Diabetes is a common disease that is characterized by elevated blood glucose. More casually, this is often referred to as high blood sugar. Normally, after you eat, some of the food is broken down into glucose (a sugar) and is transported through the body in the bloodstream. This increase in blood glucose triggers the pancreas, a small organ in the abdomen, to release insulin. Insulin is a hormone needed to move the glucose into the body cells to either be used or be stored as energy for later use. In general, diabetes results from your body’s inability to produce insulin (type 1) or to use the insulin properly to lower blood glucose levels to normal (type 2) (2).
Over 29 million Americans have some type of diabetes, and another estimated 86 million people have prediabetes, or slightly elevated blood glucose levels (44). Approximately 90 percent of people with diabetes have type 2. The remaining 10 percent have type 1 diabetes, which tends to occur in younger people, although it can develop at any age. Other categories of diabetes exist, including gestational diabetes, which occurs during pregnancy (2).
If you are reading this chapter, either you have diabetes or someone important to you does. After diagnosis, it’s common to feel shocked, concerned, frustrated, sad, angry, or a combination of emotions. A diabetes diagnosis, however, can be an opportunity to examine how to take charge of your health. Although there is no magic wand to make diabetes disappear, exercise and attention to proper nutrition are two vital factors in managing diabetes and preventing its possible health complications. Exercise is the mainstay of treatment to improve insulin resistance and the effectiveness of any diabetes medications that you take (43). Diet, along with exercise, is also important in managing all types of diabetes and even potentially preventing type 2 diabetes (3). This chapter addresses how to safely include physical activity in your life and provides general nutrition guidelines for diabetes management. Insulin and various oral or other diabetes medications are discussed as well.
Causes of Diabetes
The origin of type 1 diabetes differs from that of type 2 diabetes. Type 1 diabetes is an autoimmune disease, which occurs when your body attacks its own cells (2). In type 1 diabetes, the cells in the pancreas that produce insulin are destroyed. Thus, insulin cannot be produced to lower your blood glucose after meals and snacks. As a result, blood glucose is not able to enter the cells, causing glucose levels in the blood to become elevated. A high level of glucose in the blood is called hyperglycemia. Hyper- means a high level, and glycemia refers to blood glucose concentrations. As a result of the deficiency in insulin production, type 1 diabetes must be treated with insulin, given as injections, delivered via an insulin pump, or sometimes inhaled.
Type 2 diabetes occurs when body cells cannot properly use the insulin produced by the pancreas (2). This is called insulin resistance (i.e., impaired insulin action in which body cells are resistant to the action of insulin). Insulin normally allows glucose to enter cells in the body to provide energy; but with insulin resistance, the glucose cannot enter the cells and thus remains in the blood. In type 2 diabetes, the body’s ability to produce insulin usually decreases over time, which also contributes to hyperglycemia. As a result, some people with type 2 diabetes must also take supplemental insulin to control their blood glucose levels.
Obesity is associated with the development of type 2 diabetes, in particular upper body fat stores (i.e., an apple-shaped physique) (43). In the past, type 2 diabetes was called adult-onset diabetes because of the typically older age of onset. Unfortunately, the increased incidence of obesity and sedentary lifestyles has resulted in type 2 diabetes developing at earlier ages (6), thus exposing people to elevated blood glucose for longer periods of time and increasing their risk of health complications, such as kidney, eye, nerve, and heart disease. Other factors in addition to excessive body weight and inactivity increase the chances of developing diabetes (2):
· Prediabetes (see the sidebar How Do I Know If I Have Prediabetes or Diabetes?)
· Age (greater than 45 years old)
· Family history (parent or sibling)
· Other health concerns, including low high-density lipoprotein cholesterol, high triglycerides, high blood pressure
· Certain racial and ethnic groups, including non-Hispanic blacks, Hispanic Americans, Asian Americans and Pacific Islanders, American Indians, and Alaska Natives
· Women who had gestational diabetes or have had a baby weighing 9 pounds (4 kg) or more at birth
Although a number of factors cannot be changed (e.g., your race or age), you can control your body weight and physical activity level. These factors are the focus of this chapter.
How Do I Know If I Have Prediabetes or Diabetes?
Blood glucose exists on a continuum from normal to elevated (diabetes). Prediabetes is diagnosed when the fasting blood glucose is above normal (greater than 100 mg/dL) but below the cutoff for diagnosing diabetes (126 mg/dL) (2). If your glucose level is in this range, you are at a higher risk for cardiovascular disease in addition to developing type 2 diabetes (33). Although a diagnosis of prediabetes increases your risk, it does not mean that type 2 diabetes is unavoidable or that prediabetes is not reversible. Losing weight and increasing your physical activity level will not only lower your risk for cardiovascular disease but also decrease your likelihood of progressing to fully developed type 2 diabetes (32). Losing at little as 5 percent of body weight (for example, 10 pounds [4.5 kg] for someone weighing 200 pounds [~90 kg]) has been found to decrease the risk of developing type 2 diabetes and other obesity-related complications in people who are overweight (35).
Exercise plays a pivotal role in preventing as well as managing diabetes.

Healthy Approaches to Managing Diabetes
Physical activity and diet are two important lifestyle factors for anyone with type 1 or type 2 diabetes. This section discusses how both exercise and nutrition can help you manage your diabetes as well as improve your health and fitness.
Focusing on Nutrition
Weight loss may be a useful goal for people with type 2 diabetes who are overweight, and preventing excessive weight gain if you have type 1 diabetes can help keep your insulin action high and your insulin needs lower (9). Sustaining a weight loss of as little as 5 to 7 percent of body weight can lead to a decrease in insulin resistance and improvement in blood glucose control, therefore allowing for a reduction in the amount of medication taken (37). Weight management is discussed in detail in chapter 18; therefore the nutrition focus in this chapter is on the benefits of balancing carbohydrates, fats, and proteins in your diet to control blood glucose levels.
Dietary Macronutrients
The three macronutrients that provide energy for activity and routine body functioning are carbohydrates, fats, and proteins. Everyone, including persons with diabetes, benefits from an appropriate balance of these three nutrients. Obviously, because diabetes results from a break in the link between food eaten and the body cells receiving energy, diet is a major consideration in managing diabetes. Food choices do not need to be a frustrating mystery—just giving your diet some extra attention will allow for better control of the disease.
The macronutrients supply your body with energy or calories, although each of these nutrients has a different primary role. Protein helps to build muscle, while fat is important as a source of stored energy and contributes to the health of your brain, nerves, hair, skin, and nails. Carbohydrate is a major fuel source for your body, especially during physical activity, and is the primary supplier of energy for your brain, nerves, and muscles.
While each of these nutrients affects your blood glucose in different ways, carbohydrates in your diet have the greatest impact on the amount of glucose in your blood because they are turned into glucose quickly. You should check your blood glucose before and after meals to learn how foods affect your blood levels, particularly those containing a lot of carbohydrate (such as potatoes, bread, rice, and pasta). Focus on keeping portion sizes in check, which is helpful if weight loss is a goal and also helps manage your blood glucose levels by providing a good balance of carbohydrate, fat, and protein.
Fiber Intake
Dietary fiber, found in plant-based foods, is also a critical component of the meal plan for anyone with diabetes. Fiber cannot be digested completely because it resists acids and other digestive enzymes in the stomach and thus does not add extra calories to your diet. Fiber is found in foods such as oats, oat bran, ground flaxseed, beans and fruits, wheat bran, apple peel, and most vegetables.
Dietary fiber has many health and metabolic benefits (39). Fiber adds bulk and helps move food waste out of the body more quickly. Fiber also helps you feel full and can support your weight loss efforts. From a diabetes and health standpoint, dietary fiber may reduce blood glucose and cholesterol, all while slowing the digestion of carbohydrates to glucose, thereby keeping your blood glucose more stable. A high intake of dietary fiber, specifically cereal and fruit fiber, has been shown to lower the risk of heart disease by trapping fat and cholesterol during the digestive process and eliminating cholesterol through the stools. A good target intake is at least 20 to 35 grams of fiber per day.
Carbohydrate Intake
Your first reaction might be to avoid carbohydrates as a way to keep your blood glucose levels in check, but your body needs the fiber that is found in carbohydrate-based plant foods. Carbohydrates are also your body’s first choice of fuels during many physical activities, and not having enough in your diet may limit your ability to exercise optimally. Many people with diabetes count the grams of carbohydrate in foods to help them control their blood glucose levels, and others choose carbohydrates based on the glycemic index (how rapidly the food item raises blood glucose levels) (8). The exact amount of carbohydrate you should consume varies based on how active you are, the medications you take, and your overall insulin action. Typically, starches and sugars are factored into your daily total, whereas fiber and nonstarchy vegetables are not. Examples of nonstarchy vegetables are salad greens, peppers, tomatoes, beans, carrots, cauliflower, and onions.
Q&A
How can I know how much carbohydrate is in a food item?
To determine the grams of carbohydrate in a given product, consult the package label. Be sure to check the serving size because serving sizes can be quite small—you may actually consume more than just one serving in a meal. For more details on reading food labels, see chapter 3.
As you review food labels for the number of carbohydrates in a given product, you may run across “sugar-free” products that contain sugar alcohols, which are reduced-calorie sweeteners (usually about half the number of calories of sugar). Your blood glucose response to different products may vary; but in general, sugar alcohols (like sorbitol) have less of an impact on your blood glucose level than other carbohydrates. Although helpful in reducing calories and the effect on your blood glucose, sugar alcohols are not completely calorie-free and may cause a laxative effect or other intestinal symptoms in some people.
Along with carbohydrates, do not forget to include proteins as well as fats to balance your meals, manage your body weight, and control your blood glucose levels most effectively. If your goal is to lose weight, the calories you consume must be less than the calories your body uses for basic functions, daily activities, and exercise. If some of your diabetes medications are causing you to gain weight (or keeping you from losing weight), talk to your health care provider about which medications may help you lose weight while controlling your blood glucose.
Focusing on Physical Activity
Exercise plays a pivotal role in preventing as well as managing diabetes. Potentially of even greater importance is the role that exercise can play in preventing the complications often associated with diabetes; the benefits of exercise for those who have diabetes are well documented (12, 45). Health care providers often prescribe exercise for type 1 and type 2 diabetes in conjunction with medication, or exercise alone for type 2 diabetes (16). Exercise can not only improve blood glucose levels and glycated hemoglobin or HbA1c levels (see Blood Glucose Control and A1c), but also reduce blood pressure and cholesterol levels, decrease the risk of heart disease, promote weight loss, improve brain function, and enhance self-image. Exercise may also reduce the amount of oral diabetic medications or the amount of insulin you require (3). Exercise needs to be continued to be effective; once it is suspended, the physiological benefits related to the control of blood glucose are lost within days (25).
Type 1 diabetes requires that blood glucose levels be fairly well controlled before exercise (46). When glucose levels are poorly controlled, the liver’s production of glucose increases, which can result in higher blood glucose levels during exercise. Higher blood glucose levels can also occur transiently after very intense exercise, such as sprinting or heavy resistance training (47). When blood glucose levels are controlled, moderate-intensity exercise can reduce blood glucose by increasing blood flow to the muscles, which increases the rate of glucose absorption into the cells (20).
Blood Glucose Control and A1c
Hemoglobin is a protein found inside red blood cells that carries oxygen around the body. When blood glucose levels are high (as with diabetes), hemoglobin links with glucose that enters the red blood cells. This is referred to as glycated hemoglobin or HbA1c (or commonly just A1c) (2). The higher the glucose levels in the blood are, the greater the A1c percentage is. Since red blood cells have a limited lifespan, looking at A1c levels can give a picture of the average glucose control over two to three months. A1c cannot be used to check short-term glucose levels (you need to use your blood glucose meter for those checks) but rather gives more of an overall picture. The A1c for someone without diabetes is 4 to 6 percent, but in those with diabetes it can be elevated to 10 percent or higher if glucose levels are out of control. Your health care provider will help you establish a target value; generally, well-controlled glucose is evident by an A1c less than 7 percent. Exercise is particularly important in improving A1c levels. In general, for every 1 percentage point drop in A1c, you can reduce the microvascular complications that affect the eyes, kidneys, and nerves by 40 percent (4).
Type 2 diabetes involves dual defects in insulin action (i.e., manner in which insulin helps cells take up glucose from the blood) and insulin secretion (i.e., body’s ability to secrete insulin) (2). Exercise plays a major role in the control of type 2 diabetes (15). Being active significantly improves insulin action, and it decreases the amount of insulin needed for your body to lower blood glucose levels. Even in insulin users, improved insulin action can lead to decreases in the amount of insulin needed (46). Weight loss can also decrease abdominal fat, which can further improve insulin action and overall blood glucose levels.
Exercise is also well known to help prevent the onset of diabetes. People who have prediabetes and a family history of diabetes should focus on both diet and exercise to promote weight loss as a way to prevent type 2 diabetes. In one well-known study, the Diabetes Prevention Program, people who had a high probability of developing diabetes reduced their risk by 58 percent as a result of lifestyle interventions that included daily exercise, changes in diet, and average weight loss of about 12 pounds (5.4 kg) (32).
Precautions for Exercise
Do you need to see your doctor before you start to exercise? To determine this, follow preparticipation screening recommendations (see figures 2.1 and 2.2). In general, medical clearance is recommended if you have any signs or symptoms of disease, if you haven’t been regularly active (even if you have no signs or symptoms of disease), or if you are desiring to increase your current exercise program from moderate to vigorous intensity (36). Whether you need medical clearance before beginning or whether the screening in chapter 2 indicates that this is not necessary, recognize the value of regular moderate to vigorous activity in actually reducing your risk of a heart attack (even if you have already had one) while realizing and respecting your limitations (15, 40).
If you have preexisting microvascular disease complications (eye, kidney, or nerve disease) or macrovascular disease (disease of the large blood vessels, such as those of the heart), you should not start a vigorous exercise program without being evaluated by a health care professional first. Your doctor may want you to have a cardiac stress test (i.e., treadmill test during which your heart rhythm is monitored) before exercising, particularly if you (15)
· are planning on participating in vigorous activities, not just easy or moderate ones;
· are over 40 years old (or over 30 if any of the following apply to you);
· have had diabetes for more than 10 years;
· have heart disease, a strong family history of heart disease, or high cholesterol;
· have poor circulation in your feet or legs (or lower leg pain while walking);
· have diabetic eye disease; kidney disease; numbness, burning, tingling, or loss of sensation in your feet; or dizziness when going from sitting to standing;
· have not consistently controlled your blood glucose levels well; or
· have any other concerns about exercising, including joint pain, arthritis, or other chronic health problems.
Some medical conditions related to diabetes may also influence exercise choices, including diabetic retinopathy, peripheral neuropathy, and nephropathy. Annual dilated eye exams done by an ophthalmologist can determine if you have any eye problems and should be considered before the start of a vigorous exercise program (5). Diabetic retinopathy is a disease affecting the retina of the eye. If this disease is present, certain activities should be avoided to prevent further damage (15). Mild background retinopathy will not affect your exercise choices, but if you have moderate nonproliferative diabetic retinopathy you will need to avoid exercises that unduly affect blood pressure (e.g., heavy resistance training) (16). Avoid contact sports and heavy lifting if you have severe nonproliferative retinopathy. Anyone with unstable proliferative diabetic retinopathy should focus on low-impact cardiorespiratory exercises like walking, swimming, and stationary cycling, and people should never do any exercise if they have a retinal hemorrhage.
Water-based activities can provide low-impact aerobic conditioning.

Another potential concern is peripheral neuropathy, which is nerve damage that can alter the sensation of the hands and feet as well as your balance (17). Falls are more common with this condition, as are joint and soft tissue injuries. Proper footwear is a must to prevent blisters or ulcers. Inspect your feet both before and after exercise for blisters or ulcers, using a mirror placed on the floor under your foot if that makes it easier for you to see. If you have had foot ulcers or foot deformities, schedule an appointment with a podiatrist to be measured for shoes that fit well. Lower-impact activities, such as swimming and stationary biking, are preferred in these cases to limit complications, although aquatic activities are not an option with unhealed ulcers (17).
Precautions for Exercising With Diabetes
Having diabetes and engaging in physical activity requires some precautions to make sure that exercise is safe and effective. Follow these guidelines to get the most out of being active with diabetes:
· Have a blood glucose meter accessible to check your glucose level before, possibly during, and after exercise, or if you have any symptoms of low blood glucose.
· Immediately treat any hypoglycemia during or following exercise with quickly absorbed carbohydrates like glucose tablets, dextrose-based candy, or regular soft drinks.
· Inform your exercise partners about your diabetes, and show them how to give you glucose or another carbohydrate should you need assistance.
· Stay properly hydrated with frequent intake of small amounts of cool water, and take in adequate fluids before exercising, particularly if your blood glucose levels are elevated.
· Consult with your physician before exercising with any of the following conditions:
o Proliferative retinopathy or active retinal hemorrhage (eye disease)
o Neuropathy (nerve damage), either peripheral or autonomic
o Foot injuries (including ulcers)
o High blood pressure
o Serious illness or infection
· Seek immediate medical attention for chest pain or any pain that radiates down your arm, jaw, or neck and for serious indigestion, any of which may indicate a lack of blood to your heart and a possible heart attack.
· If you have high blood pressure, avoid activities that cause blood pressure to go up dramatically, such as heavy weight training, head-down exercises, and anything requiring breath holding.
· Wear proper footwear and check your feet daily for signs of trauma, such as blisters, redness, or other irritation.
· Immediately stop exercising if you experience bleeding into your eyes caused by active, unstable proliferative retinopathy.
· Wear a diabetes medic alert bracelet or necklace with your physician’s name and contact information on it.
· Carry a cell phone with you so that you can call someone for assistance if needed.
Since diabetes may also result in nephropathy (kidney damage), a kidney evaluation before starting an exercise program is suggested. One sign of kidney damage is the presence of proteins in the urine. Kidney damage can be exacerbated by strenuous activity because of the sudden increases in blood pressure, leading to further damage to kidney function (29). Blood pressure medications called angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers protect kidney function and may be considered when one is faced with these conditions (24).
Effects of Blood Glucose on Exercise: Hypoglycemia
What you eat and when you eat are especially important for managing your glucose levels during exercise. Exercise itself helps to move glucose from the blood into the working muscles, but this also opens the possibility of blood glucose dropping too low. This is referred to as hypoglycemia (hypo- means low, and glycemia refers to blood glucose). Symptoms of hypoglycemia are as follows:
Shakiness
Weakness
Abnormal sweating
Heart palpitations (fast heart rate)
Nervousness
Anxiety
Tingling of the mouth and fingers
Hunger
Headache
Visual disturbances
Mental dullness
Confusion
Seizures
Coma
Checking your blood glucose on a regular basis is key to managing your diabetes and ensuring safety when exercising. Handheld glucose meters require only a small drop of blood and provide an immediate digital reading of your blood glucose level (see figure 13.1 for an example of a glucose monitor). Make a habit of checking your glucose before and after exercise.
Figure 13.1 Glucose monitors provide quick feedback on blood glucose levels.

Although avoiding hypoglycemia is the goal, at times your blood glucose levels may drop. Always have some easily absorbed sources of glucose with you. When glucose levels are low (less than 70 mg/dL), consume a glucose-containing product that will rapidly become available in your blood (e.g., glucose tablets, hard candies, regular soda, or juice). Since fat and protein slow down the movement of glucose from the intestine into the blood, other snacks such as peanut butter and crackers or granola bars are better to use once glucose levels have risen or to prevent a later drop. To avoid overshooting and becoming hyperglycemic, a general recommendation is to consume 15 to 20 grams of carbohydrate and then wait 15 minutes to see how much your blood glucose level rises (13). If your glucose is still low, repeat the process. Letting those with whom you exercise know about your diabetes is important just in case your glucose levels drop so low that you become unconscious. If this happens, they can call for emergency assistance.
To avoid hypoglycemia, be consistent with your carbohydrate intake with regard to meal timing and exercise. Maintaining a regular time of day for your exercise routine is also helpful, and monitoring your blood glucose before and after exercise is a good idea especially if you take insulin or other oral medications that stimulate insulin release. If your exercise bout is prolonged, you may also want to check your blood glucose level during exercise if possible. Keeping blood glucose between 100 and 250 mg/dL (and no higher) optimizes safety by helping you avoid both hypoglycemia and hyperglycemia (14).
In individuals taking insulin or oral medications that increase the body’s insulin secretion, physical activity can cause hypoglycemia if medication dose or carbohydrate consumption is not altered. Individuals on these therapies may need to ingest some added carbohydrate if preexercise glucose levels are <100 mg/dL (5.6 mmol/L), depending on whether they can lower insulin levels during the workout (e.g., with an insulin pump or reduced preexercise insulin dosage), the time of day exercise is done, and the intensity and duration of the activity. Hypoglycemia is less common in diabetic patients who are not treated with insulin or medications that cause insulin release, and no preventive measures for hypoglycemia are usually advised in these cases. Intense activities may actually raise blood glucose levels instead of lowering them (2).
You should also take special care if you exercise later in the day due to the potential for hypoglycemia to occur following the exercise session after you have gone to bed for the night, especially if you use insulin. Delayed-onset hypoglycemia is a phenomenon that typically occurs 6 to 15 hours after exercise (36). It appears to be a result of the liver and muscles replenishing their glucose stores after exercise. This underscores the need to monitor your blood glucose during that time and to eat an extra snack if necessary. If you need a snack, it should contain both carbohydrate (about 15 grams) and protein (7 to 8 grams) to have a more lasting effect (30). Consult with your health care provider to solidify your plan of action based on your type of diabetes as well as the medications you are taking.
If you take insulin or are on a medication that stimulates insulin release (e.g., sulfonylureas or meglitinides; see table 13.4 later in this chapter for more information), be sure to check your glucose level before exercise. If your blood glucose level is low before an exercise bout (less than 100 mg/dL), you may need to consume some carbohydrate to avoid hypoglycemia during exercise, especially if you use insulin; but this really depends on how you manage your insulin doses and timing and the type of activity you do (47). Depending on the duration and intensity of your exercise session, you may need to take in additional carbohydrate and other food before, during, and after exercise to prevent hypoglycemia (14, 31).
On the opposite end of the spectrum from hypoglycemia is hyperglycemia, or high blood glucose. With type 1 diabetes, if your blood glucose is elevated (greater than 250 to 300 mg/dL), you may need to postpone or at least decrease the intensity of the exercise session (see figure 13.2 for a decision-making flowchart). You can base your decision on how you are feeling as well as whether you have ketones in your urine. Ketones make your blood more acidic, potentially causing ketoacidosis, a condition that, if ignored, can cause coma and death (see What Is Diabetic Ketoacidosis, and How Can I Avoid It? for more information). Ketoacidosis is more commonly found with type 1 diabetes than with type 2 diabetes.
Q&A
What is diabetic ketoacidosis, and how can I avoid it?
When your blood glucose levels remain elevated, the glucose needed for energy cannot enter your cells. As a result, fat is used for energy, resulting in the production of ketones (acids), which first build up in the blood and eventually also appear in the urine. You can check for ketones with a simple at-home urine test.
Situations that may result in ketones include insufficient insulin or inadequate calorie intake. Usually, ketoacidosis develops slowly, but if you become sick and are vomiting, it could develop within a few hours. Early signs include thirst or a dry mouth, frequent urination, high glucose levels, and high ketones in the urine. Over time other symptoms may appear, including constant feelings of tiredness, dry or flushed skin, nausea or vomiting, fruity-smelling breath, and confusion. Diabetic ketoacidosis is a serious medical condition, and if you have these signs or symptoms, drink plenty of water and contact your health care provider immediately (10).
Figure 13.2 Decision-making flowchart for exercise for people with type 1 diabetes.
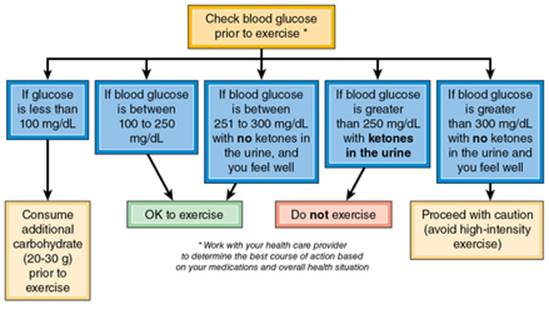
The American Diabetes Association suggests the following general guidelines to help keep your glucose levels in check (3):
· Avoid physical activity if your blood glucose is greater than 250 mg/dL and you have ketones in your blood or urine.
· Use caution if your glucose is above 300 mg/dL even if ketones are not present.
If your blood glucose level is elevated but you find no ketones in your urine and you feel well, then moderate-intensity exercise is appropriate and may actually be helpful in lowering your blood glucose level. However, if you have ketones in your urine, you should postpone exercise and contact your health care provider if you have not already established a response plan for such situations. Often, treatment includes the administration of insulin to regain normal glucose levels, along with adequate hydration (10).
For type 2 diabetes, additional carbohydrate is not typically needed before exercise because hypoglycemia is not common unless one is being treated with insulin or insulin-stimulating medications (see the previous recommendations on carbohydrate consumption if these medications are included in your treatment plan). Other medications (e.g., metformin, thiazolidinediones, and alpha-glucosidase inhibitors) do not tend to cause hypoglycemia and thus do not require that you take in additional carbohydrate. With regard to hyperglycemia and type 2 diabetes, when ketones are present, vigorous exercise should be avoided. However, light to moderate exercise may actually help lower your blood glucose levels, especially if the high glucose level occurs after a meal (18). The American Diabetes Association suggests that as long as you feel well, are adequately hydrated, and have no ketones in your urine, it is not necessary to postpone exercise based on hyperglycemia alone. To optimize your safety when exercising, discuss your medical situation, including the medications you are taking, with your health care provider so you will know what steps are most appropriate for you.
Physical Activity Recommendations
All physical activity you do during the day counts toward your daily total. Until recently, it was believed that vigorous exercise was required for optimal health and fitness. While you may stand to gain more health benefits from harder workouts, almost any activity (including golfing, gardening, mowing the lawn, moderate walking) done for 30 to 45 minutes per day is also beneficial to your health. Furthermore, lower-intensity exercises are beneficial even if you do them for only 10 minutes at a time. The latest research shows benefits from simply breaking up sedentary time with any activity, even standing, once in a while (19). Start by standing up or walking around for 5 minutes after each hour that you spend doing something sedentary.
Exercise comes in many forms, and your structured exercise program should be tailored to your situation. Although your age and type of diabetes may call for different exercise programs, the goal is the same—to improve health outcomes. Following appropriate screening and armed with blood glucose monitoring skills, you are ready to get started. A complete exercise program should include aerobic activities, resistance training, and flexibility exercise, and even some balance training if you are over 40 years old.
Aerobic Exercise
Aerobic activities, which help improve the efficiency of the cardiovascular system, can be beneficial for regulating blood glucose levels. Examples include walking, jogging, swimming, and biking. If you cannot do weight-bearing or high-impact activities, chair exercises, water aerobics, and recumbent biking can be beneficial. Table 13.1 presents recommendations for type 1 and type 2 diabetes based on the FITT principle discussed in chapter 5, which addresses frequency, intensity, time, and type of activities (11, 15).
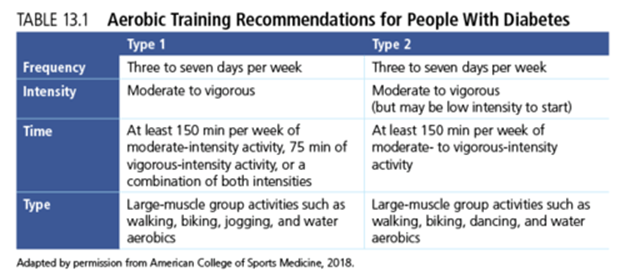
Working up to daily aerobic activity has benefits for both type 1 and type 2 diabetes (7, 27). For people with type 1, daily physical activity helps maintain the balance between insulin doses and food consumed. For those with type 2 diabetes, the focus is on burning calories and weight management, but improving overall fitness levels is also important for long-term health. Keep in mind that the recommendations in table 13.1 are targets, not initial levels. If you are just starting out, begin gradually because your body needs to adapt to the exercise, and you also have to monitor how your blood glucose levels are affected. Consult chapter 5 for suggestions on beginning or advancing in your aerobic training program.
Resistance Training
Resistance training can lower A1c levels and confer other health benefits as well (see chapter 6 for more details on resistance training) (28). Including both aerobic exercise and resistance training can optimize the benefits related to managing your glucose levels (15, 21). A few precautions do need to be mentioned. If you have microvascular disease, be aware of the potential concerns about damage to the eyes, kidneys, and joints. Straining while lifting weights can lead to an increased risk of bleeding and retinal detachment for those with proliferative and severe nonproliferative eye disease. Resistance training may not be appropriate if you have unstable diabetic retinopathy. Also, be careful if you have nerve involvement; you are more susceptible to foot ulcers and bone damage because of the lack of sensation and weakening of the muscles and ligaments in the foot. If you have nephropathy (kidney damage) related to diabetes, strenuous activity can increase protein excretion. With these precautions in mind, you can implement a safe and effective resistance training program. Increasing your muscle mass while reducing fat tissue can decrease insulin resistance and improve blood glucose control. Having stronger muscles can also improve your balance, posture, ability to move, and daily functions.
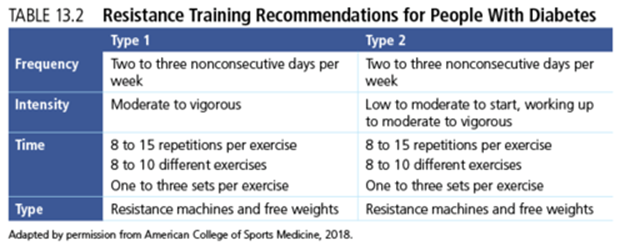
The goal of resistance training is to focus on exercises involving the major muscle groups including the legs, back, chest, arms, shoulders, thighs, and abdominal area. Table 13.2 provides resistance training recommendations for type 1 and type 2 diabetes based on the FITT principle (15). Details regarding the many exercise options for resistance training are in chapter 6.
Flexibility
Flexibility is also an integral part of an exercise program for people with diabetes (26). Typically, static stretching is recommended. This involves placing the body into a position that creates tension in the muscles and holding that position for 15 to 30 seconds. Dynamic stretching done during movement can also work. Table 13.3 provides flexibility recommendations for persons with any type of diabetes based on the FITT principle (15). Details regarding stretching are found in chapter 7.

Balance Training
Particularly if you are middle-age or older, you will want to add one more activity to your weekly routine: functional fitness training that includes elements of balance training (23). Everyone starts to lose some natural balance with aging, but having diabetes can accelerate the loss and increase your risk of falling and losing your ability to live independently well into your later years (38). If you lose any of the feeling in your feet, this can alter the way you walk (your gait) and increase your risk, and having autonomic neuropathy that makes you dizzy when you stand up also raises your risk. Balance training can be as simple as practicing standing on one leg at a time. Resistance training that works the lower body or the core muscles improves your ability to balance while standing and walking. In addition, flexibility exercises that work the full range of motion around your joints can improve balance, as well as some alternative activities like tai chi and yoga. Even taking up dancing can help you stay on your feet at any age.
Influence of Medications
Diabetes can be controlled with the appropriate use of medications, including oral and injected medications (for type 2) as well as insulin injections (for type 1 mainly but also for some with type 2). A general understanding of how these medications work will help you see how they can fit into your total treatment plan.
Oral and Injected Medications for Type 2 Diabetes
Oral medications are the most common treatment for type 2 diabetes, but a few newer ones are taken by injection. In some situations, insulin, or a combination of insulin and other diabetes medications, is used to better control blood glucose levels (34, 42).
Several classes of medications are used to treat type 2 diabetes. Table 13.4 includes general information on how the medications work as well as some special considerations. As with all medications, there are side effects as well as situations in which certain medications may not be appropriate. Some of these issues are outlined in table 13.4.
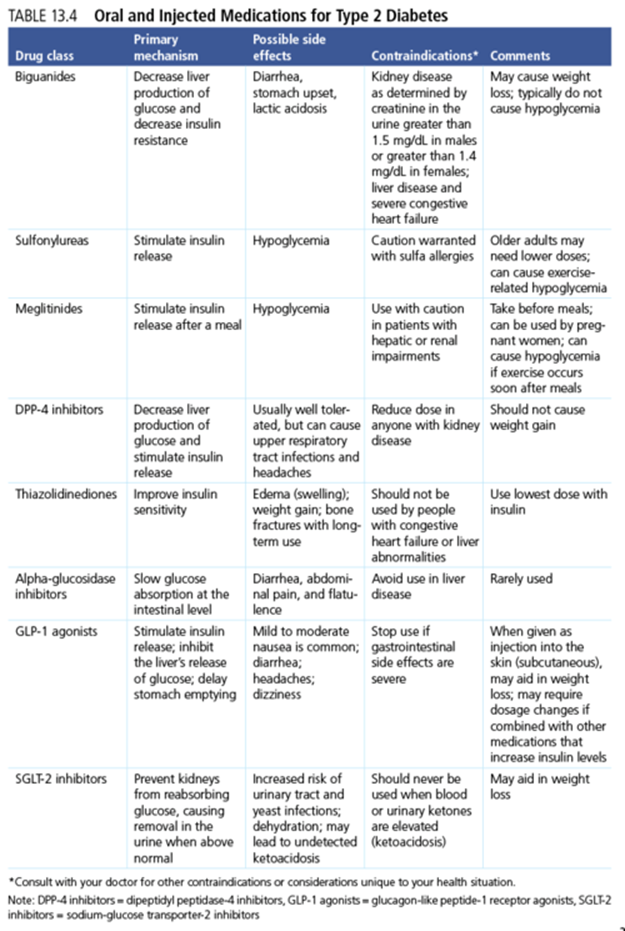
For optimal outcomes, becoming more physically active and making other healthy lifestyle changes should be in conjunction with medication use. Exercise can contribute to weight loss, which can decrease insulin resistance and improve glucose tolerance. Exercise also increases insulin sensitivity and makes the body work more efficiently. In most people with well-controlled type 2 diabetes, most medications do not need to be adjusted for exercise. However, two classes of diabetes medications to watch closely are the sulfonylureas and the meglitinides, both of which can cause hypoglycemia (41). Insulin use also increases the risk of hypoglycemia. Discuss your exercise program with your health care provider to see if any of these medications need to be reduced on the days you exercise.
Frequent monitoring of blood glucose levels before, during, and after exercising is important to avoid potential problems (22). When you are exercising and losing weight, your overall medication doses may need to be decreased or discontinued. Work with your health care provider to adjust your medications (especially insulin if that is part of your treatment plan), instead of snacking and taking in more calories to prevent or treat hypoglycemia. When you are trying to lose weight, having to eat more to balance your glucose level will sabotage your efforts. Instead, enjoy the benefit of exercise for your body and be pleased that you have taken positive steps to decrease your reliance on medications.
Insulin Options for Diabetes
A number of types of insulin are used to treat type 1 and type 2 diabetes. Insulin must be injected; it cannot be consumed orally, although a new inhaled insulin (Afrezza) has been approved for use in people with type 2 diabetes. Insulin taken to provide background levels is called basal insulin, and what you use to cover meals or snacks is bolus insulin. One other option for delivering insulin is to use an insulin pump programmed to deliver basal and bolus doses.
Q&A
What is an insulin pump, and how does it work?
Insulin pumps are small devices that are attached either directly to the body or indirectly via a tube (figure 13.3) to deliver insulin continuously throughout the day in a way intended to mimic the natural activity of the pancreas. Insulin levels can be adjusted up (when one is eating) or down (when one is being active) with a couple of button pushes. This gives users more flexibility with respect to timing meals as well as engaging in activity. For physically active people, the ability to more precisely administer insulin and reduce levels during and following exercise can make it easier to avoid hypoglycemia (13). In addition, the pump takes the place of separate insulin vials and syringes so it is much simpler to handle, especially for active, on-the-go people and youth.
Figure 13.3 Insulin pumps are an alternate way to deliver insulin throughout the day.

The types of insulin are grouped based on their onset of action, time of peak activity, and duration of activity in the body. Details on these characteristics and common brands are listed in table 13.5. In general, rapid-acting and short-acting insulins have a relatively quick onset and time of peak action. These types of insulin are taken before meals and often need to be adjusted before exercise. The extent to which insulin should be decreased depends on the intensity of exercise. If activity occurs within 2 hours of eating, premeal insulin should be decreased 5 to 30 percent (5 percent for low-intensity exercise and 30 percent for high-intensity and long-duration exercise) (13). Intermediate-acting insulin has a longer onset of action as well as longer duration. Unless you are engaging in prolonged exercise, intermediate-acting insulin often does not need to be adjusted. Long-acting basal insulin does not have much of a peak; rather, it provides a low but constant level of insulin for 24 hours or longer (depending on the type). Like intermediate-acting insulin, long-acting insulin may or may not need to be adjusted for exercise (before or afterward).

Exercise is not recommended during peak insulin times unless doses are lowered before exercise or you eat extra carbohydrates to compensate (13, 14). The combination of the high levels of insulin and the glucose-lowering effect of exercise can lead to hypoglycemia unless you make adjustments. By monitoring your blood glucose levels (before, during, and after exercise), you can make additional adjustments to your food intake and insulin.
Regular exercise and a sound nutritional plan are the two cornerstones of managing and thriving with diabetes. Your individualized exercise program should include aerobic activity as well as resistance training, stretching, and possibly balance training. Your exercise program should improve your health and blood glucose control without worsening or causing health-related complications. A health care provider or diabetes educator can be helpful with regard to making adjustments in medications and insulin when you are starting or expanding your exercise program. In addition, diet is a key part of managing blood glucose levels effectively. With type 1, balancing your intake of carbohydrate, fat, and protein will help you with sustained blood glucose control. With type 2 diabetes, attention to calories consumed is an asset for weight loss. A better diet is an essential complement to your exercise program to achieve the greatest possible control over your diabetes and your overall health.