IN THIS CHAPTER
![]() Getting to the bottom of the causes, symptoms, and types of diabetes
Getting to the bottom of the causes, symptoms, and types of diabetes
![]() Knowing and modifying your risk factors and receiving a diagnosis
Knowing and modifying your risk factors and receiving a diagnosis
![]() Discovering how regulating carb intake is part of the treatment
Discovering how regulating carb intake is part of the treatment
Twenty-nine million Americans have diabetes. About 90–95 percent have type 2 diabetes, while 5–10 percent have type 1 diabetes. A couple other forms of diabetes make up a smaller percentage of cases. Eighty-six million American adults — over one-third of the population — have prediabetes, a condition of elevated glucose levels but not yet a diagnosis of diabetes.
If you rewind the clock by 50 to 100 years, diabetes was not nearly as prevalent as it is today. The societal trend is that Americans are now heavier and less active than our ancestors were a few generations ago. Being overweight and physically inactive are key risk factors for developing prediabetes and type 2 diabetes. It is now predicted that by the year 2050, one out of every three adults will have diabetes. It’s time to turn those trend lines around.
The Centers for Disease Control and Prevention (CDC) say, “Obesity-related conditions including heart disease, stroke, and type 2 diabetes are among the leading causes of preventable death.” Very convincing studies from all around the globe show that lifestyle interventions can delay or prevent diabetes. Those lifestyle interventions are also at the core of treating diabetes and are focused on improving dietary patterns, exercise habits, and weight management.
Diabetes can go undetected for many years, so screening is critically important. The CDC estimates that 25 percent of people with blood-glucose levels in the diabetes range remain undiagnosed, and an alarming 90 percent of people in the prediabetes range don’t realize that their glucose levels are elevated. This chapter identifies the risk factors and potential symptoms of diabetes, the diagnostic and classification criteria, and where to go next if you’re diagnosed.
Wrapping Your Brain around Diabetes and Related Conditions
We rely on foods to provide our bodies with energy, vitamins, minerals, and essential nutrients. On the most basic level, food and water are required for survival, but food is so much more than just a way to survive. We savor and enjoy food. We have cultural traditions, family recipes, and memories associated with food. Friends and relatives socialize around dinner tables and celebrate holidays and special occasions over meals.
When you’re diagnosed with diabetes, the focus on food shifts, and the next thing you know you are being asked to read food labels and break out the measuring cups. Your vocabulary expands to include the words “pancreas,” “insulin,” “carbohydrate,” and “blood glucose.” The good news is diabetes is manageable, now more than ever before. The first step in successfully managing your diabetes is to understand how the body is supposed to work and what has gone awry if you’ve developed diabetes. The following sections cover these topics.
Seeing how the body is supposed to process carbs
Human bodies need fuel to function. Glucose is the primary fuel source for the brain and red blood cells. It is also the preferred fuel source for muscles. Carbohydrate-containing foods provide glucose through the process of digestion and absorption. Glucose travels throughout the body via the bloodstream to all awaiting organs, tissues, and cells. For more on that process, see Chapter 4 .
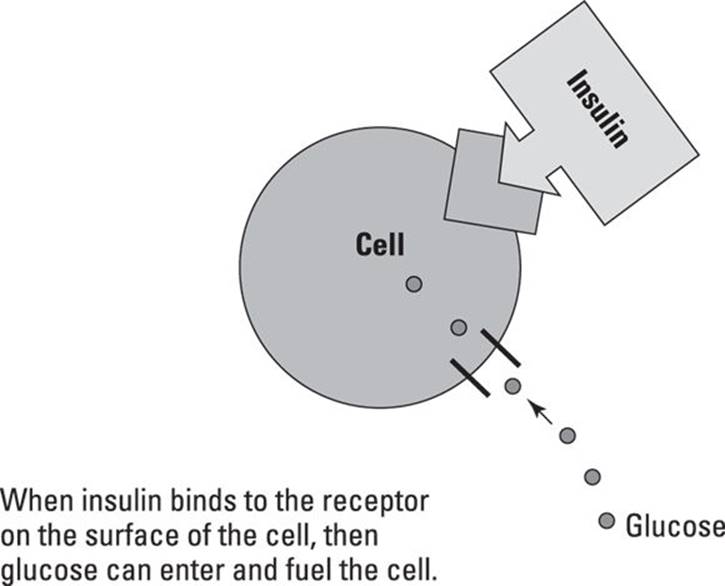
When all systems are working properly, a hormone called insulin helps the glucose move from the bloodstream into the cells where it’s burned for energy. The pancreas is the organ that makes and secretes insulin. Think of insulin as a “key” that has to unlock the cells to allow the glucose in. Insulin is supposed to bind to an insulin receptor on the surface of the cell. Once the insulin and the receptor are coupled, then the glucose may enter the cell. See Figure 2-1 .
© John Wiley & Sons, Inc.
FIGURE 2-1: Insulin allows glucose to enter the cell.
If you have diabetes, it means either you don’t make enough insulin, or the insulin you make simply doesn’t work effectively. The next section elaborates further.
Discovering what causes diabetes
The surface of the pancreas has insulin-producing cells called beta-cells or islet cells. In the case of type 1 diabetes, the beta-cells are destroyed so they are no longer able to produce insulin. Without insulin, glucose cannot properly nourish the body.
 Prior to 1921 when insulin was first discovered, people with type 1 diabetes didn’t survive very long. Initially insulin was harvested from cattle and pig pancreases and injected into humans. It wasn’t perfect and it caused allergic reactions, but people lived. In the 1970s genetically “human” insulin was produced in the lab and became widely available. Fast forward to today: There are numerous types of insulin and advanced technologies for administering them. Researchers around the globe continue to make progress in leaps and bounds, and they likely won’t stop until they find a cure.
Prior to 1921 when insulin was first discovered, people with type 1 diabetes didn’t survive very long. Initially insulin was harvested from cattle and pig pancreases and injected into humans. It wasn’t perfect and it caused allergic reactions, but people lived. In the 1970s genetically “human” insulin was produced in the lab and became widely available. Fast forward to today: There are numerous types of insulin and advanced technologies for administering them. Researchers around the globe continue to make progress in leaps and bounds, and they likely won’t stop until they find a cure.
Type 2 diabetes is a state of “insulin resistance.” People with type 2 are able to make insulin, but the insulin isn’t fully effective. It’s similar to having a key made for your front door, but when you attempt to use it, you are frustrated to find out that it doesn’t work smoothly. The key is there, the lock is there, but it takes persistence and jiggling and coaxing until finally the door opens. That’s the case with type 2 diabetes. The insulin is there and the insulin receptor is there, but the cell isn’t responding properly. Glucose uptake is delayed due to insulin resistance, so blood-glucose levels rise.
Insulin resistance precedes the onset of type 2 diabetes. Long before the diagnosis, the pancreas responds to rising blood-glucose levels by working harder to produce extra insulin. The pancreas works overtime because insulin levels have to rise higher than normal in order to manage glucose levels. Eventually the pancreas tires out and the beta-cells can no longer keep up the pace, so blood-glucose levels rise into diabetic ranges. (When glucose levels rise high enough, you may have symptoms, but not always. Symptoms are explained in the next section.)
Noticing the symptoms of diabetes
With insufficient amounts of insulin or insulin that doesn’t work properly, glucose can’t effectively get into the cells. Instead, the glucose accumulates in the bloodstream. Blood is filtered through the kidneys. Kidneys dispose of some of the excess glucose by removing it from the blood and dumping it into the urine. The bladder fills more quickly, which leads to frequent urination. Because the calories from glucose are flushed down the toilet, the cells aren’t fed as much and weight loss may occur.
There’s an interesting history behind the naming of the disease. The Greeks called it Diabetes Mellitus. Diabetes means “a siphon,” which refers to the excessive urination associated with the disease. Mellitusmeans “like honey,” which refers to the sweet smell and taste of the urine. Doctors in ancient Greece relied on their sense of taste and smell to make the diagnosis.
 Symptoms are associated with uncontrolled diabetes. However, some people are asymptomatic, so diabetes can brew undetected for many years. In fact, some people are diagnosed with diabetes after developing a complication associated with uncontrolled, long-duration diabetes. It is important to have standard screening protocols for those at risk. Identifying risk factors and screening criteria are addressed later in this chapter.
Symptoms are associated with uncontrolled diabetes. However, some people are asymptomatic, so diabetes can brew undetected for many years. In fact, some people are diagnosed with diabetes after developing a complication associated with uncontrolled, long-duration diabetes. It is important to have standard screening protocols for those at risk. Identifying risk factors and screening criteria are addressed later in this chapter.
The common symptoms associated with elevated blood glucose include
· Increased urination: This occurs because the kidneys are dumping some of the excess glucose into the urine.
· Thirst: Frequent urination can lead to dehydration, which triggers thirst.
· Hunger: The result is hunger as glucose is lost in the urine instead of being available to feed the cells and tissues. Additionally, when cells aren’t fed, muscles and body fat break down to provide an alternate fuel source. The body can break itself down to feed itself, which can lead to weight loss.
· Additional symptoms: These may include fatigue, blurred vision, tingling or numbness in feet and hands, yeast and fungal infections, and wounds that are slow to heal.
o When glucose isn’t used properly, the body lacks its main energy supply, which may result in fatigue or weakness.
o Blurry vision is usually temporary. It’s caused by glucose accumulating in the lens of the eye, which in turn causes fluid retention and swelling of the lens. Once glucose levels are controlled, the lens goes back to its usual shape and vision should improve.
 Do not buy a new pair of glasses when your blood glucose is out of control. The lens of the eye may be temporarily misshapen due to concentrated glucose levels, and that can alter vision. Your eye specialist should evaluate your baseline vision once your glucose levels have stabilized in the near normal range.
Do not buy a new pair of glasses when your blood glucose is out of control. The lens of the eye may be temporarily misshapen due to concentrated glucose levels, and that can alter vision. Your eye specialist should evaluate your baseline vision once your glucose levels have stabilized in the near normal range.
o Uncontrolled diabetes can lead to nerve damage. Peripheral neuropathy, which refers to the nerves farthest from the brain and spinal cord, can cause tingling, burning, pain, or numbness in the feet or hands.
o High blood glucose means more sugar is available for yeast and bacteria to thrive on, so infections can fester.
o Healing may be impaired because the body’s immune system is compromised when glucose is out of control.
 The symptoms associated with diabetes are not diagnostic and are sometimes related to other medical conditions. Discuss all medical concerns with your healthcare providers. Diabetes screening protocols are based on risk factors including weight and age and are clarified later in the chapter.
The symptoms associated with diabetes are not diagnostic and are sometimes related to other medical conditions. Discuss all medical concerns with your healthcare providers. Diabetes screening protocols are based on risk factors including weight and age and are clarified later in the chapter.
Distinguishing the types of diabetes
There are several types of diabetes. The suggested treatment depends upon the type. The vast majority of people have type 2 diabetes. Some people with type 2 diabetes can achieve control through diet and exercise modifications, while others need to add one or more oral medications. Everyone with type 1 diabetes and some people with type 2 diabetes require insulin.
Type 1 diabetes
Type 1 diabetes is an autoimmune disease. The body’s immune system, which is supposed to fight off bacteria, mistakenly destroys the insulin-producing beta-cells of the pancreas. People with type 1 diabetes no longer make insulin, so they must take insulin to live.
In the past this form of diabetes was called juvenile diabetes, insulin-dependent diabetes, or IDDM (short for insulin-dependent diabetes mellitus). The preferred term is type 1 diabetes, which may be abbreviated T1DM or T1D. The old terms don’t hold true for all cases. Not all kids with diabetes have type 1; there are many adolescents with type 2 diabetes. Insulin is used to treat other forms of diabetes, not just type 1. While it is true that type 1 diabetes is most often diagnosed when a person is below the age of 20, some adults are diagnosed with type 1 diabetes in their 20s, 30s, 40s, and even later.
Blood tests can determine whether the diagnosis is type 1 diabetes by detecting autoimmune markers in the blood. Another lab test called C-peptide estimates the amount of insulin being produced. (Find out more about diagnosing diabetes later in this chapter.)
Type 2 diabetes
Type 2 diabetes is due to insulin resistance. People with type 2 diabetes make insulin, but the insulin doesn’t work very well. Their own cells are resistant to the action of their insulin. Type 2 diabetes is due to a progressive insulin deficiency imposed on top of the initial insulin resistance.
Previously it was called adult-onset, non-insulin-dependent diabetes, or NIDDM (non-insulin-dependent diabetes mellitus). The current standard is to call it type 2 diabetes, which can be abbreviated T2DM or T2D. Unfortunately, type 2 diabetes often occurs alongside of high blood pressure and dyslipidemia (abnormal blood fats). A major shift must take place in the lifestyle of Americans to turn this trend around.
Prediabetes
Prediabetes is when blood-glucose levels are above normal but not yet in the range of diabetes. One in three American adults has blood-glucose levels in the prediabetes range. Up to 90 percent of them don’t know it. Prediabetes can lead to type 2 diabetes within five to ten years. The good news is that studies clearly show that progressing to type 2 diabetes isn’t inevitable. Weight loss of roughly 5–10 percent of starting weight coupled with moderate exercise of at least 150 minutes per week reduces the risk by up to 58 percent. Early detection and intervention may return blood-glucose levels to near normal ranges.
Gestational diabetes
Gestational diabetes is typically diagnosed in the second or third trimester of pregnancy. Pregnancy hormones interfere with the way insulin works by inducing a state of insulin resistance. As the pregnancy progresses, the mother’s pancreas has to work harder to make enough insulin to keep blood-glucose levels controlled. Some women simply can’t keep up with the demand, and they get diabetes during pregnancy, which resolves after delivery. Gestational diabetes is abbreviated as GDM (gestational diabetes mellitus). Women should be screened for GDM at 24 to 28 weeks of pregnancy. GDM also indicates a risk for developing type 2 diabetes in the future. (See Chapter 17 and the nearby sidebar “Diabetes and pregnancy ” for more information.)
Other forms of diabetes
Other forms of diabetes make up only a small fraction of the cases of diabetes. These forms include the following:
· Neonatal diabetes occurs within the first six months of life and can be transient or permanent. Genetic testing is needed to clarify the defect, because some babies are best treated with oral medications while others require insulin.
· Cystic fibrosis–related diabetes (CFRD) can affect as many as half of the adults and 20 percent of the children who have cystic fibrosis. Insulin is the therapy of choice for CFRD.
· Maturity-onset diabetes of the young (MODY) is inherited and caused by any number of different chromosomal mutations. Treatment depends upon the specific genetic defect, so testing is required to clarify the diagnosis.
DIABETES AND PREGNANCY
Diabetes during pregnancy is considered a high-risk pregnancy. It is imperative for women with type 1 and type 2 diabetes to have tightly controlled blood-glucose levels prior to becoming pregnant. Uncontrolled diabetes can have devastating consequences. When maternal glucose levels are elevated, the extra glucose readily passes to the baby and that can cause big problems. High blood glucose in the first trimester increases the risk of birth defects and miscarriage. Gestational diabetes doesn’t develop until later in the pregnancy, so birth defects aren’t a concern with GDM.
There are late-pregnancy risks that apply to women with type 1, type 2, and gestational diabetes. High glucose in the second half of the pregnancy can cause the baby to grow too big, which makes for a riskier delivery for both baby and mom. Uncontrolled glucose levels also increase the risk of preeclampsia and stillbirth. Stringent glucose control throughout the entire pregnancy is critical. Women with diabetes who are of childbearing age should have preconception counseling. Some medications are not safe for the baby and thus must be discontinued prior to conception, including meds used to treat hypertension and cholesterol. Have a discussion with your healthcare provider. For more information on managing diabetes during pregnancy, see Chapter 17 .
Recognizing Diabetes Risk Factors and Getting Diagnosed
The onset of type 1 diabetes tends to be sudden and come as a complete surprise. Prediabetes and type 2 diabetes can go undetected for years. Early diagnosis and intervention improve outcomes. I address screening protocols and diagnostic testing in the following sections.
Type 1 diabetes risk factors
The risk factors for type 1 diabetes are still being researched but may include the following:
· Family history and genetics: Caucasians have the highest risk of developing type 1 diabetes. The risk is increased if you have a parent, sibling, or child with type 1. If a mother has type 1 diabetes, her child has a 2–3 percent chance of developing it. If the father has type 1, the chance is a little higher: about 6–8 percent. If a child in the family has type 1 diabetes, the chance that a sibling will develop it is close to 4 percent. Family members can be screened with a lab test that identifies markers in the blood. Often, however, a person with type 1 diabetes has no relatives with the condition.
 TrialNet is a network of clinical centers dedicated to the study of type 1 diabetes. They have numerous ongoing clinical trials aimed at finding better ways to prevent, diagnose, and treat type 1 diabetes. If someone in the family has type 1 diabetes, then the parents, children, and siblings can be screened to see whether they have markers in the blood that indicate the risk of developing diabetes. For more information, visit www.diabetestrialnet.org .
TrialNet is a network of clinical centers dedicated to the study of type 1 diabetes. They have numerous ongoing clinical trials aimed at finding better ways to prevent, diagnose, and treat type 1 diabetes. If someone in the family has type 1 diabetes, then the parents, children, and siblings can be screened to see whether they have markers in the blood that indicate the risk of developing diabetes. For more information, visit www.diabetestrialnet.org .
· Geography: Interestingly, the incidence of type 1 diabetes increases the farther you travel north away from the equator. Northern European countries have a high prevalence, with Finland being the highest. In general the colder climates have a higher prevalence of type 1 diabetes.
· Viral triggers: Exposure to the following viral infections is being investigated: Epstein-Barr, Coxsackie, mumps, and cytomegalovirus. However, none have yet to be proved causal.
· Early infant feeding practices: These factors are being explored to see whether what babies are fed matters; breastfeeding seems to decrease the risk of type 1.
Screening for T1DM in asymptomatic low-risk individuals is not cost-effective or recommended. If you have an immediate family member with T1DM, you can be screened for auto-antibodies. These markers in the blood indicate risk but do not mean that you will develop the disease.
Type 2 diabetes risk factors
Diabetes is often linked with other health issues in what is referred to as metabolic syndrome. Body fat accumulated around the waistline is linked to developing diabetes more so than having extra pounds in the hips and thighs. High blood pressure and lipid issues also seem to go hand in hand with type 2 diabetes.
 Many of the risk factors for developing diabetes are modifiable. Food choices and eating habits affect overall health. The right food choices can promote health and healing, while poor eating habits can hinder health and increase the risk of chronic diseases. Diabetes, weight, blood pressure, blood fats, and heart health all respond to improvements in eating habits.
Many of the risk factors for developing diabetes are modifiable. Food choices and eating habits affect overall health. The right food choices can promote health and healing, while poor eating habits can hinder health and increase the risk of chronic diseases. Diabetes, weight, blood pressure, blood fats, and heart health all respond to improvements in eating habits.
The following risk factors are associated with developing type 2 diabetes and indicate the need for screening:
· Inheriting the risk: Type 2 diabetes runs in families. Having the risk doesn’t mean a certain diagnosis. Eating healthfully, controlling weight, and being more physically active can reduce the risk of developing diabetes. If you have diabetes, your children are at increased risk, so it’s important to teach them healthy habits. All overweight children with risk factors associated with type 2 diabetes should be screened every three years starting at age 10 or puberty. Early detection and treatment improves outcomes.
· Being from a high-risk ethnic group: Certain ethnicities have a stronger risk of developing type 2 diabetes: African Americans, American Indians, Pacific Islanders, Asian Americans, Hispanics, and Latinos. However, anyone can develop type 2 diabetes.
· Getting older: Aging increases the risk of developing type 2 diabetes. Being above 45 years old is considered a risk factor and is the recommended age to begin screening. Having other risk factors means you should be screened earlier. If screening results are negative, you should be rescreened at least every three years.
· Being overweight: Obesity tends to run in families. There is a genetic component to weight, but families also tend to share similar eating and exercise habits. Modest weight loss reduces the risk of developing diabetes; studies show that weight loss and exercise are the most effective strategies to prevent prediabetes from progressing to type 2.
· Living a sedentary lifestyle: Exercise lowers the risk of developing diabetes in several ways. Exercise improves the way insulin works and how muscles burn glucose. Exercise reduces the risk of developing diabetes because it helps with weight management and preserves muscle mass. (See Chapter 14 for more about fitness.)
· Struggling with insulin resistance or impaired glucose tolerance: If you’ve had borderline or high glucose levels at any point in your life, it may indicate an underlying issue with the way your insulin works.
· Having lipid issues: People with diabetes may have high LDL (the bad cholesterol), but they most commonly have low HDL (the good cholesterol) and high triglycerides (blood fats).
· Battling high blood pressure: Hypertension is a common co-morbidity. High blood pressure should be managed aggressively as it can increase the risk that a person with diabetes will develop long-term complications to blood vessels in the eyes, kidneys, and even the heart.
· Contending with cardiovascular disease: If you have a history of cardiovascular disease, your risk of having diabetes increases.
· Being a woman under some circumstances: Women who had gestational diabetes (GDM), delivered a baby that weighed over 9 pounds, or have polycystic ovarian syndrome (PCOS) are also at an increased risk of developing type 2 diabetes. Gestational diabetes indicates a struggle to manage blood glucose when faced with insulin resistance caused by pregnancy hormones. Future variables such as aging, weight gain, or inactivity could push you again into a situation where your insulin cannot keep up with the demand. PCOS has a component of insulin resistance.
· Having acanthosis nigricans: Dark, thick patches that may occur on the back of the neck and in the armpits are called acanthosis, which is an indicator of insulin resistance.
Anyone who is overweight and has one or more of the preceding risk factors associated with type 2 diabetes should be screened at a lab. If results come back normal, testing should be repeated at a minimum of every three years. All adults should begin screening at age 45 regardless of other risk factors because aging is a risk factor. Overweight children should begin screening at puberty or age 10.
Diagnosing diabetes
Diabetes is diagnosed using one or more of the three blood tests shown in Table 2-1 .
· Fasting blood glucose requires an eight-hour fast.
· The oral glucose tolerance test (OGTT) test checks blood-glucose response two hours after drinking 75 grams of glucose.
· The A1C test is reflective of a three-month average, so you do not need to be fasting to have this lab test.
 The A1C test measures the amount of glucose attached to a specific protein known as hemoglobin A protein, located on the surfaces of red blood cells (RBCs). Glucose binds to proteins in a process known as glycosylation. A1C is reflective of glycosylation throughout the body, so it’s also used to assess blood-glucose control and risk for complications. Glycosylation can damage delicate tissues such as the retina of the eye, nerves, kidneys, and blood vessels. See Chapter 23 for more on glucose monitoring and A1C.
The A1C test measures the amount of glucose attached to a specific protein known as hemoglobin A protein, located on the surfaces of red blood cells (RBCs). Glucose binds to proteins in a process known as glycosylation. A1C is reflective of glycosylation throughout the body, so it’s also used to assess blood-glucose control and risk for complications. Glycosylation can damage delicate tissues such as the retina of the eye, nerves, kidneys, and blood vessels. See Chapter 23 for more on glucose monitoring and A1C.
TABLE 2-1 Screening Tests and Diagnostic Criteria
|
Screening Test |
Normal |
Prediabetes |
Diabetes |
|
Fasting blood glucose |
Under 100 |
100–125 |
126 or more |
|
Oral glucose tolerance test (OGTT) |
Under 140 |
140–199 |
200 or more |
|
A1C |
Under 5.7 |
5.7–6.4 |
6.5 or more |
If just one of the lab tests comes back abnormal it should be repeated to confirm the diagnosis. If two lab tests are done and both are abnormal, that confirms diagnosis.
The screening tests in Table 2-1 diagnose prediabetes and diabetes but don’t differentiate between type 1 diabetes and type 2 diabetes. A definitive diagnosis of type 1 diabetes requires additional blood work to identify autoimmune markers.
Moving Forward with Managing Diabetes
Healthy lifestyle behaviors can prevent or delay the development of type 2 diabetes. If you already have diabetes (either type 1 or type 2), then nutrition and exercise are foundation management strategies. Blood-glucose control is essential because poorly controlled diabetes increases the risks of heart disease, stroke, and serious complications including blindness, cataracts, glaucoma, kidney damage, blood vessel and nerve damage, impotence, altered digestion, infections, and lower limb amputations.
Take a breath and listen to this important message: Well-controlled diabetes is the leading cause of nothing! That’s right. Complications aren’t an automatic inevitability. They are preventable. What you eat affects your health. You need to eat carbohydrates, but it is important to understand how to manage carbs in order to manage diabetes, and that’s what this section and this book are all about.
Knowing that diet matters
Carbs are an important part of a balanced diet. This book focuses on learning to eat the right carbs, in the right amounts, at the right time. Diabetes management means controlling your blood-glucose levels, which ultimately requires knowing how to manage carb choices. It doesn’t mean divorcing carbs.
Think about the big picture. Weight control, blood-pressure control, lipid control, and overall health and happiness are also influenced by dietary choices. That means paying attention to more than just the carbs. If you make the right food choices most of the time, you should see a payoff in terms of your health and quality of life. See Chapter 13 for more on healthy eating.
Keeping in touch with your diabetes team
Many variables affect diabetes control and outcomes. Managing diabetes is a bit like solving a puzzle. You have to figure out how diet, exercise, glucose monitoring, and medications all fit together. It’s pretty tough to figure it all out on your own. Try the following:
· Build your diabetes team. Ask your doctor to refer you to a diabetes self-management class or make appointments to see a nurse and a registered dietitian (RD or RDN). Choose professionals who are well-versed in diabetes management, such as Certified Diabetes Educators, if available.
Note: The abbreviations RD (registered dietitian) and RDN (registered dietitian nutritionist) are synonymous and indicate a trained medical professional who is credentialed by the Commission on Dietetic Registration. RDs and RDNs have a college degree, have passed a stringent national exam, and participate in ongoing continuing education to maintain their credential. Be aware that anyone can call himself a nutritionist regardless of training or experience because that term isn’t regulated.
· Sometimes life just gets in the way and it’s hard to prioritize diabetes self-management. If diabetes is altering your mood and you’re feeling depressed or just plain “stuck,” then you may benefit from counseling with a mental-health specialist familiar with the issues associated with chronic illness.
· Keep in mind that diabetes management strategies may need to be tweaked along the way. Over time what used to work may no longer be effective. Things change. Have diabetes evaluations and tune-ups by meeting with your diabetes experts on a regular basis.
 If you search for health information online, be sure to access reputable resources. See Chapter 25 for a list of worthwhile websites.
If you search for health information online, be sure to access reputable resources. See Chapter 25 for a list of worthwhile websites.
Embracing your central role in your own self-care
You are the most important person in your healthcare team. In the course of a month, year, or lifetime, you spend only a small fraction of time face to face with the medical providers. Enlist the support of your family and friends, but ultimately remember that it is up to you to integrate diabetes management into your daily routine. Check your blood-glucose levels and know how to interpret the results. Let your medical providers know if your blood glucose isn’t being well-controlled. Medication regimens may need to be adjusted or intensified with long-standing diabetes. Advocate for yourself. Don’t settle for sub-optimal control. You are in it for the long haul, and you’re worth it.