Bussell 2011); the wastage enormous, the risk to health substantial.)
· What are the drug’s side effects?
· Perhaps the single most challenging aspect of risk management and risk communication. This is discussed extensively in the previous chapter and in relation to specific medicines below. Here we note only that information about known risks and their level of certainty will be crucial to a patient’s decisions about therapy and that clear communication of these issues is one of the most difficult tasks for a doctor or pharmacist. Benefit-risk trade-offs for a patient will not always match those preferred by a professional. Early recognition of side effects and knowledge of what action to take is a further critical component of the communications process. Regulatory information about side effects in package inserts is often impenetrable and obscure and can never be a substitute for active professional interpretation and communication.
· What substances interact with the drug?
· It’s important that the discussion should cover all substances including food, alcohol, herbal and traditional remedies, supplements, oral and topical – as well as other prescribed and OTC medicines. For women, it’s important to know that interactions with oral contraceptive (OC) medicines may reduce the efficacy of OCs and OCs may also affect the effectiveness of other medicine (see Chap. 5).
· What behaviour is contraindicated?
· The starkest example here is the risk of fetal abnormality from teratogenic drugs such as isotretinoin and valproic acid. The management of this risk is extremely demanding, and none of even the most persistent warnings or elaborate protocols has succeeded in preventing some pregnancies and the delivery of some damaged babies (see also section “Anti-convulsants in Pregnancy” later in this chapter). The requirement for two reliable methods of contraception used concurrently is, for some patients, difficult to meet practically and psychologically and women do underestimate the risk of unintended pregnancy (see below, p. 600.) Some drugs may make driving or the operation of machinery hazardous; we must know if such issues are relevant for a patient.
· What should you expect the drug to do?
· This sector of information relates to symptom relief, disease eradication and time scales. Patients need to have accurate and realistic expectations so that they are not disappointed or prematurely relieved, and do not abandon the medicine as soon as symptoms disappear. They need to recognise whether or not the drug has been effective and what to do if it has failed in some way. They need to know the degree of uncertainly in relation to effectiveness.
· How should the drug be stored?
· Instructions on package inserts and patient information are not always explicit or comprehensive enough to cover the circumstances of all patients. How can you hope to store a medicine ‘between 15 °C and 30 °C’ and in a ‘dry place’ if you live in the tropics? Can you store medicines in a refrigerator? What is the impact on medicines of temperatures above 30 °C in humid conditions? If there’s no effect, then the storage instructions are irrelevant; if there is an effect, what is that doing for the health of millions whose pills are stored in hot places (including pharmacies without air-conditioning)? Thousands of children are poisoned by ingesting carelessly-stored pharmaceuticals intended for others (CDC 2012); specific warnings about this risk and (where available) the provision of child-proof containers are important risk management measures.
· Should you use a generic version of the drug?
· In countries where regulation is adequate there is usually no problem with substitution. It’s a different matter in countries where regulation and enforcement are lax and counterfeit or sub-standard drugs may be common. Patients need to understand the risks and make wise choices in the balance between cost and quality. Patients also need to know that the safety-profile of generics may not be identical to branded drugs, in relation, for example, to excipients.
· What laboratory tests should be done to monitor the effects of the drug?
· This is essentially a clinical rather than a communications issue, but the necessity for tests and the meaning of results are challenges for communication, especially in the controversial field of screening. Thresholds for concern, in for example blood pressure and lipid levels, are matters of some debate as are the treatment choices based on them. When an option is the starting of life-time drug therapy in currently healthy people, patients need to have a very clear grasp of the true benefits and risks, the degree of uncertainty, and their personal view of them, which may be quite different from the prevailing marketing messages and general assumptions (statins are a good example, see Chap. 18, p. 540). There is evidence that doctors don’t communicate bad test results to about 7 % of patients (Casalino et al. 2009), so patients need to be alert and active in seeking full information. Language is again important: patients may misunderstand a term such as ‘positive,’ for example, believing it means a good result.
In all aspects of risk communication, the language used must be tailored exactly to the literacy and abilities of the patient; technical forms should be avoided (‘pain-killers,’ not ‘analgesics,’ for many patients, ‘food,’ not ‘diet,’ for example). Information needs to be prioritised with regard to the needs of the individual and critical aspects always repeated and checked through asking the patient what they have heard and understood. A fine example of good communication is provided in (Fig. 19.1). (For a comprehensive review of all the communications challenges in healthcare, see Healthcare Communication (Hugman 2013b)).
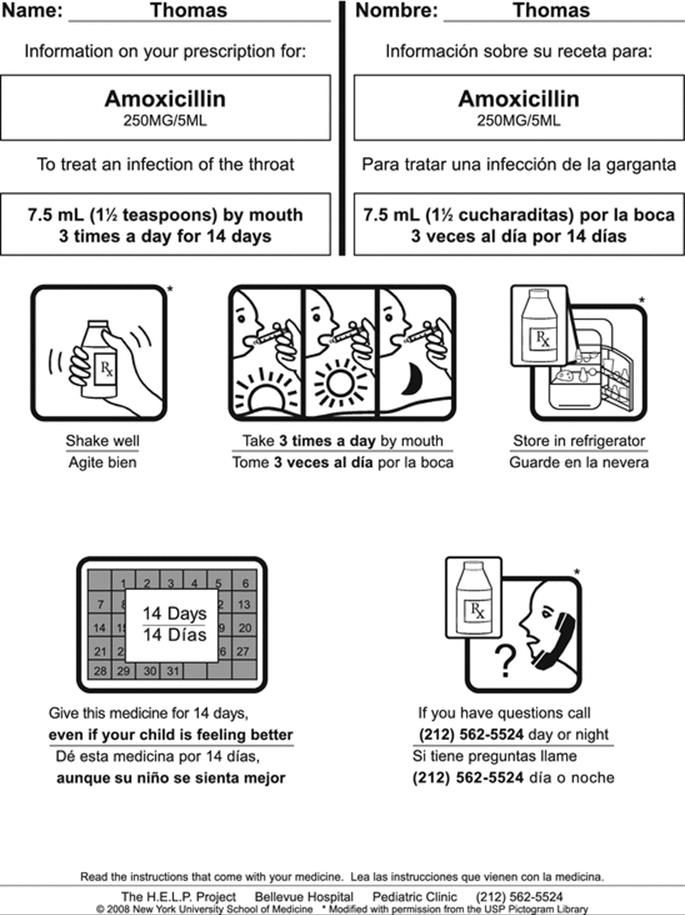
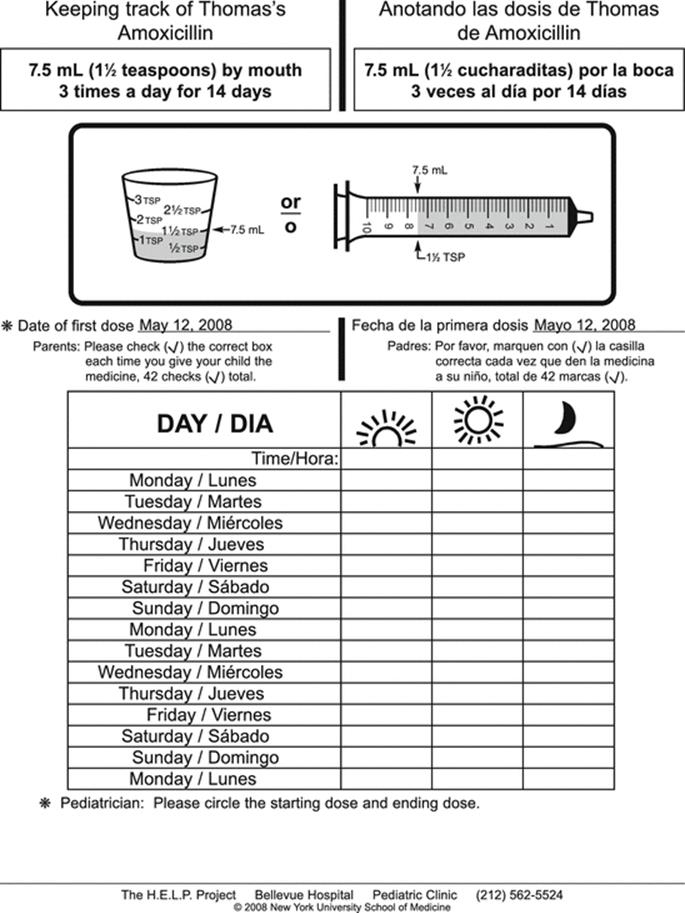
Fig. 19.1
This is an elegant, simple, perfectly tailored risk management tool: it is personalised, presented in English and the primary local minority language; it uses words and pictures; dosage quantity is visualised; there is a daily tick-off calendar and an enquiry line. Following a verbal explanation, the sheets require almost no interpretation through literacy skills, though they would be helpful to patients, literate or not. This is a very good example of communication at its best, reinforcing verbal explanation and translating complex verbal and technical information into easily accessible, self-evident images and activities
Specific Medicines for Women
In the previous chapter, I outlined a range of important variables that profoundly influence a woman’s psychology, life-chances, health and safety. All aspects of the risk communication elements reviewed above are subject to those influences, crucially the extent to which a woman feels that her uniqueness and the specific particulars of her life are recognised, factored into the discussion and valued in each moment of the relationship and its communications.
If you now bring to mind all the risk and risk communication issues that we have covered so far, we can begin to apply them to particular medicines for women.
The writer of the material in this chapter is a communications expert with no professional medical background. While every effort has been made to ensure the currency of clinical evidence referred to, it is not offered here as direct guidance for practice but for illustrative purposes only. There is no attempt to provide reliable, comprehensive, up-to-date risk information about the medicines discussed. The focus here is on the knowledge, skills and processes relating to risk communication for women, illustrated by four high priority practice challenges and the medicines associated with them.
Anti-convulsants in Pregnancy
The term ‘epilepsy’ refers to a group of disorders and is commonly a symptom rather than a distinctive disease. It is one of the least understood of major syndromes (Global Campaign 2012). It varies considerably in incidence across the world, being highest in sub-Saharan Africa and Latin America (BMJ 2013). The risks of epilepsy in pregnancy, and of the medications used to treat it, to both fetus and mother are significant and pose a considerable challenge for benefit-risk communication and patient choice. (Anti-convulsant medicines in pregnancy are reviewed in more detail in Chap. 4.)
Failure to recognise and communicate the risk of anti-convulsant medication may have tragic consequences. On the UK website Epilepsy Action, a mother recounts the effects of lack of risk information when she became pregnant (EpilepsyAction 2014):
No one was overly concerned that I was taking sodium valproate.
The outcome was serious for child and parents:
At 10 days over [the] due date I was induced, and [he] was born 31 hours later. At birth he did not breathe straight away, was floppy, and needed help to start his life…For the next six months we felt that everything was fine. However, the doubts began to start and we knew that [he] was not developing as he should… After reading a news article about anti-epileptic drugs and pregnancy, things started to click into place. I saw my GP and told him of my fears…We were referred to a genetics consultant who diagnosed (when [he] was just 16 months old) fetal anti-convulsant syndrome (FACS)…[he] has three types of epilepsy, medical problems and complex learning difficulties.
So what risk information do women with epilepsy need to have, and how should it be delivered, if they are thinking of becoming pregnant or if, too late for some information, they find themselves pregnant already?
They need to know, for example, that women being treated for epilepsy have a higher risk of pregnancy complications, fetal malformations with certain medicines and maternal death than the general population, though the absolute risks are very small (Tomson and Hiilesmaa 2007). They need to know this in order that they can first decide if they wish to take the risks of pregnancy and treatment at all; second, recognise side effects and signs of complications, the risks of non-adherence and the necessity for frequent monitoring of blood-serum levels. In prospect and as they occur, each of these aspects will have their own set of risk communications and benefit-risk assessments. The possible complications, according to the Mayo Clinic in its web-based information for patients, include (Mayo Clinic 2011):
· Severe morning sickness
· Anemia
· Vaginal bleeding during and after pregnancy
· Premature separation of the placenta from the uterus (placental abruption)
· High blood pressure and excess protein in the urine after 20 weeks of pregnancy (preeclampsia), with a higher risk if they are high-risk HPV exposed
· Premature birth
· A low birth weight baby
· Failure to progress during labor and delivery
· Babies with congenital abnomalies
This does not conform with best communication practice because no figures are given for the risks of these complications.
Borthen et al. investigated some of these risks in a large cohort study and do provide some figures (Borthen et al. 2009):
RESULTS: We compared 2805 pregnancies in women with a current or past history of epilepsy (0.8 %) and 362 302 pregnancies in women without a history of epilepsy. Women with epilepsy had an increased risk of mild pre-eclampsia, [odds ratio 1.3: 95 % confidence interval (1.1-1.5)] and delivery before week 34 [1.2: (1.0-1.5)]. Antiepileptic drugs were used in 33.6 % (n=942) of the pregnant women with epilepsy. Compared to women without epilepsy, women with epilepsy and AED [anti-epileptic drug] use had an increased risk of mild pre-eclampsia [1.8: (1.3-2.4)], gestational hypertension [1.5: (1.0-2.2)], vaginal bleeding late in pregnancy [1.9: (1.1-3.2)], and delivery before 34 weeks of gestation [1.5: (1.1-2.0)]. No significant increase in the risk of these complications was observed in women with epilepsy not using AED. These results remained unchanged after exclusion of multiple pregnancies.
CONCLUSION: Women with epilepsy have a low complication rate, but special attention should be paid to those using AED during pregnancy.
But what do the statistics mean? When we tell a patient that these risks are low, she may ask, “how low?” We need to be able to tell her in absolute terms (see Chap. 18 for more on this challenge).
Here is some of the current advice that a woman searching for information would find through the internet. The extent to which a patient can rely on such information is always open to question (see Box 19.2 on websites) and physicians clearly need to have the latest evidence at their finger-tips.
· All authorities agree that seizures pose a greater risk to mother and baby than well-managed medication
· A year or so before planning to become pregnant, anticonvulsant medication needs to be reviewed and changed if it would pose a high risk to a fetus (this would be the case with sodium valproate due to the risks of NTDs etc (see Chap. 4), for example)
· A regimen of daily folic acid is recommended (though the evidence for the benefits of this is not strong, see below) (American Academy of Neurology 2009)
· Women with epilepsy taking anti-seizure medication may wish to know that their risk of having a child with birth defects is around twice that of non-epileptic mothers (4–8 % compared with 2–3 %; or, to change the framing to its opposite: more than 90 % of women with epilepsy deliver normal, healthy babies). It appears that the risk is increased with particular drugs or when more than one anticonvulsant is used, particularly at high doses (WebMD 2014)
· Topamax (topiramate) taken during the first trimester doubles or trebles the rate of the risk of a child having a cleft palate and cleft lip compared with other anticonvulsants, to about 1.6 % (FDA 2011)
· Women should be prepared to discuss the possibility of the dose of their anticonvulsant being increased because of faster metabolism of anticonvulsants during pregnancy and as their blood volume increases throughout the pregnancy. Use of a drug such as Lamictal (lamotrigine), however, to protect against the possibility of breakthrough seizures, especially in the first trimester, poses a possible risk to the fetus (Drugs.com 2014b).
There are estimated to be ten million people with epilepsy in Africa (WHO 2004), maybe four fifths of whom receive no treatment at all. The disease is also associated with considerable social stigmatisation in many places, making access to care, or even help during seizures, problematic for large numbers of women.
The causes of epilepsy in Africa may differ from other parts of the world:
In all developing countries, and particularly in the African region, a very large number of new onset seizures are a consequence of poor perinatal management, the high impact of infectious diseases, and head trauma. (Ngugi et al. 2013)
So there are these and many other additional risks to any otherwise healthy baby, delivered by a woman with epilepsy or not, besides the possibility of defects induced by anticonvulsant medications. The primary risk management action for women here, across the board, is to find expert pre-pregnancy care and a committed healthcare partnership throughout pregnancy, out of the question though it may currently be for millions of women.
Information for Women with Epilepsy
The Epilepsy Foundation/Epilepsy Therapy Group have a good website that, amongst much else, provides written risk information that is admirable in its clarity and simplicity (Epilepsy Foundation 2011). Here I will quote two or three of the sections answering common questions and experiences as models for good practice.
This first illustrates the dilemma of a patient with a doctor who has not heard about respect for patients or the ethical imperative of joint decision-making and consent.
My doctor told me that because I need to take antiepileptic medication, I should never get pregnant. Now that I am pregnant he recommends an abortion, but I want my baby. Am I wrong to think that my baby will be okay?
It’s instructive that the doctor’s paternalistic and unhelpful advice was ignored, though that fact doesn’t seem to have taught him anything. Here we see, as discussed elsewhere, that healthcare providers are themselves, sometimes, among the risks that patients face.
Elsewhere from the Epilepsy Foundation:
For women who have epilepsy, the risk of having a baby with a birth defect is double the risk for women in the general population. Any woman, whether she has epilepsy or not, has a two to three percent chance of having a baby with a birth defect. For women with epilepsy, the risk is four to eight percent. Even so, mothers with seizures have a better than 90 percent chance of having a normal, healthy baby.
The actual cause of the increased risk of malformations has not been determined, but there are three strong possibilities:
1.
2.
3.
Whatever the cause of the malformations, they do not occur often enough to support avoiding or terminating a pregnancy. However, if an eight percent risk of having a child with a malformation is unacceptable to you, it is important that you make the decision that’s best for you.
Stillbirths or miscarriages are also more common for women who have epilepsy, occurring in 1.7 percent of pregnancies, which is about three times the amount in the general population.
There is also a small increase in mortality rates during the first year of life for children of mothers with epilepsy. That risk is only about 0.6 percent, but is higher if the mother’s seizures are not well controlled.
This is excellent risk communication. What do we notice?
· Relative and absolute risks are characterised in words and figures
· The framing is balanced (reference to both the scale of harm and the scale of not-harm)
· The uncertainty about causation is explained
· A judgement about the level of risk is offered, but quickly qualified by recognition that the patient may have her own views and feelings about it that should determine her decision
· Two other serious risks are mentioned, along with absolute figures (which could also be expressed, for example, as less than 2 women in 100 (1.7 %) or less than 1 in a 100 (0.6 % – but see comments on less than 1 whole person, Chap. 18), or as less than 17 in a 1,000 and less than 6 in a 1,000, respectively. Does one or other of these make the risk seem less or greater? For some, the larger denominator may have that effect.)
Use of Contraceptive Medicines in Women with Epilepsy
We deal with oral contraceptives at greater length below, but here are the risk issues specific to women with epilepsy, again from the Epilepsy Foundation website.
How do I know which method is best for me?
You need to work with your gynecologist and your neurologist to choose the birth control method that is most appropriate for you. It is possible that your antiepileptic drug (AED) may make your hormonal birth control less reliable, resulting in an unwanted pregnancy. You and your physicians may consider different combinations of hormonal birth control and seizure medications to find the one that works best for you.
And details of the very specific issues that relate to particular pills and their risks:
How will my seizure medication affect my hormonal birth control?
There are complex interactions between the hormones (estrogen and progesterone) contained in birth control pills or devices, and some of the medications used to control seizures. Some of these medications increase the breakdown of contraceptive hormones in the body, making them less effective in preventing pregnancy. The seizure medications that have this effect are often called “liver enzyme-inducing” drugs because the liver is the organ that breaks down these hormones. They are carbamazepine (Tegretol, Carbatrol), oxcarbazepine (Trileptal), phenytoin (Dilantin), phenobarbital (Luminal), primidone (Mysoline), and topiramate (Topamax). Valproate (Depakote) and felbamate (Felbatol) do not increase breakdown of hormones, and may even increase hormonal levels, which may require an adjustment in the dose of your birth control. Gabapentin (Neurontin), lamotrigine (Lamictal), levetiracetam (Keppra), and tiagabine (Gabitril) have no effect on this system and do not interfere with the effectiveness of hormonal birth control.
This represents more detailed information than most women might wish, but the risks of hormonal pills or devices and the rationale for a particular suggestion or choice, contained in this text, are topics that will interest many women and help them make a final choice with confidence.
Finally, in this short selection of extracts from the Epilepsy Foundation website, here is an explanation of the risk of pregnancy while on the pill and anti-epileptic drugs:
Are there special concerns about “the pill” for women with epilepsy?
Yes, there are. The popular low-dose combined oral contraceptive pill has a relatively small amount of estrogen (less than 35 micrograms). That’s not enough to protect women with epilepsy who take enzyme-inducing AEDs from becoming pregnant. You may need contraceptive pills with higher doses of estrogen, and even then, there is a risk of unexpected pregnancy. It is a good idea to use barrier methods (a diaphragm, spermicidal cream or a condom) in addition to the contraceptive pill, if you are taking one of the seizure medications that speed up the breakdown of the hormones in birth control pills.
The risk of unexpected/unintended pregnancy is not given a figure here, so that cannot be easily assessed by a woman faced with the possibility of using an additional barrier method; for some, any risk at all may be unacceptable; for others, trading a small risk for the simplicity of pill-only contraception may be preferable. The risks of unintended pregnancy are actually much higher than one might expect: around 50 % in the US, with higher than average incidence, ‘…among poor and low-income women, women aged 18–24, cohabiting women and minority women.’ (Guttmacher Institute 2013). Risk communication in relation to this must negotiate the tricky diplomatic waters evident from the fact that some women may be less in control of their fertility than they naturally assume.
All websites I have reviewed state or assume the importance for women to be working in partnership with expert physicians or family planning advisers. However, the Epilepsy Foundation points out:
Many physicians are not aware of this statistic [that more than 90 percent of pregnancies in women with epilepsy have a good outcome], nor are they up to date on the best medication choices for women with epilepsy considering pregnancy or already pregnant. (Epilepsy Foundation 2014)
Being reminded that they may not be entirely up-to-date in their knowledge is a challenge to the self-image of professionals, especially if the reminder comes from a patient. Active, well informed patients do reduce the risk of harm from less than optimal treatment, but there is never any substitute for professionals to know, or have quick access to, the latest data and evidence. A degree of humility in the face of complexity – and of patients – is a useful quality for doctors.
The American Academy of Neurology publishes a useful fact sheet on epilepsy, a summary of a much longer report. It has a similar question/answer section as the Epilepsy Foundation (above), but also a very good page on the evidence for the treatment of women with epilepsy (WWE). A selection of a couple of issues to illustrate the powerful value of such summaries for the planning of risk communication appears in Box 19.1 (American Academy of Neurology 2009). Note also the classification of the strength of evidence, an issue I have not discussed elsewhere but is vital to the enterprise of risk communication.
Box 19.1
Does preconceptional folic acid supplementation reduce the risk of birth defects in neonates of WWE taking AEDs?
Weak evidence Preconceptional folic acid supplementation in WWE may be considered to reduce the risk of major congenital malformations (MCMs) (Level C).
Clinical context Folic acid supplementation is generally recommended to reduce the risk of MCMs during pregnancy, and although the data are insufficient to show that it is effective in WWE, there is no evidence of harm and no reason to suspect that it would not be effective in this group. Therefore, all women of childbearing potential, with or without epilepsy, should be encouraged to take at least 0.4 mg of folic acid daily prior to conception and during pregnancy. There was insufficient published information to address the dosing of folic acid.
What is the risk of hemorrhagic disease in neonates born to WWE taking AEDs?
Insufficient evidence Counseling of WWE who are pregnant or are contemplating pregnancy should reflect that there is insufficient evidence to support or refute an increased risk of hemorrhagic complications in the newborns of WWE taking AEDs (Level U).
They classify the strength of evidence according to this hierarchy:
A =
Established as effective, ineffective or harmful (or established as useful/predictive or not useful/predictive) for the given condition in the specified population. (Level A rating requires at least two consistent Class I studies.)
B =
Probably effective, ineffective or harmful (or probably useful/predictive or not useful/predictive) for the given condition in the specified population. (Level B rating requires at least one Class I study or two consistent Class II studies.)
C =
Possibly effective, ineffective or harmful (or possibly useful/predictive or not useful/predictive) for the given condition in the specified population. (Level C rating requires at least one Class II study or two consistent Class III studies.)
U =
Data inadequate or conflicting; given current knowledge, treatment (test, predictor) is unproven. (American Academy of Neurology 2009)
The Dilemma for Women with Epilepsy
Epilepsy presents some of the most agonising of risk decisions, with the welfare of both mother and baby at stake. If we add the further anxieties and risks around pregnancy itself, we have a situation where a woman may feel distressingly confused or oppressed by the choices she faces. Only genuinely empathetic, patient, measured counseling can hope to provide a degree of clarity and open the door to voluntary, informed choice. If, as we saw in the anecdote above, the doctor’s behaviour is patronising or prejudiced, or simply out of touch with a woman’s feelings, advice will simply be ignored and a patient will be left angry and disillusioned – and she and her baby will be at greater risk.
While internet forums and patient communities are not all to be trusted (some are sponsored by or infiltrated by commercial, ideological and other interests), there are rich and reliable resources available to inform and support women with many different conditions. Doctors need the humility to refer patients to reliable additional, alternative, resources that may provide a much broader spectrum of options and experiences than any professional can draw on. In the previous chapter we saw elsewhere how much some women favour and rely on the wisdom of their mothers and their female peers (in Tibet, Africa and elsewhere); interaction with such a virtual community of peers may lead to much more confident and positive risk perception and to choices that are more deeply acceptable, and to regrets that are fewer even when there’s an unfavourable outcome.
On the other hand, informal social or anecdotal information, women’s magazines, out-of-date websites or websites with an axe to grind, may be serious threats to authoritative understanding; patients’ interpretative and authentication abilities vary enormously (Peterson et al. 2003).
Oral Contraception
The advent of the contraceptive pill in the 1960s was widely hailed, accurately, as ushering in a revolution for women: for the first time in history, they had simple, direct, permanent, largely reliable control over their fertility, without depending on much planning ahead, on more troublesome devices, on the whims and behaviour of men, or on other, less effective methods.
Nevertheless, all methods of contraception bring some risks (detailed in Chap. 5), not least of conception, resulting from non-adherence or imperfect or inconsistent use. A woman taking OCs runs the very small chance of becoming pregnant (less than 1 in 100 in study populations, though still slightly more than some other methods) (Trussell 2011). Oral contraception (OC) is the third most common method used by women, aged 15–49, who are married or in unions, with a worldwide prevalence of 9 %, after female sterilisation (19 %) and IUDs (14 %) (United Nations 2011). The UN reports unmet needs for contraception in more than 140 million women worldwide, the great majority of whom live in developing regions.
In spite of declining rates everywhere, Singh et al. estimated the number of unintended pregnancies worldwide and found that about 41 % of 208 million pregnancies in 2008 fell into that category (Singh et al. 2010).
The Guttmacher Institute’s research (Guttmacher 2013) shows that in 2008, in the US, about half of all pregnancies (51 %; 3.4 m/6.6 m) were unintended (that is mistimed or unwanted), an increase of about 3 % on 2001, and, as noted above: “unintended pregnancy rates are highest among poor and low-income women, women aged 18–24, cohabiting women and minority women”.
This finding reinforces the critical issues argued in Chap. 18: the risks a woman faces and her needs for risk communication are profoundly influenced by the characteristics of her life, her socio-economic status, her age and a multitude of other factors. ‘Medicines for women’ becomes a viable and safe concept in practice only when it is reformulated as ‘a medicine for this unique woman.’
Unintended pregnancy is the principal reason for abortion, and though abortion rates declined overall in the US between 2001 and 2008, for poor women it increased 17.5 % from 44.4 per 1,000 births to 52 (Jones and Jerman 2014):
How can this apparent failure of contraception (and, therefore, of public health communication) be explained in the wealthiest nation on earth? In the Guttmacher study, nearly 11 % of women were using no contraception at all. A belief in their low risk of pregnancy, lack of forethought, distaste for contraceptive methods and male reservations were amongst their explanations. Dude gives us a further insight with her finding that 31 % of young women in the US, aged 15–24, had used withdrawal (coitus interruptus) at least once; that 7.5 % of them were likely to depend on emergency contraception and that 21 % of them had become pregnant (Dude et al. 2013). There is clearly a large space that public health education and risk communication need to fill.
The situation is very different in the developing world, where the overall prevalence of contraception is lowest and the unmet needs are greatest. In Unintended Pregnancy and Induced Abortion in Uganda The Guttmacher Institute reports (Guttmacher Institute 2006):
An estimated 297,000 induced abortions are performed each year in Uganda, which translates to an annual abortion rate of 54 per 1,000 women aged 15–49… More than half of all abortions are believed to be carried out by medically trained providers (doctors, nurses, midwives). The remaining procedures are performed by nonprofessionals, including pharmacists, traditional providers and women themselves.
According to the UN, only about a third of Ugandan women of reproductive age use contraception of any sort and over a third of the remainder have an unmet need for contraception. In 2008–2010 there were 1.47 m births in Uganda (crude birth rate 42.1/1,000). Guttmacher reports:
This means that 42 % of pregnancies in Uganda (the 16 % that resulted in abortions plus the 26 % that resulted in unintended births)—a minimum of 775,000 each year—can be classified as unintended. This analysis points to the fact that not all unintended pregnancies end in abortion: About 38 % [of 775,000] do, and the remainder lead to unintended births.
So, where does all this lead us in the context of risk communication? Some major issues that must influence medical practice and counseling:
· To a greater or lesser extent, depending on location, many women are not using contraception at all and many of those have unmet needs for contraception
· A major risk factor for low contraceptive use, unwanted pregnancies and abortions is poverty
· Among those not using contraception, whether or not with perceived unmet needs, there are a number of influential factors (many of which will vary according to the socio-political and religious environment in which women live):
· Voluntary choice or forced decision, resulting from
· Perception of low risk
· Accidental or unexpected insemination
· Male reservation (or refusal in many cases) about contraception in general or male contraception in particular
· Pressure (usually male) in some societies to have a large family
· Lack of access to contraception
· Lack of resources, facilities and information
· Poverty
· Some women (mainly in developing countries) are at physical risk from frequent births and from abortions, especially conducted by unlicensed practitioners
· Many women are almost certainly at risk for psychological damage or trauma as a result of the stresses of child-rearing because of unintended or unwanted births. They are also at risk of poverty and being unable to support their children financially
Good decision-making in this area for women requires an intimate knowledge of self in the patient (preferences, habits, intentions) and very good counseling and risk communication that takes into account many variables, including the risk of adverse effects, which we move onto now.
The Pill, Risks, Scares and the Media
Combined oral contraceptives (COCs) are associated with a risk of venous thromboembolism (VTE); this risk is discussed in detail in Chap. 6. Here I will focus on issues which arose from the 1990s onwards when government agencies in Europe badly handled the risk communication for health professionals and women, with a number of negative outcomes.
Making Sense of Health Statistics and Deciding What to Do
In October 1995, the UK Committee on the Safety of Medicines (CSM) issued a nationwide warning to 190,000 professional recipients about the increased risks of third generation combined hormonal contraceptives compared with older types. The advice was that:
…these pills should only be used by women who were intolerant of other combined oral contraceptives and were prepared to accept an increased risk of thromboembolism. (Barnett and Breakwell 2003)
Their public announcement (which was made before the key studies had been published in peer reviewed journals) stated that the risk of venous thrombosis was ‘doubled’ for women taking these pills, containing the synthetic hormones gestodene and desogestrel. The absolute figures (an increase from 1 to 2 in 7,000 or 15 to 30 in 100,000) were not highlighted. A substantial number of health professionals did not receive their notifications until after the story had broken in the media. The author of one of the unpublished papers that the CSM had reviewed flew from Canada to the UK to assert that his findings had been misrepresented. It was a communications mess that became a crisis.
Large numbers of women besieged their doctors or called helplines; many stopped taking their pills immediately and numbers of prescriptions dropped dramatically for a long time afterwards (de Jong-van den Berg L et al. 2003). There was evidence of an increase of 13,000 abortions in the following year, especially among young women (de Jong-van den Berg et al. 2003). It was all pretty chaotic and alarmed a lot of women.
The following year, the European medicines regulation body, The Committee for Proprietary Medicinal Products (CPMP), cast doubt on the CSM’s advice for women to change to older types of OCs:
[The CPMP] acknowledged the data indicates that the blood-clot risk of desogestrel or gestodene-containing Pills is higher than other brands but said the impact of “biases and confounders [in the studies] on the differences could not be fully evaluated…[and they had] failed to establish any scientific reason to change advice to women taking these Pills in the EU, or recommend a change in the drug-licensing requirements.” (Health Editor 1996)
In 1999, the MHRA changed its advice:
…provided women are fully informed of these very small risks and do not have medical contraindications, it should be a matter of clinical judgement and personal choice which type of oral contraceptive should be prescribed. (MHRA 1999)
When questioned about the quality of the 1995 advice, Dr Jeremy Metters, Deputy Chief Medical Officer in the UK, is reported as saying:
We would have been criticised if we had sat on the data. Contraception is a very personal thing and women have a right to all the information that is available. (Lattimer)
Here, we see a national institution taking a precautionary stance, and, in their original advice, a probably over-cautious view of the risks, expressed through unsatisfactory risk communication practices that did not anticipate its likely effects at all.
This so-called ‘U-turn’ irritated a lot of people and led them to reflect on the damage they felt had been caused:
The advice given by the CSM in 1995 that these pills should not be prescribed was unnecessary and alarmist. The pill scare that followed was a disaster that should never have happened. It caused a massive increase in the rates of unintended pregnancies and undermined general confidence in the safety of the pill. It reversed a downward trend in the number and rate of abortion. (Lattimer)
Since then, indeed since 1995, the science and risk of third generation OCs has hardly changed, with most authorities in agreement that they are equally effective as second generation pills, but carry a higher risk of VTE (probably about twofold) and that they should not be prescribed as first-line medication. Nevertheless, the potential for scares in the media does not seem to have reduced at all. After the European Medicines Agency (EMA) completed a review of target combined hormonal contraceptives (CHCs) in 2013, the agency concluded:
…that the benefits of CHCs in preventing unwanted pregnancies continue to outweigh their risks, and that the well-known risk of venous thromboembolism (VTE) with all CHCs is small. (EMA 2013)
These very moderate conclusions, including somewhat reduced estimates of the risks, more or less confirmed what had been known for over a decade, yet the UK tabloid, The Mail on Sunday, in a headline occupying one third of its front page, and the full width, declared:
“DEADLY RISK OF PILL USED BY 1m WOMEN”
and reported: “..doctors in the UK have been ordered to alert women to the deadly dangers” (Daily Mail Online 2014).
Even the broadsheet Times of London was alarmist in its headlining (Dixon 2014):
GPs warn 1m women of deadly blood clot risk
There is, indeed, a potentially ‘deadly blood clot risk’ that may kill healthy, young women. We know the risk is actually very small and that it is not one million women who are all equally and immediately at risk as the headlines imply. The newspaper headlines are not untrue, but in their unqualified starkness, they are misleading and alarmist.
Fortunately, the risk information provided by the EMA in 2013 is a fine example of how the job should be done by authorities and doctors, hardly justifying the dramatic headlines, characterising the small risks of venous thrombosis clearly and simply, and in absolute figures as detailed in Table 19.1 below:
Table 19.1
Absolute risks of VTE in women taking the combined pill
|
Women not using a combined hormonal pill/patch/ring and are not pregnant |
About 2 out of 10,000 women |
|
Women using a CHC containing levonorgestrel, norethisterone or norgestimate |
About 5–7 out of 10,000 women |
|
Women using a CHC containing etonogestrel or norelgestromin |
About 6–12 out of 10,000 women |
|
Women using a CHC containing drospirenone, gestodene or desogestrel |
About 9–12 out of 10,000 women |
|
Women using a CHC containing chlormadinone, dienogest or nomegestrol |
Not yet known |
Source: EMA (2013)
And the textual information from the EMA is also simple and clear and provides a good model for face-to-face counseling:
Advice for women:
· If you have been taking CHCs [combined hormonal contraceptives] without any problem, there is no reason for you to stop taking them on the basis of this review. But it is important that you are aware of the risk of blood clots associated with these medicines, even though it is very low.
· The risk of blood clots in the veins varies between CHCs, depending on the type of progestogen (a hormone) they contain, and ranges from 5 to 12 cases of blood clots per 10,000 women who use them for a year (see table [above]). This compares with 2 cases of blood clots in the veins each year per 10,000 women who are not using CHCs.
· You should also be aware of the factors that increase your risk of a clot and be aware of how these may change over time. Risk factors include, among others, being very overweight, increasing age, having a member of your family who has had a blood clot at a relatively young age (e.g. below 50), having migraine or being immobilised for a long time (e.g. because of an illness or injury). Your risk of a blood clot is higher in the first year of using a CHC.
· You should discuss with your doctor or nurse what is the most appropriate type of contraception for you.
· When taking CHCs, you should be alert for the signs and symptoms of blood clots, which may include severe pain or swelling in the legs, sudden unexplained breathlessness, rapid breathing or cough, chest pain, and weakness or numbness of the face, arm or leg. If you develop any of these signs and symptoms you should seek medical advice immediately.
· If you have any questions or concerns, speak with your doctor, pharmacist or nurse.
In this chapter, we cannot review all the risks of contraception (most are covered in other chapters in Part II of this book). Of interest is the information about relative risks of different methods. One example from a Danish study of incidents of venous thrombosis reported in the BMJ:
Compared with non-users of the same age, women who used a skin patch had an eight times increased risk (9.7 events per 10,000 exposure years), while women who used a vaginal ring had a 6.5 times increased risk (7.8 events per 10,000 exposure years).
Use of a progestogen-only subcutaneous implant carried a slightly increased risk, while use of a progestogen-only intrauterine device did not confer any risk, and may even have a protective effect, say the authors. Unlike combined pills, no reduction in risk was seen with long-term use of a patch or a vaginal ring.
Based on these findings, the authors calculated that 2,000 women using a vaginal ring and 1,250 women using a skin patch should shift to a combined pill containing levonorgestrel to prevent one event of venous thrombosis in one year. (Conley 2012; Lidegaard et al. 2012)
How, then, can women make judgements about the relative risks of contraceptive methods and the risk of the method they might prefer? They should not, it seems, rely on the product information accompanying their medications; according to the Royal College of Obstetricians and Gynaecologists, in their politely restrained observation:
Summaries of product characteristics and patient information leaflets produced by the manufacturers of contraceptives are often at odds with evidence and with national guidance and can cause confusion. (RCOG 2013)
They might, on the other hand, turn to a website like Womenshealth.gov, where they would find many common questions answered, and a table (Women’shealth.gov 2012):
Contraceptive methods and their risks of pregnancy per 100 users in 1 year
|
Method |
Failure rate (the number of pregnancies expected per 100 women) |
|
Sterilization surgery for women |
Less than 1 pregnancy |
|
Sterilization implant for women (Essure) |
Less than 1 pregnancy |
|
Sterilization surgery for men |
Less than 1 pregnancy |
|
Implantable rod (Implanon) |
Less than 1 pregnancy Might not work as well for women who are overweight or obese. |
|
Intrauterine device (ParaGard, Mirena) |
Less than 1 pregnancy |
|
Shot/injection (Depo-Provera) |
Less than 1 pregnancy |
|
Oral contraceptives (combination pill, or “the pill”) |
5 pregnancies Being overweight may increase the chance of getting pregnant while using the pill. |
|
Oral contraceptives (continuous/extended use, or “no-period pill”) |
5 pregnancies Being overweight may increase the chance of getting pregnant while using the pill. |
|
Oral contraceptives (progestin-only pill, or “mini-pill”) |
5 pregnancies Being overweight may increase the chance of getting pregnant while using the pill. |
|
Skin patch (Ortho Evra) |
5 pregnancies May not work as well in women weighing more than 198 pounds. |
|
Vaginal ring (NuvaRing) |
5 pregnancies |
|
Male condom |
11–16 pregnancies |
|
Diaphragm with spermicide |
15 pregnancies |
|
Sponge with spermicide (Today Sponge) |
16–32 pregnancies |
|
Cervical cap with spermicide |
17–23 pregnancies |
|
Female condom |
20 pregnancies |
|
Natural family planning (rhythm method) |
25 pregnancies |
|
Spermicide alone |
30 pregnancies It works best if used along with a barrier method, such as a condom. |
|
Emergency contraception (“morning-after pill,” “Plan B One-Step,” “Next Choice”) |
1 pregnancy It must be used within 72 h of having unprotected sex. Should not be used as regular birth control; only in emergencies. |
CDC also has an excellent page on these issues. Some of the CDC risk statistics vary from those in this table, but the primary message – that there are risks with every method – remains the same (CDC 2013)
This is the kind of simple data that provides information that many women will not know and permits informed choice, albeit in discussion with a physician. Readers need to know that I deleted the side effects column from this table, which appears on the website alongside the two columns above. This is because there were doubts about the evidence-base for some of the material (weight-gain from OCs for example) and the authority of the list was, therefore brought into question. It required a physician to point out to me that there might be weak or inaccurate information, and it raises the unnerving question, as to how patients can judge the reliability of information they discover on their own. The answer is – they probably can’t and must consult with their health professionals. Women do need accurate and quantified risk data for their contraceptive choices, and only a review of a variety of resources and discussion with their doctors will allow them to make the best decisions (see Box 19.2 on website reliability).
Box 19.2 Reflection on the Reliability of Websites
Our research for this book has confronted us with a huge range of websites, covering the entire spectrum from wacky and dangerous to professional and authoritative. Even at the positive end of the spectrum, however, it is very difficult to judge how reliable and up-to-date the information is, even when the ‘updated’ event is recent (some ‘updating’ is no more than token). The National Institutes of Health and WHO have some useful guidance for assessing websites (NIH 2011; WHO 1999). There are schemes, such as the HONCode (HONCode), run by an NGO, which offer certification of websites on a number of demanding criteria, but it is unclear how rigorous the certification process is and whether or not the approval and logo might remain on a website past its currency. The gold standard of evidence has to be in professional publications, largely inaccessible to the public, such as BMJ Clinical Evidence and Cochrane Reviews. How quickly best evidence from these sources appears on publicly-accessible sites is far from certain. Patients will come with information and opinions based on unreliable sources and doctors need to be alert to the risks and have the current knowledge to manage them. All official guidance suggests that information from the internet should be mediated through consultation with a professional. Gigerenzer in his remarkable book, Risk Savvy, proposes that free access to the Cochrane Library, to journal articles and to medical records are amongst the reforms necessary to support literate patients in their pursuit of the best possible information and decisions (Gigerenzer 2014).
Summary of Risk Communication Issues with Contraceptive Medicines
· Even nationally responsible agencies may come to premature conclusions and provide guidance that will not survive professional scrutiny or stand the test of even a quite short period of time
· Their methods of communicating risk, particularly in relation to ensuring that health professionals have information before stories break in the media, are not always timely or reliable
· The use of relative risk statistics without reference to the absolute figures has the potential to mislead, confuse and alarm
· The media have a tendency to amplify risk and to generate public reactions that are distressing and disproportionate
· Poor risk communication in the public domain can lead to very serious public and individual health consequences
· Women (and men) must be helped to understand that no contraceptive method is without risk; that although population risks may be known, each individual’s risks are unique to them; that, in all things, there is a measure of uncertainty
· Product information, provided by manufacturers, may not be a reliable guide to effectiveness or risk (nor may information on the internet)
· There are reliable, up-to-date data about risks and benefits of contraceptive medicines available: women themselves, and their physicians, need to know where to find them and how to judge what is reliable.
HPV Vaccination
This is now established as an effective and safe vaccine which is significantly reducing morbidity and mortality from cervical cancer and other diseases (see Chap. 9). It’s a good news story for women (Australian 2014), but it has not been universally accepted and, in some places, has been mired in controversy that has led to low-uptake. I must remark on the use of the word ‘safe’ in this context. To the public, ‘safe’ means without risk. We know that no medicine is 100 % safe for all people in all circumstances, so any claim that a vaccine or drug is ‘safe’ must be made with great circumspection. The professional definition of ‘safe’ – i.e. may cause minor (‘non-serious’) adverse effects and rare serious effects; has benefits that significantly outweigh harms – does not match public expectation of the concept. Any parent whose child has even a mildly unpleasant reaction to a vaccine that they have been assured is ‘safe’ may be disappointed, angry or lose faith in the source of the information; temporal association with a serious adverse event or a death will have even more radical impact. Over-blown claims or unqualified assertions, especially about safety and the degree of certainty about evidence, even with the best intentions, are, without exception, intolerable and unethical practice in risk communication.
In 2008 the Government of Romania – a country with the highest incidence of cervical cancer in the European Union – initiated an HPV vaccination programme for 11–12 year-old girls. Very rapidly there was a national storm of controversy with apparently overwhelming opposition to the programme among parents, doctors and the media. The project was abandoned. What underlies this kind of public hostility to vaccination in general and the HPV vaccine in particular?
Craciun and Banan interviewed mothers in Romania after the crisis and concluded:
…[the] main reasons for not vaccinating their daughters perceiving the vaccine as risky, the belief that the vaccine represents an experiment that uses their daughters as guinea pigs, the belief that the vaccine embodies a conspiracy theory that aims to reduce the world’s population and general mistrust in the ineffective health system. Mothers stated they would need clear, factual information about the HPV vaccine and its link to cervical cancer in order to motivate them to accept it for their daughters. (Craciun and Baban 2012)
Field-testing of Gardasil®, and subsequently all HPV vaccination, was suspended by the Indian Government in 2010 after alleged protocol violations and concerns about unexplained deaths and serious adverse events. The depth of anger and suspicion about the programme is evident in one commentator’s remarks at the time:
Unfortunately, the rest of the world does not seem to care as much for their citizens as does India. Similar concerns about HPV vaccine efficacy, benefits versus risks, questionable marketing campaigns, political ‘deals’, and the risk of serious adverse events, including death have been raised by at least 12 other countries around the world, with virtually no response. (Seumasach 2010)
A more recent study in Sweden investigated parental attitudes to vaccination and low take-up rates:
Some parents say no to allowing their daughters to be vaccinated against … HPV. The reasons include insufficient information, the child’s age and distrust of authorities… (Gran Dahl 2014)
The US National Coalition of Organised Women is implacably opposed to HPV vaccination. They have produced a powerful, emotive video in which pediatricians, parents and allegedly injured girls plead, often passionately and tearfully for the removal of HPV vaccines from the market (National Coalition of Organized Women 2012).
On 8 June 2005, the US FDA approved Gardasil® for the prevention of cervical cancer and other HPV-related diseases. Very quickly, and well before the controversy about adverse side effects erupted, conservative groups and politicians raised the objection that the vaccine would encourage promiscuity, on the grounds that young women would have irresponsible, unprotected sex because they were safe from (some strains) of HPV. There is now some evidence that this is not the case (Bednarczyk et al. 2012; Choices 2012), but the prejudice and the myth linger on, contributing, alongside other factors, to relatively low take-up in the US and other countries.
Managing Concerns About Vaccination Programmes
How can public health officials and physicians respond effectively to widespread and emotive issues that fly in the face of all the scientific evidence? (HPV is not the first, by the way: there was the pertussis row in the US some years ago which continues to damage public health (California Department of Public Health 2014); the polio disasters in northern Nigeria and Pakistan; the MMR fiasco, amongst many others; vaccination programmes are particularly vulnerable to this kind of disruption. These, and some others, are discussed and analysed in Expecting the Worst, Chap. 9 (Hugman 2013a))
The first line of useful response is probably not simply coming up with the evidence. Although the Romanian mothers (quoted above) said they wanted clear information, that alone would almost certainly not deal with their perceptions and emotions (risk as feelings and as politics, Chap. 18, p. 534). Parents will be deaf to scientific evidence while they are under the influence of compelling beliefs about unexpected death or injuries, however flimsily based; about political, neo-colonial, religious or commercial conspiracies; or about associated moral issues. Distrust of public authorities and Western influence is a common and damaging perception in many parts of the world and it requires radical changes in official behaviour and intensive, enlightened communication interventions, aimed at education and reconciliation, far beyond the ambit of specific campaigns (and well beyond the scope of this chapter).
(One fact in the genesis of such distrust cannot be passed over: some public authorities and pharmaceutical companies have been guilty of selective communication, misrepresentation, culpable error, dishonesty, arrogant dismissal of public concerns, lack of transparency and blatant fraud, especially with regard to the risks of medications. As long as such things happen, and linger in the public memory, a response of scepticism or distrust is not in the least unreasonable. In such a climate, a doctor’s response to a patient’s question, ‘Can I trust this information?’ has to be: ‘I understand your worries, but I’ve looked into this very carefully, and to the best of my knowledge this is my conclusion....’ But no doctor should pretend that there’s only one view of any risk, nor imply a degree of certainty that the data do not support.)
At the individual level, professional empathy must engage with the depth and passion of these feelings as the essential starting point. If a conversation with a sceptical or hostile parent does not start with ‘Tell me about your feelings and beliefs,’ followed by a period of very intense, respectful listening, there’s little hope of progress. Parents are, after all, defending what they believe are the health and best interests of their children; they will fight against all comers if they believe they are being harassed or manipulated into a decision they do not agree with. Furthermore, their trust in medicine and doctors across the board will be badly damaged.
There will be some particular risk communication issues and problems that may emerge once the encounter has moved on to a phase of discussion and debate:
· The confusion between temporal association and causality: ‘She had the vaccine and never walked again’ (See section “Causality”, Chap. 18, p. 544)
· The power of anecdotes in the media and in social interaction, those vivid, compelling stories without science: ‘We buried my daughter today’
· The influence of ‘experts’ in the public eye, in the media and on the internet who promote compelling, ostensibly science-based arguments challenging the status quo
· The influence of politicians who have broader agendas (and little knowledge of science) in which scientific issues get swept up into political and moral crusades
· The influence of religious leaders, the impact of some of whose principles may have the effect of damaging health and the public interest
· Reluctance to put a healthy child at even a very small risk of adverse effects
· The issue of small immediate risk as trade-off for large, future risk reduction
· The interaction of individual choice and community health, herd-immunity, in particular
Here, you can see the complex mix of issues and problems that may be influencing a parent, only some of which are amenable to rational argument and scientific evidence. Nevertheless, the facts and the evidence, such as they are, do need to be presented at some point and, as far as possible, in ways that are as compelling as the arguments used by the opposition.
Finding Facts About HPV
Where do we go to find the facts and good information about benefit-risk? The US CDC website is a good place to start.
Approximately 79 million Americans are infected with human papillomavirus (HPV), and approximately 14 million people will become newly infected each year. Some HPV types can cause cervical, vaginal, and vulvar cancer among women, penile cancer among men, and anal and some oropharyngeal cancers among both men and women. Other HPV types can cause genital warts among both sexes. Each year in the United States an estimated 26,000 new cancers attributable to HPV occur, 18,000 among females (of which 11,500 are cervical cancer) and 8,000 among males (of which 5,900 are oropharyngeal cancers). (CDC 2014)
Gardasil® and Cervarix® are the vaccines that protect against the types of HPV infection that cause most cervical cancers and their safety record appears to be good, according to the US Vaccine Adverse Event Reporting System (VAERS):
From June 2006-March 2013, approximately 57 million doses of HPV vaccines were distributed and VAERS received approximately 22,000 adverse event reports occurring in girls and women who received HPV vaccines; 92 % were classified as “non-serious.” Reports received by VAERS peaked in 2008 and decreased each year after that; the proportion of female HPV reports classified as “serious” (reports are classified as “serious” if they contain information that the event resulted in hospitalization, prolongation of an existing hospitalization, permanent disability, life-threatening illness, or death) peaked in 2009 at 12.8 % and decreased after that to 7.4 % in 2013. (CDC 2014)
These figures provide the starting point for further exploration and discussion of the data and the risks. Parents will want to know exactly what is meant by ‘non-serious,’ and ‘serious’ and just how frequent such events are; they may want to hear about the alleged deaths from vaccination about which CDC and EMEA are unequivocal:
· There is no diagnosis at death that would suggest that the Gardasil® vaccine caused the death (CDC)
· No causal relationship has been established between the deaths of the young women and the administration of Gardasil (EMEA 2009).
Can these official assertions stand up beside the claims of an active anti-vaccination campaigning group like Judicial Watch (Judicial Watch 2007):
The FDA adverse event reports on the HPV vaccine read like a catalog of horrors,” stated Judicial Watch President Tom Fitton. “Any state or local government now beset by Merck’s lobbying campaigns to mandate this HPV vaccine for young girls ought to take a look at these adverse health reports. It looks as if an unproven vaccine with dangerous side effects is being pushed as a miracle drug.
These battles are country-dependent. The picture is very different in Australia where the national HPV vaccination programme began in 2007 and has achieved a first-dose coverage of over 80 % (compared with 30 % in the US) with very little controversy or evidence of exceptional serious adverse effects (six million doses; anaphylaxis at a rate of 2.6 per million, for example, comparable with other vaccines in international studies, and ‘no deaths.’) (TGA). A study of the Australian programme in BMJ (2013) reported:
· In women, with 83 % first dose vaccine coverage, a 93 % decline in diagnosis of genital warts was seen by the fifth year of the national quadrivalent HPV vaccination programme in Australia
· Despite men not being vaccinated, an 82 % decline in genital warts occurred in heterosexual men, attributable to herd immunity
· No women who reported that they had been vaccinated were diagnosed as having genital warts in the final year of the study (Ali et al. 2013)
This study, published in a high ranking peer reviewed journal indicates positive outcomes from the HPV programme, even though there is active anti-vaccination campaigning in the country.
Navigating our way through all this is bewildering: ‘facts’ presented by opposing parties will appear to contradict each other. To balance the heart-wrenching stories of those who believe they have been injured we can find no comparably weighty advocacy in favour of the vaccine in the scientific and regulatory literature, nor in most public health campaigns; the facts are promoted, but they do not have the drama and colour of stories about alleged injury to children. It’s no wonder parents are confused and hesitant.
What Can We Tell Parents?
We cannot anticipate what every young girl’s parents will want to know, but we can speculate that these are some of the primary questions and issues they may seek information about and want to resolve:
· What are the risks and consequences of (a) HPV infection, (b) genital warts, and (c) cervical cancer and are those risks individually and collectively larger or smaller than the risks of HPV vaccination?
· What causes other than HPV are linked to cervical cancer? How far are those risks reduced by vaccination? How likely is my child to get cervical cancer even if she has the vaccination?
· If my child is vaccinated will she still need to be tested for cervical cancer in the future?
· If my child has an adverse reaction, will she recover from it?
· Are there any serious reactions she might not recover from?
· How strong is evidence for the safety of the vaccine?
· How can you explain the stories in the media about children being made sick or dying after vaccination?
· Has anyone died from the vaccine?
· How can I explain the vaccine to a young girl?
· Won’t the vaccine encourage young women to have more unsafe sex?
· Can’t she wait until she’s a bit older and can understand the vaccine?
Many of these questions you’ll be able to answer now you’ve read this chapter. Few physicians in the world will have time to work through such extensive material with their patients and this highlights the profound need for supplementary reliable risk communication resources, including leaflets, videos, websites, and so on. Chapter 9 of this book (HPV vaccines) includes a useful and concise ‘frequently asked questions’ primarily aimed at physicians (see p. 283).
As with all vaccination programmes, as noted above, it is critical that the antecedent conditions in the community are accurately understood (especially any kind of well articulated opposition), that such conditions are assessed as risks to the programme, and are thoroughly managed long in advance of the first dose being offered.
I wrote earlier about the complex emotional, psychological and, for some, moral and spiritual aspects associated with the HPV vaccine (and other vaccines too). Those, along with the specific issues just listed, encapsulate many of the biggest challenges in risk communication. They demonstrate just how empathetic, skilled and knowledgeable programme managers, physicians and health workers need to be in every aspect of medical, scientific, social and psychological wisdom in order to help lay people make good decisions that they will not regret. Those decisions cannot always be based simply on data: intuition or ‘gut feeling’ may also be an important element, not to be dismissed as inevitably unreliable, especially under conditions of uncertainty, as Gigerenzer points out:
A gut feeling is neither caprice nor a sixth sense, nor is it clairvoyance or God’s voice. It is a form of unconscious intelligence. (Gigerenzer 2014)
He calls for a ‘heuristic revolution’ that requires ‘learning how to deal with uncertain worlds with the help of smart rules of thumb.’ While a doctor needs ‘statistical thinking to understand the results of medical research,’ he also needs ‘good intuitions to understand the patient’ (p. 32).
Hormone Replacement Therapy (HRT) and Menopause
Transition or Tragedy? Deficiency or Opportunity?
There are several contrasting narratives of menopause. We have to understand these in order to arrive at an authentic view for ourselves and to understand the differing feelings, values and beliefs of women who may seek advice or treatment. Appropriate risk communication will be shaped by how women view themselves and their time of life, as well as the nature and intensity of their symptoms.
First, a brief historical excursion to illuminate some of the roots of modern attitudes to female sexuality and reproduction. The myths of history: women’s organs, the uterus in particular, have, since ancient Greece, been thought to be the source of many diseases and afflictions, both physical and psychological. Hippocrates thought a ‘wandering womb’ might explain a range of symptoms. In the English-speaking world the Greek word for womb, ‘hystera,’ led to coining of the term ‘hysteria’ used as a label for all kinds of women’s problems, later, in the nineteenth century, especially applied to sexual dysfunction. Such was the negative and ill-informed view of women’s sexual anatomy, largely a male-construct, out of which modern attitudes to menstruation, pre-menstrual tension and menopause arose.
Many of the ‘witches’ executed at Salem in 1686 were menopausal women (Sarudy 2013). In the West, menopausal women were, in most respects, stigmatised as being past the useful (child-bearing) stages of their lives and, when they spoke up were seen as wilfully disruptive, and probably making a fuss about very little. In some cultures, menopause marked the transition to freedom, serenity and social respect, especially in the East (Southin 2014a). Worldwide, menstruation has been associated with all kinds of myths and superstitions covering the whole spectrum from being a sign of women’s superior powers to being evidence of a pact with the Devil (Southin 2014a). Menopause was first used as a technical term, almost certainly by de Gardanne in 1821. In the 1920s, hormones and the part they played in women’s biology began to be understood, and the modern era began, though many of the old prejudices and myths lingered on. (A fascinating historical timeline at (seahare.com); An Interdisciplinary Analysis of the Hormone Replacement Therapy Saga at (Ashton and Alvarez-Dardet 2005).)
Major Narratives
This section of the chapter is a socio-cultural exploration of menopause and its meaning, intended to help practitioners clarity their own position on the issue, and to illuminate the widely differing views that women will hold. Apart from an understanding of the risks and benefits of HRT, women will have quite different views on medication in general and on specific symptoms (for example, hot flushes, sleeplessness or mood-swings), depending on many variables, including their mental concept of menopause itself, their self-image and their levels of tolerance for discomfort. Risk communication and all aspects of the consultation must take account of these. If a physician is working from a different mental model, and does not recognise the discrepancy she may not offer or facilitate a solution that sensitively matches the patient’s preferences and needs.
1.
2.
3.
In a study of women from five racial/ethnic groups in the US, one study found:
Caucasian women reported significantly more psychosomatic symptoms than other racial/ethnic groups. African-American women reported significantly more vasomotor symptoms. Perimenopausal women, hormone users, and women who had a surgical menopause reported significantly more vasomotor symptoms. (Avisa et al. 2001)
Differing views of menopause and its meaning may have profound psychological effects:
…studies on Mayan and Greek rural women [referenced in the document referenced here] have reflected that they enjoy their sex life more after attaining menopause because they do not have the fear of becoming pregnant again…This could be a plausible explanation why Greek and Mayan women have fewer psychosomatic and psychological problems during midlife. (Dasgupta and Ray 2009)
Ignorance may, in some respects, be a kind of benefit:
Generally, women from developing countries, including those of the present study, tend to view menopause and its symptoms as a natural process that does not require medical care, so they are less aware about the health-related issues of menopause.
This is not to say that some women in developing countries don’t need help or support – even medication – to cope with menopause, but it does highlight the possibility that shining a spotlight on the problematic aspects of a condition may upset an otherwise balanced and tolerant view of it.
4.
This superficial sketch, then, indicates the complex and variable influences and context in which women experience menopause and in which they may (or may not) want health professionals to intervene. Risk communication, as noted earlier, must take account of all these variables, not least because of the damage that may be caused by women being treated by doctors whose views are not in line with their own or by their uncritically accepting marketing messages or solutions driven by male prejudice.
What Advice Can We Offer?
Women’s particular beliefs and values, fed from many sources, will influence how they experience menopause, what they want to do about the effects it has on their lives and how they view the remaining years of their lives. Physicians need to be very sensitive about their patients’ beliefs and values and highly aware of their own assumptions and prejudices (for example, do women have to be rescued from the pathology of menopause or supported through a normal phase of life?). Women who regard menopause as an intolerable plague in their lives, anxious to take any path that will relieve them of symptoms, need to be very carefully cautioned about the risks of excessive medication, of ostensible ‘bioidenticals’ and of unregulated, untested ‘natural’ remedies. Other women, however, maybe on very strong principle, will be looking for helpful advice about ways of managing symptoms (hot flushes or night sweats, for example) that do not involve medication. Reaching for the prescription pad will not please them.
Hormone Replacement Therapy
At the point a woman wishes to consider the possibility of HRT, she must have good risk information. Chapter 11 (Menopausal Hormone Therapy) summarises the best current knowledge and I shall not repeat the substance of that here.
If HRT is a suitable and acceptable method, then there is some good, high level risk information that appears to be agreed by most authorities:
The evidence suggests that HRT may be associated with an increased risk of: coronary heart disease; stroke; venous thromboembolism …; breast cancer; ovarian cancer; or endometrial cancer. These risks depend on how long HRT has been taken for, [type of HRT—ie, oestrogen-only or oestrogen plus progestogen], the woman’s age and underlying health, and are lower in healthy younger women.
The balance of risks and benefits differs between individual women according to her need for treatment. For all women, the lowest effective dose should be used for the shortest possible time, and treatment should be reviewed yearly.
No single recommendation for optimum duration of treatment or safe upper-age limit for use of HRT is therefore possible (MHRA 2007)
A number of sources of information for patients are available on the internet, but searchers are, as always, faced with the problem of knowing which are reliable and up-to-date. The Australian Menopause Society (AMS) is one such impressive-seeming source, but there are elements of that website that are not in line with the MHRA report (see reference above) which is regarded by many as the most authoritative current statement of evidence and knowledge.
The question of evidence aside, AMS has some useful material. There’s a short list of questions a woman might like to ask herself (or her doctor might ask her) as she weighs benefits and risks:
· How much do my symptoms impact on my quality of daily life?
· What could happen if I did nothing at all?
· What are my treatment choices?
· What are their risks and benefits? How reliable is the evidence for these risks and benefits? Are the findings of these studies relevant to me and my treatment?
· Have I now got enough information to make a decision?
Specifying the Risks
The MHRA report presents tables of attributable risk for oestrogen-only and combined HRT for women of various age groups, with and without a uterus, for treatment periods of 5 or 10 years. These provide the absolute figures, against background incidence, and overcome the sometimes alarming impact of relative risk figures. Here’s one of those tables, showing aggregation of all HRT risks, to illustrate the point (Table 19.2):
Table 19.2
Comparison of overall balance of benefits and risks associated with oestrogen-only and combined HRT in different prescribing scenarios (Table 6 (ii) from MHRA report) 5 years’ use of HRT in women aged 60–69 years
|
Type of HRT |
Baseline risk per 1,000 women |
Absolute risk in 1,000 HRT users |
Attributable risk in 1,000 HRT users |
|
Oestrogen-only (women with uterus) |
82 |
88 (82–97) |
6 (0–15) |
|
Oestrogen-only (women with uterus) |
85 |
97 (90–108) |
12 (5–23) |
|
Combined HRT |
70 |
92 (86–101) |
22 (16–31) |
Overall, this presentation of risk information is clear and simple for those with some level of numeracy, but it will not suit everyone.
Presentation as charts or on one of Paling’s palettes (Paling) as illustrated in Fig. 19.2 would offer further methods that might be more attractive or meaningful for some women.
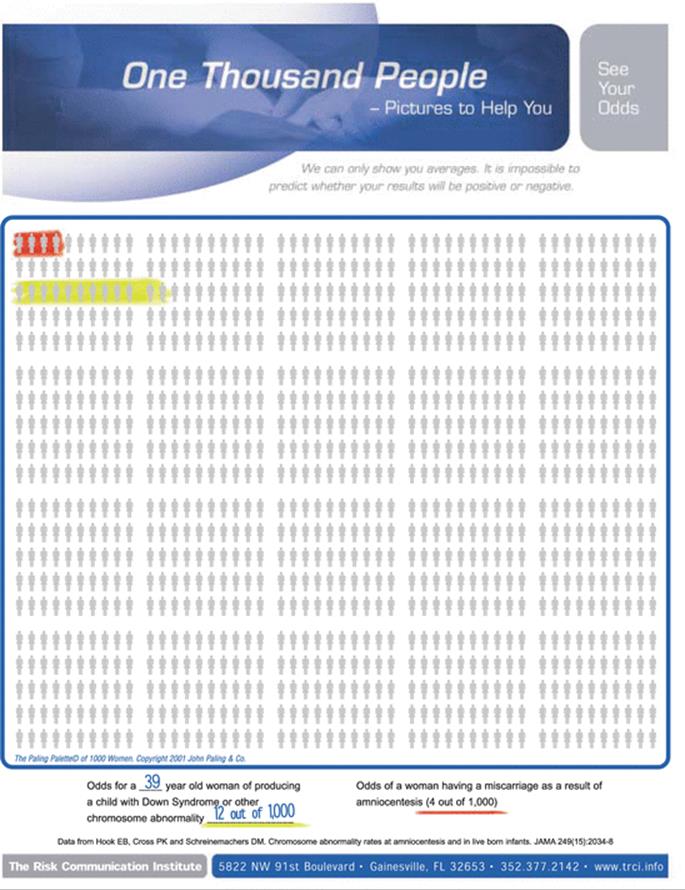
Fig. 19.2
John Paling’s work in risk communication is an invaluable resource. One of the principal tools he has developed is the palette, which allows absolute risk figures to be displayed visually for different populations (women, men, families) and different denominators (particularly 100 and 1,000). This one shows the odds of a woman aged 39 having a child with Down syndrome or other chromosomal abnormality (12/1,000) and the odds of a miscarriage as a result of amniocentesis. The great benefit of this approach is the display of harm and not-harm with absolute equity; the framing does not skew the data in either direction. For some patients this approach will be welcome, helpful and reassuring. (Paling) Gigerenzer also offers a range of imaginative and useful methods of graphic presentation of data, including excellent materials from the Harding Centre for Risk Literacy of which he is Director (Gigerenzer 2014)
In the booklet, produced by AMS, Menopause, Presenting a positive outlook (MacLennan and MacLennan 2012), there are some very elegant, well designed, well framed charts, like those shown in Fig. 19.3.
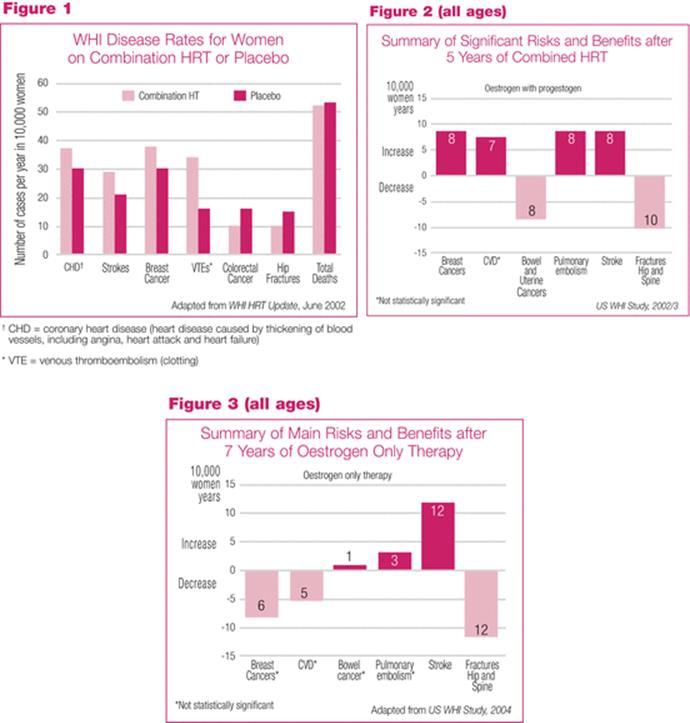
Fig. 19.3
Elegant and lucid presentation of complex information from the Australian Menopause Society (MacLennan and MacLennan 2012)
However, there are potential problems for some women. It may not be possible for many women to make sense of so much information on their own. Even these elegant and lucid materials will be quite beyond the reach of those with poor literacy and/or poor health literacy. Even literate women will wish to turn to their medical adviser for some kind of verbal exposition, overview and guidance about how the evidence applies to them. In any case, doctors and health workers need to have on hand first, the evidence and knowledge, and, second, a wide range of alternative methods of presenting it.
Decision Aids
The evidence and risk information, of course, relates to populations, not to individuals. The risks are different for every individual, dependent on many variables. One very effective way for a woman to better understand her own risk, or for a physician to help her do so, is to use a decision aid. The University of Sydney School of Public Health provides one such useful tool in its HRT risk calculator (Sydney). This is for a specific population of Australian women, around 50 years of age, suffering serious hot flushes and contemplating starting a regimen of combined HRT. It produces an individual risk profile derived from the population data. The calculations would be different for women in different parts of the world and specific decision aids would be necessary for them.
Because of the known risks of hormonal medication in menopause, there is pressure for the development of non-hormonal treatments. The FDA approved the first such medication in 2013 but rapid and heated controversy immediately arose about its safety (see Box 19.3).
Box 19.3 Controversial Non-hormonal Treatment for Moderate to Severe Vasomotor Symptoms
In June 2013, against the recommendation of its advisory committee, the FDA approved the first non-hormonal treatment for vasomotor symptoms, Brisdelle (paroxetine) which is a lower dose version of the antidepressant Paxil. The advisory committee voted 10 to 4 against there being any clinically significant benefit at 12 weeks in the company-sponsored trial. There was evidence of multiple harms, including dizziness, nausea, fatigue, mood swings and suicidality, side effects well recognised in patients taking higher dose SSRIs. The list of side effects for Brisdelle, from ‘rare,’ through ‘incidence unknown,’ to ‘more common’ has more than 100 items. It is in Worstpills.org’s stringent ‘Do not use’ category. It is marketed in a comfortingly mauve pack as the ‘first and only’ approved non-hormonal treatment for women who cannot or do not wish to use HRT.
Women and their physicians must make their own judgement about the benefit-harm profile of this drug, the comparative risks of HRT and the effects of no treatment. For the writer of this chapter, the question is how such a drug was ever approved (Drugs.com 2014a).
Risk Communication, Timing and the Media
HRT was the subject of a major public health scare in Australia in 2002 after the results of the Women’s Health Initiative (WHI) study were released. Although the absolute risk figures were included in the small print of the press releases, it was the relative risk figures that caught the attention of journalists and hit the headlines.
The front-page story in Australia’s largest circulation newspaper, the Sydney Daily Telegraph, was headlined as follows:
Medical warning
A study of sixteen thousand women shows links between long-term HRT and breast cancer. Don’t panic but Call your GP
A further dimension of the problem was that neither the Therapeutic Goods Administration (TGA) nor doctors had had prior information about the story and could not provide immediate information to the 600,000 women taking HRT, many of whom thought they now had a 26 % risk of breast cancer. The TGA handled the crisis with exemplary speed and decisiveness (critical for crisis management and resolution) by assembling its expert drug evaluation committee and issuing a definitive statement within 30 hours of the crisis breaking. Within 2 days, the issue had largely subsided and everyone began more or less calmly reassessing their view of the risks of long-term HRT (Case study in Expecting the Worst, Appendix 1A (Hugman 2013a)).
The simple lesson: relative risk figures are dangerous for everyone: any claim for risks or benefits, put forward by any party at all, that does not include absolute figures must be treated with critical scepticism, if not grave suspicion, even supposing the trials or figures on which they are alleged to be based are to be taken seriously which, from time to time, they are not. We must ask: a percentage or factor of what in terms of absolute numbers and class of event.
Conclusions About HRT
HRT has a complex mix of benefits and harms across a range of symptoms, organs and diseases. Some non-hormonal and non-medical treatments are available for some women for mild, even serious symptoms, one of which, referred to above, may be very risky indeed. Those who feel drawn to HRT as their favoured choice, maybe because of severely distressing symptoms, need to have a very clear idea of the benefits and risks as they apply to them individually. Doctors need a very considerable knowledge-bank of good evidence about HRT itself; about other methods of symptom management; and a creative, tailored range of methods for presenting and discussing it with each individual.
Conclusions
The challenging process of risk communication with individual patients has been presented in all its demanding detail. Apart from the pharmaceutical risks of medicines themselves, there are further substantial risks to safety, adherence and effectiveness, inherent in the disposition and character of the patient, that must be specifically addressed by prescribers or dispensers. Risk communication must take account of multiple variables intrinsic within patients and in the total context of their lives; it must also take account of the fact that many patients and many health professionals are seriously deficient in risk literacy.
In reviewing the risk communication elements of a small group of women’s conditions and medicines, it was clear that there was mostly good evidence about the benefits and harms of most of the medicines. However, as with all reproductive concerns, especially issues touching directly on motherhood and gender identity, there are other potent influences that will exercise women in their decision-making. ‘Clinical significance’ and perceived quality of life issues may not always be in step. Women, in all their immense and remarkable variety, need a synthesis of risk information that matches the profile of their individual needs, presented in ways that leave them free to make a decision that is best for them.
Take Home Messages
· Risk assessment is multi-factoral and requires painstaking, empathetic review and discussion for every patient
· Women will have profoundly different views of their sexuality and reproductive concerns depending on their personal philosophy, socio-economic status, country of domicile and many other factors
· Benefit-risk communications must be based on credible evidence and be shaped by the perceptions and priorities of the patient, including their response to uncertainty
· Risk communication about a specific medicine requires detailed and thorough attention if the patient is to avoid a number of common and unexpected risks and pitfalls and to gain maximum benefit from therapy
· Women’s health embraces a wide range of crucial issues beyond disease symptoms and the traditional concerns of medicine
· Some women’s medicines and conditions are subject to strong social, cultural and religious influences which must be taken account of in risk counseling
· Risk information for women is vulnerable to many distortions and misrepresentations, including male prejudices, social scares and commercial pressure, that require careful interpretation and management
· Risk communication demands the exercise of intense empathy if all individual, psycho-social and cultural obstacles and pitfalls are to be avoided and if the safety of patients is to be protected as far as is humanly possible
Acknowledgements for Chaps. 18 and 19 and Impressions of Women and Risk in West Africa (p. 502).
A number of colleagues, friends and members of my family, kindly helped me in the development of this material and their support is gratefully acknowledged: Edinam Amavi, Priya Bahri, Pia Caduff-Janosa, Ralph Edwards, Anna Gabrielsson, Andrew Herxheimer, Jenny Hugman, Laura Hugman, Marie Lindquist, Nana Yaw Osei-Bediako, Czarina Baeta Ribeiro, Audrey Sainsbury, Ch. Supt Ellen Sam, Kristina Star.
References
Ali H, Donovan B, Wand H, Read TRH, Regan DG, Grulich AE, Fairley CK, Guy RJ (2013) Genital warts in young Australians five years into national human papillomavirus vaccination programme: national surveillance data. BMJ 346:f2032PubMedCrossRef
American Academy of Neurology (2009) Management issues for women with epilepsy – focus on pregnancy: vitamin K, folic acid, blood levels, and breastfeeding. AAN summary of evidence-based guideline for CLINICIANS
Ashton JR, Alvarez-Dardet C (2005) An interdisciplinary analysis of the hormone replacement therapy SAGA. J Epidemiol Community Health 59(9):713
Australian T (2014) Gardasil not linked to blood clots: study. 9 July 2014
Avisa NE, Stellatoa R, Crawforda S, Brombergerb J, Ganzc P, Caind V, Kagawa-Singer M (2001) Is there a menopausal syndrome? Menopausal status and symptoms across racial/ethnic groups. Social Sci Med 52(3):345–356CrossRef
Barnett J, Breakwell GM (2003) The social amplification of risk and the hazard sequence: the October 1995 oral contraceptive pill scare. Health Risk Soc 5(3):301–313. doi:10.1080/13698570310001606996CrossRef
Bednarczyk R, Davis R, Ault K (2012) Sexual activity–related outcomes after human papillomavirus vaccination of 11- to 12-year-olds. Pediatrics, Published online 15 Oct 2012. doi:101542/peds2012-1516
BMJ (2013) Clinical evidence handbook. BMJ Evidence Centre, London
Boodman SG (2011) Many Americans have poor health literacy. The Washington Post, 28 Feb 2011
Borthen I, Eide M, Veiby G, Daltveit A, Gilhus N (2009) Complications during pregnancy in women with epilepsy: population-based cohort study. BJOG 116(13):1736PubMedCrossRef
Briesacher B, Gurwitz JH, Soumerai SB (2007) Patients at-risk for cost-related medication nonadherence: a review of the literature. J Gen Intern Med 22(6):864–871PubMedCentralPubMedCrossRef
Brown MT, Bussell JK (2011) Medication adherence: who cares? Mayo Clin Proc 86(4):304–314. doi:104065/mcp20100575 PMCID: PMC3068890
California Department of Public Health (2014) California experiencing a whooping cough epidemic. http://www.cdph.ca.gov/Pages/NR14-056.aspx
Casalino LP, Dunham D, Chin MH, Bielang R, Kistner EO, Karrison TG, Ong MK, Sarkar U, McLaughlin MA, Meltzer DO (2009) Frequency of failure to inform patients of clinically significant outpatient test results. Arch Intern Med 169(12):1123–1129PubMedCrossRef
CDC (2012) The PROTECT initiative: advancing children’s medication safety. http://www.cdc.gov/MedicationSafety/protect/protect_Initiative.html
CDC (2013) Reproductive health: contraception. http://www.cdc.gov/reproductivehealth/unintendedpregnancy/contraception.htm
CDC (2014) Vaccine safety: human papillomavirus (HPV) vaccine http://www.cdc.gov/vaccinesafety/Vaccines/HPV/index.html
Choices NHS (2012) HPV jab and teen promiscuity: ‘no link’. http://www.nhs.uk/news/2012/10October/Pages/No-link-found-between-HPV-jab-and-teen-sex-promiscuity.aspx
Conley M (2012) Blood clot risk higher in non-oral contraceptives. ABC News, 11 May 2011. http://abcnews.go.com/Health/higher-risk-blood-clots-oral-contraceptives/story?id=16321863
Craciun C, Baban A (2012) Who will take the blame?: understanding the reasons why Romanian mothers declined HPV vaccination for their daughters. ScienceDirect (Received 21 May 2012, Revised 23 July 2012, Accepted 7 Sept 2012, Available online 24 Sept 2012)
Dasgupta D, Ray S (2009) Menopausal problems among rural and urban women from eastern India. J Social Behav Health Sci 3(1):20–33. ©Walden University, Minneapolis. doi:105590/JSBHS200903102
Daily Mail Online (2014) Deadly risk of pill used by 1m women. Daily Mail, 2 Feb 2014
de Jong-van den Berg L, Tobi H, Bijker B, van den Berg P (2003) Influence of the third generation pill controversy on prescriptions for oral contraceptives among first time users: population based study. BMJ 326(254):254
Dixon S (2014) GPs warn 1m women of deadly blood clot risk. The Times, 2 Feb 2014
Drugs.com (2014a) Brisdelle side effects. http://www.drugs.com/sfx/brisdelle-side-effects.html
Drugs.com (2014b) Lamictal. http://www.drugs.com/lamictal.html
Dude A, Neustadt A, Martins S, Gilliam M (2013) Use of withdrawal and unintended pregnancy among females 15–24 years of age. Obstet Gynecol 122(3):595–600. doi:10.1097/AOG.0b013e31829d8074PubMedCrossRef
EMEA (2009) PRESS RELEASE EMEA statement on the safety of Gardasil. www.emea.europa.eu/docs/en_GB/document_library/Press_release/2009/11/WC500015448.pdf
EpilepsyAction (2014) How I coped when things didn’t go to plan. https://www.epilepsy.org.uk/pregnancy-diaries/how-i-coped-when-things-did-not-go-to-plan
Epilepsy Foundation (2011) Pregnancy and epilepsy. http://www.epilepsyfoundation.org/answerplace/Life/adults/women/Professional/pregnancy.cfm
Epilepsy Foundation (2014) Health outcomes in pregnancy and epilepsy. http://www.epilepsy.com/article/2014/3/health-outcomes-pregnancy-and-epilepsy-hopeforum-–-overview
FDA (2011) Topamax (topiramate) tablets and sprinkle capsules. http://www.fda.gov/safety/medwatch/safetyinformation/ucm195797.htm
Gigerenzer G (2014) Risk savvy. Allen Lane, London
Global Campaign ae (2012) Addressing the hidden, neglected but global problems of people with epilepsy. http://www.globalcampaignagainstepilepsy.org/
Gran Dahl M (2014) Distrust behind attitudes against the HPV vaccine. Upsala Nya Tydning, 15 Feb 2014
Greer G (1991) The Change: Women, ageing, and the menopause, Penguin Books, London
Guttmacher Institute (2006) Unintended pregnancy and induced abortion in Uganda
Guttmacher Institute (2013) Fact sheet; unintended pregnancy in the United States
Health Editor (1996) Pill scare based on wrong data EU claims. Independent, 20 Apr 1996
HONCode http://www.healthonnet.org/HONcode/Conduct.html
Hugman B (2013a) Expecting the worst, 2nd edn. Uppsala Monitoring Centre, Uppsala
Hugman B (2013b) Healthcare communication. Pharmaceutical Press, London
Jones R, Jerman J (2014) Abortion incidence and service availability in the United States, 2011. Perspect Sex Reprod Health 46(1):3–14, doi:101363/46e0414 46 (1):3–14. doi:10.1363/46e0414
Judicial Watch (2007) Judicial watch uncovers three deaths relating to HPV vaccine. http://www.judicialwatch.org/press-room/press-releases/judicial-watch-uncovers-three-deaths-relating-hpv-vaccine/
LaMendola B (2012) Up to one-third of patients don’t fill prescriptions. Sun Sentinel, 8 Apr 2012
Lattimer M. Advice on pill safety that led to the 1995 pill scare is reversed. http://www.prochoiceforum.org.uk/comm4.php
Lidegaard Ø, Nielsen LH, Skovlund CW, Løkkegaard E (2012) Venous thrombosis in users of non-oral hormonal contraception: follow-up study, Denmark 2001-10. BMJ 344(e2990)
Lock M (1998) Menopause: lessons from anthropology. Psychosom Med 60(4):410–419PubMedCrossRef
MacLennan A, MacLennan A (2012) Menopause, presenting a positive outlook. http://www.menopause.org.au/images/stories/public/docs/MenopausePositive2012.pdf.
Mayo Clinic (2011) Epilepsy and pregnancy: what you need to know. http://www.mayoclinic.org/healthy-living/pregnancy-week-by-week/in-depth/pregnancy/art-20048417?footprints=mine
MHRA (1999) Medicines Commission advice on third generation oral contraceptives and risk of venous thromboembolism. http://www.mhra.gov.uk/Safetyinformation/Safetywarningsalert-sandrecalls/Safetywarningsandmessagesformedicines/CON019572
MHRA (2007) UK public assessment report hormone-replacement therapy: safety update. Medicines and Healthcare Products Regulatory Agency, UK
National Coalition of Organized Women (2012) HPV Gardasil vaccine proves lethal – 47 girls now dead. http://www.youtube.com/watch?v=O7LH9TRCHuA
Ngugi A, Bottomley C, Kleinschmidt I, Wagner R, Kakooza-Mwesige A, Ae-Ngibise K, Owusu-Agyei S, Masanja H, Kamuyu G, Odhiambo R, Chengo E, Sander J, Newton C (2013) Prevalence of active convulsive epilepsy in sub-Saharan Africa and associated risk factors: cross-sectional and case-control studies. Lancet Neurol 12(3):253–263. doi: 101016/S1474-4422(13)70003-6. Epub 31 Jan 2013
NIH (2011) How to evaluate health information on the internet: questions and answers. http://ods.od.nih.gov/Health_Information/How_To_Evaluate_Health_Information_on_the_Internet_Questions_and_Answers.aspx
Ogbru O (2009) What you should know about your drugs. http://www.medicinenet.com/drugs_what_you_should_know_about_your_drugs/article.htm
Paling J. The Paling palettes. The Risk Communication Institute. http://www.riskcomm.com/paling_palettes.htm
Peterson G, Aslani P, Williams KA (2003) How do consumers search for and appraise information on medicines on the internet? A qualitative study using focus groups. J Internet Med Res 5(4). doi:http://dx.doi.org/10.2196/jmir.5.4.e33
Royal College of General Practitioners (2009) Assessment of adherence. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0015344/
Royal College of Obstetricians and Gynaecologists, UK (2013) Contraception and contraceptive use – study group statement
Sarudy BW (2013) 17C American women: timeline Salem witches -1692 Salem’s anti-woman witch hunt. http://b-womeninamericanhistory17.blogspot.com/2013/10/witches-timeline-of-1692-salems-anti.html
seahare.com. Menopause timeline 300 B.C.E. to present. http://www.seahare.net/Timelines/MenoChart.html
Seaman B (2003) The greatest experiment ever performed on women: exploding the estrogen myth. Hyperion, New York
Seumasach (2010) HPV vaccine controversy: India’s response puts the world to shame. InTheseNewTimes.com, Posted by seumasach on 31 Dec 2010
Singh S, Sedgh G, Hussain R (2010) Unintended pregnancy: worldwide levels, trends, and outcomes. Stud Fam Plann 41(4):241–250. doi:10.1111/j.1728-4465.2010.00250.xPubMedCrossRef
Southin TE (2014a) History and menopause. BellaOnline The Boice of Women. http://www.bellaonline.com/articles/art18392.asp
Southin TE (2014b) Japanese women and menopause. BellaOnline. http://www.bellaonline.com/articles/art16980.asp
Stopes M (1936) Change of life in men and women. Putnam, New York
Sydney Uo HRT DEcision Aid
TGA Gardasil (human papillomavirus vaccine) (2010). http://www.tga.gov.au/safety/alerts-medicine-gardasil-070624.htm#.UxtJpTGPLq1
Tomson T, Hiilesmaa V (2007) Epilepsy in pregnancy. BMJ 335(7623):769–773PubMedCentralPubMedCrossRef
Trussell J (2011) Contraceptive failure in the United States. Contraception 83(5):397–404PubMedCentralPubMedCrossRef
United Nations (2011) World contraceptive use 2011, United Nations, Department of Socail and Economic Affairs, http://www.un.org/esa/population/publications/contraceptive2011/contraceptive2011.htm
WebMD (2014) Seizure medication linked to birth defects. http://www.webmd.com/epilepsy/news/20040430/seizure-medication-linked-to-birth-defects
WHO (1999) Medical products and the internet: a guide to finding reliable information. World Health Organization, Geneva. http://apps.who.int/medicinedocs/en/d/Js2277e/
WHO (2004) Epilepsy in the WHO African region – World Health Organization, Geneva. http://www.who.int/mental_health/management/epilepsy_in_African-region.pdf
WHO (2003) Adherence to long-term therapies: evidence for action, World Health Organization, Geneva. http://www.who.int/chp/knowledge/publications/adherence_report/en/
Wilson RA (1968) Feminie forever. M Evans and Company, New York
Wolf N (2002) The beauty myth. Harper Perennial, New York
Women’shealth.gov (2012) Birth control methods fact sheet. US Dept Health and Human Sciences. http://www.womenshealth.gov/publications/our-publications/fact-sheet/birth-control-methods.html#d
Women’s Health Initiative (2002) Risks and benefits of estrogen plus progestin in healthy postmenopausal women, principal results from the women’s health initiative randomized controlled trial. JAMA 288(3):321–333. doi:10.1001/jama.288.3.321CrossRef