GENERAL PRINCIPLES
Sarcomas (from the Greek sarx for flesh) are a rare group of malignancies of the connective tissue. They represent over 100 different histologies of tumors derived from the mesenchymal or ectodermal germ layers. The presenting signs and symptoms depend on the anatomic site of origin and can vary markedly. In general, sarcomas can be divided into two large groups: soft tissue tumors and bone tumors.
Epidemiology
Sarcomas are rare tumors, comprising 1% of adult malignancies and 7% of pediatric malignancies. Sarcomas occur with equal frequency in both genders.1 In the United States in 2010, the estimated incidence of soft tissue sarcomas (STSs) and bone sarcomas is 13,170 cases per year, with 5380 deaths expected.1 Compared to other rare tumors, sarcomas carry a high mortality rate.
Risk Factors
Most cases of sarcoma are sporadic; however, a number of etiologic factors have been identified, as detailed below.
![]() Radiation
Radiation
Sarcomas have been found to originate in or near tissues that have received prior external-beam radiation therapy and tend to develop at least 2 years after radiation therapy, but can develop decades after radiation.2–4 The majority of these lesions are high grade, and they are typically osteosarcomas, malignant fibrous histiocytomas, and angiosarcomas. The relative risk of radiation-induced sarcoma is 0.6 for patients that receive 10 Gy of radiation and 38.3 for patients that receive 60 Gy.5
![]() Chemical exposure
Chemical exposure
Thorotrast, an IV contrast dye, has been found to cause hepatic angiosarcomas.6 Other agents such as vinyl chloride,7 arsenic,8 and dioxin in chemical workers and farmers but not in Vietnam Veterans (i.e., dioxin is in Agent Orange) has also been linked to sarcomas.9 Alkylating chemotherapy, particularly when used to treat childhood malignancies, has also been associated with the development of sarcomas in adulthood.5
![]() Genetic conditions
Genetic conditions
Patients with neurofibromatosis type I have a 10% risk of developing a malignant peripheral nerve sheath tumor.10 Sarcomas also occur in patients with Li-Fraumeni syndrome.11 Familial retinoblastoma is linked to the development of osteosarcoma5 and Werner syndrome is a risk factor for multiple types of sarcomas.12
![]() Other risks associated with sarcomas
Other risks associated with sarcomas
Lymphangiosarcomas have been known to develop in a lymphedematous arm after mastectomy (Stewart-Treves syndrome).13 Kaposi sarcoma is associated with co-infection with the human immunodeficiency virus and the human herpes virus 8.14 Paget disease of bone is a risk factor for the development of osteosarcoma or fibrosarcoma.15
SPECIAL CONSIDERATIONS
The treatment of sarcoma is complex because sarcoma is an ever growing group of many very rare diseases that are historically treated as large group in clinical trials. As many of specific subtypes are driven by known translocations, the treatment and understanding of each individual subtype is rapidly evolving.16–18 Translocation-based treatment of sarcoma is the reason patients with sarcomas should be treated by physicians that specifically sub-specialize in the treatment of sarcoma.
SOFT TISSUE SARCOMAS
DIAGNOSIS
Clinical Presentation
Soft tissue sarcomas represent greater than 75% of all sarcomas diagnosed each year.1 Patients typically present with an asymptomatic mass. Pain may be present if there is entrapment of neurovascular structures or involvement of bone. Sarcomas may grow quite large before they become obvious on physical exam.19
![]() Extremity sarcomas
Extremity sarcomas
Approximately half of all soft tissue sarcomas arise in the extremities. The majority are first seen as a painless soft tissue mass.
![]() Retroperitoneal sarcomas
Retroperitoneal sarcomas
Most patients have an abdominal mass and approximately half have abdominal pain that is vague and nonspecific. Weight loss is seen less frequently, with early satiety, nausea, and emesis occurring in <40% of patients. Neurologic symptoms, particularly paresthesia, occur in up to 30% of patients.20,21
Physical Examination
Physical examination of a patient presenting with a soft tissue mass should include an assessment of the size of the mass and its mobility with respect to the underlying tissue. If a mass is >5 cm and deep, it should be presumed to be sarcoma until proven otherwise. High-grade sarcomas may have significant necrosis and can be confused with a hematoma or abscess. A site-specific neurovascular examination should also be performed.
Differential Diagnosis
The differential diagnosis includes benign soft tissue tumors as well as carcinoma, lymphoma, and melanoma. The most common benign tumors include lipoma, desmoid tumor, neurofibroma, hemangioma, and schwannoma.
Diagnostic Testing
Imaging
Patients with masses suspicious for sarcoma should undergo radiologic evaluation and biopsy. The studies needed for adequate staging vary depending on the site of disease. Sarcoma of the head and neck or extremities should be evaluated with plain films and MRI. Plain films may reveal soft tissue mineralization (which is typical for synovial sarcoma) or may reveal skeletal reaction to the tumor. MRI is valuable for assessing fat and distinguishing it from surrounding tissues. This may assist in the diagnosis of the lesion and allows for planning of the biopsy and subsequent surgery. For retroperitoneal and abdominal sarcomas, CT is the imaging modality of choice, as this provides the best anatomic definition of the tumor.
In addition to evaluating the primary lesion with imaging, distant metastatic disease may also be assessed. STS spreads hematogenously, and the lung is the most common site of metastasis. Chest x-ray may be sufficient for small, low-grade lesions, but in patients with high-grade tumors or tumors larger than 5 cm, a staging CT of the chest should be performed.
Diagnostic Procedures
![]() An accurate biopsy diagnosis is essential for STS. Any lesion >5 cm or any rapidly growing lesion should be biopsied. The placement of the biopsy tract is also critical, as it can be seeded with tumor and must be excised at the time of resection. Generally, the preferred technique is open incisional biopsy performed by a surgeon with experience in resection of STS. Hemostasis is also very important, as a hematoma may require enlarging radiation fields or may interfere with resection planning.
An accurate biopsy diagnosis is essential for STS. Any lesion >5 cm or any rapidly growing lesion should be biopsied. The placement of the biopsy tract is also critical, as it can be seeded with tumor and must be excised at the time of resection. Generally, the preferred technique is open incisional biopsy performed by a surgeon with experience in resection of STS. Hemostasis is also very important, as a hematoma may require enlarging radiation fields or may interfere with resection planning.
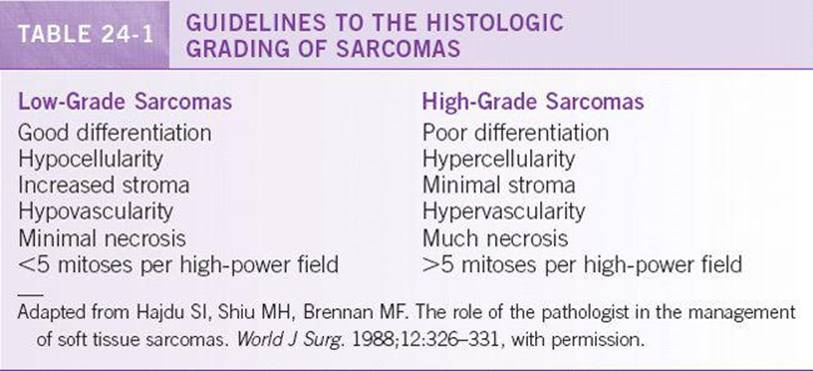
![]() Histologic evaluation should be performed at an experienced center, as grade is critically important to determining prognosis. STSs are named for their tissue of origin based on light microscopy examination, and there are many possible histological types (Table 24-1). Tumors are also carefully evaluated for grade, which takes into account cellularity, mitotic activity, nuclear atypia, and necrosis. In general, the grade, size, and depth are more important factors than the histologic type. Immunohistochemistry and FISH studies are used to subclassify STS. The three most common types of STS are malignant fibrous histiocytoma, liposarcoma, and leiomyosarcoma.
Histologic evaluation should be performed at an experienced center, as grade is critically important to determining prognosis. STSs are named for their tissue of origin based on light microscopy examination, and there are many possible histological types (Table 24-1). Tumors are also carefully evaluated for grade, which takes into account cellularity, mitotic activity, nuclear atypia, and necrosis. In general, the grade, size, and depth are more important factors than the histologic type. Immunohistochemistry and FISH studies are used to subclassify STS. The three most common types of STS are malignant fibrous histiocytoma, liposarcoma, and leiomyosarcoma.
TREATMENT
Early-Stage Disease (Stages I to III)
![]() Extremity soft tissue sarcomas
Extremity soft tissue sarcomas
![]() Surgery. Surgery is the mainstay of therapy for early-stage STSs of the extremities. Sarcomas grow along planes and grossly appear to be well encapsulated. However, they usually extend into the pseudocapsule (an area around the tumor that is composed of tumor fimbriae and normal tissue), and “shelling-out” of lesions is associated with high local recurrence rates, 37% to 63%. In the past, radical excision and amputation were utilized to avoid this problem. Over the past 20 years, there has been a gradual shift in the surgical management of extremity soft tissue sarcomas away from radical ablative surgery toward limb-sparing surgery. Amputation is only required in [H33522] 5% of patients today.
Surgery. Surgery is the mainstay of therapy for early-stage STSs of the extremities. Sarcomas grow along planes and grossly appear to be well encapsulated. However, they usually extend into the pseudocapsule (an area around the tumor that is composed of tumor fimbriae and normal tissue), and “shelling-out” of lesions is associated with high local recurrence rates, 37% to 63%. In the past, radical excision and amputation were utilized to avoid this problem. Over the past 20 years, there has been a gradual shift in the surgical management of extremity soft tissue sarcomas away from radical ablative surgery toward limb-sparing surgery. Amputation is only required in [H33522] 5% of patients today.
![]() Radiation therapy. Wide local excision alone is all that is necessary for small (T1), low-grade, STSs of the extremities, with a local recurrence rate of <10%. Adjuvant radiation therapy, however, is required in a number of situations: (a) virtually all high-grade extremity sarcomas, (b) lesions larger than 5 cm (T2), and (c) positive or equivocal surgical margins in patients for whom re-excision is impractical. When adjuvant radiation is planned, metal clips should be placed at margins of resection to facilitate radiation field planning. Neoadjuvant radiation may be needed prior to definitive resection. This is most commonly performed for tumors that are borderline resectable or for tumors located adjacent to the joint capsule. A phase III National Cancer Institute of Canada trial comparing adjuvant (postoperative) and neoadjuvant (preoperative) radiation demonstrated similar local control rates, metastatic outcome, and overall survival rates between the two arms. However, patients receiving preoperative radiation had a significantly higher incidence of wound complications (35% vs. 17%).22
Radiation therapy. Wide local excision alone is all that is necessary for small (T1), low-grade, STSs of the extremities, with a local recurrence rate of <10%. Adjuvant radiation therapy, however, is required in a number of situations: (a) virtually all high-grade extremity sarcomas, (b) lesions larger than 5 cm (T2), and (c) positive or equivocal surgical margins in patients for whom re-excision is impractical. When adjuvant radiation is planned, metal clips should be placed at margins of resection to facilitate radiation field planning. Neoadjuvant radiation may be needed prior to definitive resection. This is most commonly performed for tumors that are borderline resectable or for tumors located adjacent to the joint capsule. A phase III National Cancer Institute of Canada trial comparing adjuvant (postoperative) and neoadjuvant (preoperative) radiation demonstrated similar local control rates, metastatic outcome, and overall survival rates between the two arms. However, patients receiving preoperative radiation had a significantly higher incidence of wound complications (35% vs. 17%).22
![]() Radiation as definitive therapy alone in the treatment of unresectable or medically inoperable soft tissue sarcoma patients yields a 5-year survival rate of 25% to 40% and a local control rate of 30%. Radiation doses should be at least 65 Gy, if feasible, given the site of the lesion.
Radiation as definitive therapy alone in the treatment of unresectable or medically inoperable soft tissue sarcoma patients yields a 5-year survival rate of 25% to 40% and a local control rate of 30%. Radiation doses should be at least 65 Gy, if feasible, given the site of the lesion.
![]() Brachytherapy also has been used in treatment for sarcomas. Iridium-192 is the most commonly used agent. It has similar local control rates to adjuvant external beam radiation and has the advantage of a decrease in the patient’s entire treatment from 10 to 12 weeks to 10 to 12 days. In addition, smaller volumes of tissues are irradiated, which may be useful if important structures, such as joints, are nearby.
Brachytherapy also has been used in treatment for sarcomas. Iridium-192 is the most commonly used agent. It has similar local control rates to adjuvant external beam radiation and has the advantage of a decrease in the patient’s entire treatment from 10 to 12 weeks to 10 to 12 days. In addition, smaller volumes of tissues are irradiated, which may be useful if important structures, such as joints, are nearby.
![]() Adjuvant chemotherapy. The benefit of adjuvant chemotherapy for extremity STSs is controversial. The only exception to this is rhabdomyosarcomas, in which adjuvant chemotherapy is accepted as standard of care.
Adjuvant chemotherapy. The benefit of adjuvant chemotherapy for extremity STSs is controversial. The only exception to this is rhabdomyosarcomas, in which adjuvant chemotherapy is accepted as standard of care.
![]() A formal meta-analysis of individual data from 1568 patients who participated in 13 trials was performed by the Sarcoma Meta-Analysis Collaboration. The analysis demonstrated a significant reduction in the risk of local or distant recurrence in patients who received adjuvant chemotherapy. There also was a decrease in the risk of distant relapse (metastasis) by 30% in treated patients. Overall survival, however, did not meet criteria for statistical significance between the control groupand adjuvant chemotherapy arm, with a hazard ratio of 0.89.23 Most of the randomized trials examined in this meta-analysis were limited by patient numbers, inclusion of all subtypes of STS and of low-grade tumors, heterogeneous patient and disease characteristics, and varied chemotherapy regimens.
A formal meta-analysis of individual data from 1568 patients who participated in 13 trials was performed by the Sarcoma Meta-Analysis Collaboration. The analysis demonstrated a significant reduction in the risk of local or distant recurrence in patients who received adjuvant chemotherapy. There also was a decrease in the risk of distant relapse (metastasis) by 30% in treated patients. Overall survival, however, did not meet criteria for statistical significance between the control groupand adjuvant chemotherapy arm, with a hazard ratio of 0.89.23 Most of the randomized trials examined in this meta-analysis were limited by patient numbers, inclusion of all subtypes of STS and of low-grade tumors, heterogeneous patient and disease characteristics, and varied chemotherapy regimens.
![]() Certain subgroups of patients, such as those with high-grade lesions, may benefit from adjuvant chemotherapy, but further studies are needed.
Certain subgroups of patients, such as those with high-grade lesions, may benefit from adjuvant chemotherapy, but further studies are needed.
![]() Retroperitoneal sarcomas
Retroperitoneal sarcomas
![]() Surgery. As with other soft tissue sarcomas, surgery is the primary treatment of retroperitoneal sarcomas. Tumors that are <5 cm and that not located close to adjacent viscera or critical neurovascular structures are considered resectable. If a tumor is thought to be a sarcoma and is resectable, a preoperative biopsy is not necessary. One should consider a preoperative CT-guided core biopsy if an incomplete resection is a reasonable possibility to allow neoadjuvant therapy.
Surgery. As with other soft tissue sarcomas, surgery is the primary treatment of retroperitoneal sarcomas. Tumors that are <5 cm and that not located close to adjacent viscera or critical neurovascular structures are considered resectable. If a tumor is thought to be a sarcoma and is resectable, a preoperative biopsy is not necessary. One should consider a preoperative CT-guided core biopsy if an incomplete resection is a reasonable possibility to allow neoadjuvant therapy.
![]() Unfortunately, only 50% of patients with early-stage retroperitoneal sarcomas are able to undergo complete surgical resection. Of the tumors removed, approximately half will develop a local recurrence. Adjuvant therapy, therefore, plays an important role in the management of retroperitoneal sarcomas.
Unfortunately, only 50% of patients with early-stage retroperitoneal sarcomas are able to undergo complete surgical resection. Of the tumors removed, approximately half will develop a local recurrence. Adjuvant therapy, therefore, plays an important role in the management of retroperitoneal sarcomas.
![]() Radiation therapy. Adjuvant radiation therapy is most frequently recommended for patients with high-grade tumors or positive margins. The radiation is typically started 3 to 8 weeks following surgery to allow wound healing. Two-year local control rates of 70% have been reported with the addition of postoperative radiation therapy. Neoadjuvant radiation therapy can be given to patients with marginally resectable tumors and to those in whom one would expect postoperative radiotherapy to be required. It has a number of advantages over postoperative radiotherapy including smaller radiation portals and reduction of the extent of the surgical procedure.
Radiation therapy. Adjuvant radiation therapy is most frequently recommended for patients with high-grade tumors or positive margins. The radiation is typically started 3 to 8 weeks following surgery to allow wound healing. Two-year local control rates of 70% have been reported with the addition of postoperative radiation therapy. Neoadjuvant radiation therapy can be given to patients with marginally resectable tumors and to those in whom one would expect postoperative radiotherapy to be required. It has a number of advantages over postoperative radiotherapy including smaller radiation portals and reduction of the extent of the surgical procedure.
![]() Management of unresectable, locally advanced retroperitoneal sarcomas. Unresectable retroperitoneal sarcomas can be managed in a number of ways. Radiation therapy can be given for palliation and with the hope that the tumor could be made resectable. Palliative surgery to reduce local symptoms can be performed. Chemotherapy can also be administered (see management of metastatic patients for specific regimens).
Management of unresectable, locally advanced retroperitoneal sarcomas. Unresectable retroperitoneal sarcomas can be managed in a number of ways. Radiation therapy can be given for palliation and with the hope that the tumor could be made resectable. Palliative surgery to reduce local symptoms can be performed. Chemotherapy can also be administered (see management of metastatic patients for specific regimens).
Stage IV Metastatic Soft Tissue Sarcomas
Metastatic STSs can be divided into limited metastasis and extensive metastasis. Limited metastatic disease is defined as resectable metastasis involving one organ system. The prognosis of these two subsets of patients is very different. It is possible to cure limited metastatic disease, whereas patients with extensive metastatic disease can only be palliated.
![]() Management of limited metastatic disease. For patients with a limited number of pulmonary metastases, metastasectomy has been performed with some improvement in survival compared with no surgery. In patients with visceral sarcomas and limited liver metastasis, it is sometimes possible to perform a metastasectomy by surgery, chemoembolization, or radiofrequency ablation.
Management of limited metastatic disease. For patients with a limited number of pulmonary metastases, metastasectomy has been performed with some improvement in survival compared with no surgery. In patients with visceral sarcomas and limited liver metastasis, it is sometimes possible to perform a metastasectomy by surgery, chemoembolization, or radiofrequency ablation.
![]() Management of extensive metastatic disease. The goal of therapy for patients with metastatic sarcoma is palliation and prolongation of survival. Cure is no longer a viable goal. Systemic chemotherapy is the primary modality of treatment. Radiation and surgery may be used with a goal of palliation.
Management of extensive metastatic disease. The goal of therapy for patients with metastatic sarcoma is palliation and prolongation of survival. Cure is no longer a viable goal. Systemic chemotherapy is the primary modality of treatment. Radiation and surgery may be used with a goal of palliation.
Numerous chemotherapy agents have been used as single agents or in combination for the treatment of soft tissue sarcomas. These include epirubicin, doxorubicin, ifosfamide, cyclophosphamide, dacarbazine, gemcitabine, and taxanes amongst others.
PROGNOSIS
![]() The most important prognostic factors for STS are size, grade, depth, and relationship to fascial planes. The American Joint Committee on Cancer (AJCC) staging system for STSs incorporates histologic grade (G), size of the primary (T), nodal involvement (N), and distant metastasis (M) (Table 24-2).24
The most important prognostic factors for STS are size, grade, depth, and relationship to fascial planes. The American Joint Committee on Cancer (AJCC) staging system for STSs incorporates histologic grade (G), size of the primary (T), nodal involvement (N), and distant metastasis (M) (Table 24-2).24
![]() Grade of the tumor is the predominant feature predicting early metastatic recurrence and death. Beyond 2 years of follow-up, the size of the lesion becomes as important as the histologic grade.
Grade of the tumor is the predominant feature predicting early metastatic recurrence and death. Beyond 2 years of follow-up, the size of the lesion becomes as important as the histologic grade.
![]() Nomograms exist for the relapse-free survival prediction by histology.
Nomograms exist for the relapse-free survival prediction by histology.
BONE SARCOMAS
GENERAL PRINCIPLES
Bone sarcoma may arise from any tissue within the bones. The most common bone sarcomas are osteosarcoma, chondrosarcoma, and Ewing sarcoma.
Classification
![]() Osteosarcoma
Osteosarcoma
Osteosarcoma is the most common primary bone tumor, accounting for 40% to 50% of bone sarcomas.25 It usually presents with pain and swelling. Approximately 60% occur in adolescents and children. Ten percent may occur in the third decade. There is a second peak in the fifth and sixth decades, which is frequently due to radiation-associated osteosarcomas or transformation of existing lesions. They are spindle cell neoplasms that produce bone and are more common in long bones. Most osteosarcomas occur in the metaphyseal region, near the growth plate, of skeletally immature long bones. The distal femur, proximal tibia, and proximal humerus are common sites. The majority is classified as “classic,” and this type is more common at between 10 and 20 years of age. Most of these lesions are high grade and highly vascular.
![]() Chondrosarcoma
Chondrosarcoma
Chondrosarcoma is the second most frequent malignant primary bone tumor, representing approximately 20% of bone sarcomas. They generally occur between the fourth and the sixth decades. They tend to develop in flat bones, including the shoulder and pelvic girdles. They may arise de novo or from preexisting lesions. They are indolent and are generally low grade. Chondrosarcoma may arise peripherally or centrally. Imaging studies may be bland, particularly in central lesions, which may make it difficult to distinguish between benign and malignant lesions. New pain, increasing size, and signs of inflammation point toward malignant lesions. In general, these malignancies are resistant to chemotherapy and radiation.

![]() Ewing sarcoma
Ewing sarcoma
Ewing sarcoma accounts for 10% to 15% of bone sarcomas, and incidence peaks in the second decade. It is the second most common malignant tumor of the bone in childhood and adolescence. It tends to occur in the diaphysis of long bones. The femoral diaphysis is the most common location. These are highly aggressive tumors and are best considered a systemic disease. A characteristic chromosomal translocation, t (11:22), is associated with this sarcoma and with peripheral primitive neuroectodermal tumor (PNET). Ewing sarcoma is one of the small, round, blue cell tumors.
DIAGNOSIS
An accurate tissue biopsy is needed for diagnosis. Imaging studies may be suggestive of tumor type; however, it can be difficult to distinguish benign and malignant bone tumors. Biopsy specimens are used to determine the histologic type of tumor as well as the grade. As with STSs, open incisional biopsy is preferred for bone sarcomas. The biopsy should be performed by a surgeon experienced in sarcoma so that it does not compromise the definitive surgical procedure.
Clinical Presentation
History
Localized pain and swelling are the hallmark clinical features of bone sarcomas. The pain is initially insidious but can become unremitting. Occasionally, a pathologic fracture will bring the patient to medical attention. If the tumor arises in the lower extremities, the patient may have a limp. Constitutional symptoms are rare but can be observed in patients with Ewing sarcoma or patients with metastatic disease. A pertinent history should note how long a lesion has been present and any change in it. Rapid growth or change in a lesion favors a malignant etiology.
Physical Exam
Physical exam may reveal a palpable mass. A joint effusion may be observed, and range of motion of the joint may be limited, with stiffness or pain. Neurovascular and lymph node examinations are usually normal.
Diagnostic Testing
Imaging
![]() Patients who are suspected to have bone sarcoma should undergo imaging studies, including plain films, MRI, and biopsy.
Patients who are suspected to have bone sarcoma should undergo imaging studies, including plain films, MRI, and biopsy.
![]() Plain films may demonstrate characteristic lesions for bone sarcoma. Osteosarcoma is associated with destructive lesions showing a moth-eaten appearance. In addition, a spiculated periosteal reaction and cuff of periosteal new bone may be seen. Plain films in chondrosarcoma show lesions with a lobulated appearance with punctate or annular calcification of cartilage. Ewing sarcoma is associated with an “onion peel” periosteal reaction and soft tissue mass. Metastatic disease may be associated with either osteolytic or osteoblastic lesions, depending on the type of primary malignancy.
Plain films may demonstrate characteristic lesions for bone sarcoma. Osteosarcoma is associated with destructive lesions showing a moth-eaten appearance. In addition, a spiculated periosteal reaction and cuff of periosteal new bone may be seen. Plain films in chondrosarcoma show lesions with a lobulated appearance with punctate or annular calcification of cartilage. Ewing sarcoma is associated with an “onion peel” periosteal reaction and soft tissue mass. Metastatic disease may be associated with either osteolytic or osteoblastic lesions, depending on the type of primary malignancy.
![]() MRI is the imaging modality of choice to evaluate the relationship of the tumor to surrounding structures and determine resectability. CT scan of the primary site may be considered in place of MRI to demonstrate cortical destruction more accurately and for evaluation of pelvic tumors. CT scan of the chest is used to evaluate for pulmonary metastases. Bone scan helps to evaluate for the local extent of the tumor as well as to evaluate for other lesions.
MRI is the imaging modality of choice to evaluate the relationship of the tumor to surrounding structures and determine resectability. CT scan of the primary site may be considered in place of MRI to demonstrate cortical destruction more accurately and for evaluation of pelvic tumors. CT scan of the chest is used to evaluate for pulmonary metastases. Bone scan helps to evaluate for the local extent of the tumor as well as to evaluate for other lesions.
Diagnostic Procedures
![]() Tissue biopsy, preferably open incisional biopsy, is essential for diagnosis.
Tissue biopsy, preferably open incisional biopsy, is essential for diagnosis.
![]() Bone sarcomas are staged using the American Joint Committee on Cancer staging system based on grade, tumor size, and metastatic disease as reported in Table 24-3. Adverse prognostic indicators include elevated lactate dehydrogenase (LDH), elevated alkaline phosphatase, and an axial primary. Patients with Ewing sarcoma should have bilateral bone marrow biopsies as part of staging.
Bone sarcomas are staged using the American Joint Committee on Cancer staging system based on grade, tumor size, and metastatic disease as reported in Table 24-3. Adverse prognostic indicators include elevated lactate dehydrogenase (LDH), elevated alkaline phosphatase, and an axial primary. Patients with Ewing sarcoma should have bilateral bone marrow biopsies as part of staging.
TREATMENT
The treatment of bone sarcoma is dependent on histologic subtype.
![]() General principles of local therapy
General principles of local therapy
![]() Surgical excision is the mainstay of treatment for patients with low-grade bone sarcomas. For high-grade tumors, multimodality therapy is indicated. As an example, for high-grade osteosarcomas, preoperative multiagent chemotherapy is followed by surgical removal of the tumor and then further adjuvant chemotherapy. Physical therapy and prosthetics are of great importance in these patients because of the highly invasive nature of the treatment.
Surgical excision is the mainstay of treatment for patients with low-grade bone sarcomas. For high-grade tumors, multimodality therapy is indicated. As an example, for high-grade osteosarcomas, preoperative multiagent chemotherapy is followed by surgical removal of the tumor and then further adjuvant chemotherapy. Physical therapy and prosthetics are of great importance in these patients because of the highly invasive nature of the treatment.
![]() The Musculoskeletal Tumor Society and the National Comprehensive Cancer Network (NCCN) recognize wide excision, either by amputation or by a limb-salvage procedure, as the recommended surgical approach for all high-grade bone sarcomas. This type of resection is predicated on complete tumor removal, effective skeletal reconstruction, and adequate soft tissue coverage.
The Musculoskeletal Tumor Society and the National Comprehensive Cancer Network (NCCN) recognize wide excision, either by amputation or by a limb-salvage procedure, as the recommended surgical approach for all high-grade bone sarcomas. This type of resection is predicated on complete tumor removal, effective skeletal reconstruction, and adequate soft tissue coverage.
![]() Osteosarcoma therapy. The 5-year survival for osteosarcoma with surgery alone is <20%. This occurs because microscopic metastatic dissemination is likely to be present in 80% of patients at the time of diagnosis. The addition of adjuvant chemotherapy has improved survival for high-grade osteosarcoma, permitting long-term survival as high as 80% is selected patients.
Osteosarcoma therapy. The 5-year survival for osteosarcoma with surgery alone is <20%. This occurs because microscopic metastatic dissemination is likely to be present in 80% of patients at the time of diagnosis. The addition of adjuvant chemotherapy has improved survival for high-grade osteosarcoma, permitting long-term survival as high as 80% is selected patients.
![]() Neoadjuvant and adjuvant chemotherapy. Neoadjuvant chemotherapy began as a strategy to permit limb-sparing surgery, allows time for creation of custom-made prosthetics. Since its acceptance, other advantages have been recognized with this approach. It permits earlier treatment of occult micrometastatic disease, preventing emergence of resistant clones and potentially allows for the debulking of the primary to improve chances for limb-sparing surgery.
Neoadjuvant and adjuvant chemotherapy. Neoadjuvant chemotherapy began as a strategy to permit limb-sparing surgery, allows time for creation of custom-made prosthetics. Since its acceptance, other advantages have been recognized with this approach. It permits earlier treatment of occult micrometastatic disease, preventing emergence of resistant clones and potentially allows for the debulking of the primary to improve chances for limb-sparing surgery.
![]() Chemotherapeutic agents active in osteosarcomas include doxorubicin, cisplatin, ifosfamide, and high-dose methotrexate with leucovorin rescue. These agents are typically used in combination to improve response, although the optimal combination and duration of therapy remain controversial.
Chemotherapeutic agents active in osteosarcomas include doxorubicin, cisplatin, ifosfamide, and high-dose methotrexate with leucovorin rescue. These agents are typically used in combination to improve response, although the optimal combination and duration of therapy remain controversial.
![]() Histologic response to preoperative therapy is recognized as a significant prognostic factor. Various systems have been developed for grading histologic response to chemotherapy, but >90% necrosis of tumor cells is associated with the best prognosis. If the tumor has been resected to negative margins and had a good histologic response to chemotherapy, the patient continues on chemotherapy for an additional 2 to 12 cycles. If the tumor was fully resected but has <90% necrosis, salvage chemotherapy with agents not used in induction is attempted, but the effect of this change in chemo-therapy on outcomes is unclear. If the tumor margins are positive, additional local surgery should be attempted.
Histologic response to preoperative therapy is recognized as a significant prognostic factor. Various systems have been developed for grading histologic response to chemotherapy, but >90% necrosis of tumor cells is associated with the best prognosis. If the tumor has been resected to negative margins and had a good histologic response to chemotherapy, the patient continues on chemotherapy for an additional 2 to 12 cycles. If the tumor was fully resected but has <90% necrosis, salvage chemotherapy with agents not used in induction is attempted, but the effect of this change in chemo-therapy on outcomes is unclear. If the tumor margins are positive, additional local surgery should be attempted.

![]() Radiation therapy. Radiation is not routinely used in the therapy of osteosarcoma, but it may prove helpful in patients who refuse definitive resection or in palliation of patients with metastatic disease.
Radiation therapy. Radiation is not routinely used in the therapy of osteosarcoma, but it may prove helpful in patients who refuse definitive resection or in palliation of patients with metastatic disease.
![]() Management of metastatic disease. Approximately 10% to 20% of patients with osteosarcoma have evidence of metastatic disease at presentation. Some of these patients may be candidates for the surgical resection of pulmonary metastases. For patients with more extensive metastatic disease, chemotherapy is used to provide control of disease and palliation of symptoms.
Management of metastatic disease. Approximately 10% to 20% of patients with osteosarcoma have evidence of metastatic disease at presentation. Some of these patients may be candidates for the surgical resection of pulmonary metastases. For patients with more extensive metastatic disease, chemotherapy is used to provide control of disease and palliation of symptoms.
![]() Ewing sarcoma
Ewing sarcoma
Therapy for Ewing sarcoma and the related primitive peripheral neuroectodermal tumors uses a combined-modality approach.26
![]() Treatment of the primary tumor. The optimal treatment for local tumor control is not well defined. Historically, radiation therapy has been the mainstay of local therapy, but there has been a recent trend toward surgery. No prospective randomized trials have been performed to compare the two modalities, but retrospective data suggest improvements in local control and survival when surgery is done with a complete resection of the tumor. Patients with unresectable disease or positive margins require radiation therapy to improve local control.
Treatment of the primary tumor. The optimal treatment for local tumor control is not well defined. Historically, radiation therapy has been the mainstay of local therapy, but there has been a recent trend toward surgery. No prospective randomized trials have been performed to compare the two modalities, but retrospective data suggest improvements in local control and survival when surgery is done with a complete resection of the tumor. Patients with unresectable disease or positive margins require radiation therapy to improve local control.
![]() Chemotherapy. Before the availability of effective chemotherapeutic agents, <10% of patients with Ewing sarcoma survived beyond 5 years, despite the fact that only 15% to 35% of patients with Ewing sarcoma/primitive peripheral neuroectodermal tumors had evidence of metastatic disease at presentation. This suggests that many patients with Ewing sarcoma have occult microscopic dissemination of the disease at the time of diagnosis. The current standard regimen is to use vincristine, actinomycin D, and cyclophosphamide (VAC) alternating with ifosfamide and etoposide (IE).
Chemotherapy. Before the availability of effective chemotherapeutic agents, <10% of patients with Ewing sarcoma survived beyond 5 years, despite the fact that only 15% to 35% of patients with Ewing sarcoma/primitive peripheral neuroectodermal tumors had evidence of metastatic disease at presentation. This suggests that many patients with Ewing sarcoma have occult microscopic dissemination of the disease at the time of diagnosis. The current standard regimen is to use vincristine, actinomycin D, and cyclophosphamide (VAC) alternating with ifosfamide and etoposide (IE).
![]() Recurrent metastatic Ewing sarcoma. In this setting, cure is not a realistic goal. Palliation and prolongation of survival are more realistic expectations. Fortunately, aggressive combination chemotherapy (VAC or IE) and radiation therapy can still lead to prolonged progression-free survival.
Recurrent metastatic Ewing sarcoma. In this setting, cure is not a realistic goal. Palliation and prolongation of survival are more realistic expectations. Fortunately, aggressive combination chemotherapy (VAC or IE) and radiation therapy can still lead to prolonged progression-free survival.
REFERENCES
1. Jemal A, Siegel R, Xu J, et al. Cancer Statistics, 2010. CA Cancer J Clin. 2010;60:277–300.
2. Brady MS, Gaynor JJ, Brennan MF. Radiation-associated sarcoma of bone and soft tissue. Arch Surg. 1992;127:1379–1385.
3. Robinson E, Neugut AI, Wylie P. Clinical aspects of postirradiation sarcomas. J Natl Cancer Inst. 1988;80:233–240.
4. Pitcher ME, Davidson TI, Fisher C, et al. Post irradiation sarcoma of soft tissue and bone. Eur J Surg Oncol. 1994;20:53–56.
5. Tucker MA, D’Angio GJ, Boice JD Jr, et al. Bone sarcomas linked to radiotherapy and chemotherapy in children. N Engl J Med. 1987;317:588–593.
6. Da Horta JS, Da Motta LC, Abbatt JD, et al. Malignancy and other late effects following administration of thorotrast. Lancet. 1965;1:201–205.
7. Creech JL Jr, Johnson MN. Angiosarcoma of liver in the manufacture of polyvinyl chloride. J Occup Med. 1974;16:150–151.
8. Falk H, Caldwell GG, Ishak KG, et al. Arsenic-related hepatic angiosarcoma. Am J Ind Med. 1981;2:43–50.
9. Steenland K, Bertazzi P, Baccarelli A, et al. Dioxin revisited: developments since the 1997 IARC classification of dioxin as a human carcinogen. Environ Health Perspect. 2004;112:1265–1268.
10. Sorensen SA, Mulvihill JJ, Nielsen A. Long-term follow-up of von Recklinghausen neurofibromatosis. Survival and malignant neoplasms. N Engl J Med. 1986;314:1010–1015.
11. Schneider K, Garber J. Li-Fraumeni syndrome. Gene Reviews Online Journal. 2010. Last accessed 3/27/2011 .
12. Yu CE, Oshima J, Fu YH, et al. Positional cloning of the Werner’s syndrome gene. Science. 1996;272:258–262.
13. Chung KC, Kim HJE, Jeffers LLC. Lymphangiosarcoma (Stewart-Treves syndrome) in postmastectomy patients. J Hand Surg Am. 2000;25:1163–1168.
14. Mesri EA, Cesarman E, Boshoff C. Kaposi’s sarcoma and its associated herpesvirus. Nat Rev Cancer. 2010;10:707–719.
15. Mankin HJ, Hornicek FJ. Paget’s sarcoma: a historical and outcome review. Clin Orthop Relat Res. 2005;438:97–102.
16. Osuna D, de Alava E. Molecular pathology of sarcomas. Rev Recent Clin Trials. 2009;4:12–26.
17. Jain S, Xu R, Prieto VG, et al. Molecular classification of soft tissue sarcomas and its clinical applications. Int J Clin Exp Pathol. 2010;3:416–428.
18. Ordonez JL, Osuna D, Garcia-Dominguez DJ, et al. The clinical relevance of molecular genetics in soft tissue sarcomas. Adv Anat Pathol. 2010;17:162–181.
19. Luis AM, Aguilar DP, Martin JA. Multidisciplinary management of soft tissue sarcomas. Clin Transl Oncol. 2010;12:543–553.
20. Jaques DP, Coit DG, Hajdu SI, et al. Management of primary and recurrent soft-tissue sarcoma of the retroperitoneum. Ann Surg. 1990;212:51–59.
21. Alvarenga JC, Ball AB, Fisher C, et al. Limitations of surgery in the treatment of retroperitoneal sarcoma. Br J Surg. 1991;78:912–916.
22. O’Sullivan B, Davis AM, Turcotte R, et al. Preoperative versus postoperative radiotherapy in soft-tissue sarcoma of the limbs: a randomised trial. Lancet. 2002;359:2235–2241.
23. Sarcoma Meta-analysis Collaboration. Adjuvant chemotherapy for localised resectable soft-tissue sarcoma of adults: meta-analysis of individual data. Sarcoma meta-analysis collaboration. Lancet. 1997;350:1647–1654.
24. Edge S, Byrd D, Compton C, et al. AJCC (American Joint Committee on Cancer) Cancer Staging Manual. New York:Springer;2010:291.
25. Maki RG. Pediatric sarcomas occurring in adults. J Surg Oncol. 2008;97:360–368.
26. Schiffman JD, Wright J. Ewing’s sarcoma and second malignancies. Sarcoma. 2011:736841. Epub 2010 Oct 13.