Arthur F. Haney
Leiomyomata represent the most common gynecologic tumors and are responsible for approximately 300,000 hysterectomies per year. They can cause a variety of symptoms, including menometrorrhagia, dysmenorrhea, pelvic pain, infertility, preterm birth, and compression of adjacent pelvic viscera. Paradoxically, large subserosal leiomyomata may be totally asymptomatic. These tumors are often multiple, are almost always benign, and represent gonadal steroid–responsive aberrant clonal expansions of individual myometrial cells. Leiomyomata are more common in African-American women and have a nonmendelian inheritance pattern with up to a 50% recurrence rate after myomectomy. Treatment of patients with leiomyomata should be undertaken only to address a specific clinical problem and the therapy choice depends on the goal of therapy, with hysterectomy most often used for definitive management and myomectomy when preservation of childbearing potential is desired. Intracavitary and selected submucous leiomyomata can be removed by hysteroscopic resection and, although laparoscopic myomectomy is technically feasible, the risk of uterine rupture during subsequent pregnancy is potentially greater with the endoscopic removal of intramural leiomyomata. Although gonadotropin-releasing hormone (GnRH) agonist–induced hypogonadism can reduce the volume of leiomyomata by up to 50%, the severe side effects and prompt reenlargement after discontinuance make this approach useful only for short-term goals such as: (a) shrinking an intracavitary tumor prior to hysteroscopic resection, (b) preoperatively correcting anemia, or (c) reducing the overall size of the uterus to facilitate surgery. Nonextirpative approaches, such as myolysis and uterine artery embolization (UAE), are being evaluated and may prove useful options for carefully selected women if proven safe and efficacious in long-term follow-up studies. The impact of these nonextirpative options on fertility and pregnancy has not been determined. Ultimately, if the genetic basis for fibroid development or the molecular mechanism(s) of myometrial proliferation are better understood, additional nonsurgical therapeutic interventions may be forthcoming.
INTRODUCTION
Uterine leiomyomata are by far the most common benign tumors of the female genital tract and likely the most common soft tissue tumors of all. Approximately 300,000 hysterectomies and 20,000 myomectomies are performed annually in the United States because of symptoms caused by leiomyomata. These tumors can attain very large size with few if any symptoms and, alternatively, small leiomyomata may cause massive uterine bleeding, marked abdominal distension, and disabling dysmenorrhea. Although representing one of the most frequent indications for gynecologic surgery, the incidence of leiomyomata far exceeds the frequency of clinical problems, with estimates of as high as 50% of women having at least one identifiable fibroid at menopause. Understanding what is known regarding the pathophysiology, genetic risk predisposition, and natural history of leiomyomata is invaluable for the practicing clinician.
CLINICAL PICTURE
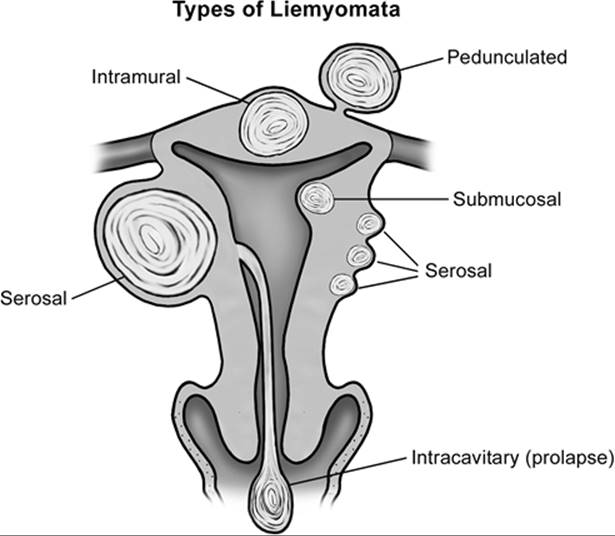
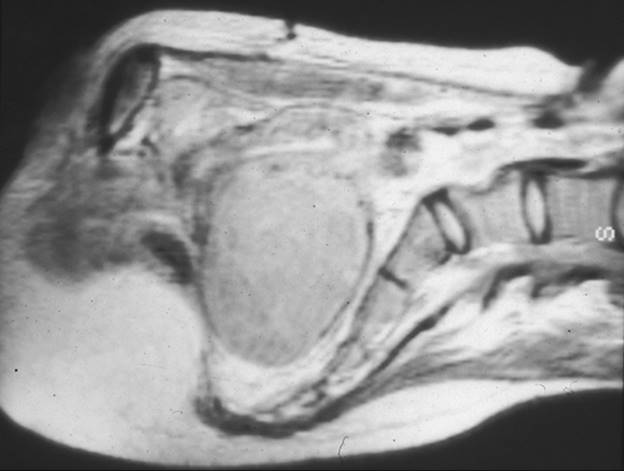
Leiomyomata come to clinical attention for a variety of reasons, and the symptoms (Table 49.1) depend upon tumor size and location (Fig. 49.1). It is unusual but not rare for fibroids to become symptomatic before a woman reaches age 30. Excessive menstrual bleeding (menorrhagia) leading to anemia, debilitating dysmenorrhea, generalized pelvic pain, or symptoms of pressure on the adjacent pelvic viscera my occur, but pain other than dysmenorrhea is typically a late symptom. Vaginal bleeding apart from the expected menses, despite being heavy, is not typically a sign of uterine fibroids and usually indicates an underlying endocrine abnormality such as anovulation. Furthermore, the typical scenario is not a sudden heavy bleeding episode, but rather a gradual increase in menstrual bleeding that parallels the growth of the fibroids. Leiomyomata occasionally undergo rapid enlargement during pregnancy with central avascular necrosis, the so-called red degeneration, resulting in extreme pain requiring hospitalization and narcotics. As the size and number of the leiomyoma increase, particularly with single large subserosal leiomyomata, the adjacent pelvic viscera may become compressed, resulting in urinary frequency, constipation and, occasionally, dyspareunia. Rarely, when the fibroids are large and fill the pelvis or grow laterally from the midportion of the uterine body, they can compress the ureters and cause hydronephrosis (Fig. 49.2). Intracavitary fibroids often are on a vascular pedicle and may be extruded through the cervix, appearing as a necrotic mass. Rarely, large uterine leiomyomata will become entrapped in the pelvis when the expanding tumors are juxtaposed against the promontory of the sacrum and cause the cervix to descend in the vagina and occasionally appear at the introitus. This is particularly true when a woman with large serosal leiomyomata conceives and the tumors, as well as the gravid uterus, enlarge rapidly and can become incarcerated in the pelvis. Although fibroids can be present and cause symptoms at any age after puberty, they typically do not become a clinical problem until the early to mid-30s. With a rising age at which women first attempt pregnancy, this increasingly represents a difficult management problem which did not exist a generation ago when simple hysterectomy was the frequent curative choice. Preserving reproductive potential while relieving symptoms is the challenge today, with the rising age at first pregnancy increasing the likelihood that leiomyomata will develop prior to completing childbearing.
|
|
|
TABLE 49.1. Symptoms of leiomyomata |
|
|
|
FIG. 49.1. Possible locations of leiomyomata. This schematic diagram illustrates the many locations at which leiomyomata may develop. Symptoms related to heavy vaginal bleeding generally are greater when the leiomyomata are in close proximity to the endometrial cavity, with serosal tumors that can attain large size with virtually no change in menstrual bleeding. Fibroids can develop anywhere in the uterus, with the cervix having proportionally fewer because of its lower complement of myometrial cells. |
|
|
|
FIG. 49.2. Magnetic resonance imaging of leiomyomata. This magnetic resonance image demonstrates a large leiomyoma arising from the posterior aspect of the uterus and filling the entire pelvis. It directly contacts the promontory of the sacrum. |
Anatomic Features
Leiomyomata represent benign sex steroid–responsive smooth uterine muscle tumors originating as clonal expansions of individual myometrial cells. The histology is virtually indistinguishable from normal myometrium, except for a circular whorling pattern with the cellularity and mitotic activity being highly variable. The number of mitoses per high-power field is usually low, and increased numbers are critical to the risk of malignancy. Assessing the number of mitoses is typically part of the pathologic evaluation when fibroids are removed. There are often interspersed areas of fibrosis and occasional calcification, especially after pregnancy-induced degeneration and in postmenopausal women. Leiomyomata typically grow in a spheric or nodular fashion with a relatively distinct demarcation from the surrounding normal myometrium, reflecting their clonal origin.
Leiomyomata can arise from anywhere in the myometrium (see Fig. 49.1) and may be single or multiple, with occasional women having very large numbers of fibroids. When the cell of origin is near the serosal surface, the path of least resistance to expansion is to bulge outward into the peritoneal cavity, termed a serosal or subserosal fibroid. Serosal tumors can grow very large without symptoms, because they virtually represent external appendages to the uterus. When a tumor is very superficial, this can result in a pedunculated fibroid, with a pedicle narrower than the tumor diameter containing the vascular supply. Occasionally, a pedunculated tumor will become detached from the uterus completely and derive its blood supply from an adjacent site. This is likely the result of pressure necrosis of the interface between the tumor and the adjacent viscera, or torsion of the pedicle and attachment at the new site during healing. When the myometrial cell of origin is deep within the myometrium, an intramural fibroid develops. These are associated more commonly with menorrhagia and dysmenorrhea, with the normal prostaglandin-mediated uterine contractions resulting in higher intrauterine pressures and failing to constrict the vessels feeding the endometrium during menses. If the myometrial cell of origin is near the endometrium, a submucosal tumor will develop and these are very likely to be associated with menorrhagia and dysmenorrhea, even at a relatively small size. When clonal expansion occurs in a cell immediately under the endometrial layer, the tumor may protrude into the endometrial cavity, and an intracavitary tumor on a pedicle may develop. Intracavitary tumors can cause severe symptoms despite their small size. With uterine contractions, the fibroid's stalk may elongate, extruding the fibroid through the cervix, typically associated with significant cramps and sanguineous vaginal discharge. Compression of the vascular pedicle may cause aseptic necrosis and the degenerating tumor becomes secondarily infected, making it appear similar to a necrotic cervical cancer. Although cervical fibroids can occur, they are infrequent, paralleling the small number of myometrial cells within the cervix. However, because of their proximity to the bladder, urinary symptoms typically can be very distressing.
There is virtually no neovascularity within fibroids, and individual leiomyomas derive their vascular supply from the vessels on the periphery of the tumor at the interface with the normally vascularized myometrium. Although fibroids are stimulated by sex steroids, the vascular supply is more likely to be the limiting factor for the growth of individual tumors. Often the uterine blood vessels are visibly enlarged because of the increased metabolic requirements of the uterus containing leiomyomata. However, the anatomic relationship of the vessels to the surrounding viscera is not altered, despite enlarged vascular pedicles. Collateral vascular channels are comparably engorged and represent a challenge to the surgeon if they are not considered in the surgical approach. Not surprisingly, this increased vascularity may increase the blood loss with any extirpative surgery, even if performed by the most experienced surgeon. When rapid fibroid growth does occur, such as is observed occasionally during pregnancy, the vascular demands of the tumor may exceed the capability of the vasculature. The leiomyoma then undergoes aseptic necrosis and, reflecting the peripheral nature of the vascular supply, the center of individual tumors undergoes degeneration with the outer layers relatively spared. This is initially described as red degeneration and later, as the devitalized central tissue is replaced by fibrosis, described as hyalinized degeneration, and ultimately may become calcified. It is not unusual to find marked calcium deposits in leiomyomata which have long ago undergone degeneration and were never symptomatic.
Influence of Sex Steroids
There is little doubt that the growth of leiomyomata is related to exposure to sex steroids, because they (a) are not noted prior to puberty, (b) typically regress after menopause, (c) possess sex steroid receptors (estrogen and progesterone), (d) often enlarge dramatically during pregnancy when estrogen and progesterone levels are very high, and (e) can be made to shrink with medically induced hypogonadism. Clearly, the uterus, like other secondary sex organs such as the breasts, enlarge with exposure to the higher levels of ovarian steroids produced at puberty. However, this growth is programmed and should cease once reaching the appropriate development, despite continued exposure to sex steroids throughout the reproductive lifespan.
There is no evidence that higher or aberrant patterns of ovarian steroid secretion of estrogens, progestins, or androgens contribute to the development of leiomyomata. However, myomatous tissue has the same number of estrogen receptors but a higher number of progesterone receptors than the adjacent normal myometrium. This, coupled with the observations that mitoses within myomas are more frequent in the luteal phase of the cycle and that progesterone up-regulates several growth factors, suggests that progesterone is causally involved somehow in either myomatous development or growth. Because estrogen stimulates the synthesis of progesterone receptors in other reproductive tissues, a more complex relationship among the two dominant female sex steroids and leiomyomata is likely present. Additionally, some data indicate that the development of fibroids may be related to postpubertal weight gain, which may relate to endogenous nonovarian estrogen production. Despite these observations, there is no consensus on the specific roles of the various sex steroids aside from a general positive relationship with development of leiomyomata.
Oral contraceptive use has not been associated with an increased incidence of leiomyomata or more rapid recurrence or progression. Treatment of postmenopausal women with hormonal replacement therapy occasionally, but not consistently, allows continued growth of existing leiomyomata. There is no evidence, however, that if leiomyomata are not present, they will develop in response to hormone replacement therapy after menopause. For clinical purposes, withholding hormone replacement therapy for fear of stimulating leiomyomata in otherwise appropriate candidates is not appropriate, given its well-documented benefits. Special note should be made of postmenopausal women with breast cancer treated with tamoxifen, because this compound has both estrogen agonist and antagonist activity, which has the potential to influence the pattern of fibroid growth. Undoubtedly, gonadal steroids are important in the development or growth of leiomyomata and, as more selective estrogen, progestin, and androgen response modulators become available for clinical use, their impact on the development or growth of leiomyomata will become apparent. Potentially, some of these agents will be found therapeutically useful.
GENETIC INHERITANCE PATTERN
It has been estimated that more than 40% of first-degree female relatives of women with leiomyomata will develop fibroids sometime during their lifetime. These will not necessarily be symptomatic, and the number and location are not predictable. Although leiomyomata are common in all races, African-Americans appear to have a somewhat higher incidence than women of other ethnicities, despite being a common disease in women of all ethnicities. African-American women undergoing hysterectomies have increased numbers of and larger fibroids, and it has been estimated that nearly 90% of uteri removed from these women for clinical symptoms contain leiomyomata. Regardless of ethnicity, leiomyomata are, by far, the commonest genital tract tumors and remain the most frequent indication for gynecologic surgery. This familial pattern seems most consistent with a multifactorial genetic inheritance pattern, rather than simple mendelian genetics, which is modified by confounding cofactors, such as the impact of gonadal steroids. Aside from the disease's apparent familial, age, and ethnic associations, there is little clinical predictability for an individual woman. Given the high prevalence of leiomyomata, virtually all women are at risk for developing them in their latter reproductive years.
Molecular Mechanisms and Genetic Dysregulation
Leiomyomas represent monoclonal neoplasms, in which etiologic genetic mutations in individual tumors are highly likely. Cytogenetic studies of individual leiomyomas reveal that approximately one third have some type of chromosomal aberration, but these are not consistent among individual leiomyomata, even among fibroids in the same woman, further supporting the clonal nature of leiomyomata. The most common aberrant patterns are translocations between chromosomes 12 and 14, deletions of the short arm of chromosome 7, and rearrangements of the long arm of chromosome 6. It is not clear whether there is real clinical relevance to these differences in the rate of tumor growth, recurrence rates, and responses to various therapies. Interestingly, when tumors have translocations between chromosomes 12 and 14, they are more likely to be larger myomas, whereas deletions of the long arm of chromosome 7 are found more often in smaller myomas. Although there are no consistent alterations in gene expression noted in leiomyomata, the transcription-factor high-motility group A2 is up-regulated in leiomyomata with expression of the 12;14 chromosome translocation. These observations imply that, despite similar histologic appearance and benign growth characteristics, there may be several molecular mechanisms by which these tumors develop, with correspondingly different clinical implications.
Undoubtedly, individual myometrial cells become neoplastic as a result of a complex interaction of factors including genetic mutations, endogenous sex steroid production–stimulating growth, reproductive patterns and, potentially, medicinal hormonal exposure after menopause. Molecular geneticists have noted abnormal expression of a variety of genes leading to altered growth factors and steroid receptors in individual leiomyomata, but there remains no single predominant molecular mechanism or group of mechanisms underlying their development and growth. Although this molecular dysregulation may explain the propensity to grow disproportionately to the normal pattern of myometrial growth throughout life, the molecular evidence does not suggest a progression from benign leiomyomata to leiomyosarcoma. Undoubtedly, the mechanism of clonal expansion of individual myometrial cells involves the interplay of gonadal steroids and aberrant expression of autocrine, paracrine, and endocrine growth factors. During the coming years, this molecular puzzle undoubtedly will be better understood but will just as likely prove to be very complex, without a single abnormality responsible for most leiomyomata. Clarifying the pathophysiologic mechanism(s) of growth of this most common of neoplasias should provide opportunities for better predicting the clinical course, genetic inheritance, as well as optimal prevention and therapeutic strategies for individual women.
Impact of Leiomyomata on Reproduction
The impact of leiomyomata on the ability to reproduce remains difficult to define in clinical terms useful for individual patients (Table 49.2). Clearly, the most logical approach for women with leiomyomata is to attempt to conceive and elect treatment only if they encounter difficulty. There is general agreement that intracavitary and submucosal leiomyomata are likely to cause infertility by preventing implantation, comparable to the effect of an intrauterine device. Fibroids within the endometrial cavity or impinging on the cavity contour can be detected by hysterosalpingography, sonohysterography, or hysteroscopy, and their removal can be expected to improve fertility. With intramural leiomyomata, a relationship to infertility is less certain and all other potential causes should be considered before concluding that the leiomyomata are causal. Intramural leiomyomata have been associated with a reduced pregnancy rate following assisted reproductive technology (in vitro fertilization and gamete intrafallopian transfer, known collectively as ART), indicating they may interfere with implantation. Given the time, expense, and complicated nature of ART, it is prudent to remove intramural fibroids in carefully selected infertile women before they undergo ART, when other therapeutic options have failed and no other cause is identified. Whether postoperative adhesions form after myomectomy is of lesser importance under these circumstances, because the oocytes will be retrieved transvaginally, regardless of whether adhesions involving the adnexae are present. The most important issue is that the couple be given the highest chance of success with ART, given the stress, expense, and time involved.
|
|
|
TABLE 49.2. Mechanisms of infertility with leiomyomata |
Although fibroids can be found anywhere in the myometrium, when they arise adjacent to the entry of the fallopian tubes into the uterus there is concern about occluding a tube or altering its function. This rarely occurs, likely due to the relatively slow growth of leiomyomata and the distensibility of soft tissues such as the fallopian tubes. However, because oocyte capture by the ciliated epithelium of the fimbria is necessary for fertilization, growth of fibroids near the distal end of the oviduct, which increases the distance between the surface of the ovary and the tubal ostia, theoretically can reduce the chance of conception. For this to be considered a problem, however, both fallopian tubes would need to be affected similarly. This is an infrequent circumstance, and a myomectomy should be performed to improve tubal function only when the uterine fibroids visibly distort the ovarian tubal anatomy bilaterally and after all other possible infertility factors have been excluded.
Whether leiomyomata are associated with a higher risk of first-trimester pregnancy loss, preterm labor, or intrauterine growth restriction is much more controversial. The impact of fibroids in each patient is critically dependent on location, not simply size or number. Clearly, many women with large myomatous uteri deliver infants without difficulty, while in others, fibroids may compromise the ability of the endometrial cavity to accommodate a growing fetus or the maternal vascular adaptation necessary for normal placental function. Complicating this picture is our inability to predict which women with leiomyomata will experience rapid enlargement of their fibroids during pregnancy. An abruption may occur rarely when the placental bed overlies an enlarging fibroid. Lower segment fibroids have the potential to obstruct labor, and a classic cesarean section occasionally is required when the presenting part cannot be applied directly to the cervix. If the leiomyomata are extremely large and intramural in location, preconception removal or other management of the fibroids may be considered, but the potential benefit must be weighed carefully against the complications of the procedure. There simply is no predicting which women will encounter problems and which will not. Clinical judgment will be sorely taxed to make correct decisions in the absence of a previous adverse clinical outcome. Overall, term delivery rates following myomectomy for symptomatic leiomyomata in an unselected patient population vary from 40% to 50%. The need to perform a cesarean section following myomectomy needs to be considered in any risk–benefit analysis.
LEIOMYOSARCOMA
Rarely, a leiomyosarcoma is encountered that is clinically indistinguishable from simple leiomyomata, but these are typically in older postmenopausal women, with the average age well over 60. The diagnosis often is suggested by enlargement of the uterus after menopause in the absence of any hormone replacement therapy. Uterine fibroids present prior to menopause may enlarge when the gonadal steroids are replaced, but this is not common and does not represent a frequent enough problem to preclude the use of any type of hormone replacement therapy. A leiomyosarcoma is not thought to develop from a preexisting leiomyoma, rather it arises de novo, with the factors leading to this rare cancer obscure. Rapid growth is not a very ominous sign of malignancy, because this is a common occurrence in women with leiomyomata before menopause. No physical findings or unique imaging differences can reliably distinguish leiomyomata from leiomyosarcoma. The diagnosis of a leiomyosarcoma typically is based on histology, not gross appearance. Degenerating leiomyomata may have unusual and varied features, including necrosis and central liquefaction. The histologic changes suggesting malignancy include increased numbers of mitoses, cellular pleomorphism, and thrombotic degeneration within the tumor. Many fibroids are very cellular but without other characteristics suggestive of malignant potential. Typically, more than 10 mitoses per high-power field suggests a risk that the tumor is malignant, between 5 and 10 represents a “cellular” or actively growing fibroid, and below 5 is usual for the typical myoma. Because of the difficulty accurately characterizing the number of mitoses by frozen section microscopy, the intraoperative diagnosis of a leiomyosarcoma is difficult to make with confidence and permanent sections usually are required. When a leiomyosarcoma is diagnosed following surgery, a second procedure for extirpation of any remaining pelvic organs and lymph node sampling for staging usually is required to plan optimal management. Leiomyosarcomas are estimated to account for 0.1% of all uterine tumors, but 1.7% of women undergo hysterectomy for leiomyomata during their seventh decade of life. For practical purposes, leiomyomata always should be considered benign in premenopausal women and rarely malignant in elderly women, but with the caveat that all excised specimens should undergo careful pathologic examination.
DIAGNOSTIC STUDIES
The vast majority of leiomyomata are detected on pelvic examination performed for routine health maintenance or because of a gynecologic symptom, such as increasing dysmenorrhea, menorrhagia, or pelvic pressure. The uterus typically is enlarged and irregular on bimanual examination. It is important to distinguish leiomyomata from other pelvic masses such as ovarian tumors. This is done most easily with an endovaginal or abdominal ultrasonographic examination, because the leiomyomata appear solid by sonography, with acoustic impedance similar to that of the normal myometrium. Other imaging techniques, such as computerized tomography or magnetic resonance imaging, can prove useful in selected circumstances (see Fig. 49.2, Table 49.3). Indeed, it must be appreciated that detecting an unrelated but clinically important adnexal mass may be difficult when there is a large leiomyoma. Unless the tumor has been stable on pelvic examination for many years in women in the latter reproductive years and beyond, some diagnostic imaging modality is warranted to ensure that the abnormal physical examination findings reflect leiomyomata and not another type of pathology with a greater potential for malignancy. Other imaging modalities, such as computerized tomography or magnetic resonance imaging, can distinguish leiomyomata from adnexal pathology, but they are much more expensive and time consuming and yield no more useful information than simple office sonography.
|
|
|
TABLE 49.3. Diagnostic techniques |
The proximity of the leiomyomata to the endometrial cavity usually can be demonstrated by taking advantage of the acoustic differences between normal myometrium, fibroid tumors, and the endometrial cavity. The endometrial stripe is a reliable marker of the endometrial cavity, and a smooth continuous endometrial stripe with normal underlying myometrium between the cavity and any fibroids suggests that palpably detectable fibroids are primarily in a subserosal location. Simultaneously injecting saline into the endometrial cavity while performing an endovaginal ultrasonographic examination (sonohysterography) improves the delineation of submucous and intracavitary leiomyomata. However, it is not possible to distinguish an endometrial polyp from an intracavitary myoma with any imaging technology.
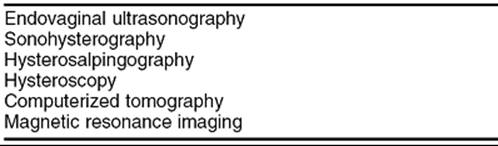
The closer the fibroid is to the endometrial cavity, the greater the likelihood and severity of dysmenorrhea and menorrhagia. Additionally, distortion of the endometrial cavity increases the probability of difficulty in achieving and maintaining a pregnancy. Hysterosalpingography often is undertaken if infertility is present concurrently, because this technique can identify intracavitary tumors or an otherwise normal endometrial cavity enlarged by stretching of the normal myometrium around leiomyomata (Fig. 49.3). This radiographic technique has the added advantage of determining tubal patency. Removal of leiomyomata will not improve the likelihood of conception unless an enlarged endometrial cavity, an irregular endometrial contour, or an intracavitary defect is present. Increasingly, office hysteroscopy is being used when tubal patency is not an issue, because this technique allows clear differentiation between leiomyomata and other intracavitary pathology, such as endometrial adhesions, uterine septae, and endometrial polyps.
|
|
|
FIG. 49.3. An intracavitary leiomyoma. A: A hysterosalpingogram using a water-soluble contrast medium demonstrates a large, smooth filling defect within the endometrial cavity resulting from an intracavitary fibroid. The mass effect on the study is nonspecific, and only direct visualization can confirm that it is caused by a fibroid. B: The hysteroscopic view of this intracavitary leiomyoma. |
Another disease involving the myometrium, adenomyosis, occasionally can be difficult to distinguish clinically from leiomyomata, and imaging studies may not be helpful. This disease process represents functional endometrial glands and stroma within myometrium, with these cells presumably infiltrating into the underlying myometrium from the endometrium. This is an infiltrative process, which is found immediately adjacent to the endometrial cavity and parallels the contours of the endometrial cavity. It is always continuous with the endometrium but not necessarily present in all subendometrial areas. Frequently, a marked fibrotic reaction is present around the isolated endometrial cells within the myometrium, presumably because of the irritation caused by menstrual shedding in the midst of the muscle. When the process is localized, these fibrotic areas may be difficult to distinguish on palpation from leiomyomata and the true diagnosis made only with surgery. Leiomyomata typically have a clear demarcation from the underlying myometrium, whereas a nodule of adenomyosis has a very indistinct infiltrating border which makes complete surgical removal virtually impossible. Adenomyosis tends to have more variability in shape, but the two pathologic entities occasionally may be indistinguishable by any of the available imaging techniques and the diagnosis made only after excision of the lesion. Magnetic resonance imaging is useful in differentiating adenomyosis from leiomyomata, because it better delineates the borders of the intramyometrial pathology; however, this is not used routinely preoperatively because of the expense involved. Like endometriosis, adenomyosis may be associated with an elevation in serum CA-125, but this is a nonspecific serum marker and cannot be used alone to diagnose adenomyosis.
Because most leiomyomata are identified only after symptoms are present and treatment carries considerable risk and expense, development of an inexpensive screening tool with reasonable sensitivity and specificity would be a major clinical advance. There are no laboratory markers which detect leiomyomata which are too small to cause symptoms or be palpated on pelvic examination. Detecting small leiomyomata in women with a familial risk would be very helpful, because it would assist in determining their true prevalence, better define the natural history, identify risk factors, and lead to earlier medical intervention, potentially reducing the need for surgical excision.
PREVENTING DEVELOPMENT, PROGRESSION, AND RECURRENCE
The ultimate goal of understanding the pathophysiology of leiomyomata is to prevent their occurrence in both genetically susceptible women and those without a family history. With further insight regarding the molecular mechanism(s) of growth, it may be possible to identify medicinal approaches to interfere with the molecular pathway(s) and reduce the risk of development, progression, and recurrence of leiomyomata. This will be particularly useful for women at risk of leiomyomata because of a strong family history, those with previous myomectomy, and women with leiomyomata approaching menopause who can anticipate spontaneous regression once ovarian function ceases. Additionally, understanding the impacts of childbearing, lactation, the various forms of steroidal contraception, and estrogen and hormone replacement therapy on the development, progression, and recurrence of leiomyomata should help optimize clinical recommendations. There are few, if any, predictors of the development of leiomyomata, aside from a family history. Endocrine markers such as early puberty, late menopause, parity, oral contraceptive use, and hormone replacement therapy of any kind are not correlated with either the development or the recurrence of fibroids after myomectomy.
TREATMENT
When to Treat
Although fibroids are responsible for a large number of gynecologic surgeries, management of these benign tumors requires the same risk–benefit analysis as any other therapeutic decision. Often, a prostaglandin synthetase inhibitor or oral contraceptives will relieve the symptoms. Although an increasing variety of options exist, it is important that the management be goal directed to alleviate specific symptoms. Simply identifying leiomyomata does not imply that they will continue to grow, become symptomatic, or require management. Occasionally, however, it may be appropriate to remove asymptomatic large leiomyomata in an effort to prevent anticipated problems before attempting pregnancy. Similarly, when a woman has intracavitary or large submucous myomas but has not attempted to conceive, it is likely, but not unequivocal, that removal of her fibroids will improve her chances. Removing myomas which cause significant distortion of the endometrial cavity in an infertile population will improve the likelihood of pregnancy and the maintenance of early pregnancy. Large tumors which fill the pelvis can impinge on the pelvic sidewalls, causing hydronephrosis, and their removal is critical. However, therapeutic intervention generally should be focused on the alleviation of symptoms, and observation is all that is necessary in the vast majority of asymptomatic women.
The growth characteristics of individual leiomyomata remain highly unpredictable, because many leiomyomata have limited growth potential and, thus, may remain static in size until the sex steroid levels decline at menopause, when they shrink. Paradoxically, some leiomyomas have already undergone rapid growth, aseptic necrosis, or replacement by fibrosis without symptoms and will not shrink after menopause. Although many fibroids may enlarge gradually, causing symptoms well before the anticipated regression at menopause, the growth pattern is so varied that there are simply no predictive characteristics helpful in identifying which women will need intervention and which will not.
The symptoms caused by leiomyomata vary, depending on the size, number, and location of the tumors, and can include dysmenorrhea, menorrhagia, increased abdominal girth, pelvic pressure (frequent urination or constipation), and pelvic pain with physical activity or intercourse. Dysmenorrhea and menorrhagia are more frequently linked than other symptoms. When the dysmenorrhea or menorrhagia is mild, nonsteroidal antiinflammatory agents and oral contraceptives are often useful, and the symptoms may improve sufficiently to avoid further intervention. In most cases, a therapeutic medical trial is indicated before proceeding to more aggressive medical or surgical options. When dysmenorrhea and menorrhagia are caused by leiomyomata, they are typically of secondary onset and worsen gradually in severity paralleling the enlargement of the tumors.
Location of the fibroids is critically important; the closer they are to the endometrial cavity, the greater and earlier the symptoms. Intramural, submucosal, and intracavitary fibroids are far more likely to cause dysmenorrhea and menorrhagia than intramural or subserosal myomas. Severe symptoms may warrant intervention at a relatively small size, particularly for an intracavitary or submucosal fibroid. Typically, the closer to the serosal surface the fibroids are located, the larger the size will be attained before symptoms occur. Indeed, some extremely large leiomyomata will not be associated with any symptoms aside from increased abdominal girth. This explains why many patients with extremely large leiomyomata are either minimally symptomatic or asymptomatic, while those with small submucosal or intracavitary fibroids may have dramatic bleeding and pain. Because of the proximity of the bladder, the most frequent symptom associated with a large subserosal or pedunculated myoma is frequent urination, comparable to what women experience during pregnancy. Rarely, compression of the colon against the sacrum may cause difficulty with defecation, although this is infrequent and, more often than not, feelings of constipation are not relieved completely by removing or shrinking the leiomyomata. As the tumors enlarge, these pressure symptoms intensify and ultimately may require medical or surgical intervention.
Selecting the Appropriate Therapy
When clear indications for therapy are present, the most critical questions which must precede a decision are as follows: (a) Is future reproduction is desired? and (b) How soon can menopause be anticipated? Because a simple hysterectomy represents a definitive cure, this is an attractive option for many symptomatic women when maintenance of reproduction is not desired, menopause is not imminent, and more conservative measures have failed to alleviate the symptoms (Fig. 49.4). This also requires an assessment of the woman's individual preferences, as well as her surgical and anesthetic risks. Clearly, women view extirpation of the uterus in their own social, cultural, and religious contexts, and removal of any genital structure cannot be viewed as inconsequential, even if there is no wish to preserve reproductive capacity. As a result, many women wish to preserve the uterus independent of reproduction, and they should be provided with all the therapeutic options and their choices respected. When the preservation of reproductive capacity is desired, a myomectomy is the primary choice. However, because the recurrence risk of symptomatic leiomyomata is high, myomectomy should be viewed as providing a disease-free interval and the women encouraged to attempt to reproduce as soon as is reasonable. As a result, many women without reproductive desires are interested in other, less well-established options such as UAE or myolysis, which may reduce the symptoms and retain the uterus.
|
|
|
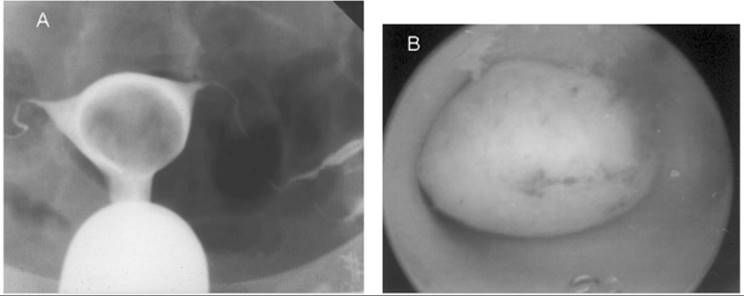
FIG. 49.4. Submucous leiomyoma. A: A submucous fibroid visualized at hysteroscopy is from a woman with a history of menometrorrhagia unresponsive to medical management with NSAIDs and oral contraceptives. Although the tumor protrudes into the endometrial cavity, most of it is still within the underlying myometrium. B: The hysterectomy specimen which demonstrates the submucous myoma responsible for the excessive vaginal bleeding. |
Extirpative Surgery for Leiomyomata
The mainstay of management for symptomatic leiomyomata is surgical, either hysterectomy or myomectomy, depending on the woman's desires regarding childbearing (Table 49.4). Given the risks inherent with all surgical procedures, the decision to proceed with any surgery should be based on a personalized clinical risk–benefit assessment, with the pivotal issue being future reproduction. Virtually no woman with leiomyomata need be faced with the painful choice of having to endure the symptoms in order to maintain reproductive potential versus relieving symptoms at the price of terminating reproductive options. A myomectomy is virtually always an option, even if a large number of fibroids are present or the tumors are very large or both. The uterus functions well in pregnancy after a myomectomy, despite the impact of multiple incisions. Although improvements in surgical technique, particularly minimally invasive surgery, have the potential to improve the benefits for women with symptomatic leiomyomata, comparative clinical trials of the various surgical approaches are urgently needed.
|
|
|
TABLE 49.4. Extirpative options |
Hysterectomy
When childbearing is not desired and the symptoms are severe enough to warrant treatment, a simple hysterectomy often is chosen, because it relieves the symptoms permanently, prevents recurrence, provides permanent contraception, and improves the quality of life as measured by questionnaires, presumably by eliminating further vaginal bleeding. An infrequently considered and poorly appreciated additional benefit is making hormone replacement therapy after menopause much simpler, with estrogen replacement without progestin the favored option. The decision to proceed with removal of the uterus should be based on a risk–benefit decision weighing the severity of the symptoms with the personalized surgical risk, and not on a concern that the leiomyomata might be malignant. The surgical approach, either abdominal or vaginal, should be individualized, based on the size and location of the fibroids, the degree of uterine descensus, the woman's habitus, and whether or not an oophorectomy is being considered or other pathology is present. The available techniques are an abdominal hysterectomy, vaginal hysterectomy, or a laparoscopically assisted hysterectomy.
Preservation of the cervix in appropriately selected women is an increasingly popular option. The myometrium is the portion of the uterus at risk for growth of leiomyomata and, because the cervix is composed primarily of fibrous tissue, the potential for the development of leiomyomata in a retained cervix is extremely low. The structural ligamentous support for the cervix and vaginal apex remains intact when the cervix is retained with, at least theoretically, lower rates of vaginal prolapse. Additionally, a major portion of the surgical morbidity associated with hysterectomy by any technique relates to the surgical dissection necessary for removal of the cervix. This morbidity is avoided when choosing a supracervical hysterectomy, without risk of recurrence or the need to add a progestin to a hormone replacement regimen. The risk of subsequent cervical dysplasia is very low in this age group, and it is managed easily on an outpatient basis if it occurs, with the same methods used if the fundus is still in place. However, when choosing to retain the cervix, the continued need for screening cervical cytology should be emphasized.
The risks of complications with a hysterectomy are significant and, when prospectively documented, are approximately 17% with abdominal hysterectomy, 23% for vaginal hysterectomy, and 19% for laparoscopically assisted hysterectomy. The risk of complications is apparently higher when the hysterectomy is done for fibroids. The complications include the usual problems associated with abdominal operations but, specifically, hemorrhage and injuries to the bladder and ureters. The risk of ureteral injury is 7 times greater with the vaginal approach, likely secondary to the limitations in visualization of the anatomy when operating through the vagina. Despite these concerns, hysterectomy is associated with a high level of patient satisfaction, even if there are surgical complications.
Hysteroscopic Myomectomy
With improvements in endoscopic surgical technology, most intracavitary and a substantial number of submucous leiomyomata can be resected via surgical hysteroscopy in an ambulatory setting. If the tumor protrudes completely into the endometrial cavity via a stalk, such as a completely intracavitary myoma, a hysteroscopic resection is by far the most cost-effective method of removal. This does require an experienced hysteroscopic surgeon and should not be attempted unless the requisite skill is available. When a submucosal leiomyoma is predominately within the endometrial cavity, most are similarly amenable to removal via hysteroscopic resection. However, if despite protruding into the endometrial cavity, the bulk of the tumor is still contained within the underlying myometrium, a hysteroscopic approach will likely not prove successful and, indeed, can prove hazardous if the surgeon does not recognize the depth of the myoma. In this circumstance, extreme caution should be exercised when resecting a submucous fibroid, and resorting to an abdominal procedure should not be perceived as a failure but rather should be considered the safest option.
A hysteroscopic myomectomy typically is performed using a hysteroscopic resectoscope comparable to that used for transurethral prostate resection. It is inserted through the cervix, the endometrial cavity distended with a nonconductive media, and the leiomyoma resected by electrical loop excision. The fragments are removed with the effluent of the distending media through an inflow–outflow system. Careful preoperative selection of patients is required to ensure safe, effective removal in an ambulatory setting. Preoperative shrinkage of the leiomyoma with a gonadotropin hormone–releasing hormone agonist often may be helpful and affords a reduction in the height of the surrounding endometrium. Preoperative atrophy of the endometrium, to provide a clear operative field without resorting to complete pituitary down-regulation, can be accomplished with a 10-day preoperative course of a progestin (20 mg/day of medroxyprogesterone acetate) or an androgen (danazol 800 mg/day). Care must also be taken to avoid excessive intravascular absorption of the distending medium, which can result in fluid overload, electrolyte imbalance, or a bleeding diathesis, depending upon the type of medium.
Abdominal Myomectomy
When symptomatic leiomyomata are not completely within the endometrial cavity but in an intramural location, an abdominal surgical approach usually is required. With infrequent exceptions, a low transverse incision yields adequate surgical exposure. Rarely, a vaginal myomectomy can be performed with proper patient selection, but this clinical situation is rare and requires a high degree of surgical skill. The goal of a myomectomy is to remove all the identifiable leiomyomata with the least possible alteration of the reproductive tract. There are numerous surgical techniques but, in general, the myometrium is incised, the myoma dissected from the surrounding myometrium, and the incision closed in layers with absorbable suture to ensure hemostasis and myometrial integrity (Fig. 49.5). Entry into the endometrial cavity is not associated with any significant morbidity, but it is essential not to place sutures though the endometrial cavity wall as if it is a layer to close. Because the distance to the opposite endometrial surface is small, approximating the myometrium underlying the endometrium to the corresponding opposite side is all that is necessary. Cervical fibroids can represent a significant surgical challenge because of their proximity to the bladder and ureters, as well as the difficulty attaining hemostasis. Similarly, parasitic fibroids can be difficult to remove depending on their vascular supply (Fig. 49.6).
|
|
|
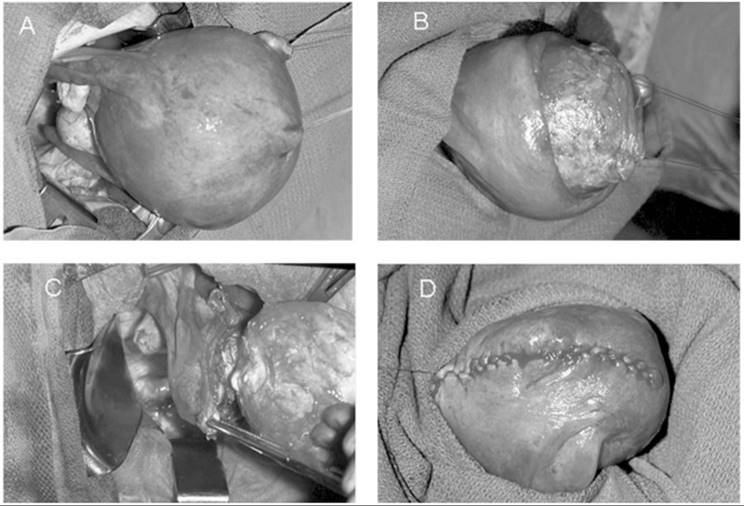
FIG. 49.5. Myomectomy. A: Surgical exposure of a large uterus containing an intramural leiomyoma is depicted. The fibroid is dissected from the underlying myometrium in (B). C: The uterine incision is extended down into the cavity and the fibroid is removed. The myometrium is reapproximated in layers (D) and the uterine muscle wall closed. |
|
|
|
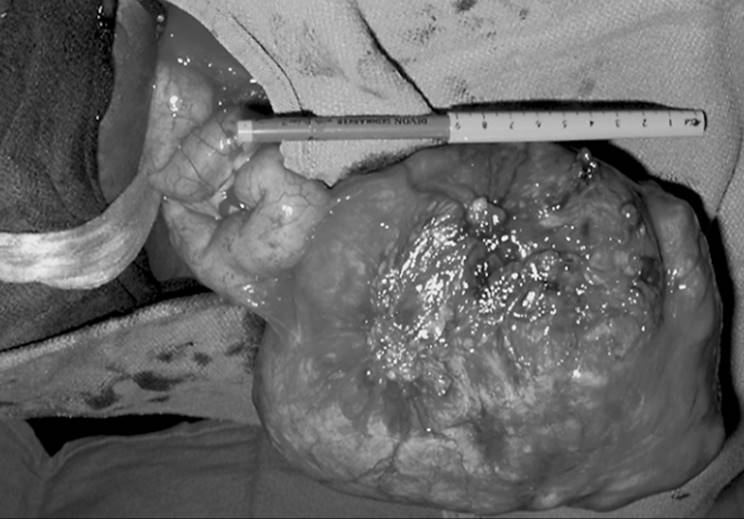
FIG. 49.6. A parasitic fibroid. A large tumor has become parasitic to a loop of small bowel, deriving its blood supply from the new vascular source. This typically happens only with large posterior or fundal tumors and is more common when they are pedunculated. The mechanism is felt to be pressure necrosis and revascularization during healing of the necrosis of the bowel wall. |
Because myometrium is extremely well supplied with vasculature, significant intraoperative blood loss is encountered frequently. Myomectomy at the time of an operative delivery is particularly hazardous because of the increased vascularity of the myometrium associated with pregnancy. Careful surgical technique, applying a tourniquet around the lower uterine segment to compress the uterine arteries, intramyometrial injection of vasospastic agents such as vasopressin, and employing an intraoperative blood scavenger system can reduce the net blood loss. These steps, coupled with the preoperative correction of anemia, storage of autologous blood, and mild overhydration to reduce the amount of red blood cell loss per unit of blood lost, have reduced dramatically the need for homologous transfusion. Rarely, if ever, is a hysterectomy necessary because of intraoperative blood loss when a myomectomy is undertaken. Caution should be exercised when using the injection of intramyometrial vasopressin, because uterine incisional bleeding after the metabolism of the vasopressin may result in unappreciated blood loss which, even if it does not put the patient at a hemodynamic risk, increases the time required for resolution of the postoperative anemia and may complicate efforts to reduce adhesion formation. During the immediate postoperative interval, it is common that women with multiple uterine incisions experience febrile morbidity unrelated to any demonstrable infection. Whether this is related to a tissue reaction from the relatively large surgical area of the uterine incision(s) or a response to hemorrhage within the myometrium is not clear, but it is a benign occurrence, and antibiotic therapy should be reserved for women with clinical findings suggesting infection.
Once the myometrium has sustained a surgical incision involving a significant portion of the uterine wall, an elective cesarean section generally is recommended as the route of delivery. When a myomectomy incision is repaired properly, the likelihood of a dehiscence during pregnancy is very remote, estimated to be approximately 0.002%. The incisions required for myomectomy are not similar to the low transverse uterine incisions used for most cesarean sections; rather, it is more comparable to the fundal incision used in a classic cesarean section. Furthermore, the endometrial cavity does not need to be entered for there to be concern regarding the integrity of the uterine wall during labor. Following a myomectomy, the couple should wait 2 to 3 months before attempting pregnancy, to allow complete healing of the uterine incisions and to minimize the potential for myometrial scar disruption before labor. This recommendation is based on the clinical experience with the rate of dehiscence of classic cesarean section scars which involve the contractile part of the uterus. Because the myomectomy incision is comparable in location, it has an impaired ability to withstand the force of a prolonged labor without rupture, a catastrophic occurrence for both the mother and fetus. The selection of women for an operative delivery should be based on the depth and extent of the myomectomy incision and the adequacy of the incisional repair, because the risk of uterine rupture is not well defined in the modern era but appears to be lower than when a cesarean section has been performed. Further data regarding circumstances following an abdominal myomectomy under which a vaginal delivery does not represent an increased the risk to the mother and fetus will likely not be forthcoming. As a result, an elective cesarean section is usually the preferred route of delivery for most women with a previous abdominal myomectomy.
Laparoscopic Myomectomy
Improvements in endoscopic surgery allow myomectomy to be accomplished via the laparoscope. It is clear that pedunculated, serosal, and superficial intramural leiomyomas can be removed via laparoscopy, but the surgery is lengthy, technically difficult, and should be undertaken by only the most experienced endoscopic surgeons. Furthermore, because only clearly obvious leiomyomata can be removed via laparoscopy, this therapy should be undertaken only when removal of a specific tumor can be anticipated to relieve the symptoms. Many smaller intramural fibroids will not be identified by this technique, so it is anticipated that a higher rate of subsequent symptomatic leiomyomata can be anticipated. Endoscopic closure of the uterine incisions is also technically difficult, and there have been several reports of spontaneous uterine rupture after laparoscopic myomectomy. This is additionally disconcerting, because this may occur during pregnancy prior to the onset of labor, as early as 33 weeks of gestation. This is distinct from that observed with abdominal myomectomy, when the risk of uterine rupture is felt to be limited primarily to the labor process. This suggests that even with careful attention to incision closure by skilled endoscopic surgeons, uterine rupture should be major risk factor considered in choosing the endoscopic approach. In the absence of long-term safety studies, selection of laparoscopic myomectomy for patients desirous of pregnancy should be done very carefully. By contrast, when the symptoms can be attributed to an isolated fibroid in a woman not desirous of childbearing, a laparoscopic myomectomy performed by an experienced surgeon can be a reasonable option.
Recurrence of Leiomyomata Following Myomectomy
There appears to be a genetic basis for the development of leiomyomata. Even when all of the palpable leiomyomata have been removed by myomectomy, the rate of recurrence and persistence with continued growth has been variably reported as high as 30%, depending on the number of tumors present and the length of follow-up. Indeed, between 10% and 25% of women undergoing myomectomies require another surgical procedure within the next decade. There is a suggestion that a delivery after a myomectomy may reduce the likelihood of recurrence, but this has a relatively small impact. Virtually all the data regarding recurrence or, more properly termed, development of new leiomyomata has been derived from women undergoing myomectomy with all the palpable fibroids removed. Obviously, small tumors may remain, and this will be impossible to separate from new clonal expansion of isolated myometrial cells or from persistence of small nonpalpable tumors not identified during surgery.
Some women who have symptoms but lack absolute evidence of existence of fibroids have undergone one of the newer nonextirpative therapies such as myolysis or UAE. The “recurrence” of fibroids has not been assessed in these women. Obviously, if leiomyomata are felt responsible for symptoms following a therapeutic procedure during which they are not removed, it will be impossible to distinguish persistence from the development of entirely new fibroids. It may be more appropriate to consider the frequency and time to recurrence of symptoms rather than simply when and at what interval fibroids are again present. If the newer techniques are applied mainly to women close to menopause, this may be a nonissue considering the natural loss of the stimulation by gonadal hormones. However, if younger women elect the nonextirpative therapies, only long-term comparative trials will yield useful discriminating information. Given the climate favoring broader nonextirpative options, such studies are needed urgently to assist women with therapeutic decision making.
In general, the size, location, or histologic pattern of the myomas have limited predictive ability for recurrence rates. The size of individual myomas may be of greater predictive value, because it appears that extremely large fibroids have a lower recurrence rate after myomectomy than do smaller tumors, despite an overall smaller volume of leiomyomata. It is not clear if the cytogenetic abnormalities have any predictive value for recurrence. The number of leiomyomata may be important in predicting recurrence, with women having single large tumors less likely to have subsequent fibroids detected than women with multiple, particularly smaller diameter, fibroids (Fig. 49.7).
|
|
|
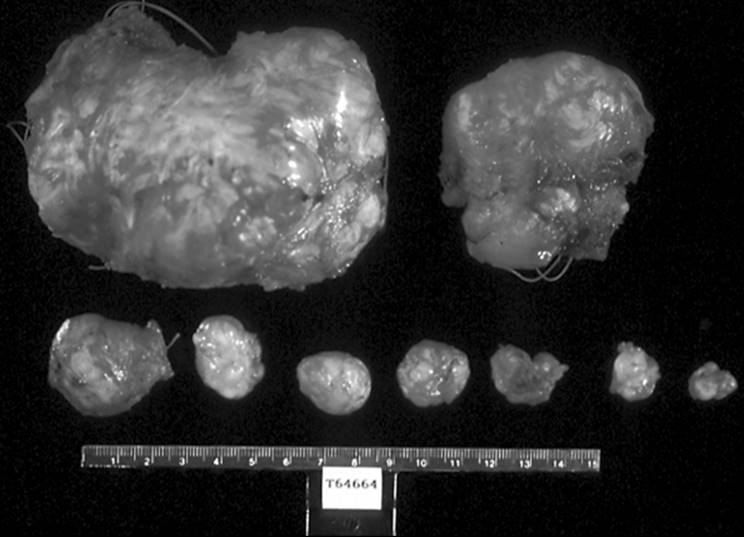
FIG. 49.7. Multiple leiomyomata excised at myomectomy. Many individual fibroids of different sizes and shapes can be encountered within the same patient. Some are very large and obvious, while others may be small and difficult to palpate. |
The time of follow-up affects the risk of a clinical recurrence, with the longer the interval of observation correlated with the greater the apparent recurrence risk. It is no surprise that the younger the woman is when fibroids are detected, the greater the likelihood of recurrence after myomectomy. When leiomyomata do recur, it is typically 3 to 5 years following the myomectomy, giving most women an opportunity to reproduce before fibroids are again present. When fibroids are noted in a shorter time frame, it is more likely that not all the myomas were removed. Although too few endoscopic myomectomies are available to reach a meaningful conclusion, it can be anticipated that higher recurrence rates will be observed, because it is difficult to identify all the tumors present without direct palpation of the uterus. Similarly, when a GnRH agonist is used preoperatively, the leiomyomata usually shrink and some smaller tumors might become too small to be detected at surgery, only to reemerge as symptomatic or palpable fibroids relatively quickly. As with the myolysis procedures, these “recurrences” may simply represent the persistence of tumors. Many small leiomyomata with the potential to enlarge simply will not be identified visually because they are intramural and deep within the myometrium. Undoubtedly, the technical skill to remove all the leiomyomata by any procedure is critically important and will influence the rate of apparent persistence or recurrence.
The methodology used to identify recurrent myomas will undoubtedly influence the recurrence rates. If clinical symptoms lead to evaluation, palpation will detect a larger tumor than will routine surveillance by transvaginal ultrasonographic examination. Other imaging techniques such as magnetic resonance imaging or computerized tomography, although rarely used for routine monitoring, would probably detect small fibroids before clinical symptoms develop and thus influence the apparent recurrence rate. If a clinically significant recurrence does occur, the typical time frame for the return of symptomatic fibroids after abdominal myomectomy is 3 to 5 years. Women with a single large leiomyoma appear to have lower recurrence rates than those with multiple intramural tumors. Women clearly should be counseled that when all the palpable myomas are removed during abdominal myomectomy, an interval free of symptoms and the opportunity to reproduce is provided, but it does not “cure” an inherited predisposition to the their development. No long-term data are available regarding the recurrence or persistence risks with experimental myolysis procedures or UAE, but when such data are available, clinical decision making will need to incorporate these findings.
Postoperative Pelvic Adhesions
A major complication of any myomectomy is postoperative adhesions. These can involve viscera adherent to the uterine incision sites, as well as de novo adhesions at nonsurgical sites, generally attributable to the unavoidable peritoneal trauma associated with surgery. The frequency of postoperative adhesions following myomectomy exceeds 50% and can result in reduced fertility, pain, or bowel obstruction. Interestingly, endoscopic surgery has not reduced the rate of postoperative adhesions at the site of the surgery, but it does appear to reduce the de novo adhesion rate. Careful surgical technique to minimize the degree of surgical trauma, confining the incisions to the anterior uterine surface so as to prevent contact with the bowel and adnexal structures, and covering the posterior uterine incisions with surgical barriers have been advocated to minimize the rate of postoperative adhesions. The materials used as adhesion prevention barriers are quite varied and include oxidized regenerated cellulose that is degraded by leukocytes; polytetrafluoroethylene, a nonreactive permanent material which is typically removed several weeks following surgery after the peritoneum has reconstituted itself (Fig. 49.8); and a hydrolyzable barrier composed of a combination of hyaluronic acid and carboxymethylcellulose. All of these materials have their advantages and disadvantages, and few comparative studies are available. In the only direct comparative study, fewer postoperative adhesions were associated with the use of the barrier composed of polytetrafluoroethylene versus oxidized regenerated cellulose. Improvements in surgical barrier technology, other systemic or intraperitoneal medicaments, and alternative surgical strategies will undoubtedly be forthcoming to help reduce the rate of postoperative adhesions.
|
|
|
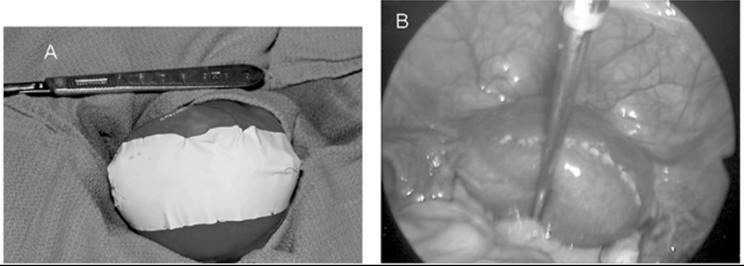
FIG. 49.8. Placement of a barrier of polytetrafluoroethylene at the time of myomectomy. To reduce the risk of adhesion formation between the visceral peritoneum of the uterus and the tubes and ovaries, a permanent barrier composed of polytetrafluoroethylene is anchored over the uterine incision with permanent sutures (A). The barrier is removed several weeks later via laparoscopy. B: The appearance of the uterine incision a year after the barrier was retrieved at a laparoscopy done for unrelated reasons. Note the healed uterine incision does not have any adhesion and represents an optimal surgical result. |
Nonextirpative Management of Leiomyomata
When removing fibroids is not appropriate, either because of patient choice or when confounding medical problems exist, a nonextirpative approach should be taken. A variety of options exist (Table 49.5) including medical suppression, in situ destruction of the myomas, or depriving them of their vascular supply. These approaches all suffer because long-term data are lacking and because the fibroids themselves, although regressed, are not removed. However, with the onset of menopause, the tumors can be anticipated to regress spontaneously, so a temporizing measure may suffice to relieve symptoms permanently.
|
|
|
TABLE 49.5. Nonextirpative options |
Medical Suppression
Many medicinal agents have been considered for the management of leiomyomata including estrogen antagonists, progesterone antagonists (RU-486), androgens (danazol), and pituitary down-regulation with GnRH agonists. However, only suppressing ovarian steroid production and creating a state of hypogonadism with GnRH agonists has been demonstrated to reduce the size of leiomyomata and relieve symptoms to such a degree as to be clinically useful. Although the volume of the leiomyomata typically decreases by 35% to 50%, this is somewhat misleading. Physicians consider a reduction in the diameter of a fibroid to be the most clinically useful measure of shrinkage, and the diameter decreases far less than the total volume as determined using imaging measurements. Unfortunately, most leiomyomata rapidly return to the pretreatment size upon discontinuance of GnRH agonist therapy, and the return of symptoms parallels the enlargement. Prolonged hypogonadism may cause central necrosis of large cellular tumors and permanently reduce the size of individual fibroids. However, few data address this possibility or the circumstances under which it might occur. As a result, the reexpansion of the fibroids to their pretreatment size is the most likely clinical outcome, when ovarian function resumes after discontinuing the GnRH agonist.
Hypogonadism cannot be sustained for a prolonged interval because of the significant side effects, such as vasomotor hot flashes, accelerated bone loss, genital tract atrophy, and loss of the cardiovascular benefits of estrogen. Approximately 1% of the bone mass is lost per month after the onset of hypoestrogenism, and the hot flashes and genital tract atrophy can be very debilitating. Although most of the bone mass is regained if the therapy is limited to 6 months in young women, longer intervals or use in women closer to menopause may result in a permanent loss of age-adjusted bone mineral density. In an attempt to alleviate the severity of the hypogonadal symptoms, the simultaneous administration of low doses of estrogen and progestin simultaneously with GnRH agonists, the so-called add-back regimens, have been advocated. Although these regimens certainly relieve the hypoestrogenic symptoms and prevent bone loss, they have yet to be demonstrated to be as efficacious as GnRH-agonist therapy alone and do not offer any other objective benefit. The GnRH agonist with add-back approach will require a substantial amount of long-term data demonstrating a meaningful clinical benefit before it is considered a viable therapeutic option.
The important question to ask is “What is the goal of medical suppression?” The most important reason for using a GnRH agonist is to stop excessive vaginal bleeding and improve the hemogram prior to surgery, or to temporarily stop the bleeding and delay surgery in order to correct other medical problems posing an increased surgical risk. It is important to recognize that there is an initial action of the GnRH agonist that lasts 2 to 3 weeks before attaining the hypogonadal state. Hence, the bleeding may worsen transiently before stopping, and GnRH agonists are of little use for acute management of bleeding problems. Although reduced surgical blood loss and shortened operative time by preoperative use of a GnRH agonist often are espoused as benefits, scant data support these contentions. Indeed, the softening of small intramural leiomyomata by the hypogonadism may be a detriment. It may be virtually impossible to palpate them during a myomectomy and perhaps even make those identified more difficult to remove by reducing the surgeon's ability to demarcate clearly the boundary between normal myometrium and the fibroid. Given the variation in blood loss with surgery, it will be very difficult to demonstrate reduced intraoperative blood loss with GnRH-agonist pretreatment. Until convincing clinical data are available, the use of GnRH agonists for other than for preoperative correction of anemia will remain controversial.
Myolysis
There have been many attempts to induce therapeutic necrosis of cells within the center of a fibroid, such as myolysis, and thereby to shrink the tumor size, relieve symptoms, and prevent progressive growth of the tumors. These strategies typically involve repeatedly inserting a surgical probe of some sort into the tumor, typically at laparoscopy, and then causing tissue injury by the means of the following: (a) monopolar or bipolar electrocautery, (b) laser hyperthermia, (c) fiber laser vaporization, (d) diathermy (heat-generating ultrasonography), or (e) cryotherapy. All of these techniques require substantial operative time, result in a variable amount of cellular injury within the fibroid, and occasionally injure a portion of the normal myometrium, as well. Aseptic necrosis may cause significant pain during the immediate posttreatment interval, comparable to that observed with degeneration of leiomyomata seen in pregnancy. Long-term data for the efficacy of the various myolysis techniques are lacking, particularly with respect to the normalcy of subsequent pregnancy, safety, and persistence or recurrence rates. As a result, myolysis should be considered experimental until these issues are clarified by well-designed, long-term comparative trials.
Uterine Artery Embolization
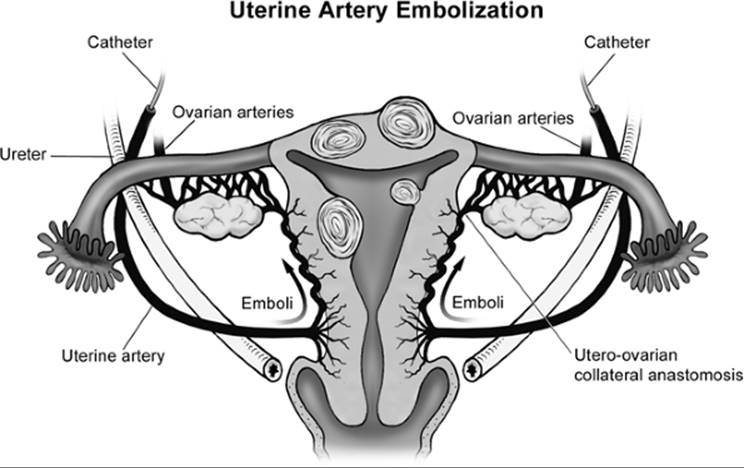
When menorrhagia is the primary clinical symptom and either the surgical risk is judged unacceptable or the patient declines extirpative surgery, therapeutic UAE has been advocated to deprive leiomyomata of blood supply, induce necrosis, and reduce the volume of blood loss (Fig. 49.9). Importantly, there is no dominant vascular pedicle to individual fibroids, so bilateral embolization of both uterine arteries is required to reduce the blood supply to the leiomyomata. The procedure involves cauterizing the femoral artery on one or both sides and identifying the uterine arteries. An embolic agent is then infused to induce clotting and to obstruct blood flow to the uterus. This approach has been used in women with otherwise uncontrollable postpartum hemorrhage and palliatively for women exsanguinating from locally eroding advanced cervical cancer. In those clinical situations, the uterine arteries are the primary vascular supply to the bleeding sites involved, and occluding them reduces this vascular supply. UAE has been employed successfully under these circumstances with comparatively little morbidity relative to the other available options, such as emergency surgery. Based on its success for acute genital tract bleeding, UAE has been promoted actively by interventional radiologists as a primary therapy for virtually any symptoms attributable to fibroids.
|
|
|
FIG. 49.9. The technique of uterine artery embolization. This schematic diagram demonstrates the technique used to inject emboli into the uterine arteries and deprive the normal myometrium as well as the leiomyomata of blood supply. Note that the uterine arteries have collateral connections with the ovarian arteries and provide a pathway for potential embolization to the ovarian vasculature. |
With leiomyomata, the situation is nonemergent and significantly different from postpartum hemorrhage or an eroding cervical cancer. The vascular supply to the myomatous uterus varies significantly from woman to woman, with a large aberrant blood supply developing from normally minor collateral vasculature. UAE, by the nature of the technique, deprives the normal myometrium, as well the tumors enclosed within the uterus, of its blood supply. The technique's success depends on a large differential requirement of blood supply to the fibroids compared with that to the surrounding myometrium. Several case series of carefully selected women with leiomyomata have demonstrated a resolution of the menorrhagia ranging from 65 to 90%, but virtually no data are available for the efficacy for other symptoms attributable to leiomyomata, such as dysmenorrhea, pressure on adjacent viscera, and pelvic pain. The impact of UAE on the size of fibroids is not as well documented, with estimates ranging from 30% to 50%, comparable to the reduction seen with GnRH-agonist management. The leiomyomata typically shrink but, because they are not removed, not always enough to eliminate symptoms such as dysmenorrhea, pelvic pain, and pressure on adjacent viscera.
Although the benefits of UAE for stopping massive bleeding in women with postpartum hemorrhage and with eroding cervical cancer are obviously lifesaving, the long-term safety and efficacy in women with fibroids remain to be demonstrated. This is particularly true for women wishing to retain fertility, whose increased uterine blood flow during pregnancy is a normal physiologic adaptation, critically important to the survival and normal development of the fetus. Few pregnancies have been reported, because most women undergoing UAE are over 40 years of age and not desirous of further childbearing. No information is available regarding intrauterine growth restriction, abnormal placentation, or the value of a cesarean section to prevent uterine rupture during pregnancy or labor. As with an abdominal myomectomy, the risks involved are likely to be related to the number, size, and location of the fibroids being treated.
Another concern for women wishing to retain their fertility is ovarian function. Because there are substantial anatomic collateral connections between the uterine and ovarian vasculature, it is possible for the embolic agents to enter the ovarian vasculature, reduce blood supply to the ovary, and cause premature ovarian failure. The overall rate of ovarian failure is between 5% and 10%, with most of these women being over age 40 at the time of the UAE. However, because the surgical removal of one ovary does not result in earlier menopause, many oocytes may be lost without causing premature menopause. Women may also experience postprocedure amenorrhea when ovarian function is normal, indicating loss of the integrity of the endometrium, which is also of concern regarding fertility. It is imperative that controlled trials with long-term follow-up be performed in order to counsel accurately women with childbearing desires as to the results to be attained with UAE.
UAE has been widely touted as avoiding the risks of abdominal surgery, causing less pain, and requiring less recovery time than surgical extirpation. However, the aseptic necrosis often causes such intense abdominal pain that women undergoing UAE are hospitalized routinely for parenteral narcotic administration for 24 to 48 hours. If intracavitary or submucous myomas are present, the avascular necrosis following UAE may result in prolapse of the degenerating myoma through the cervix, necessitating surgical removal. A postembolization syndrome can develop, similar to that observed after a myocardial infarction, manifested by a flulike syndrome with general malaise, elevated temperature, and leukocytosis. This is difficult to distinguish from an infection and usually is treated with antibiotics. Sepsis can occur, but whether is secondary to an ascending infection or from another source is not clear.
As the number of women undergoing UAE increases, serious acute complications necessitating hysterectomy, and even including death, are being reported. Until randomized comparative trials with long-term follow-up are available demonstrating a benefit of UAE over surgery in a defined clinical setting, this technique will remain a controversial addition to our therapeutic armamentarium. UAE should be considered primarily for women with unacceptably high surgical risks or those women without reproductive desires who do not want surgery. It should be undertaken with the understanding that, although UAE may relieve symptoms, it is not without the risk of serious complications, including death, and that no data are available regarding recurrence rates and long-term complications such as premature ovarian failure.
Another nonextirpative option is the laparoscopic cauterization of both uterine arteries to reduce the flow of blood to the myomatous uterus. As with UAE, the theoretic value is to reduce the vascular supply to both the normal myometrium and the leiomyomata and, thus, cause tissue schemia, with the uterus tolerating this to a greater degree than the myomas. Also like UAE, this therapy has not been assessed adequately in large long-term trials, but in a few highly selected patients it has reduced the symptoms attributable to the leiomyomata. This must be considered an experimental therapy, and its clinical application should await the results of randomized clinical trials with long-term follow-up.
SUMMARY POINTS
· Leiomyomata represent the most common gynecologic tumors and can grow to impressive size, despite being almost invariably benign in the reproductive age group.
· Fibroids cause a variety of gynecologic symptoms and account for a substantial proportion of gynecologic surgery.
· Although some insights into the molecular mechanisms responsible for growth of leiomyomata have been gained, much remains to be learned about this gynecologic tumor, because no consistent molecular mechanism of tumor growth has been identified.
· The therapeutic choices focus on extirpation, with hysterectomy most often used for definitive treatment and myomectomy when preservation of reproductive potential is desired, albeit with a significant recurrence risk.
· Medical therapy focused on hypogonadism is successful for temporarily treating symptoms, but the leiomyomata rapidly return to the pretreatment size upon discontinuance, and this approach does not represent a long-term treatment nor eliminate the risk of recurrent symptoms.
· Newer techniques of UAE and myolysis have not yet been evaluated adequately in comparative clinical trials to establish accurately their risks and long-term recurrence rates, particularly their impact on future reproduction.
· Until a better understanding of the factors involved in initiating leiomyomata growth is achieved, management will remain focused primarily on the surgical relief of symptoms.
SUGGESTED READINGS
Clinical and Anatomic Features
Agency for Healthcare Research and Quality of Life. Management of uterine fibroids. Evidence report. AHRQ Technology Assessment No. 34, 2000. http://www.ahcpr.gov. Accessed January 27, 2003.
Buttram V, Reiter R. Uterine leiomyomata: etiology symptomatology and management. Fertil Steril 1981;36:433–445.
Cramer SF, Patel A. The frequency of uterine leiomyomas. Am J Clin Pathol 1990;94:435–438.
Stewart EA, Nowak RA. Leiomyomata-related bleeding: a classic hypothesis updated for the molecular era. Hum Reprod Update 1996;2:295–306.
Influence of Sex Steroids
Ang WC, Farrell E, Volenhoven B. Effect of hormone replacement therapies and selective estrogen receptor modulators in postmenopausal women with uterine leiomyomas: a review. Climacteric 2001;4:284–292.
Chiaffarino F, Parazzini F, la Vecchia C, et al. Use of oral contraceptives and uterine fibroids: results from a case-control study. Br J Obstet Gynaecol1999;106:857–860.
Parazzini F, Negi E, Vecchia C, et al. Reproductive factors and risk of uterine fibroids. Epidemiology 1996;7:440–442.
Sener AB, Seckin NC, Ozmen S, et al. The effects of hormone replacement therapy on uterine fibroids in postmenopausal women. Fertil Steril 1996;65:354–357.
Genetic Inheritance Pattern
Faestein E, Szklo M, Rosenshein N. Risk factors for uterine leiomyomata: a practice-based case control study. I. African-American heritage, reproductive history, body size and smoking. Am J Epidemiol 2001;153:1–10.
Luoto R, Kaprio J, Rutanen EM, et al. Heritability and risk factors of uterine fibroids-the Finnish twin cohort study. Maturitas 2000;37:15–26.
Marshal LM, Spiegelman D, Barbieri RL, et al. Variation in the incidence or uterine leiomyomata among premenopausal women by age and race. Obstet Gynecol 1997;90:967–973.
Molecular Mechanisms and Genetic Dysregulation
Andersen J. Growth factors and cytokines in uterine leiomyomas. Semin Reprod Endocrinol 1996;14:269–282.
Ligon AH, Morton CC. Genetics of uterine leiomyomata. Genes Chromosomes Cancer 2000;28:235–245.
Rein MS, Friedman AJ, Barbieri RL, et al. Cytogenetic abnormalities in leiomyomata. Obstet Gynecol 1991;97:1923–1926.
Schoenberg Fejzo M, Ashar HR, Krautner KS, et al. Translocation breakpoints upstream of the HMGIC gene in uterine leiomyomata suggest dysregulation of this gene by mechanism different from that in lipomas. Genes Chromosomes Cancer 1996;17:1–6.
Townsend DE, Sparkes RS, Baluda MEC, et al. Unicellular histogenesis of uterine leiomyomas as determined by electrophoresis of glucose-6-phosphate dehydrogenase. Am J Obstet Gynecol 1970;107:1168–1173.
The Impact of Leiomyomata on Reproduction
Bajekal N, Li TC. Fibroids, infertility and pregnancy wastage. Hum Reprod Update 2000;6:614–620.
Benson CB, Chow JS, Chang-Lee W, et al. Outcome of pregnancies in women with uterine leiomyomas identified by sonography in the first trimester. J Clin Ultrasound 2001;29:261–264.
Eldar-Geva T, Lowe PJM, Healy DL, et al. Effect of intramural, subserosal, and submucosal uterine fibroids on the outcome of assisted reproductive technology treatment. Fertil Steril 1998;70:687–691.
Pritts EA. Fibroids and infertility: a systematic review of the evidence. Obstet Gynecol Surv 2001;56:483–491.
Rice JP, Kay HH, Mahony BS. The clinical significance of uterine leiomyomas in pregnancy. Am J Obstet Gynecol 1989;160:1212–1216.
Stovall DW, Parrish SB, Van Voorhis BJ, et al. Uterine leiomyomas reduce the efficacy of assisted reproduction cycles: results of a matched follow-up study. Hum Reprod 1998;13:192–197.
Vercellini P, Maddalena S, DeGiorgi O, et al. Abdominal myomectomy for infertility: a comprehensive review. Hum Reprod 1998;13:873–879.
Leiomyosarcoma
Leibsoln S, d'Ablaing G, Mishell DR, et al. Leiomyosarcoma in a series of hysterectomies performed for presumed uterine leiomyomas. Am J Obstet Gynecol1990;162:968–976.
Parker WH, Fu YS, Berek JS. Uterine sarcoma in patients operated on for presumed leiomyoma and rapidly growing leiomyoma. Obstet Gynecol1994;83:414–418.
Schwartz LB, Diamond MP, Schwartz PE. Leiomyosarcomas: clinical presentation. Am J Obstet Gynecol 1993;168:180–183.
Hysterectomy
Carlson KJ, Miller BA, Fowler FJ Jr. The Maine women's health study: outcomes of hysterectomy. Obstet Gynecol 1994:83:556–565.
Lumsden MA, Twaddle S, Hawthorn A, et al. A randomized comparison and economic evaluation of laparoscopic assisted hysterectomy and abdominal hysterectomy. Br J Obstet Gynaecol 2000;107:1386–1391.
Wilcox LS, Koonin LM, Pokras R. Hysterectomy in the United States, 1988–1990. Obstet Gynecol 1994;83:549–555.
Hysteroscopic Myomectomy
Derman SG, Rehnstrom J, Neworth RS. The long term effectiveness of hysteroscopic treatment of menorrhagia and leiomyomas. Obstet Gynecol1991;77:391–394.
Hallez JP. Single-stage total hysteroscopic myomectomies: indications, techniques and results. Fertil Steril 1995;63:703–708.
Abdominal Myomectomy
Acien P, Quereda F. Abdominal myomectomy: results of a simple operative technique. Fertil Steril 1996;65:41–51.
Davids A. Myomectomy: surgical techniques and results in a series of 1150 cases. Am J Obstet Gynecol 1952;63:592–604.
Fletcher H, Frederick J, Hardie M, et al. A randomized comparison of vasopressin and tourniquet as hemostatic agents during myomectomy. Obstet Gynecol1996;87:1014–1018.
Frederick J, Fletcher H, Simeon D, et al. Intramyometrial vasopressin as a haemostatic agent during myomectomy. Br J Obstet Gynaecol 1994;101:435–437.
Ginsburg ES, Benson CM, Garfield JM, et al. The effect of operative technique and uterine size on blood loss during myomectomy: a prospective randomized study. Fertil Steril 1993;60:956–962.
Reilly R, Nour N. Abdominal myomectomy is associated with few surgical complications. J Gynecol Techniques 1998;4:107–112.
Verkauf BS. Myomectomy for fertility enhancement and preservation. Fertil Steril 1992;58:1–15.
Laparoscopic Myomectomy
Dubuisson JB, Chavet X, Chapron C, et al. Uterine rupture during pregnancy after laparoscopic myomectomy. Hum Reprod 1995;10:1475–1477.
Dubuisson JB, Lecuru F, Foulot H, et al. Myomectomy by laparoscopy: a preliminary report of 43 cases. Fertil Steril 1991;56:827–830.
Harris WJ. Uterine dehiscence following laparoscopic myomectomy. Obstet Gynecol 1992;80:545–546.
Mais V, Ajossa S, Guerriero S, et al. Laparoscopic versus abdominal myomectomy: a prospective randomized trial to evaluate benefits in early outcome. Am J Obstet Gynecol 1996;174:654–658.
Nezhat C. The “cons” of laparoscopic myomectomy in women who may reproduce in the future. Int J Fertil Menopausal Stud 1996;41:280–283.
Reich H. Laparoscopic myomectomy. Obstet Gynecol Clin North Am 1995;22:757–780.
Seinera P, Arisio R, Decko A, et al. Laparoscopic myomectomy: indications, surgical technique and complications. Hum Reprod 1997;12:1927–1930.
Seracchioli R, Rossi S, Govoni F, et al. Fertility and obstetric outcome after laparoscopic myomectomy of large myomata: a randomized comparison with abdominal myomectomy. Hum Reprod 2000;15:2663–2668.
Postoperative Pelvic Adhesions
Diamond MP, Daniell JF, Feste J, et al. Adhesion reformation and de novo adhesion formation following reproductive pelvic surgery. Fertil Steril1987;47:864–866.
diZerega GS. Contemporary adhesion prevention. Fertil Steril 1994;61:219–235.
Tulandi T, Murray C, Guralnick M. Adhesion formation and reproductive outcome after myomectomy and second-look laparoscopy. Obstet Gynecol1993;82:213–215.
Medical Suppression
Coddington CC, Coillins RL, Shawker TH, et al. Long-acting gonadotropin hormone-releasing hormone analog used to treat leiomyomata uteri. Fertil Steril1986;45:624–629.
Murphy AA, Kettel LM, Morrales AJ, et al. Regression of uterine leiomyomata in response to the antiprogesterone RU 486. J Clin Endocrinol Metab1993;76:513–517.
Murphy AA, Morrales AJ, Kettel LM, et al. Regression of uterine leiomyomata to the antiprogesterone RU 486: dose-response effect. Fertil Steril1995;64:187–190.
Schlaff WD, Zerhouni EA, Huth JAM, et al. A placebo-controlled trial of a depot gonadotropin-releasing hormone agonist (Leuprolide) in the treatment of uterine leiomyomata. Obstet Gynecol 1989;74:856–862.
Stovall TG, Muneyyirci-Delale O, Summitt RL Jr, et al. GnRH agonist and iron versus placebo and iron in the anemic patient before surgery for leiomyomas: a randomized controlled trial: Leuprolide Acetate Study Group. Obstet Gynecol 1995;86:65–71.
Zullo F, Pellicano M, De Stefano R, et al. A prospective randomized study to evaluate leuprolide acetate treatment before laparoscopic myomectomy: efficacy and ultrasonographic predictors. Am J Obstet Gynecol 1998;178:108–112.
Myolysis
Arcangeli S, Pasquarette MM. Gravid uterine rupture after myolysis. Obstet Gynecol 1997;89:857.
Goldfarb HA. Laparoscopic coagulation of myoma (myolysis). Obstet Gynecol Clin North Am 1995;22:807–819.
Olive DL, Rutherford T, Zreik T, et al. Cryomyolysis in the conservative treatment of uterine fibroids. J Am Assoc Gynecol Laparosc 1996;3(Suppl 4):S36.
Uterine Artery Embolization
Goodwin SC, McLucas B, Lee M, et al. Uterine embolization for the treatment of uterine leiomyomata. Mid term results. J Vasc Interv Radiol 1999;10:1159–1165.
Lipman JC. Uterine artery embolization for the treatment of symptomatic uterine fibroids: a review. Appl Radiol 2000;29:15–20.
Lumsden MA. Embolization versus myomectomy versus hysterectomy. Hum Reprod 2002;17:253–259.
Ravina JH, Ciraru-Vigneron N, Aymard A, et al. Pregnancy after embolization of uterine myoma: report of 12 cases. Fertil Steril 2000;73:1241–1243.
Ravina JH, Herbreteau D, Ciraru-Vigneron N, et al. Arterial embolization to treat uterine myomata. Lancet 1995;346:671–672.
Recurrence of Leiomyomata Following Myomectomy
Candiani GG, Fedele L, Parazzini F, et al. Risk of recurrence after myomectomy. Br J Obstet Gynecol 1991;98:385–389.
Fauconnier A, Chapron C, Babaki-Fard K, et al. Recurrence of leiomyomata after myomectomy. Hum Reprod Update 2000;6:595–602.
Fedele L, Parazzini F, Luchine L, et al. Recurrence of fibroids after myomectomy: a transvaginal ultrasonographic study. Hum Reprod 1995;10:1795–1796.
Iverson R, Chelmow D, Strohbehn K, et al. Relative morbidity of abdominal hysterectomy and myomectomy for management of uterine leiomyomata. Obstet Gynecol 1996;88:415–419.
Stewart EA, Faur AV, Wise LA, et al. Predictors of subsequent surgery for uterine leiomyomata after abdominal myomectomy. Obstet Gynecol 2002;99:426–432.