Marcelle I. Cedars
Michele Evans
The ovary is unique in that the age associated with decline in function (to frank failure) appears to have remained constant despite the increase in longevity experienced by women over the last century. Because the loss of ovarian function has profound impact on the hormonal milieu in women and on the subsequent risk for the development of disease via the loss of estrogen production, improving our understanding of reproductive aging is critical to care for all women.
Human follicles begin their development during the fourth gestational month. Approximately 1,000 to 2,000 germ cells migrate to the gonadal ridge and multiply, reaching a total of 5 to 7 million around the fifth month of intrauterine life. At this point, replication stops and follicle loss begins, declining to approximately 1 million by birth. In the human male, the dividing germ cells will become quiescent and maintain their stem cell identity. In women, between the weeks of 12 and 18, the germ cells will enter meiosis and differentiate. Thus, in the female, all germ stem cells have differentiated prior to birth. In the adult woman, the germ cells may remain quiescent, be recruited for further development and ovulation, or undergo apoptosis. Over time, the population of oocytes will be depleted, without regeneration, through recruitment and apoptosis until fewer than a thousand oocytes exist and menopause ensues. Approximately 90% of women experience menopause during the early 50s. The other 10% of women experience menopause prior to 46 years (often termed early menopause), with 1% of women experiencing menopause at an age less than 40 years (premature menopause or premature ovarian failure).
Menopause occurs at a median age of 51.4 years, with the age range in normal women being 42 to 58 years. The age of menopause appears to be determined largely by genetics and is due to exhaustion of the oocyte pool. Menopause and the years preceding are characterized by hormonal changes, decline in reproductive potential, and increased risk for physical and psychological changes.
The average age of menopause has remained constant throughout recorded history. It does not appear to be related significantly to race, parity, height, weight, socioeconomic status, or age at menarche. Evidence suggests that genetic and environmental factors influence age of menopause, although the specific nature of these relationships is poorly characterized. Given the strong association between age at menopause between mothers and daughters, this is likely a largely genetically determined trait. Environmental factors may not have a significant effect in themselves, but the interplay among environmental factors such as smoking (known to accelerate the age of menopause by 1.5–2 years), body mass index (BMI), alcohol use, and socioeconomic status and genetic risk, may be important.
According to the 2000 census data, 35% of the population is age 45 or older and 21% are over 55 years of age. Of the population, 7.3% are women 65 years or older (approximately 20 million women in the United States). Over 50 million women in the United States are in the menopausal transition or menopause.
REPRODUCTIVE STAGES
Reproductive aging is a continuum beginning in utero and ending with menopause. The stages along this continuum have been difficult to define. Numerous terms have been used clinically, including perimenopause, menopausal transition, climacteric, menopause, and postmenopause, to describe the end of this continuum. The Stages of Reproductive Aging Workshop (STRAW) was convened in July 2001 to address the lack of a pertinent reproductive staging system and to establish a nomenclature and guidelines, a consistent reproductive aging system for health practitioners, the medical research community, and the public.
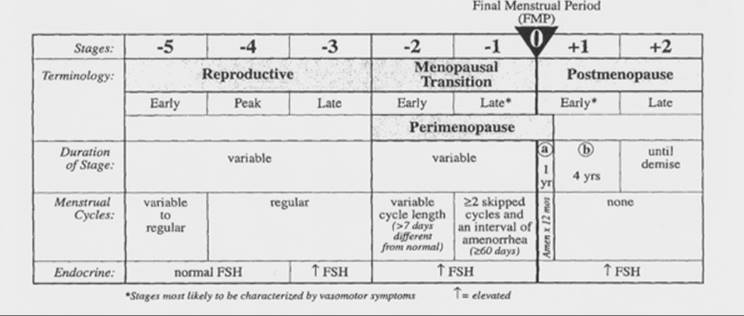
The staging system developed takes into account menstrual cyclicity, endocrinology and symptomatology beginning with menarche and ending with a woman's demise. The foundation of the staging system is the final menstrual period (FMP). Five stages precede the FMP and two follow it, for a total of seven stages. Stages -5 to -3 are called the reproductive interval, stages -2 to -1 are termed the menopausal transition, and stages +1 and +2 are known as the postmenopause (Fig. 41.1).
|
|
|
FIG. 41.1. Stages of reproductive aging. (From Soules MR, Sherman S, Parrott E, et al. Stages of Reproductive Aging Workshop (STRAW). J Womens Health Gend Based Med 2001;10:843–848, with permission.) |
The menopausal transition begins with variation in the menstrual cycle length (>7 days different from normal) in a woman with an elevated follicle stimulating hormone (FSH) level. This stage ends with the FMP, which cannot be determined conclusively until after 12 months of amenorrhea. Early postmenopause is defined as the first 5 years following the FMP. Late postmenopause is variable in length, beginning 5 years after the FMP and ending with the woman's death.
Although this staging system is said to include endocrinologic aspects of ovarian aging, it still depends largely on menstrual cyclicity as a key indicator of ovarian aging. It does include measurement of FSH; however, by the time FSH is elevated, even with cyclic menstrual cycles, oocyte depletion already has proceeded to such an extent that fertility (as a marker of reproductive aging) is diminished significantly. As noted above, evidence suggests that genetic and environmental factors influence both age of menopause and the decline in fertility, although the specific nature of these relationships is characterized poorly. Premature menopause can be due to a failure to attain adequate follicle numbers in utero or to an accelerated depletion thereafter. Potentially, either of these factors could be affected by genetic and environmental risk. The timing of menopause has a consistent impact on overall health with respect to osteoporosis, cardiovascular disease (CVD), and cancer risk. Over the next decade, it's estimated that more than 40 million women will enter menopause.
Oocyte Depletion
As discussed above, the leading theory regarding the onset of menopause relates to a critical threshold in oocyte number. Approximately 1,000 to 2,000 germ cells migrate to the gonadal ridge and multiply, reaching a total of 5 to 7 million around the fifth month of intrauterine life. At this point, replication stops and follicle loss begins, with a reduction to approximately 1 million by birth and 500,000 to 600,000 by menarche. As the number of oocytes in the reserve pool continues to decline, menstrual irregularity, followed by cessation, will occur. The theory that menopause is triggered primarily by ovarian aging is supported by the coincident occurrence of follicular depletion, elevated gonadotropin levels, and subsequent menstrual irregularity with ultimate cessation of bleeding.
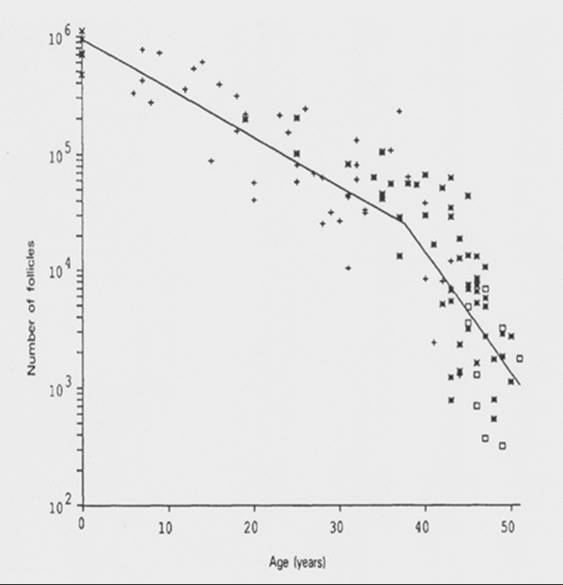
A mathematical model that predicts the rate of follicular decline has been developed (Fig. 41.2). It utilized existing data, which ultimately showed a bi-exponential decline, with an acceleration in oocyte loss when the remaining oocyte number equaled approximately 25,000. In this model, the decline occurred at 37.5 years of age. At this point, the rate of follicular atresia accelerates. In the absence of this acceleration, the model suggests menopause would be delayed until age 71. The cause of this accelerated depletion is not well defined. It is also clear that if the factor influencing the rate of decline is follicle number and not age, other factors which might account for a diminished follicle number (genetic risk and possible toxic exposure) would lead to an earlier rate of accelerated decline and an earlier age of menopause.
|
|
|
FIG. 41.2. Bi-exponential model of declining follicle numbers in pairs of human ovaries from neonatal age to 51 years old. Data were obtained from the studies of Block (1952, 1953) (x, n = 6; +, n = 43), Richardson and others (1987) (squares, n = 9), and Gougeon (unpublished) (*, n = 52). (From Faddy MJ, Gosden RG, Gougeon A, et al. Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Hum Reprod1992;7:1342–1346, with permission.) |
Coincident with the decline in the number of follicles in the ovary, there appears to be an increase in random genetic damage within these structures. Evidence for this comes from an observed increase in aneuploidy in the offspring of older mothers and the observation that, in women over 40 years old, oocytes harvested for in vitro fertilization are karyotypically abnormal approximately 40% of the time. Further examples in nature, such as Turner syndrome, shed some light on the process of oocyte aging. Individuals with this syndrome are, by and large, born with dysgenetic gonads which are devoid of follicles. Ninety-five percent of these individuals are aborted spontaneously prior to birth. If one examines the ovaries of a 20-week abortus, a full compliment of oocytes is present. Two factors have been isolated from the ovary: oocyte maturation inhibiting factor (OMI) and luteinizing inhibitor, which may control the rate of maturation of follicles. It has been suggested that individuals with dysgenetic gonads may fail to produce adequate OMI, thus allowing all follicles to progress prematurely toward maturity. The control mechanisms are conceptual rather than factual at this juncture, and new information will have to accumulate before the factors governing human oocyte atresia are elucidated more clearly.
Endocrinology
The entire endocrine system changes with advancing age. The somatotrophic axis begins to decline during the fourth decade prior to the loss of ovarian function. This decline in growth hormone is accelerated during ovarian failure and may, itself, accelerate the ovarian failure. However, pituitary concentrations of growth hormone, as well as adrenocorticotropic hormone and thyroid stimulating hormone, remain constant into the ninth decade. Although the thyroid gland undergoes progressive fibrosis with age and concentrations of T3 decline by 25% to 40%, elderly patients remain clinically euthyroid. Beta-cell function also undergoes degeneration with aging such that, by age 65 years, 50% of subjects have an abnormal glucose tolerance test result. Frank diabetes is rare, however, occurring in only 7%. The female reproductive system, on the other hand, undergoes virtually complete failure at a relatively early age.
As noted above, during the late fourth decade, FSH levels begin to rise even when cyclic menses continue. The most likely cause is a decrease in functional granulosa cells from the oocyte pool, with a decrease in inhibin B negative feedback allowing a monotropic rise in FSH. Early on, there is also a decline in luteal phase progesterone levels. As ovarian aging progresses, estradiol levels may be quite variable, with chaotic patterns and, occasionally, very high and very low levels. This dramatic variability may lead to an increase in symptomatology during the perimenopause (stages -2 to -1). As peripheral gonadotropin levels rise, luteinizing hormone (LH) pulsatile patterns become abnormal. There is an increase in pulse frequency with a decrease in opioid inhibition.
Estrogens
The main circulating estrogen during the premenopausal years is 17β-estradiol. These levels are controlled by the developing follicle and resultant corpus luteum. Oophorectomy will reduce peripheral estradiol levels from 120 to 18 pg/mL, which suggests more than 95% of circulating estradiol is derived from the ovary. Other sources include the peripheral conversion of testosterone and estrone. Very small amounts are secreted by the adrenal gland. Because the two-cell theory requires aromatization of androgens produced by the theca in the granulosa cell, follicular exhaustion is associated with gradual declines in estradiol concentrations.
The predominant estrogen in the postmenopausal woman is estrone, which has a biologic potency of approximately one third that of estradiol. Estrone is derived largely from peripheral conversion of androstenedione. Extraglandular aromatase is found in liver, fat, and some hypothalamic nuclei. This activity increases with aging and with a higher fat content (also an age-related change). Estrone and estradiol production rates during the postmenopause are 40 and 6 µg/day, respectively. This compares with 80 to 500 µg/day for estradiol during the reproductive years. Essentially, all the estradiol in the postmenopausal women is derived from conversion of estrone.
Androgens
Dehydroepiandrosterone (DHEA) and its sulfated conjugate, DHEAS, have been shown to decrease, along with adrenal corticotropin responsiveness, with aging. DHEAS levels decrease in both men and women. The decline is greater in women and may be due to the relative estrogen deprivation. Ovarian failure, at any age, accelerates this decline. Evidence suggests physiologic levels of DHEA may protect against neoplasia, enhance insulin action, protect against osteoporosis, increase immune competency, and offer some cardioprotection. Changes in DHEA levels also have been associated with alterations in body composition which, in themselves, appear to impact cardiac and breast cancer risk. DHEAS levels may also have an impact on “sense of mental well-being.”
Androstenedione is the predominant androgen during the reproductive years and production declines from 1,500 to 800 pg/mL in postmenopausal women. The postmenopausal ovary contributes only 20% to the circulating androstenedione. Testosterone levels also decline after menopause, but not to the same extent as estradiol levels. Postmenopausal testosterone is derived from the ovary (25%), the adrenal gland (25%), and extraglandular conversion from androstenedione (50%). The postmenopausal ovary produces a larger percentage of testosterone (50%) than does the premenopausal ovary.
Systemic Effects of Declining Ovarian Function
The decline in ovarian function brings about profound changes in secondary sexual organs. The endometrium becomes atrophic and the uterus decreases in size. Evidence is accumulating in animal models that the uterus may be partially responsible for the initial decline in reproductive capacity. On the other hand, data from human oocyte donor programs have shown that transfer of ova from younger donors to menopausal recipients produced normal gestations and offspring. It should be noted that these women are stimulated with an artificial sequential overlapping regimen of estrogen and progesterone. This produces an endometrium that is indistinguishable from that of the premenopausal state. Our own data have shown high implantation rates in older women with a hormonally induced endometrium. Only those women who receive pelvic irradiation have responded poorly, suggesting an alteration of the microvascular system.
The postmenopausal vagina, devoid of estrogen treatment, becomes smaller in both length and caliber. There is decreased elasticity of the vaginal wall, and the karyopyknotic index changes to show fewer superficial cells. The fallopian tubes contain both ciliated and secretory components. After age 60, cilia begin to disappear in the isthmic region, although they remain until a very old age in the ampulla infundibulum. The mammary gland develops secretory potential at the time of puberty and maintains this function until menopause. Like other secondary sex organs, it is dependent on female sex steroids for its maintenance. With cessation of the production of estrogen and progesterone, glandular, ductal, and stromal involution occurs. The basement membrane thickens and the luminal space becomes obliterated. Connective tissue of the lobule becomes indistinguishable from other types of connective tissue. There is an accumulation of adipose tissue in the breast, which occurs simultaneously with this involutional process.
Despite the involutional changes of the breast, 6% of patients with breast carcinoma are over the age of 50, with a median of 55. There is evidence for a bimodal distribution of breast carcinoma, with the first peak occurring at 45 years of age and the second at 65 years of age. The portion of estrogen receptor–positive breast cancers increases until ages 60 to 74 years. Therefore, a dichotomy appears to exist that ducts and glands, rapidly undergoing involution, the result of failing steroid production, become susceptible to malignant transformation while retaining a receptor molecule (E2), which normally is self-induced.
PREMATURE OVARIAN FAILURE
Premature ovarian failure (POF) is a unique entity in which a woman undergoes changes consistent with menopause, such as amenorrhea, elevated FSH levels, and depletion of ovarian follicles, prior to the age of 40. POF occurs in 0.1% of women under 30 years of age and 1% of women by age 40.
Genetic factors are thought to have a strong relationship with POF. There is a higher incidence of family history of early menopause and a suggestive increase in the family history of infertility, as well as an increased incidence of familial cases of early menopause amongst patients with idiopathic POF. Twin studies have likewise noted a strong genetic component to the age of menopause. Although inheritance appears to be either X linked or autosomal dominant sex limited, paternal transmission cannot be excluded. Women who have idiopathic early menopause (between the ages of 40 and 45) have a genetic pattern similar to whose with POF. These observations support the hypothesis of common underlying genetic factors, which may lead to an early decrease in fertility, early menopause, and POF.
POF may not be the same as age-appropriate menopause, which results from the depletion of the primordial follicle pool, because POF may be reversible, with follicles in the ovary, estradiol production, and even pregnancies long after the diagnosis. When using ultrasonography to evaluate the follicles in women with POF compared with age-appropriate menopausal and young women on oral contraceptives (OCPs), the mean ovarian volumes were smaller in patients with POF compared with women on OCPs, but not different from the women with age-appropriate menopause. Approximately 40% of patients with POF had follicles in the ovary, albeit fewer than in the normal premenopausal women.
Menstrual Cycle
Prior to the menopausal transition, the average length of a menstrual cycle ranges from 21 to 35 days. The menopausal transition is defined partially by menstrual irregularity that occurs in response to changes within the ovary, specifically, a dramatic decline in follicle number (and granulosa cell content). As a result, inhibin B levels fall, decreasing negative feedback on FSH, causing a monotrophic rise in FSH. This early cycle rise in FSH may shorten the follicular phase due to accelerated folliculogenesis. Estradiol levels remain relatively constant with age until the menopausal transition, when they initially rise in response to increased FSH levels. As the ovary fails, progesterone levels decline, leading to a shortened (or inadequate) luteal phase. Thus, an early sign of waning ovarian function may be a decreased intermenstrual interval. Precycle spotting may also signal deficiencies in progesterone production. These clinical signs of reproductive aging indicate a poor prognosis for those women still interested in reproduction. As the FMP approaches and the oocyte complement declines to a critical level, estradiol levels fall, leading to hot flashes, vaginal atrophy, and accelerated bone mineral density (BMD) loss. Also, as the FMP approaches, there is a steady trend toward an increased mean cycle length. In a woman's final 10 to 20 cycles, average cycle lengths are characteristically 40 to 42 days.
As menstrual irregularity increases during the menopausal transition, many women seek medical care. Treatment can be approached in several ways. After a complete history and physical examination, bleeding irregularities can be treated with different hormonal regimens including OCPs, cyclic hormone replacement therapy (HRT), or progestin-only therapy. Many of these patients continue to ovulate, albeit irregularly, so the addition of cyclic progestin (without estrogen) may further increase cycle irregularity and does not offer contraceptive protection. Thus, treatment with OCPs or a combined, cyclic estrogen-progestin regimen is advisable.
There is always the risk of endometrial hyperplasia in this age group. Patients considered high risk (history of chronic anovulation or obesity, or suspicious bleeding patterns such a watery, bloody discharge) should undergo endometrial sampling. Pelvic ultrasonography for measurement of endometrial stripe thickness is not a reliable predictor of risk in cycling women. For those who have a relatively new onset of bleeding irregularity (consistent with the menopausal transition in a previously ovulatory woman), consideration can be given for initial hormonal treatment, with endometrial biopsy reserved only for those whose cycles fail to normalize after 3 months of therapy.
Postmenopausal bleeding always should be considered abnormal and must be evaluated accordingly. Bleeding can occur from the rectum, vagina, cervix, urethra, or uterus. A thorough history and physical examination is crucial. If the source of bleeding is uterine, a transvaginal ultrasonographic examination can be very helpful. If the endometrial stripe is thinner than 5 mm, the bleeding is typically the result of an atrophic endometrium. If the endometrium is 5 mm or thicker, it is imperative to perform a diagnostic test, either an endometrial biopsy or dilation and curettage, to sample the endometrium.
Menopausal Syndrome
Given the above endocrinologic changes with aging, many symptoms associated with aging in women are due to estrogen deficiency, but the decline in adrenal androgens and growth hormone may contribute. Symptoms definitely due to estrogen deprivation include vasomotor symptoms and urogenital atrophy. Osteoporosis is likely, largely due to estrogen deficiency, but this may be exacerbated by the relative growth hormone decline. The same may be said for the hormone-related changes of increasing atherosclerotic CVD and psychosocial symptoms including insomnia, fatigue, short-term memory loss, and depression. Both DHEAS and growth hormone may well have an impact on these age-related symptoms.
Vasomotor Symptoms
Vasomotor instability in the form of a hot flash (flush) is one of the most consistent and bothersome symptoms that women face as they enter the menopausal transition and subsequent menopause. Hot flashes result from estrogen deficiency and a resetting of the hypothalamic thermoregulatory set point. They occur in 65% to 76% of women who undergo spontaneous menopause or surgical oophorectomy. Symptoms may begin during the menopausal transition, when estrogen levels may fluctuate dramatically from cycle to cycle and even day to day.
A hot flash usually is characterized by intense warmth, described as “heat or burning” that usually begins in the head, neck, and thorax and can spread in waves over the entire body. It may be preceded by pressure in the head and may be accompanied by heart palpitations. The hot flash usually is followed by an outbreak of sweating, followed by chills as the body's thermostat resets. The length of the episode varies from seconds to approximately 5 minutes, although episodes as long as 30 minutes have been described. The event frequency varies from a few per year to 30 per day.
For most women, the hot flashes commence prior to the FMP, although initially this may be perceived only as a sleep disturbance. In general, the episodes are noted more frequently at night, and the dysfunctional sleep pattern that follows may result in fatigue, irritability, loss of concentration, and depression, symptoms that often are elicited from patients in the menopausal transition. More than 80% of women who experience hot flashes will experience them for longer than 1 year. Twenty-five percent of women complain of severe hot flashes. Without treatment, the symptoms usually subside slowly over 3 to 5 years. Investigators in 25-year longitudinal study from Gothenburg, Sweden, with 1,462 participants, found the prevalence of hot flashes a maximum of 60% at 52 to 54 years of age. Interestingly, 9% of subjects still reported hot flashes at age 72.
The etiology of hot flashes seems to be the withdrawal of estrogen rather than the state of hypoestrogenism. For example, women with Turner syndrome who have not been treated with exogenous estrogen do not experience hot flashes. Those who are treated with estrogen, which is later withdrawn, will experience symptoms of vasomotor instability. Obese women seem to be less symptomatic than matched controls with lower BMI. The explanation may be that obese women are less hypoestrogenic secondary to peripheral conversion of adrenal androgens into estrone or that obesity lowers sex hormone-binding globulin levels, allowing a greater proportion of their estrogen to remain unbound and able to act on target tissues. Studies of hot flashes with external monitoring of skin temperature and resistance have shown a frequency of approximately 54 plus or minus 10 minutes. This frequency has been shown to interrupt random eye movement sleep and potentially contributes to some of the psychosocial complaints. Hot flashes are correlated temporally with pulses of LH; however, exogenous LH does not induce a flash, suggesting there is some central mediator leading simultaneously to hot flashes and LH pulses.
Several biochemical alterations are associated with the hot flash. During the actual episode, there is evidence of a rise in plasma LH, epinephrine, corticotropin, cortisol, androstenedione, DHEA, β-lipotropin, β-endorphin, and growth hormone. Levels of estradiol, estrone, prolactin, thyroid stimulating hormone, FSH, and norepinephrine are unchanged.
Treatment
Vasomotor symptoms are the most common indication for use of estrogen treatment in menopause and are also a U.S. Food and Drug Administration (FDA)-approved indication. Estrogen therapy, in either oral or transdermal form, has a greater than 95% efficacy for the treatment of hot flashes. Hot flash frequency is first notably reduced after 2 weeks of treatment, and the full effect of a certain dosage can be determined reliably after 4 weeks. Due to concerns over the risk-benefit analysis of HRT use, it is recommended that women be treated for vasomotor symptoms for short periods (1-4 years) and then gradually tapered, because symptoms often recur when treatment is discontinued abruptly. For patients with contraindications to estrogen use, vasomotor symptoms can be treated, albeit less efficiently, with progestins, α2-adrenergic agonists (clonidine, methyldopa, lofexidine) and, possibly, antidepressants (selective serotonin reuptake inhibitors [SSRIs], venlafaxine hydrochloride [Effexor]).
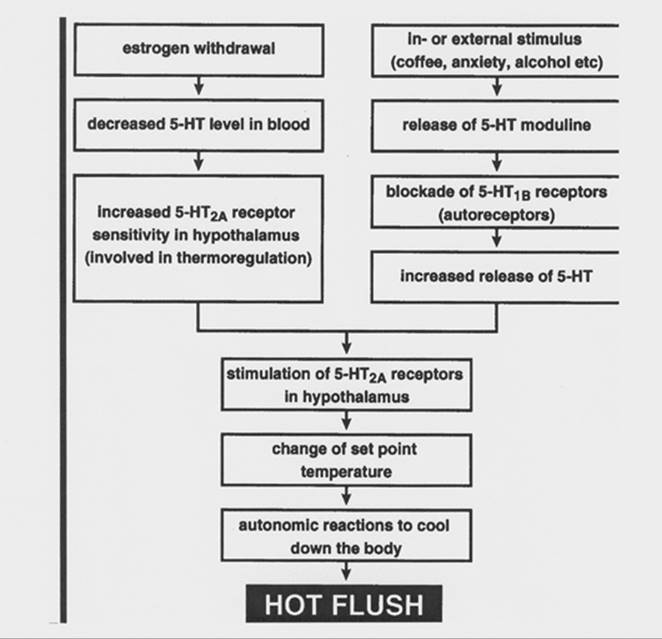
The role of serotonin (5-hydroxytryptamine [5-HT]) in symptoms of menopause is being investigated increasingly. Serotonin levels fall with menopause, either naturally or surgically induced, and replacement estrogen is known to increase serotonergic tone. The 5-HT2A receptor subtype is thought to underlie changes in thermogenesis. Stimulation of this receptor may lead to changes in the set-point temperature, leading to autonomic changes which cool the body. An increased skin temperature and sweating may result. Thus, an involvement for the 5-HT2A receptor in the etiology of hot flashes has been suggested. A theoretical model, illustrating a role for 5-HT in the mechanism of the hot flash, is shown in Figure 41.3.
|
|
|
FIG. 41.3. Possible mechanism by which a hot flush is induced. (From Berendsen HH. The role of serotonin in hot flushes. Maturitas 2000;36:155–164, with permission.) |
Most studies using SSRIs for the treatment of vasomotor symptoms have been in patients with breast cancer. The differential between the antidepressant effects of these agents versus a direct effect on vasomotor symptoms may be more difficult to detect in this population.
Genitourinary Atrophy
Vagina
A decrease in circulating estrogen levels has deleterious effects on urogenital epithelium. Up to 50% of postmenopausal women experience symptoms of vaginal atrophy. The most common symptoms include dryness, irritation, itching, burning, and dyspareunia. Atrophic vaginitis is associated with a rise in vaginal pH, which can lead to more frequent infections and worsening, irritative symptoms. A concurrent decrease in vaginal lubrication can lead to bleeding and decreased sexual comfort and pleasure.
Estrogen replacement therapy (ERT) is an effective treatment for vaginal atrophy. The systemic dosage necessary for vaginal protection is somewhat higher than needed for bone protection (see below) and, thus, topical therapy by means of creams or vaginal rings may be advisable to limit systemic absorption. Unless systemic HRT is required for vasomotor instability, local estrogen therapy can be used effectively to treat urogenital atrophy. Vaginal estrogen cream or tablets can be used daily for approximately 2 to 3 weeks, and then twice weekly after initial symptoms have improved and vaginal vascularization (hence, hormone uptake) have increased. Treatment is usually long term, because symptoms tend to recur when estrogen is discontinued. The twice-weekly estrogen regimen can be used without supplemental progestin without an increase in endometrial thickness. The dosage should be kept low, however, because the well-vascularized vagina is extremely efficient in the absorption of steroids. The new low-dose vaginal ring may also be used without progestin protection of the endometrium.
Vaginal estrogen frequently will improve symptoms of urinary frequency, dysuria, urgency, and post-void dribbling. A direct effect to improve urinary incontinence is less clear. Alternatives to estrogen include vaginal moisturizers and lubricants. There is no evidence to support the use of agrimony, black cohosh, chaste tree, dong quai, witch hazel, or phytoestrogens for the treatment of atrophic vaginitis.
Urinary Tract Infections
Urinary tract infection (UTI) is common among women of all ages. Worldwide, an estimated 150 million UTIs occur annually. In the United States, UTIs account for more than $6 billion in health care costs. The incidence is highest in 18- to 24-year-old women at 17.5% and is 9% for women older than 50 years. In younger women, the major risk factors for recurrent UTI are sexual intercourse and spermicide exposure. In older, institutionalized women, the most important risk factors include urinary catheterization and functional status.
Healthy, postmenopausal women have different risk factors for recurrent UTI than those mentioned above. Recurrent UTIs in healthy postmenopausal women are associated with urinary incontinence, cystocele, and increased post-void residual volumes. Other significant risk factors include at least one episode of UTI prior to menopause, urogenital surgery, and reduced urinary flow. From the Heart and Estrogen/progestin Replacement Study (HERS) of postmenopausal women with coronary heart disease (CHD), additional risk factors included diabetes, vaginal itching, and vaginal dryness.
Changes in the vaginal environment after menopause may also predispose to UTI. These alterations include the absence of lactobacilli, elevated vaginal pH, and increased rate of vaginal colonization with Enterobacteriaceae. The intravaginal administration of estrogen has been shown to reduce the rate of recurrent UTI by normalizing the vaginal environment. Low-dose oral hormone therapy, with conjugated estrogen plus medroxyprogesterone acetate (MPA), does not reduce the frequency of UTIs in older women.
Urinary Incontinence
The prevalence of urinary incontinence in menopausal women is estimated to be in the range of 17% to 56%. Urinary incontinence is the eighth most prevalent chronic medical condition among U.S. women. Anatomic and physiologic alterations associated with aging and incontinence include thinning of the urethral mucosa, reversal of the proteoglycan-to-collagen ratio in the paraurethral connective tissue, decrease in urethral closure pressure, and changes in the normal urethrovesical angle.
Many risk factors have been associated with incontinence. Menopause often is considered to be one of these risk factors, especially because a prevalence peak in midlife has been reported by many authors. Epidemiologic studies generally have not found an increase in the prevalence of urinary incontinence in the menopausal transition.
A risk factor for incontinence is an increased BMI. This is an especially important factor, because it is modifiable. Vaginal delivery is associated with transient postpartum incontinence, as well as an increased risk of incontinence later in life. Interestingly, a study of nulliparous nuns, with mean age of 68, found that 50% of the nuns had urinary incontinence. Meta-analyses have found an association between hysterectomy and urinary incontinence, with an increase in incontinence of 60%. Considering that more than 600,000 hysterectomies are performed yearly in the United States and that approximately 40% of women have undergone hysterectomy by age 60, these results are quite relevant. Women should be counseled about this relationship prior to undergoing hysterectomy. Other significant risk factors include history of UTI and depression.
Treatment
Oral ERT has been shown to restore the genitourinary connective tissues to that of premenopausal women, but it seems to have little short-term clinical benefit in regard to urinary incontinence. Interestingly, oral estrogen replacement is associated consistently with an increased risk of incontinence in women aged 60 years and older in epidemiologic studies. This increase may reflect that women with more severe symptoms seek medical care and HRT more often than asymptomatic women. It is also possible that the local levels of estrogen in these studies was too low to benefit fully the urogenital system, given the data suggesting higher systemic dosages may be needed for a vaginal effect.
Osteoporosis
Osteoporosis is a condition in which bone loss has been sufficient to allow mechanical fracture with limited stress. The likelihood of developing osteoporosis is dependent on the combination of peak bone density (stressing the importance of bone building in the young) and the rate of loss (accelerated with estrogen deficiency). Primary, or “senile,” osteoporosis usually affects women between the ages of 55 and 70 years. The most common sites include the vertebrae and the long bones of the arms and legs. Secondary osteoporosis is caused by a specific disease (such as hyperparathyroidism) or medication usage (glucocorticoids, thyroid hormone excess, anticonvulsants).
Menopausal bone loss begins before the FMP during stage -1. Postmenopausal osteoporosis causes over 1.3 million fractures annually. Most of the 250,000-plus hip fractures are due to primary osteoporosis. Excess mortality may exceed 20% within a year of a hip fracture and, because 75% of patients lose their independence, the social costs, not to mention the financial costs, are great.
Bone loss following natural menopause is approximately 1% to 2% per year, compared with 3.9% per year following oophorectomy. A woman's genetic background, lifestyle, dietary habits, and coexisting disease will impact the development of osteoporosis. Cigarette smoking, caffeine use, and alcohol consumption are associated with increased bone loss, while weight-bearing activity appears to slow it.
Approximately 30% of postmenopausal women have osteoporosis. The World Health Organization has defined osteoporosis as a hip BMD value, as measured by dual x-ray absorptiometry (DEXA), that is greater than 2.5 standard deviations below the adult peak (mean level for young, white women: t-score). Women with existing fractures, regardless of BMD, are also classified as osteoporotic. Both groups are at increased risk for fractures. Those patients with a low z-score (age-matched comparison) should be investigated for secondary causes of osteoporosis.
Peak bone mass in women is achieved by the end of the third decade and is an important contributor to bone strength in later life. Adolescence is a critical period of rapid skeletal growth during which almost one half of the adult bone mass is accrued. Many factors contribute to a woman's peak skeletal mass including heredity, diet, physical activity, and endocrine milieu. Hormones which may be a factor in peak bone mass attainment include insulinlike growth factor (IGF)-1, which regulates skeletal growth, and gonadotropins which stimulate sex steroid production and epiphyseal maturation. Estrogen deficiency and amenorrhea can decrease peak bone mass, whereas weight-bearing exercise leads to an increase. Early influences, including birth weight and poor childhood growth, are linked directly to risk of hip fracture. Independent predictors of low peak bone mass include low body weight, menarche at over 15 years of age, and physical inactivity as an adolescent. Early intervention during childhood and adolescence may reduce a woman's risk for osteoporosis in later life—this includes adequate calcium intake and education regarding diet, ideal weight, and physical activity.
Treatment
Hormone Replacement Therapy. HRT has been used widely for the prevention of osteoporosis and is FDA approved for this indication. It is clear that HRT helps prevent bone loss, as indicated by increased BMD. Whether these benefits translate into decreased fracture risk has been an important topic of research for the past decade. Observational studies have shown lower vertebral and nonvertebral fracture rates in women receiving estrogen compared with those not receiving this therapy. The addition of a progestin does not alter these results. However, observational studies may be biased, because women using HRT have better access to medical care and maintain healthier lifestyles in general.
Estrogen therapy acts via an inhibition of bone resorption. Although both BMD and fracture rate are improved with estrogen therapy, there is a rapid and progressive loss of bone mineral content after cessation of estrogen therapy. By 4 years after therapy, bone density is no different from that of patients who were never treated with estrogen.
Although estrogen is approved for prevention of osteoporosis, there is some evidence to support its usage in treatment. Dosages of 0.625 mg of conjugated estrogen and, more recently, as low as 0.3 mg have been shown to slow bone loss and provide adequate protection against the development of osteoporosis. Higher dosages may be required to treat existing disease.
Meta-analysis of randomized trials shows an overall 27% reduction in nonvertebral fractures in a pooled analysis, with the effect being greater in women under 60 years of age. The HERS trial showed no evidence of reduction in incidence of fractures or rate of height loss in older women with CHD not selected for osteoporosis. The Women's Health Initiative (WHI), the first randomized primary prevention trial studying the effects of postmenopausal HRT, showed a significant reduction in hip fracture (hazard ratio [HR] = 0.66; CI = 0.45–0.98). It seems clear that HRT must be taken indefinitely to preserve bone mass.
Calcitonin. Calcitonin is a hormone normally secreted by the thyroid gland and responsible for calcium homeostasis. Calcitonin is now available as a nasal spray, specifically developed to decrease local side effects caused by the earlier subcutaneous injection. Intranasal calcitonin has been shown to improve spinal bone density and decrease the vertebral fracture rate in women with established osteoporosis. The increase in bone density appears to peak in as little as 12 to 18 months. This may be due to down-regulation of the calcitonin receptors and the development of neutralizing antibodies. Although few studies have been performed and no data are available regarding calcitonin-related reductions in hip fracture, calcitonin does seem to be especially beneficial for women with a recent and still painful vertebral fracture. Unfortunately, it appears some patients do not respond to this therapy and those nonresponders cannot be identified prospectively.
Bisphosphonates. These nonhormonal compounds are analogs of pyrophosphates which have an affinity for hydroxyapatite in bone. The basic molecular structure of bisphosphonates allows a large number of manipulations, producing different types of bisphosphonates which vary considerably in their potency. The first one used clinically was etidronate, the least potent. In succeeding order of development were pamidronate, alendronate, and risedronate, which is the most potent of these compounds. Etidronate, if given continuously for more than 6 months, impairs mineralization of bone and may cause osteomalacia. There have been occasional reports of pamidronate also causing impairment of mineralization of bone. However, continuous administration of either alendronate or risedronate has not caused osteomalacia.
Alendronate has been evaluated more extensively than calcitonin and has a proven track record, reducing the risk of all major fracture types (vertebral and nonvertebral) in women with osteoporosis. In one study, risk of hip fracture was reduced by 53%, clinical vertebral fracture by 45%, and wrist fracture by 30%. For all fracture types, some reduction in fracture risk was evident within the first year of treatment. Bisphosphonates have only a modest effect on BMD early in the treatment course. Because alendronate is effective so quickly in reducing fracture risk, mechanisms other than increased BMD, such as changes in bone remodeling rates, may play a role in fracture reduction.
Alendronate has been shown to inhibit markers of bone remodeling and to increase BMD at the lumbar spine, hip, and in all other bones. Bone density increases with alendronate are greater than with calcitonin and are equal to that with HRT. The escape phenomenon seen with calcitonin is not seen with alendronate, which has the advantage of oral administration. The recommended daily dosage of 10 mg, however, must be taken according to a very strict dosing schedule (in the morning on an empty stomach, with the patient required to remain upright for 30 minutes thereafter). The medication has very poor bioavailability (approximately 1%) and, thus, these restrictions must be followed precisely. Alendronate also has a propensity for irritation of the esophagus and stomach, especially in women with preexisting esophageal reflux or gastric or duodenal disease. A newer formulation allows for once-weekly administration, and development of a once-yearly intravenous formulation may further decrease side effects and administration difficulties.
Risedronate has been shown to reduce substantially the risk of both vertebral and nonvertebral fractures, also. Bone density is increased in both early postmenopausal women and those with established osteoporosis.
The final remaining question concerning bisphosphonates has to do with the near-permanent changes in bone with the incorporation of this agent into the bone matrix. Although short-term fracture data appear favorable, the long-term effects of these agents and the ability of bone treated with bisphosphonates to heal (e.g., following hip fracture) are not known.
Raloxifene. Raloxifene is the first of a new generation of compounds known as selective estrogen receptor modulators (SERMs) to have a treatment indication for osteoporosis. It is likely that there will be an explosion in the development of SERMs in the years to come. They may represent a new alternative for our patients with breast cancer or for long-term use in all patients. These new agents act as selective estrogen receptor agonists on the bone and possibly the heart and antagonists of estrogen action on the breast and uterus. Effects on the brain are not well characterized and likely will vary among compounds (see below). Data on raloxifene suggests good preservation of bone density, albeit less than seen with alendronate or HRT, and fracture data further supports a protective effect.
It is believed that the differential effect of estrogen agonists (estrogens) and estrogen antagonists (“anti”-estrogens) is related to the transcriptional activation of specific estrogen-response elements. There appear to be two different domains of the estrogen receptor (AF-1 and AF-2) responsible for this transcriptional activation. Estrogen agonists and estrogen antagonists appear to act via different domains, resulting in their differential effects. Both appear to act to maintain bone density, at least partially, via regulation of the gene for transforming growth factor-β. It has further been suggested that there may be a raloxifene-response element, which is distinctly different from the estrogen-response element.
In women with osteoporosis, the 60-mg or 120-mg daily dose of raloxifene increases bone mass density in the spine and femoral neck and reduces the risk of vertebral fracture by 30% to 50% over no treatment. However, as with estrogen use, women receiving raloxifene have an increased risk of deep vein thrombosis compared with women receiving placebo.
Calcium and Vitamin D. Calcium and vitamin D are important components of all three antiresorptive agents (calcitonin, bisphosphonates, SERMs). Decreased ability to absorb calcium among older women is due, in part, to impaired vitamin D activation and effect. In addition, older women may have limited exposure to sunlight, and their dietary vitamin D intake may be lower than that of their younger counterparts. Daily calcium intake of 1,500 mg and 400 to 800 IU of vitamin D per day is, in and of itself, probably sufficient to reduce the risk of fragility fractures by about 10%.
Summary-Osteoporosis
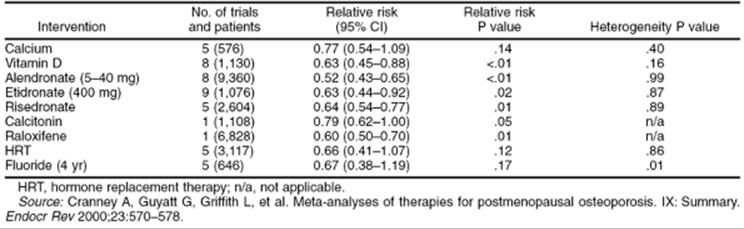
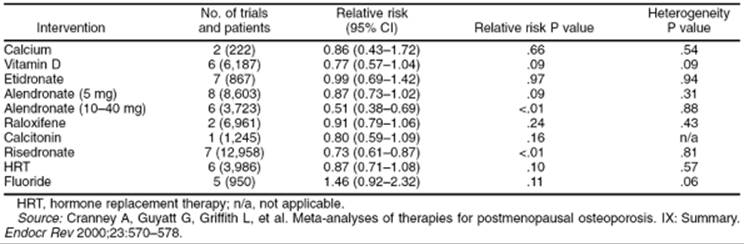
Most current strategies regarding osteoporosis treatment have focused on identifying postmenopausal women who have low BMD and are already at increased risk for fracture. An evidence-based approach is to recommend appropriate calcium and vitamin D intake, smoking cessation, weight-bearing exercise, moderation in alcohol consumption, and fall prevention. If pharmacologic therapy is indicated, one of the above FDA-approved regimens should be instituted (Table 41.1 and Table 41.2). An alternative (complementary) approach to prevention is to focus on intervention beginning in childhood and adolescence, with attention to achieving maximal peak bone mass and minimizing premenopausal and postmenopausal bone loss.
|
|
|
TABLE 41.1. Magnitude of Effect on Vertebral Fractures |
|
|
|
TABLE 41.2. Magnitude of Effect on Nonvertebral Fractures |
Cardiovascular Disease
CVD is the number one killer of both men and women in Western societies and is attributed primarily to age and lifestyle. Lifestyle modifications are well known to decrease the incidence of CVD. For women, CVD is largely a disease of the after menopause. Women will now spend more than a third of their lives beyond menopause and, thus, preventive measures are paramount. A large body of observational evidence supports a protective effect of ERT on CVD. Observational data, however, are limited by the confounding variables of patient self-selection. Animal and in vitro studies, as well as assessment of surrogate markers in women, have shown a positive effect of estrogen and (less so) HRT against CVD development.
Approximately 2.5 million women in the United States are hospitalized each year for cardiovascular illness. CVD claims the lives of 500,000 women annually. One half of these deaths are due to CHD, making this the most frequent cause of death among U.S. women. CVD can be separated into two categories, (a) CHD and (b) noncoronary CVD, such as stroke, valvular heart disease, peripheral vascular disease, congestive heart failure, and sudden death from cardiac causes.
A woman's risk of heart disease is far lower than a man's risk until after menopause. This change in incidence of heart disease may be related to advancing age, changes in hormonal milieu, or other unknown factors. CHD entails a worse prognosis for women than for men following either medical or surgical therapies. These sex discrepancies may reflect the older age, smaller body size, more frequent and severe coexisting illnesses of women and, perhaps, a higher incidence of delayed or suboptimal care.
Chest pain or tachycardia may be overlooked as benign problems in women, potentially caused by depression, anxiety, or panic disorders. These misperceptions may lead to bias in evaluating women with chest pain. Chest pain in women may also have atypical clinical pictures compared with the more “classic” symptomatologty in men. Chest pain, regardless of symptoms compatible with angina pectoris, warrants evaluation for CHD, regardless of sex.
If a woman seeks treatment for typical, or atypical, signs and symptoms of myocardial ischemia, a careful clinical history, including assessment of cardiac risk factors, should be taken. Electrocardiographic exercise testing is recommended for women who give a history typical of angina pectoris if the resting electrocardiogram findings are normal. When the resting electrocardiogram results are abnormal, the patient should be referred for either perfusion imaging studies or coronary arteriography. No screening test is of value for asymptomatic patients, even when risk factors are present.
Fewer symptomatic women than men undergo diagnostic coronary arteriography and therapeutic angioplasty or bypass surgery. Women who do undergo bypass surgery more often require emergency surgery and typically are sicker than men at the time of intervention. They have increased operative mortality rates and postoperative complications. It seems that women are referred for revascularization procedures at a later, more symptomatic, stage of illness. Both coronary angioplasty and coronary bypass surgery have a comparable long-term survival for men and women who survive the initial hospital stay. Beta-blockers and aspirin are equally efficacious in both sexes in preventing reinfarction after myocardial infarction.
Women should be encouraged to seek medical attention if they have any symptoms suggestive of myocardial ischemia. Physicians should emphasize the importance of modifiable risk factors for CHD, most notably weight management, fat restriction, increased physical activity, treatment of hypertension, and smoking cessation.
Randomized, controlled studies have failed to support a protective role for HRT. This is in conflict with earlier observational studies, studies utilizing surrogate markers, and animal studies. The differences may be due to the unbiased sample of subjects taking HRT in these newer studies and, hence, may be a more realistic reflection of the impact of HRT on CVD. However, other potential confounders may be present, even in these studies, such as the menopausal stage when treatment was begun, the particular HRT regimen selected, and the individual risk factors of each subject (although the results may be more reasonably generalized, this may not accurately reflect clinician practice).
The first reported trial evaluated HRT for secondary prevention. The HERS trial evaluated daily HRT (0.625 mg conjugated estrogen + 2.5 mg MPA) in 2,763 postmenopausal women with a mean age of 66.7 years and documented preexisting vascular disease. The study failed to demonstrate any overall difference in subsequent vascular events. This occurred despite improvements in lipid parameters in those patients receiving HRT. Although some have questioned the negative impact of the progestin, in this trial, the Estrogen Replacement and Atherosclerosis (ERA) trial published in 2000, compared 3.2 years of treatment with estrogen, combined estrogen and progestin, and placebo. Study participants were postmenopausal women aged 42 to 80 years. This, again, was a secondary prevention trial and also failed to demonstrate a significant difference in the rate of progression of coronary atherosclerosis among the three groups. The importance of this study was the inclusion of an estrogen-only arm.
The WHI is the first large, randomized study to look at primary prevention. The same combined HRT regimen used in the HERS trial was evaluated. This study was stopped when interim analyses demonstrated an unacceptable risk profile for a drug in a prevention trial. There was an increase in the incidence in breast cancer (an increase of 8 cases per 10,000 women), with no cardiovascular protection (and potentially increased cardiovascular risk). There was an increase in the absolute number of blood clots, strokes, and CHD. The risk of stroke and clot continued for the 5 years of study, while most of the CHD was limited to the first year of treatment. Whether these finding were related to the intrinsic properties of HRT, the oral administration route, or the unique regimen tested is not clear. There were, however, documented decreases in the risk of fracture and colon cancer.
Management for cardiovascular risk for women should parallel that for men. In other words, lifestyle modifications should be made and antihypertensive therapy given as needed. If hyperlipidemia persists, statin therapy should be instituted. And, as above, β-blockers and aspirin should be given to prevent recurrent myocardial infarction. There is no evidence from well-designed prospective trials supporting a role for either ERT or HRT for the primary indication of cardiovascular protection.
HORMONE REPLACEMENT
Introduction
Approximately 38% of U.S. women aged 50 to 74 use HRT of some description. Of those surveyed, 59% of users had undergone a hysterectomy and 19.6% had a uterus. In 2000, Premarin (conjugated equine estrogen [CEE]) was the second most widely prescribed drug in the United States, accounting for 46 million prescriptions and over $1 billion in sales. Historically, patients desiring hormone treatment for menopausal symptoms were supplemented initially with unopposed estrogen, regardless of the presence of a uterus. This therapy was proven clearly to increase a woman's risk of endometrial cancer, which was eliminated with the addition of either cyclic or continuous low-dose progestin. Women who have undergone hysterectomy can, and should, be treated with estrogen alone.
According to the FDA, approved indications for ERT-HRT include treatment of menopausal symptoms (e.g., hot flashes and genital tract atrophy) and the prevention of osteoporosis. During the past 30 years, it has become popular to prescribe ERT-HRT to prevent a range of chronic diseases, most notably heart disease. As above, evidence has been accumulating which suggests that estrogen-progestin therapy for prevention of chronic diseases is not evidence based.
Benefits
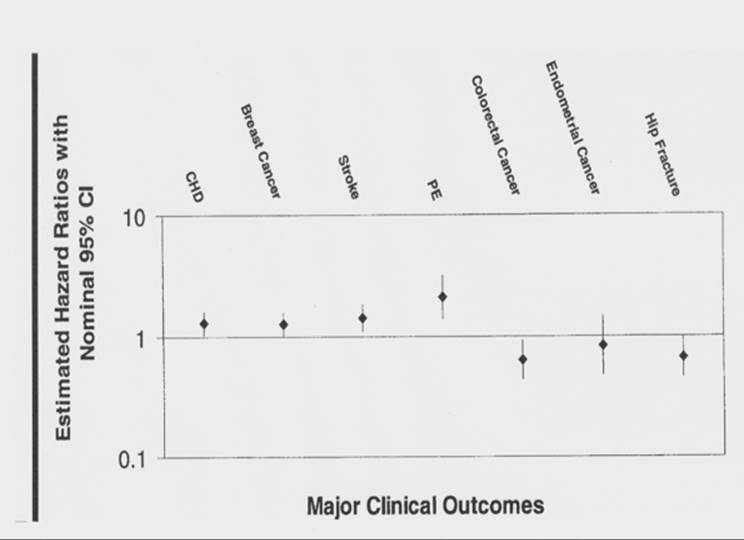
With the publication of the WHI data, HRT risks and benefits have been examined critically (Fig. 41.4). HRT benefits include reduction in hot flash frequency and severity, improvement of atrophic vaginitis and UTIs, and prevention of osteoporosis and fractures. Neither vasomotor symptoms nor vaginal atrophy were evaluated in the WHI, although likely occurrence was low, because the participants were asymptomatic and not taking HRT when enrolled. The WHI results did support an additional benefit of decreased risk of colorectal cancer.
|
|
|
FIG. 41.4. Estimated hazard ratios for major clinical outcomes in the Women's Health Initiative trial of hormone replacement therapy. CHD, coronary heart disease; PE, pulmonary embolism. (Source: Writing Group for the Women's Health Initiative investigators. From Grimes DA, Lobo RA. Perspectives on the Women's Health Initiative trial of hormone replacement therapy. Obstet Gynecol 2002;100:1344–1353, with permission.) |
A variety of areas have been studied in postmenopausal women, including estrogen effects on depression and Alzheimer disease (AD). The cognitive benefits of HRT remain more controversial than benefits in other areas. A meta-analysis from 1998 incorporating all studies published between 1966 and 1997 suggests several mechanisms by which estrogen may affect cognition, including maintenance of neural circuits, favorable lipoprotein changes, prevention of cerebral ischemia, and promotion of serotonergic and cholinergic activity in the brain. It is also possible that cognition improves in estrogen users during the menopausal transition because vasomotor symptoms improve, because there does not appear to be a clear benefit in asymptomatic women receiving HRT. The HERS data also support a cognitive benefit, concluding that the effects of HRT on emotional measures, of quality of life, depend on the presence of menopausal symptoms. The Seattle Midlife Women's Health Study showed that perceived memory functioning is more closely related to depressed mood, perceived stress, and perceived poor health than to age or reproductive stage.
AD is an enormous public health concern that intensifies as the population ages. In 1997, AD cases in the United States numbered 2.32 million, with 68% of individuals being female. In 1998, the annual number of new cases was 360,000. Interventions that could prevent this disease, or delay its onset, would have a major public health impact.
Women with high serum concentration of unbound (bioavailable) estradiol are less likely to develop cognitive impairment than women with low concentrations.
Randomized trials studying estrogen use and AD are limited but suggest that estrogen users have a reduced risk of developing AD. However, there is no therapeutic benefit of estrogen usage in women with preexisting AD. Larger randomized trials are needed to evaluate the true significance of estrogen use and dementia. The WHI includes a memory study, and these results should be available in 2005.
Risks
As more randomized trials of HRT are conducted, the risk profile has broadened. CHD was once a main off-label indication for HRT, and former guidelines from the American College of Physicians even suggested that HRT be considered for all women. The HERS trial and, more importantly, the WHI have shown that nonfatal cardiac events are increased in HRT users in the regimen tested. These studies have also reemphasized known risks of HRT including pulmonary embolus, stroke, deep vein thrombosis, and gallbladder disease.
CONTROVERSIES
Cardiovascular Disease
During the 1990s, HRT was prescribed increasingly to postmenopausal women for CHD prevention. Much of this enthusiasm was based on a meta-analysis published in 1992 that concluded that “there is extensive and consistent observational evidence that estrogen use reduces risks for CHD about 35%.” This same year, the American College of Physicians published guidelines recommending that all postmenopausal women should consider HRT. They emphasized that those who are at increased risk of CHD are especially likely to benefit. Further observational studies have supported this recommendation. For example, the Nurse's Health Study of 1996 confirmed a 40% to 60% reduction in cardiovascular events in women taking HRT.
The HERS was a randomized, blinded, secondary prevention, clinical trial with results published in 1998. The study population was 2,763 postmenopausal women with documented CHD. The average age was 67 and all women had a uterus. Subjects were randomly assigned to receive either 0.625 mg CEE with 2.5 mg MPA daily or placebo. The average follow-up was 4.1 years. The investigators found that the women assigned to receive CEE plus MPA had a 50% increased risk of coronary events during the first year of the trial compared with the placebo group. The risk was greatest during the first 4 months. The risk returned to baseline over the next 2 years and seemed to be lower in the hormone-treated group beginning in the third year of the study. The changes could have occurred by chance or may be due to detrimental effects of the hormone replacement, the specific regimen studied, or the procoagulant effect associated with oral administration. An initial prothrombogenic effect was thought to be the cause of early morbidity, and there was some expectation that longer treatment would document an improved outcome. However, HERS II, which continued to follow this group (6.8 years of follow-up), failed to see a developing protective effect of HRT.
The WHI is the first randomized, primary prevention trial studying the effects of a specific postmenopausal HRT regimen (the daily regimen of 0.625 mg CEE plus 2.5 mg MPA). In contrast to the HERS trial, these 50- to 79-year-old women were considered healthy, with only a small proportion (7.7%) of subjects having clinical signs or symptoms of CHD. The subjects were randomized to receive the HRT regimen or placebo if they had a uterus. Women without a uterus received either the estrogen alone or placebo. The planned duration of the trial was 8.5 years, but the estrogen-plus-progestin arm (16,608 women) was stopped after 5.2 years because of concerns regarding cardiovascular events and breast cancer. “The test statistic for invasive breast cancer exceeded the stopping boundary for this adverse effect and the global index statistic supported risks exceeding benefits.” Estimated HRs for diseases other than breast cancer, including CHD, were also significant. The HR results were as follows: CHD, 1.29 (95% CI = 1.02–1.63); breast cancer, 1.26 (1.00–1.59); stroke, 1.41 (1.07–1.85); pulmonary embolus (PE), 2.13 (1.39–3.25); endometrial cancer, 0.83 (0.47–1.47); colorectal cancer, 0.63 (0.43–0.92); hip fractures, 0.66 (0.45–0.98).
This important study suggests that breast cancer, nonfatal CHD events, stroke, and PE are all significantly increased in the overall cohort, of women 50 to 79 years old using combined estrogen and progestin therapy. It showed that colorectal cancer and hip fracture risk are reduced significantly in the same group. Ultimately, the data suggest that the use of this combined HRT regimen for primary prevention of CHD is not justified.
In 2001, the American Heart Association published guidelines regarding HRT and CVD. They have taken a cautious stance. These recommendations were made prior to the publication of the WHI results.
American Heart Association Recommendations
Secondary Prevention
· HRT should not be initiated for the secondary prevention of CVD.
· The decision to continue or stop HRT in women with CVD who have been undergoing long-term HRT should be based on established noncoronary benefits and risks and patient preference.
· If a woman develops an acute CVD event or is immobilized while undergoing HRT, it is prudent to consider thromboembolic prophylaxis while she is hospitalized to minimize risk of a venous thromoembolism associated with immobilization. Reinstitution of HRT should be based on established noncoronary benefits and risks, as well as patient preference.
Primary Prevention
· Firm clinical recommendations for primary prevention await the results of ongoing randomized clinical trials.
· There are insufficient data to suggest that HRT should be initiated for the sole purpose of primary prevention of CVD.
· Initiation and continuation of HRT should be based on established noncoronary benefits and risks, possible coronary benefits and risks, and patient preference.
There is still some question about whether WHI was really assessing “primary” prevention based on concern about the preexistence of atherosclerotic disease. Enrollees were asymptomatic and older (mean age, 63 years) than the typical HRT-ERT user. Some vascular biologists have suggested the early institution of HRT may inhibit the development of atherosclerotic plaque and that a delay in treatment for several years after menopause, after plaque formation is well established, would not only not offer benefit but might increase risk by destabilizing existing plaque, leading to plaque rupture and thrombosis. Although this thesis is consistent with animal studies, little human data are available to support or repute it. It is yet another consideration for patients and physicians in making this difficult decision.
Breast Cancer
A woman's lifetime risk of breast cancer is 1 in 8. There are 192,000 new cases of breast cancer per year, accounting for 41,000 deaths per year. It is the second leading cause of cancer death after lung cancer and the leading cause of death among women ages 40 to 55.
The most compelling reason to believe that long-term use of postmenopausal estrogen increases the risk of breast cancer is the inherent biologic plausibility. Many of the risk factors associated with breast cancer are thought to be linked to increased duration of exposure to estrogen over a woman's lifetime. These risk factors include early menarche, late menopause, nulliparity, and older age at the birth of her first child. Oophorectomy can induce breast tumor regression and early oophorectomy is protective against breast cancer, which seem to support further the notion that estrogen is involved, but this remains controversial. All of these risk factors take ovarian function into account, but not necessarily estrogen exposure, because the ovary is responsible for the formation of many other compounds which may influence the risk, such as androgens.
The association of estrogen therapy and breast cancer remains controversial, despite the publication of over 50 epidemiologic studies during the past 25 years. This subject is of great public health concern because of women's understandable fear of breast cancer and the complexity of the decision-making process regarding hormone therapy.
A reanalysis of the world's data on HRT-ERT and breast cancer was performed in 1997. A team of epidemiologists invited all investigators who had previously studied the association of postmenopausal hormone use and the risk of breast cancer (51 studies) to submit their original data for a collaborative combined reanalysis, an undertaking more rigorous than a standard meta-analysis (Collaborative Group of Hormonal Factors in Breast Cancer).
This analysis reached the following conclusions:
· Ever users of postmenopausal hormones had an overall increased relative risk of breast cancer of 1.14.
· Current users for 5 or more years had a relative risk of 1.35 (CI = 1.21–1.49), and the risk increased with increasing duration of use.
· Current and recent users had evidence of having only localized disease (no metastatic disease) and ever users had less metastatic disease.
· There was no effect of a family history of breast cancer.
· There was no increase in relative risk in past users.
· The increase in relative risk in current and recent users was greatest in women with lower body weights.
The WHI has brought even greater attention to any relationship between breast cancer and HRT use. The estrogen-progestin versus placebo arm of the study was stopped early, due primarily to an increase in breast cancer risk with a HR of 1.2. No similar effect was noted in the estrogen-only arm of the study, which is ongoing. Whether or not women in this category will also have an increased risk of breast cancer is unknown at this time. There is other epidemiologic evidence to suggest combined, continuous HRT may confer a higher risk of breast cancer than either cyclic estrogen-progestin regimens or those with estrogen only.
The comparison between the collaborative epidemiologic analysis described above and the WHI is interesting (relative risk, 1.35 vs. 1.26). Another relevant point the authors from the collaborative reanalysis make is that the quantitative effect of their conclusion is similar to the impact of raising the age of menopause. According to their calculations, current and recent hormone use was associated with a 2.3% increase in breast cancer risk per year, and the effect of age of menopause was equivalent to a 2.8% increase in risk per year of delay.
The presence of only localized disease, in the collaborative study, raises concern regarding screening bias and whether ERT-HRT treatment simply accelerated the detection of tumors already present. All of these studies that have examined the mortality rates of women who were taking estrogen at the time of breast cancer diagnosis have documented improved survival rates. This reflects earlier diagnosis in users, because the greater survival rate in current users is associated with a lower frequency of late-stage disease. There has been a suggestion that estrogen users develop better differentiated tumors and the surveillance-detection bias is not the only explanation for better survival. This suggests that hormone treatment accelerated the growth of a malignant locus already in place, which appears clinically at a less virulent and aggressive stage.
Selective Estrogen Receptor Modulators
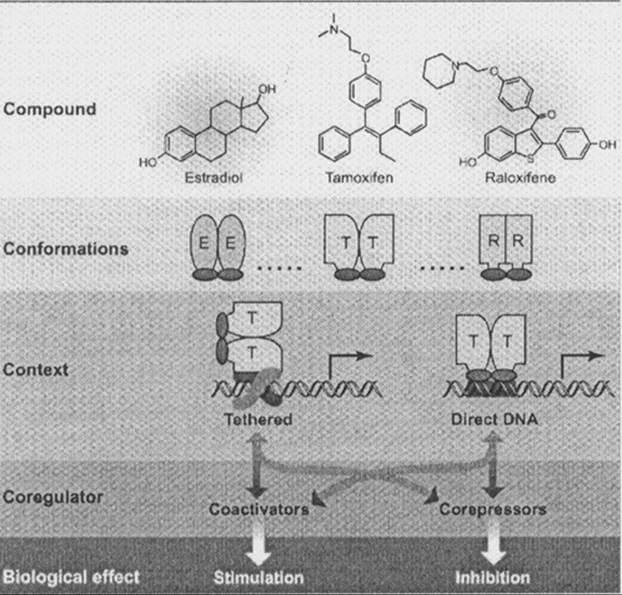
The controversy regarding HRT-ERT has heightened the call for alternatives. The term hormone-estrogen replacement implies the replacement of the beneficial aspects of premenopausal estrogen. SERMs make up a class of compounds that act like estrogen agonists on some tissues and estrogen antagonists on others. SERMs act by causing dimerization and conformational changes in the estrogen receptor, altering the interaction with the promoter regions on DNA. These conformational changes further impact function through their interactions with co-regulators and co-repressors. This is illustrated in cartoon form in Figure 41.5.
|
|
|
FIG. 41.5. Differential selective estrogen receptor modulator activity (stimulation and inhibition) is determined by the specific tissue, the endogenous milieu, and the impact of conformational changes on the interaction with regulatory sequences of DNA and co-regulatory proteins (co-activators and co-repressors). (From Katzenellenbogen BS, Katzenellenbogen JA. Defining the “S” in SERMs. Science 2002;295:2380–2381, with permission.) |
The search for the “ideal” SERM, with positive (estrogenic) effects on the heart, bone, and brain and negative (antiestrogenic) effects on the breast and uterus, continues. Improved scientific knowledge regarding estrogen receptor function (more like a rheostat than an “on-off” switch), two receptor types (α and β), more than 50 transcription factors, over 20 modifying proteins, and different response elements should enhance the development of therapeutic agents for selective clinical applications.
The beneficial aspects of raloxifene, the most studied SERM, with respect to osteoporosis, already have been discussed. There are evolving data with respect to CVD. Both raloxifene and tamoxifen decrease total cholesterol and low-density lipoprotein levels. Neither has an effect on high-density lipoprotein or triglyceride levels. Interestingly, raloxifene is either neutral or decreases two inflammatory markers (homocysteine and C-reactive protein), which might participate in the increase in cardiovascular events seen with the institution of HRT-ERT.
The available data about SERMs and CVD are, again, based on surrogate markers. A prospective study, Raloxifene Use in The Heart (RUTH), is ongoing. This study will evaluate 10,000 at-risk women and will add information to guide treatment strategies and, hopefully, increase our treatment options.
Limited data have suggested SERMs may have a beneficial effect on cognition. Although raloxifene is known not to improve (and potentially worsen) vasomotor symptoms, there is some preliminary evidence to suggest a neuroprotective effect. The extent and mechanism of this effect is not well characterized and awaits further study.
There is no doubt that the available SERMs are antiestrogenic at the breast. Tamoxifen is used primarily in the United States for cancer chemoprevention and treatment. Raloxifene also appears to decrease the incidence of estrogen receptor-positive cancer development. The Study of Tamoxifen and Raloxifene (STAR) should yield direct information regarding the benefit of raloxifene in women at risk for breast cancer as the available data are derived from osteoporosis trials. Lastly, it should be remembered that both tamoxifen and raloxifene increase the risk of thromboembolic phenomena, and this may have an impact on cardiovascular risk.
SUMMARY
The WHI did not address the effect of hormone treatment on hot flashes and vaginal atrophy. Clearly, there are alternatives for the treatment of osteoporosis and CVD that have less risk if CVD prevention is the sole reason for using HRT. Each woman should discuss with her health care provider the optimal treatment management to address her individual goals. This obviously would need to take into account medical and family history, as well as symptomatology.
If HRT-ERT is selected by the patient, progestin should be used only for those women with a uterus. Furthermore, in developing an overall treatment strategy, physicians should utilize the full armamentarium of medications (conjugated estrogens, estradiol, MPA, norethindrone, micronized progesterone, and androgens), routes of administration (oral, vaginal, transdermal), and cyclic patterns (continuous, intermittent, monthly, quarterly) available, including low-dose aspirin and statins. Duration of hormone therapy would also be an individual decision based on the original indication for treatment and its persistence. It can be recommended uniformly that menopausal women maintain appropriate nutrition, a healthy body weight, and regular exercise, including both weight-bearing aerobic exercise and muscle-strengthening exercise. This should be associated with moderation in alcohol intake and cessation of smoking.
SUMMARY POINTS
· Estrogen production in women is related to follicular maturation and the number of ovarian follicles is fixed, with declining numbers of follicles associated with hypoestrogenism.
· Declining ovarian estrogen production is associated with vasomotor instability, hot flashes, urogenital tract atrophy, and accelerated loss of BMD.
· Treatment of the symptoms associated with declining ovarian estrogen production is optimal with ERT in women without a uterus and estrogen with progestin regimens in women with a uterus.
· Although primary or secondary prevention of CVD has been suggested in observational studies, it has not been demonstrated in randomized treatment trials (HERS and WHI).
· A slight increase in the risk of breast cancer has been associated with HRT, albeit with a lower mortality likely secondary to earlier detection at a less aggressive stage of disease.
· Decisions regarding the use or ERT-HRT should be individualized, based on the woman's goals of therapy, and reevaluated periodically to ensure that the risk-benefit analysis continues to favor hormone use.
SUGGESTED READINGS
General
Chetkowski RJ, Meldrum DR, Steingold KA, et al. Biologic effects of transdermal estradiol. N Engl J Med 1986;314:1615–1620.
Faddy MJ, Gosden RG, Gougeon A, et al. Accelerated disappearance of ovarian follicles in mid-life: implications for forecasting menopause. Hum Reprod1992;7:1342–1346.
Soules MR, Sherman S, Parrott E, et al. Stages of Reproductive Aging Workshop (STRAW). J Womens Health Gend Based Med 2001;10:843–848.
Premature Ovarian Failure
Cramer DW, Xu H, Harlow BL. Does “incessant” ovulation increase risk for early menopause? Am J Obstet Gynecol 1995;172:568–573.
Mehta AE, Matwijiw I, Lyons EA, et al. Noninvasive diagnosis of resistant ovary syndrome by ultrasonography. Fertil Steril 1992;57:56–61.
Tibilietto MG, Testa G, Vegetti W, et al. The idiopathic forms of premature menopause and early menopause show the same genetic pattern. Hum Reprod1999;14:2731–2734.
Van Kasteren YM, Hundscheid RD, Smits AP, et al. Familial idiopathic premature ovarian failure: an overrated and underestimated genetic disease. Hum Reprod 1999;14:2455–2459.
Vasomotor symptoms
Berendsen HH. The role of serotonin in hot flushes. Maturitas 2000;36:155–164.
Shanafelt RD, Barton DL, Adjei AA, et al. Pathophysiology and treatment of hot flashes. Mayo Clin Proc 2002;77:1207–1218.
Weitzner MA, Moncello J, Jacobsen PB, et al. A pilot trial of paroxetine for the treatment of hot flashes and associated symptoms in women with breast cancer. J Pain Symptom Manage 2002;23:337–345.
Genitourinary Atrophy
Brown JS, Sawaya G, Thorn DH, et al. Hysterectomy and urinary incontinence: a systematic review. Lancet 2000;356:535–539.
Keil K. Urogenital atrophy: diagnosis, sequelae, and management. Curr Womens Health Rep 2002;2:305–311.
Sherburn M, Guthrie JR, Dudley EC, et al. Is incontinence associated with menopause? Obstet Gynecol 2001;98:628–633.
Willhite LA, O'Connell MB. Urogenital atrophy: prevention and treatment. Pharmacotherapy 2001;21:464–480.
Osteoporosis
Multiple authors. Meta-analyses of therapies for postmenopausal osteoporosis. Endocrine Rev 2002;23:495–578.
Cardiovascular Disease
Barrett-Conner E, Grady D, Sashegyi A. Raloxifene and cardiovascular events in osteoporotic postmenopausal women. JAMA 2002;287:847–857.
Grady D, Herrington D, Bittner V, et al. Cardiovascular disease outcomes during 6.8 years of hormone therapy: Heart and Estrogen/progestin Replacement Study follow-up (HERS II). JAMA 2002;288:49–57.
Herrington DM, Reboussin DM, Brosnihan KB, et al. Effects of estrogen replacement on the progression of coronary-artery atherosclerosis. N Engl J Med2000;343:522–529.
Hulley S, Grady D, Bush T. Randomized trial of estrogen plus progestin for secondary prevention of coronary heart disease in postmenopausal women. JAMA1998;280:605–613.
Mikkola TS, Clarkson TB. Estrogen replacement therapy, atherosclerosis, and vascular function. Cardiovasc Res 2002;53:605–619.
Postmenopausal hormone replacement therapy for primary prevention of chronic conditions: recommendations and rationale. Ann Intern Med2002;137:834–839.
Teede HJ. Hormone replacement therapy and the prevention of cardiovascular disease. Hum Reprod Update 2002;8:201–215.
Breast Cancer
Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormone replacement therapy: collaborative reanalysis of data from 51 epidemiological studies of 52,705 women with breast cancer and 108,411 women without breast cancer. Lancet 1997;350:1047–1059.
Cui Y, Whiteman MK, Flaws JA, et al. Body mass and stage of breast cancer at diagnosis. Int J Cancer 2002;98:279–283.
Cummings SR, Duong T, Kenyon E, et al. Serum estradiol level and risk of breast cancer during treatment with raloxifene. JAMA 2002;287:216–220.
Cummings SR, Eckert S, Krueger KA, et al. The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. JAMA 1999;281:2189–2197.
Ursin G, Tseng CC, Paganini-Hill A, et al. Does menopausal hormone replacement therapy interact with known factors to increase risk of breast cancer? J Clin Oncol 2002;20:699–706.
Cognitive Function
Fillit JM. The role of hormone replacement therapy in prevention of Alzheimer disease. Arch Intern Med 2002;162:1934–1942.
Yaffe K, Lui LY, Grady D, et al. Estrogen receptor 1 polymorphisms and risk of cognitive impairment in older women. Biol Psychiatry 2002;51:677–682.
Yaffe K, Sawaya G, Lieberburg I, et al. Estrogen therapy in postmenopausal women: effects on cognitive function and dementia. JAMA 1998;279:688–695.
Selective Estrogen Receptor Modulators
American College of Obstetricians and Gynecologists. Selective estrogen receptor modulators. ACOG Practice Bulletin No. 29, Oct 2002.
Katzenellenbogen BS, Katzenellenbogen JA. Defining the “S” in SERMs. Science 2002;295:2380–2381.
Morello KC, Wurz GT, DeGregorio MW. SERMs: current status and future trends. Crit Rev Oncol Hematol 2002;43:63–76.
Controversies
Grimes DA, Lobo RA. Perspectives on the Women's Health Initiative trial of hormone replacement therapy. Obstet Gynecol 2002;100:1344–1353.
McDonough PG. The randomized world is not without its imperfections: reflections on the Women's Health Initiative study. Fertil Steril 2002;78:951–956.
Writing group for the Women's Health Initiative investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women. JAMA2002;288:321–333.