GENERAL PRINCIPLES
Definition
![]() Cancer of unknown primary (CUP) is defined as biopsy-proven metastatic cancer where the site of origin of the primary tumor is not identified after standard evaluation, including a thorough history and physical examination, imaging studies, laboratory data and detailed pathologic evaluation.
Cancer of unknown primary (CUP) is defined as biopsy-proven metastatic cancer where the site of origin of the primary tumor is not identified after standard evaluation, including a thorough history and physical examination, imaging studies, laboratory data and detailed pathologic evaluation.
![]() Cancer of unknown primary includes a heterogeneous group of patients characterized by an aggressive clinical course and that is less responsive to chemotherapy. The search for the primary site of cancer has been increasingly facilitated by the advancement in diagnostic modalities. Historically, the median survival for this group of patients ranged from 6 to 10 months in clinical trials, however life expectancy has been noted to be as low as 2 to 3 months in unselected patient populations.1,2 There are, however specific subgroups of patients with CUP who have treatment-responsive disease and may be able to achieve long-term disease-free survival with appropriate management. The workup of a patient with an unknown primary tumor should focus on identifying the patients with these treatable conditions. An exhaustive search for the primary tumor after adds little to the overall management of the patient, as the primary tumor site is located in <20% of patients before death and up to 70% of cases remain undiagnosed even after autopsy. 3
Cancer of unknown primary includes a heterogeneous group of patients characterized by an aggressive clinical course and that is less responsive to chemotherapy. The search for the primary site of cancer has been increasingly facilitated by the advancement in diagnostic modalities. Historically, the median survival for this group of patients ranged from 6 to 10 months in clinical trials, however life expectancy has been noted to be as low as 2 to 3 months in unselected patient populations.1,2 There are, however specific subgroups of patients with CUP who have treatment-responsive disease and may be able to achieve long-term disease-free survival with appropriate management. The workup of a patient with an unknown primary tumor should focus on identifying the patients with these treatable conditions. An exhaustive search for the primary tumor after adds little to the overall management of the patient, as the primary tumor site is located in <20% of patients before death and up to 70% of cases remain undiagnosed even after autopsy. 3
Classification
Based on the light microscopy findings, they are classified into the below five major subtypes: moderate to well-differentiated adenocarcinoma (~60% of cases), poorly differentiated carcinoma with or without features of adenocarcinoma (~30%), neuroendocrine carcinoma (~1%), poorly differentiated or undifferentiated malignant neoplasm (~5%), and squamous cell carcinoma (~5%) as outlined in Table 33-1. The poorly differentiated tumors can include neuroendocrine tumors, lymphomas, germ cell tumors, melanomas, sarcomas, embryonal malignancies or may remain unspecified even after complete pathologic evaluation.4,5
Epidemiology
The exact incidence of CUP tumors is unknown, as they are often not reported accurately in tumor registries. The SEER database and international registries demonstrates that the estimated incidence from of CUP accounts for ~5% of all initial cancer diagnoses.4 It is generally a disease of the middle-aged, with the median age at diagnosis being 60 years and is slightly more frequent in males.1

Etiology
The extreme heterogeneity within this group of patients precludes any specific identifiable etiologic or associated risk factors that may contribute to its pathogenesis.
Pathophysiology
CUP is a heterogeneous group of tumors. The molecular basis of this entity has not been elucidated. They are known to possess a unique set of clinical characteristics apart from the obvious absence of primary tumor such as: early dissemination, unpredictable metastatic pattern, aggressive disease and overall poor prognosis. The absence of the primary site of tumor is likely attributed to the slow growth pattern of the primary tumor or involution of the tumor at its primary site.
DIAGNOSIS
Extensive workup in the evaluation of patient with CUP identifies the primary tumor ~20% to 30% of patients ante mortem and autopsy studies remains inconclusive in majority of patients.
Clinical Presentation
A thorough history and physical examination is warranted in every patient with newly diagnosed cancer of unknown primary. Patients typically present with symptoms of widely metastatic disease and often have multiple symptoms at presentation. While pain is the most common presenting symptom, other common symptoms include weight loss, anorexia, fatigue, new mass, lymphadenopathy, central nervous system abnormalities, and bone pain or fracture. A careful physical examination may point towards additional sites of metastatic disease, but these are often not helpful to identify the site of primary involvement. In a series of 657 patients studied at M.D. Anderson Cancer Center, lymph nodes were the most frequently involved site of metastasis, while other major sites of involvement included liver, bone, lung, pleura, and brain.6 Cervical adenopathy can be a manifestation of primary lung, breast, or head and neck cancer, as well as lymphoma. Lung and pancreatic cancers were most frequently identified in an autopsy series as the primary tumor site in patients with CUP, followed by other gastrointestinal and gynecological malignancies.3It is important to keep in mind that CUP tumors can metastasize to any site and the pattern of metastasis, while sometimes suggestive of an underlying primary tumor, does not confirm the diagnosis.
Diagnostic Testing
Standard diagnostic testing includes chest x-ray, blood chemistries and blood counts, standard imaging with CT scan and pathologic evaluation of the tumor. Tumor markers, mammogram, additional imaging studies including PET scan, testicular ultrasound or breast MRI and endoscopic evaluation depend on the site of the metastasis and features noted on pathology that are discussed below. The appropriate workup of an occult primary tumor after baseline evaluation with standard diagnostic tools includes identification of specific clinicopathologic subsets with favorable prognosis.
![]() Diagnostic pathology. An accurate pathologic evaluation of tumor specimen is paramount to the diagnostic evaluation of patents with CUP. An adequate tumor sample is cornerstone to obtaining valuable information from light microscopy, immunohistochemical staining and other sophisticated testing including genetic/molecular studies and electron microscopic evaluation in some cases.
Diagnostic pathology. An accurate pathologic evaluation of tumor specimen is paramount to the diagnostic evaluation of patents with CUP. An adequate tumor sample is cornerstone to obtaining valuable information from light microscopy, immunohistochemical staining and other sophisticated testing including genetic/molecular studies and electron microscopic evaluation in some cases.
![]() Light microscopy. This technique provides basic information with regards to the morphology and level of differentiation of the tumor. It rarely provides information necessary to identify the origin of the metastasis. Some special staining techniques may help to rule out sarcomas and lymphomas, however these histochemical techniques have limited utility and are less sensitive and specific than their immunohistochemistry counterparts.
Light microscopy. This technique provides basic information with regards to the morphology and level of differentiation of the tumor. It rarely provides information necessary to identify the origin of the metastasis. Some special staining techniques may help to rule out sarcomas and lymphomas, however these histochemical techniques have limited utility and are less sensitive and specific than their immunohistochemistry counterparts.
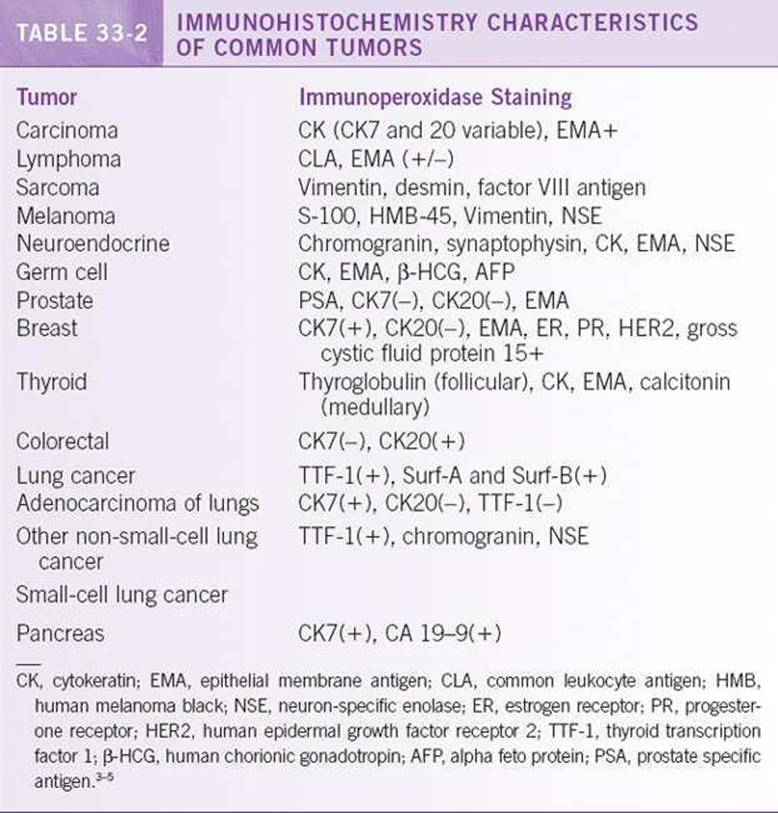
![]() Immunohistochemistry (IHC). This technique is widely available and is often useful in identification of the primary origin of malignancy. Immunohistochemistry uses a panel of monoclonal and polyclonal antibodies to various cell components including enzymes, structural components of cells, hormone receptors, oncofetal antigens and other substances identified by the immunoperoxidase technique. Important staining characteristics of some of the common malignancies are shown in Table 33-2. Among the tumors identified as adenocarcinomas, staining for the cytokeratin CK7 and CK20 is the most common first step. CK7+/CK20 – tumors include lung (adenocarcinoma), biliary tract and pancreas, ovary (nonmucinous), endometrium, thyroid, cervical and breast cancer, while CK7–/CK20+ tumors include gastrointestinal, ovary (mucinous) and Merkel cell carcinoma. CK7+/CK20+ tumors include urothelial, biliary tract and pancreas and ovary (mucinous). CK7–/CK20– tumors are head and neck, liver, lung (squamous and small cell) prostate and kidney.
Immunohistochemistry (IHC). This technique is widely available and is often useful in identification of the primary origin of malignancy. Immunohistochemistry uses a panel of monoclonal and polyclonal antibodies to various cell components including enzymes, structural components of cells, hormone receptors, oncofetal antigens and other substances identified by the immunoperoxidase technique. Important staining characteristics of some of the common malignancies are shown in Table 33-2. Among the tumors identified as adenocarcinomas, staining for the cytokeratin CK7 and CK20 is the most common first step. CK7+/CK20 – tumors include lung (adenocarcinoma), biliary tract and pancreas, ovary (nonmucinous), endometrium, thyroid, cervical and breast cancer, while CK7–/CK20+ tumors include gastrointestinal, ovary (mucinous) and Merkel cell carcinoma. CK7+/CK20+ tumors include urothelial, biliary tract and pancreas and ovary (mucinous). CK7–/CK20– tumors are head and neck, liver, lung (squamous and small cell) prostate and kidney.
![]() Electron microscopy (EM). EM is not widely available and is expensive, but it may contribute to the diagnosis in rare cases, especially in the evaluation of poorly differentiated tumors. For example, secretory granules can be seen in neuroendocrine tumors, Weibel–Palade bodies in angiosarcomas, premelanosomes in melanomas and prekeratin filaments and desmosomes in squamous cell carcinoma. Electron microscopy is recommended in the evaluation of poorly differentiated neoplasm in young adults when the IHC is inconclusive.
Electron microscopy (EM). EM is not widely available and is expensive, but it may contribute to the diagnosis in rare cases, especially in the evaluation of poorly differentiated tumors. For example, secretory granules can be seen in neuroendocrine tumors, Weibel–Palade bodies in angiosarcomas, premelanosomes in melanomas and prekeratin filaments and desmosomes in squamous cell carcinoma. Electron microscopy is recommended in the evaluation of poorly differentiated neoplasm in young adults when the IHC is inconclusive.
![]() Cytogenetics and molecular diagnostics. Cytogenetic analysis is an evolving field and may also be useful in certain situations. Isochromosome 12p and 12q are seen in germ cell tumors, translocation t(11;22) is seen in Ewing sarcoma and primitive neuroectodermal tumors, while t(8;14) translocation can be seen in some lymphoid malignancies, especially Burkitt’s lymphoma. Overexpression of c-myc, ras, c-erbB2, EGFR and VEFG among others are demonstrated by IHC in various frequencies in different studies, although the exact role of this diagnostic evaluation is not completely clear at this time.
Cytogenetics and molecular diagnostics. Cytogenetic analysis is an evolving field and may also be useful in certain situations. Isochromosome 12p and 12q are seen in germ cell tumors, translocation t(11;22) is seen in Ewing sarcoma and primitive neuroectodermal tumors, while t(8;14) translocation can be seen in some lymphoid malignancies, especially Burkitt’s lymphoma. Overexpression of c-myc, ras, c-erbB2, EGFR and VEFG among others are demonstrated by IHC in various frequencies in different studies, although the exact role of this diagnostic evaluation is not completely clear at this time.
![]() Gene expression profiling. High throughput molecular profiling technologies are rapidly accumulating data on expression of multiple genes in several human tumors. By identifying the pattern of “typical gene expression profile” for each tumor with the help of these advanced techniques, it is becoming increasingly possible to molecularly assign a primary tumor of origin in patients with CUP. The overall accuracy from 12 studies using several tumor samples is in the range of 75% to 85%.7,8 It has to emphasize that while a primary site of the metastatic tumor can be molecularly assigned, it is not yet clear if these tumors will have the same biology and response to therapy as their metastatic counterpart with known primary. The prognostic and predictive value of this diagnostic tool is presently unclear and needs to be validated in prospective trials. It is not considered a part of standard workup for CUP at this time.
Gene expression profiling. High throughput molecular profiling technologies are rapidly accumulating data on expression of multiple genes in several human tumors. By identifying the pattern of “typical gene expression profile” for each tumor with the help of these advanced techniques, it is becoming increasingly possible to molecularly assign a primary tumor of origin in patients with CUP. The overall accuracy from 12 studies using several tumor samples is in the range of 75% to 85%.7,8 It has to emphasize that while a primary site of the metastatic tumor can be molecularly assigned, it is not yet clear if these tumors will have the same biology and response to therapy as their metastatic counterpart with known primary. The prognostic and predictive value of this diagnostic tool is presently unclear and needs to be validated in prospective trials. It is not considered a part of standard workup for CUP at this time.
Laboratories
In addition to routine evaluation with standard chemistry and blood counts, tumor markers are additional laboratory testing that may be warranted in certain clinical situations to identify specific treatable CUPs.
![]() Tumor markers. Some of these clinical situations include β-HCG and AFP in young men with CUP to identify extra-gonadal germ cell tumors, PSA in men to identify metastatic prostate cancer, serum thyroglobulin in rare patients with bone metastasis to identify occult thyroid cancer and serum CA 15–3 and CA125 can be helpful in women with isolated axillary lymph node enlargement or peritoneal papillary adenocarcinomatosis. Routine evaluation of commonly used epithelial tumor markers, such as CEA, CA19–9, and CA125 are nonspecific and do not provide any additional diagnostic value in identifying the primary tumor and most often nonspecific elevation in multiple tumor markers may be noted in patients with CUP.
Tumor markers. Some of these clinical situations include β-HCG and AFP in young men with CUP to identify extra-gonadal germ cell tumors, PSA in men to identify metastatic prostate cancer, serum thyroglobulin in rare patients with bone metastasis to identify occult thyroid cancer and serum CA 15–3 and CA125 can be helpful in women with isolated axillary lymph node enlargement or peritoneal papillary adenocarcinomatosis. Routine evaluation of commonly used epithelial tumor markers, such as CEA, CA19–9, and CA125 are nonspecific and do not provide any additional diagnostic value in identifying the primary tumor and most often nonspecific elevation in multiple tumor markers may be noted in patients with CUP.
Imaging
The importance of CT scan is well established in the workup and staging of patients with newly diagnosed malignancy. Mammography and/or ultrasound of the breast are recommended in clinically suspicious cases of breast cancer. MRI of the breast is a very sensitive test to evaluate clinically occult breast cancers and can be requested in suspected cases when mammography and ultrasound are not diagnostic. The use of fluorodeoxyglucose (FDG)-PET scans done in conjunction with a noncontrast CT study is used sometimes to provide better anatomic localization. Small studies suggest that PET/CT may be more sensitive than traditional imaging studies in locating a primary tumor, but larger follow-up studies have yet to be reported. For now, clinical judgment governs the use of PET/CT in the workup of CUP, and clinicians should consider this imaging test if the results would significantly change further management.
Diagnostic Procedures
![]() Endoscopy. The decision regarding the need for endoscopy is based on the clinical presentation of the patient with CUP. Upper airway evaluation by ENT with an endoscope is recommended for patients with isolated cervical lymph node involvement. Bronchoscopy and gastrointestinal endoscopies are indicated in patients with pulmonary or abdominal signs and symptoms respectively. Proctoscopy and/or colposcopy are recommended for patients presenting with inguinal lymph node involvement.
Endoscopy. The decision regarding the need for endoscopy is based on the clinical presentation of the patient with CUP. Upper airway evaluation by ENT with an endoscope is recommended for patients with isolated cervical lymph node involvement. Bronchoscopy and gastrointestinal endoscopies are indicated in patients with pulmonary or abdominal signs and symptoms respectively. Proctoscopy and/or colposcopy are recommended for patients presenting with inguinal lymph node involvement.
TREATMENT
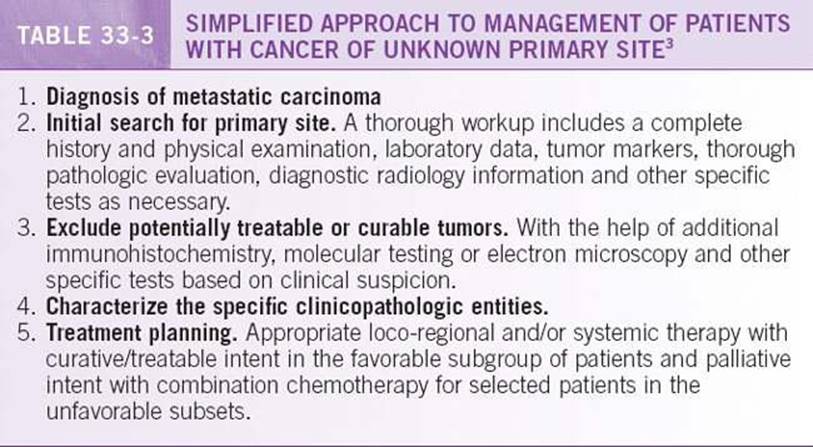
Historically patients with CUP are known to have a poor outcome. The identification of subset of patients with favorable features who enjoy a longer disease-free survival is an important step in the management of patients with CUP. These patients with favorable features have a distinct clinicopathologic characteristics and their management is outlined separately. For patients with lack of favorable characteristics, palliative approach with combination chemotherapy is the cornerstone of management. It is important to establish the goals of care and assess their candidacy for chemotherapy in patients with unfavorable features. The general principles of management are shown in Table 33-3 and the paragraphs below summarize the management based on histology.
![]() Well-differentiated or moderately differentiated adenocarcinoma. Well-differentiated or moderately differentiated adenocarcinoma is the most frequent type of CUP, accounting for 60% of cases. These patients are typically elderly, with multiple sites of metastasis and their presentation depends on the sites of involvement. Immunohistochemistry is of limited value in this group of patients, although identification of ER/PR status or PSA is valuable for treatment and prognosis. Few patients in this group fit into a favorable treatment subset. Most patients have a poor prognosis and are mainly treated with palliative intent. Patients with a good performance status should be considered candidates for systemic therapy and/or clinical trials. Multiple chemotherapy regimens have been evaluated in these patients with the aim of stabilizing their disease. The combination chemotherapy regimens listed under NCCN guidelines based on available data from clinical trials as is shown in Table 33-4.
Well-differentiated or moderately differentiated adenocarcinoma. Well-differentiated or moderately differentiated adenocarcinoma is the most frequent type of CUP, accounting for 60% of cases. These patients are typically elderly, with multiple sites of metastasis and their presentation depends on the sites of involvement. Immunohistochemistry is of limited value in this group of patients, although identification of ER/PR status or PSA is valuable for treatment and prognosis. Few patients in this group fit into a favorable treatment subset. Most patients have a poor prognosis and are mainly treated with palliative intent. Patients with a good performance status should be considered candidates for systemic therapy and/or clinical trials. Multiple chemotherapy regimens have been evaluated in these patients with the aim of stabilizing their disease. The combination chemotherapy regimens listed under NCCN guidelines based on available data from clinical trials as is shown in Table 33-4.

![]() Poorly differentiated carcinoma with or without features of adenocarcinoma. This group accounts for about ~30% of CUP cases. The majority of the patients have a poorly differentiated carcinoma histology, while a third have some features of adenocarcinoma differentiation. In comparison to patients with moderately or well-differentiated adenocarcinoma, these patients tend to be younger, have more rapidly progressive symptoms, and have peripheral lymph nodes, and mediastinal or retroperitoneal involvement. Favorable subsets with specific therapeutic implications have to be excluded from this group of patients. The prognosis and treatment for the remaining patients with unfavorable features are similar to the ones with well-differentiated adenocarcinoma group. Recent clinical trials by investigators at the Minnie Pearl Cancer Research Network incorporating several newer agents including targeted therapy have noted further improvement in outcome.4
Poorly differentiated carcinoma with or without features of adenocarcinoma. This group accounts for about ~30% of CUP cases. The majority of the patients have a poorly differentiated carcinoma histology, while a third have some features of adenocarcinoma differentiation. In comparison to patients with moderately or well-differentiated adenocarcinoma, these patients tend to be younger, have more rapidly progressive symptoms, and have peripheral lymph nodes, and mediastinal or retroperitoneal involvement. Favorable subsets with specific therapeutic implications have to be excluded from this group of patients. The prognosis and treatment for the remaining patients with unfavorable features are similar to the ones with well-differentiated adenocarcinoma group. Recent clinical trials by investigators at the Minnie Pearl Cancer Research Network incorporating several newer agents including targeted therapy have noted further improvement in outcome.4
![]() Squamous cell carcinoma. Squamous cell carcinoma accounts for 5% of all cases of CUP. Majority of patients in this subgroup fall into specific clinical syndromes and are largely treatable, hence appropriate diagnostic workup should be undertaken. Management of patients with squamous cell carcinoma involving the cervical, supraclavicular and inguinal lymph nodes are outlined below. Patients with squamous cell carcinoma involving other areas should be evaluated for occult lung primary with CT scan and bronchoscopy. Other sites of origin of tumor include head and neck, esophagus, cervix, anus, rectum, and bladder. Patients should be evaluated for additional sites when indicated, as some adenocarcinoma can undergo squamous differentiation and immunohistochemistry may be helpful in these situations. Table 33-4 outlines the chemotherapy regimens listed under the NCCN guidelines for squamous cell carcinoma of unknown primary.
Squamous cell carcinoma. Squamous cell carcinoma accounts for 5% of all cases of CUP. Majority of patients in this subgroup fall into specific clinical syndromes and are largely treatable, hence appropriate diagnostic workup should be undertaken. Management of patients with squamous cell carcinoma involving the cervical, supraclavicular and inguinal lymph nodes are outlined below. Patients with squamous cell carcinoma involving other areas should be evaluated for occult lung primary with CT scan and bronchoscopy. Other sites of origin of tumor include head and neck, esophagus, cervix, anus, rectum, and bladder. Patients should be evaluated for additional sites when indicated, as some adenocarcinoma can undergo squamous differentiation and immunohistochemistry may be helpful in these situations. Table 33-4 outlines the chemotherapy regimens listed under the NCCN guidelines for squamous cell carcinoma of unknown primary.
![]() Poorly differentiated neoplasm. Poorly differentiated neoplasm account for ~5% of CUP. Detailed pathologic evaluation is very important in this subgroup, as treatment may differ radically based on the results. Many of these tumors can be characterized as atypical lymphomas, neuroendocrine tumors, or germ cell tumors by careful pathologic testing. If a specific diagnosis cannot be made, then poorly differentiated neoplasms are treated the same as poorly differentiated adenocarcinoma. It is again important to exclude important treatable clinical scenarios, for example if a male patient aged <50 years old presents with a poorly differentiated neoplasm (especially with mediastinal or retroperitoneal mass), particular attention should be paid to exclude the diagnosis of an atypical germ cell tumor.
Poorly differentiated neoplasm. Poorly differentiated neoplasm account for ~5% of CUP. Detailed pathologic evaluation is very important in this subgroup, as treatment may differ radically based on the results. Many of these tumors can be characterized as atypical lymphomas, neuroendocrine tumors, or germ cell tumors by careful pathologic testing. If a specific diagnosis cannot be made, then poorly differentiated neoplasms are treated the same as poorly differentiated adenocarcinoma. It is again important to exclude important treatable clinical scenarios, for example if a male patient aged <50 years old presents with a poorly differentiated neoplasm (especially with mediastinal or retroperitoneal mass), particular attention should be paid to exclude the diagnosis of an atypical germ cell tumor.
![]() Neuroendocrine carcinoma. Neuroendocrine carcinoma of unknown primary site accounts for a minority of the CUP patients. Some are well differentiated or low grade with features typical of carcinoid, or islet cell tumors and have metastatic involvement of the liver or bone. They can be associated with syndromes such as Zollinger-Ellison and carcinoid from secretion of bioactive amines. In some of these patients, a primary site can be found in the small intestine, rectum, pancreas, or bronchus on further evaluation. These tumors are generally indolent and their treatment recommendation is per the standard guidelines for metastatic carcinoid or islet cell malignancies with known primary site. The other types of neuroendocrine tumors include those with aggressive behavior either with neuroendocrine histology or lack of distinctive neuroendocrine features on light microscopy. The neuroendocrine features in this later group are only recognized on detailed pathologic evaluation. treatment recommendation for small-cell carcinoma of unknown primary is combination chemotherapy as recommended for small-cell lung cancer. Patients with poorly differentiated neuroendocrine carcinoma of unknown primary site are still a highly treatable subgroup and a trial of combination chemotherapy with platinum-based regimen is recommended.
Neuroendocrine carcinoma. Neuroendocrine carcinoma of unknown primary site accounts for a minority of the CUP patients. Some are well differentiated or low grade with features typical of carcinoid, or islet cell tumors and have metastatic involvement of the liver or bone. They can be associated with syndromes such as Zollinger-Ellison and carcinoid from secretion of bioactive amines. In some of these patients, a primary site can be found in the small intestine, rectum, pancreas, or bronchus on further evaluation. These tumors are generally indolent and their treatment recommendation is per the standard guidelines for metastatic carcinoid or islet cell malignancies with known primary site. The other types of neuroendocrine tumors include those with aggressive behavior either with neuroendocrine histology or lack of distinctive neuroendocrine features on light microscopy. The neuroendocrine features in this later group are only recognized on detailed pathologic evaluation. treatment recommendation for small-cell carcinoma of unknown primary is combination chemotherapy as recommended for small-cell lung cancer. Patients with poorly differentiated neuroendocrine carcinoma of unknown primary site are still a highly treatable subgroup and a trial of combination chemotherapy with platinum-based regimen is recommended.
SPECIAL CONSIDERATIONS
Below are the distinct clinicopathologic entities that require special attention, as these represent subgroup of patients with specific therapy recommendation and relatively better outcomes given their treatable and/or curable situations.
![]() Extragonadal germ cell tumor presenting as poorly differentiated carcinoma/malignancy with midline distribution. Extragonadal germ cell tumors should be suspected in men aged <50 years old with midline tumors, either mediastinal or retroperitoneal tumors, and a relatively short duration of symptoms. Tumor markers (AFP and β-hCG) should be checked and treatment should be formulated. For example, poor prognosis germ cell tumors are treated with platinum-based regimens. High overall response rates of more than 50% with 15% to 25% complete responses and 10% to 15% long-term disease-free survival rates have been noted in this subgroup.3
Extragonadal germ cell tumor presenting as poorly differentiated carcinoma/malignancy with midline distribution. Extragonadal germ cell tumors should be suspected in men aged <50 years old with midline tumors, either mediastinal or retroperitoneal tumors, and a relatively short duration of symptoms. Tumor markers (AFP and β-hCG) should be checked and treatment should be formulated. For example, poor prognosis germ cell tumors are treated with platinum-based regimens. High overall response rates of more than 50% with 15% to 25% complete responses and 10% to 15% long-term disease-free survival rates have been noted in this subgroup.3
![]() Women with peritoneal carcinomatosis. Women may present with peritoneal carcinomatosis with histologic features suggestive of ovarian adenocarcinoma, such as psammoma bodies and papillary structure, in the absence of primary tumor even after abdominal exploration. Patients often have elevated CA-125 levels and they rarely metastasize outside of the peritoneal cavity. These women should be treated as stage III ovarian cancer with surgical cytoreduction followed by adjuvant chemotherapy with a platinum based regimen. Approximately 11% to 25% of patients are noted to have long-term survival with this management.3
Women with peritoneal carcinomatosis. Women may present with peritoneal carcinomatosis with histologic features suggestive of ovarian adenocarcinoma, such as psammoma bodies and papillary structure, in the absence of primary tumor even after abdominal exploration. Patients often have elevated CA-125 levels and they rarely metastasize outside of the peritoneal cavity. These women should be treated as stage III ovarian cancer with surgical cytoreduction followed by adjuvant chemotherapy with a platinum based regimen. Approximately 11% to 25% of patients are noted to have long-term survival with this management.3
![]() Women with adenocarcinoma involving axillary lymph nodes. Breast cancer should be suspected in this group of patients. Breast exam and mammography should be performed, as well as staining for estrogen and progesterone receptors and HER2 status. Breast MRI can also be used if initial studies are unrevealing. In this group of patients with negative exam and imaging, occult breast primary, usually measuring less than 2 cm in diameter has been found in 44% to 80% of mastectomy specimens.4 Patients should be evaluated for other meta-static involvement, and if evaluation is negative, they should be treated for stage II or III breast cancer. The treatment should include lymph node clearance with primary breast surgery and/or breast irradiation. Patients should receive adjuvant systemic treatment based on their age, lymph node status, ER/PR status, and HER2 status. If patients are found to have additional metastatic disease, they may have metastatic breast cancer and may benefit from therapy for metastatic breast cancer.
Women with adenocarcinoma involving axillary lymph nodes. Breast cancer should be suspected in this group of patients. Breast exam and mammography should be performed, as well as staining for estrogen and progesterone receptors and HER2 status. Breast MRI can also be used if initial studies are unrevealing. In this group of patients with negative exam and imaging, occult breast primary, usually measuring less than 2 cm in diameter has been found in 44% to 80% of mastectomy specimens.4 Patients should be evaluated for other meta-static involvement, and if evaluation is negative, they should be treated for stage II or III breast cancer. The treatment should include lymph node clearance with primary breast surgery and/or breast irradiation. Patients should receive adjuvant systemic treatment based on their age, lymph node status, ER/PR status, and HER2 status. If patients are found to have additional metastatic disease, they may have metastatic breast cancer and may benefit from therapy for metastatic breast cancer.
![]() Men with suspected prostate cancer. All men with metastatic adenocarcinoma with unknown primary should have their PSA levels checked. Their tumors can also be stained for PSA. Patients with elevated PSA should undergo hormonal treatment for prostate cancer even if the clinical features are atypical, as many will have significant palliation of their symptoms along with prolonged disease control.
Men with suspected prostate cancer. All men with metastatic adenocarcinoma with unknown primary should have their PSA levels checked. Their tumors can also be stained for PSA. Patients with elevated PSA should undergo hormonal treatment for prostate cancer even if the clinical features are atypical, as many will have significant palliation of their symptoms along with prolonged disease control.
![]() Patients with a single metastatic lesion. On occasion, only one site of metastatic disease is found even after complete evaluation and they represent a favorable prognostic group. Treatment should include aggressive local therapy of the metastatic lesion with surgical resection or radiation or a combination of both modalities. The role of systemic treatment is not yet defined in these patients, but can be considered for patients with good performance status and poor differentiation, especially in the context of clinical trials.
Patients with a single metastatic lesion. On occasion, only one site of metastatic disease is found even after complete evaluation and they represent a favorable prognostic group. Treatment should include aggressive local therapy of the metastatic lesion with surgical resection or radiation or a combination of both modalities. The role of systemic treatment is not yet defined in these patients, but can be considered for patients with good performance status and poor differentiation, especially in the context of clinical trials.
![]() Squamous cell carcinoma involving cervical and supraclavicular lymph nodes. Primary head and neck cancer should be suspected in patients with squamous cell carcinoma involving upper and middle cervical lymph nodes. These patients are usually elderly with history of tobacco and alcohol abuse. CT scan to evaluate the head and neck region is important to define the extent of the disease and identify the primary site. Careful direct and endoscopic evaluation of these areas is also indicated to complete the workup. The treatment recommendation is similar to the loco-regional management for locally advanced head and neck cancer with radical neck dissection, local radiation or a combined modality approach. About 30% to 40% of these patients achieve long-term disease free survival with this local therapy.4 Systemic chemotherapy administered concurrently with radiation or in the adjuvant setting can also be considered in patients with unknown primary in a similar fashion as indicated for head and neck cancers with known primary. In patients with lower cervical and supraclavicular lymph node involvement, a search for a primary lung tumor has to be undertaken. Local treatment to the neck is recommended when the primary site remains unidentified.
Squamous cell carcinoma involving cervical and supraclavicular lymph nodes. Primary head and neck cancer should be suspected in patients with squamous cell carcinoma involving upper and middle cervical lymph nodes. These patients are usually elderly with history of tobacco and alcohol abuse. CT scan to evaluate the head and neck region is important to define the extent of the disease and identify the primary site. Careful direct and endoscopic evaluation of these areas is also indicated to complete the workup. The treatment recommendation is similar to the loco-regional management for locally advanced head and neck cancer with radical neck dissection, local radiation or a combined modality approach. About 30% to 40% of these patients achieve long-term disease free survival with this local therapy.4 Systemic chemotherapy administered concurrently with radiation or in the adjuvant setting can also be considered in patients with unknown primary in a similar fashion as indicated for head and neck cancers with known primary. In patients with lower cervical and supraclavicular lymph node involvement, a search for a primary lung tumor has to be undertaken. Local treatment to the neck is recommended when the primary site remains unidentified.
![]() Squamous cell carcinoma involving inguinal lymph nodes. In patients with inguinal lymph node involvement, careful physical examination of the perineum and anorectal region should be undertaken to reveal a primary site. Anoscopy in all and pelvic examination in females should be part of the evaluation. If no primary site is identified, patients should undergo inguinal lymph node dissection with or without radiation therapy, especially if extensive disease is identified. Systemic chemotherapy can be considered in the adjuvant or neoadjuvant setting.
Squamous cell carcinoma involving inguinal lymph nodes. In patients with inguinal lymph node involvement, careful physical examination of the perineum and anorectal region should be undertaken to reveal a primary site. Anoscopy in all and pelvic examination in females should be part of the evaluation. If no primary site is identified, patients should undergo inguinal lymph node dissection with or without radiation therapy, especially if extensive disease is identified. Systemic chemotherapy can be considered in the adjuvant or neoadjuvant setting.
![]() Gestational choriocarcinoma. Metastatic gestational choriocarcinoma should be suspected in young women with poorly differentiated carcinoma and pulmonary nodules. A recent history of pregnancy, spontaneous abortion, or missed menses may be elicited. Imaging of the abdomen may show enlarged uterus and an elevated β-hCG is often helpful in making the diagnosis. These patients carry a high cure rate with single agent methotrexate.
Gestational choriocarcinoma. Metastatic gestational choriocarcinoma should be suspected in young women with poorly differentiated carcinoma and pulmonary nodules. A recent history of pregnancy, spontaneous abortion, or missed menses may be elicited. Imaging of the abdomen may show enlarged uterus and an elevated β-hCG is often helpful in making the diagnosis. These patients carry a high cure rate with single agent methotrexate.
MONITORING/FOLLOW-UP
There are no definite guidelines for monitoring and follow-up given the overall poor outcomes and short life expectancy in this patient population. Patients who fall into specific subgroup as mentioned earlier should follow the guidelines similar to the primary malignancy. While patients receiving palliative chemotherapy should follow the treatment schedule, the symptomatic patients should receive supportive management as often as needed.
OUTCOME/PROGNOSIS
This is a heterogeneous group with median survival of 6 to 10 months.1 Features such as lymph node involvement, pathologic diagnosis of carcinoma, squamous carcinoma, and neuroendocrine carcinoma confer a survival advantage, while male sex, pathologic diagnosis of adenocarcinoma, increasing number of involved organ sites and visceral involvement including liver, lung, bone, pleura, or brain are associated with poor survival. 6 Although the outcome overall is poor, it is worth mentioning again the importance identifying the patients that belong to the favorable subgroups who can be cured or treated with very encouraging long-term outcomes. The decision to treat the rest of patients in the unfavorable subgroup must be individualized and based on performance status and the patient’s desire to proceed.
REFERENCES
1. Pavlidis N, Fizazi K. Carcinoma of unknown primary (CUP). Crit Rev Oncol Hematol. 2009;69:271–278.
2. van de Wouw AJ, Janssen-Heijnen ML, Coebergh JW, et al. Epidemiology of unknown primary tumours; incidence and population-based survival of 1285 patients in Southeast Netherlands, 1984–1992. Eur J Cancer.2002;38:409–413.
3. Pavlidis N, Briasoulis E, Hainsworth J, et al. Diagnostic and therapeutic management of cancer of an unknown primary. Eur J Cancer. 2003;39:1990–2005.
4. Greco FA, Hainsworth JD. Cancer of unknown primary site. In: DeVita VT Jr., Hellman S, and Rosenberg SA, eds. Cancer: Principles and Practice of Oncology. 8th ed. Philadelphia: Lippincott Williams & Wilkins; 2008:2363–2387.
5. Hainsworth JD, Greco FA. Treatment of patients with cancer of an unknown primary site. N Engl J Med. 1993;329:257–263.
6. Abbruzzese JL, Abbruzzese MC, Hess KR, et al. Unknown primary carcinoma: natural history and prognostic factors in 657 consecutive patients. J Clin Oncol. 1994;12:1272–1280.
7. Pentheroudakis G, Greco FA, Pavlidis N. Molecular assignment of tissue of origin in cancer of unknown primary may not predict response to therapy or outcome: a systematic literature review. Cancer Treat Rev. 2009;35:221–227.
8. Pentheroudakis G, Golfinopoulos V, Pavlidis N. Switching benchmarks in cancer of unknown primary: from autopsy to microarray. Eur J Cancer. 2007;43:2026–2036.
9. NCCN clinical practice guidelines in oncology. National Comprehensive Cancer Network. Last accessed: 4/22/2011