GENERAL PRINCIPLES
Coagulopathy refers to disorders with excessive bleeding because of alterations of proteins involved in the coagulation pathway. It can be divided into two main categories: hereditary and acquired.
![]() Hereditary
Hereditary
![]() von Willebrand disease (vWD)
von Willebrand disease (vWD)
![]() Hemophilia A
Hemophilia A
![]() Hemophilia B
Hemophilia B
![]() Acquired
Acquired
![]() Liver disease
Liver disease
![]() Vitamin K deficiency
Vitamin K deficiency
![]() Disseminated intravascular coagulation
Disseminated intravascular coagulation
![]() Acquired inhibitors of coagulation
Acquired inhibitors of coagulation
HEREDITARY COAGULOPATHY
VON WILLEBRAND DISEASE (vWD)
GENERAL PRINCIPLES
vWD is caused by quantitative or qualitative abnormalities of von Willebrand factor (vWF), resulting in disorders of primary and secondary hemostasis. The usual inheritance pattern of vWD is autosomal dominant; incomplete penetrance may lead to phenotypic variability. The incidence is ~1 in 100 to 400.
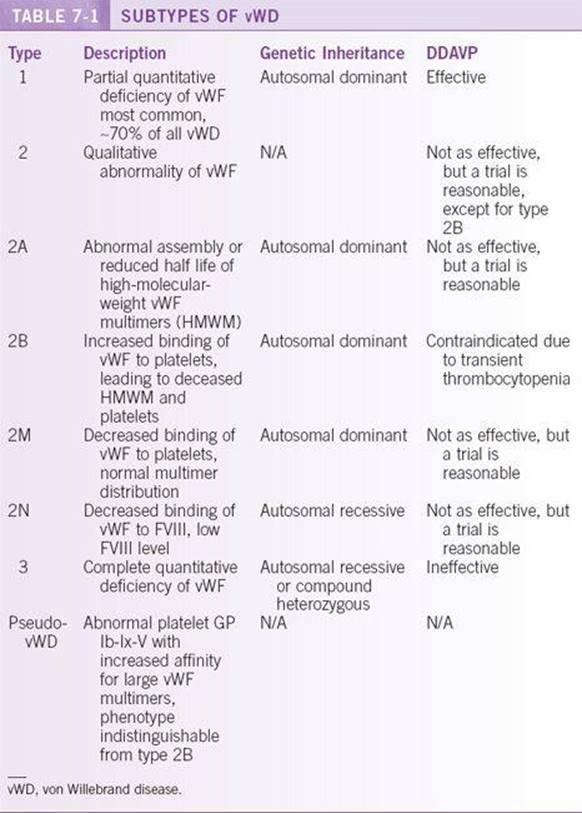
Classification1
The subtypes of vWD are presented in Table 7-1.
Pathophysiology
vWF is a glycoprotein synthesized by endothelial cells and platelets. It is stored in the Weibel-Palade bodies of endothelial cells as well as platelet alpha granules. vWF plays a role in both primary and secondary hemostasis. It mediates the adhesion of platelets at sites of vascular injury, and it stabilizes and transports factor VIII (FVIII) in the circulation. vWF is synthesized as a 300-kD monomer, which then assembles into multimers of various sizes. The largest multimers mediate platelet adhesion.
DIAGNOSIS2,3
Clinical Presentation
![]() Recurrent mucocutaneous bleeding
Recurrent mucocutaneous bleeding
![]() Prolonged bleeding after trauma or surgery
Prolonged bleeding after trauma or surgery
![]() Family history of a bleeding disorder is common.
Family history of a bleeding disorder is common.
![]() In contrast to hemophilia, musculoskeletal bleeding is rare.
In contrast to hemophilia, musculoskeletal bleeding is rare.
![]() Although the majority of affected patients have mild vWD and minor bleeding, patients with the most severe form may suffer life-threatening hemorrhage.
Although the majority of affected patients have mild vWD and minor bleeding, patients with the most severe form may suffer life-threatening hemorrhage.
Differential Diagnosis
![]() Hemophilia A
Hemophilia A
Diagnostic Testing
Laboratories (see Chap. 5 for details)
![]() CBC
CBC
![]() PT (usually normal), aPTT (can be slightly prolonged)
PT (usually normal), aPTT (can be slightly prolonged)
![]() Quantitative vWF antigen (vWF:Ag)
Quantitative vWF antigen (vWF:Ag)
![]() Qualitative vWF assay: Ristocetin cofactor assay (vWF:RCof) and/or vWF collagen-binding assay (vWF:CBA)
Qualitative vWF assay: Ristocetin cofactor assay (vWF:RCof) and/or vWF collagen-binding assay (vWF:CBA)
![]() Factor VIII level
Factor VIII level
![]() vWF multimer assay
vWF multimer assay
![]() Ristocetin-induced platelet aggregation (RIPA) analysis
Ristocetin-induced platelet aggregation (RIPA) analysis
![]() Factor VIII–binding ELISA
Factor VIII–binding ELISA
![]() vWF levels vary with physiological stress, estrogen levels, and other medical comorbidities, therefore levels should be repeated for confirmation.
vWF levels vary with physiological stress, estrogen levels, and other medical comorbidities, therefore levels should be repeated for confirmation.
TREATMENT4
![]() DDAVP (Desmopressin)5
DDAVP (Desmopressin)5
![]() Mechanism of action: Analog of antidiuretic hormone (vasopressin) that lacks vasoactive properties. It acts by releasing endothelial stores of vWF, thereby transiently increasing plasma levels of FVIII and vWF by a factor of 3 to 5 within 30 to 60 minutes of administration.
Mechanism of action: Analog of antidiuretic hormone (vasopressin) that lacks vasoactive properties. It acts by releasing endothelial stores of vWF, thereby transiently increasing plasma levels of FVIII and vWF by a factor of 3 to 5 within 30 to 60 minutes of administration.
![]() Dosage: 0.3 μg/kg IV or SC or 300 μg intranasally
Dosage: 0.3 μg/kg IV or SC or 300 μg intranasally
![]() Dosing frequency: 8 to 10 hours (guided by the half-life of FVIII after DDAVP administration)
Dosing frequency: 8 to 10 hours (guided by the half-life of FVIII after DDAVP administration)
![]() DDAVP should not be used in patients with unstable coronary artery disease, due to concern for ultra large vWF multimer-mediated platelet aggregation in regions of high shear stress near atherosclerotic plaques.
DDAVP should not be used in patients with unstable coronary artery disease, due to concern for ultra large vWF multimer-mediated platelet aggregation in regions of high shear stress near atherosclerotic plaques.
![]() At the time of vWD diagnosis or before elective treatment, a test dose of DDAVP should be administered to establish the individual pattern of response. FVIII levels and vWF:RCof should be measured at 1 and 4 hours after drug administration to determine peak factor levels and clearance rate.
At the time of vWD diagnosis or before elective treatment, a test dose of DDAVP should be administered to establish the individual pattern of response. FVIII levels and vWF:RCof should be measured at 1 and 4 hours after drug administration to determine peak factor levels and clearance rate.
![]() FVIII and vWF concentrates
FVIII and vWF concentrates
![]() The primary treatment for all vWD subtypes when significant bleeding or major surgery is involved
The primary treatment for all vWD subtypes when significant bleeding or major surgery is involved
![]() Virus-inactivated FVIII + vWF concentrates, such as Humate-P and Alphanate, are the products of choice, when available.
Virus-inactivated FVIII + vWF concentrates, such as Humate-P and Alphanate, are the products of choice, when available.
![]() FVIII levels should be obtained every 12 hours on the day concentrates are administered and every 24 hours thereafter. Target FVIII levels are similar to those detailed for hemophilia A, below.
FVIII levels should be obtained every 12 hours on the day concentrates are administered and every 24 hours thereafter. Target FVIII levels are similar to those detailed for hemophilia A, below.
![]() Cryoprecipitate, which contains 5 to 10 times more FVIII and vWF than fresh-frozen plasma, can also be used, although techniques of virus inactivation are not routinely applied to this product.
Cryoprecipitate, which contains 5 to 10 times more FVIII and vWF than fresh-frozen plasma, can also be used, although techniques of virus inactivation are not routinely applied to this product.
![]() Platelet transfusion can be useful, especially when hemorrhage is not controlled despite adequate FVIII levels after FVIII and vWF concentrates.
Platelet transfusion can be useful, especially when hemorrhage is not controlled despite adequate FVIII levels after FVIII and vWF concentrates.
![]() Antifibrinolytic amino acids (aminocaproic acid, tranexamic acid)
Antifibrinolytic amino acids (aminocaproic acid, tranexamic acid)
HEMOPHILIA A6,7
GENERAL PRINCIPLES
Hemophilia A is an inherited coagulation disorder caused by alterations of the gene encoding FVIII, leading to impaired intrinsic pathway function (see Figure 5-1 for intrinsic pathway). The inheritance pattern is X-linked recessive; the gene that encodes FVIII is located on the long arm of the X chromosome (Xq28). Thirty percent of cases are the result of spontaneous mutations. The incidence is approximately 1 in 5000 live male births among all ethnic groups.
DIAGNOSIS
Clinical Presentation
![]() Joint and muscle/soft tissue hemorrhages, easy bruising.
Joint and muscle/soft tissue hemorrhages, easy bruising.
![]() Prolonged bleeding after trauma or surgery; however, usually no excessive bleeding after minor cuts or abrasions.
Prolonged bleeding after trauma or surgery; however, usually no excessive bleeding after minor cuts or abrasions.
![]() Chronic disability can result from hemarthrosis-induced arthropathy and intramuscular bleeding.
Chronic disability can result from hemarthrosis-induced arthropathy and intramuscular bleeding.
Diagnostic Criteria
![]() Laboratory evaluations include
Laboratory evaluations include
![]() Platelet count—normal
Platelet count—normal
![]() PT—normal
PT—normal
![]() PTT—prolonged
PTT—prolonged
![]() PTT mixing study—correct with normal plasma
PTT mixing study—correct with normal plasma
![]() FVIII level—decreased (confirmation of diagnosis)
FVIII level—decreased (confirmation of diagnosis)
![]() von Willebrand factor (vWF) level—normal
von Willebrand factor (vWF) level—normal
![]() Genetic analysis is used for carrier detection and prenatal diagnosis.
Genetic analysis is used for carrier detection and prenatal diagnosis.
![]() Disease severity depends on FVIII level
Disease severity depends on FVIII level
![]() Mild disease—level > 5% of normal
Mild disease—level > 5% of normal
![]() Moderate disease—levels 1% to 5% of normal
Moderate disease—levels 1% to 5% of normal
![]() Severe disease— ≤1% of normal
Severe disease— ≤1% of normal
Differential Diagnosis
![]() Hemophilia B
Hemophilia B
![]() von Willebrand disease (vWD) type 2N
von Willebrand disease (vWD) type 2N
TREATMENT6
![]() Factor VIII replacement
Factor VIII replacement
![]() Used in severe hemophilia, for both major and minor bleeding.
Used in severe hemophilia, for both major and minor bleeding.
![]() Options consist of recombinant FVIII (agent of choice) or purified, virus-attenuated FVIII concentrates from pooled plasma.
Options consist of recombinant FVIII (agent of choice) or purified, virus-attenuated FVIII concentrates from pooled plasma.
![]() Dosage: Each unit/kg of FVIII replacement will raise the plasma FVIII level by 2%. Therefore, the bolus dose = target FVIII level (as below) × weight (kg) × 0.5.
Dosage: Each unit/kg of FVIII replacement will raise the plasma FVIII level by 2%. Therefore, the bolus dose = target FVIII level (as below) × weight (kg) × 0.5.
![]() Target FVIII level:
Target FVIII level:
![]() minor bleeding: ≥30%
minor bleeding: ≥30%
![]() more severe bleeding (e.g., muscle and joint hemorrhages): ≥ 50%
more severe bleeding (e.g., muscle and joint hemorrhages): ≥ 50%
![]() surgical procedures or life-threatening bleeding: ≥80%
surgical procedures or life-threatening bleeding: ≥80%
![]() The half life of FVIII is 8 to 12 hours, therefore, following a loading dose, repeat doses are administered every 8 to 12 hours, adjusted to measured factor VIII levels.
The half life of FVIII is 8 to 12 hours, therefore, following a loading dose, repeat doses are administered every 8 to 12 hours, adjusted to measured factor VIII levels.
![]() FVIII replacement can also be provided by continuous infusion.
FVIII replacement can also be provided by continuous infusion.
![]() Therapy should continue until hemostasis is achieved.
Therapy should continue until hemostasis is achieved.
![]() Postoperative therapy is usually continued for 10 to 14 days. Measuring peak and trough FVIII levels after the first and selected subsequent doses permits dose adjustments to ensure cost-effective therapy.
Postoperative therapy is usually continued for 10 to 14 days. Measuring peak and trough FVIII levels after the first and selected subsequent doses permits dose adjustments to ensure cost-effective therapy.
![]() Recombinant factor VIIa8
Recombinant factor VIIa8
![]() Recombinant factor VIIa promotes hemostasis by activating the extrinsic pathway.
Recombinant factor VIIa promotes hemostasis by activating the extrinsic pathway.
![]() It is currently approved for use in hemophilia A and B patients who have developed inhibitors to FVIII or factor IX (FIX).
It is currently approved for use in hemophilia A and B patients who have developed inhibitors to FVIII or factor IX (FIX).
![]() Dosage: 90 μg/kg every 2 to 3 hours until hemostasis is achieved.
Dosage: 90 μg/kg every 2 to 3 hours until hemostasis is achieved.
![]() DDAVP (Desmopressin)
DDAVP (Desmopressin)
![]() Used in patients with mild disease (FVIII level > 5%) and minor bleeding episodes
Used in patients with mild disease (FVIII level > 5%) and minor bleeding episodes
![]() Details as outlined above for vWD
Details as outlined above for vWD
COMPLICATIONS
![]() Infection from factor concentrates
Infection from factor concentrates
![]() Antibody formation, primarily in patients with severe factor deficiency9
Antibody formation, primarily in patients with severe factor deficiency9
![]() Thrombosis
Thrombosis
![]() Hemophilic arthropathy
Hemophilic arthropathy
![]() Recurrent hemorrhage into one or more joints leading to chronic effusion, joint space narrowing, limited range of motion, atrophy of adjacent musculature, and end stage arthritis
Recurrent hemorrhage into one or more joints leading to chronic effusion, joint space narrowing, limited range of motion, atrophy of adjacent musculature, and end stage arthritis
![]() Can be prevented by prophylactic factor infusions (three times a week for FVIII), intraarticular steroid injection, synovectomy, joint replacement.
Can be prevented by prophylactic factor infusions (three times a week for FVIII), intraarticular steroid injection, synovectomy, joint replacement.
HEMOPHILIA B (TABLE 7-2)
ACQUIRED COAGULOPATHIES
LIVER DISEASE10
All coagulation factors, with the exception of vWF and possibly FVIII, are produced in the liver. Liver dysfunction leads to a number of coagulation abnormalities secondary to decreased factor synthesis, decrease clearance of activated factors, dysregulation of fibrinolytic pathways, and production of abnormal fibrinogen. The coagulopathy of liver disease is usually stable unless the liver synthetic function is rapidly worsening, such as in fulminant hepatic failure. Patients with liver synthetic dysfunction frequently also have thrombocytopenia secondary to portal hypertension and splenic sequestration.

VITAMIN K DEFICIENCY
![]() Vitamin K is a fat-soluble vitamin involved in the posttranslational modification of procoagulant factors II, VII, IX, and X, and anticoagulant proteins C and S. These reactions take place in the liver, where vitamin K serves as a cofactor for the conversion of glutamic acid residues to gamma-carboxyglutamic acid, which facilitates binding of coagulation factors to phospholipid, an essential step in coagulation. Vitamin K must then be recycled by vitamin K epoxide reductase (VKOR) for further gamma-carboxylation to occur. It follows that vitamin K deficiency would render these so-called vitamin K-dependent coagulation factors ineffective.
Vitamin K is a fat-soluble vitamin involved in the posttranslational modification of procoagulant factors II, VII, IX, and X, and anticoagulant proteins C and S. These reactions take place in the liver, where vitamin K serves as a cofactor for the conversion of glutamic acid residues to gamma-carboxyglutamic acid, which facilitates binding of coagulation factors to phospholipid, an essential step in coagulation. Vitamin K must then be recycled by vitamin K epoxide reductase (VKOR) for further gamma-carboxylation to occur. It follows that vitamin K deficiency would render these so-called vitamin K-dependent coagulation factors ineffective.
![]() Disorders of vitamin K most commonly results from the use of warfarin, a VKOR inhibitor. Other causes of Vitamin K deficiency are inadequate dietary intake, which may deplete vitamin K stores in as little as 7 days, malabsorption syndromes, or use of antibiotics, which can eliminate vitamin K–producing bowel flora.
Disorders of vitamin K most commonly results from the use of warfarin, a VKOR inhibitor. Other causes of Vitamin K deficiency are inadequate dietary intake, which may deplete vitamin K stores in as little as 7 days, malabsorption syndromes, or use of antibiotics, which can eliminate vitamin K–producing bowel flora.
![]() Vitamin K deficiency results in prolonged PT that corrects during mixing studies.
Vitamin K deficiency results in prolonged PT that corrects during mixing studies.
![]() Vitamin K repletion may be provided PO, SC, or IV. PO is the preferred route. IV vitamin K is effective but carries the risk of anaphylaxis. To minimize this risk, vitamin K may be diluted in a dextrose or saline solution and slowly administered via an infusion pump. If bleeding is significant or does not respond to vitamin K therapy, factor replacement in the form of fresh-frozen plasma should be administered.
Vitamin K repletion may be provided PO, SC, or IV. PO is the preferred route. IV vitamin K is effective but carries the risk of anaphylaxis. To minimize this risk, vitamin K may be diluted in a dextrose or saline solution and slowly administered via an infusion pump. If bleeding is significant or does not respond to vitamin K therapy, factor replacement in the form of fresh-frozen plasma should be administered.
DISSEMINATED INTRAVASCULAR COAGULATION11
DIC is a hemostatic derangement of multiple etiologies characterized by small- and medium-vessel thrombosis with consumption of platelets and coagulation factors. It leads to microangiopathic hemolytic anemia, thrombocytopenia, and coagulation abnormalities (see Chap. 4).
ACQUIRED INHIBITORS OF COAGULATION
Acquired inhibitors of coagulation are immunoglobulins, usually IgG, which exert their effects by inhibiting the activity or increasing the clearance of coagulation factors. They can be directed against any of the coagulation factors, with inhibitors of FVIII being most common. Inhibitors of coagulation can occur in the following settings:
![]() Extensive blood product exposure in patients with inherited factor deficiency, most commonly in hemophilia A
Extensive blood product exposure in patients with inherited factor deficiency, most commonly in hemophilia A
![]() Lymphoproliferative malignancies
Lymphoproliferative malignancies
![]() Autoimmune disorders such as rheumatoid arthritis or lupus
Autoimmune disorders such as rheumatoid arthritis or lupus
![]() Drug reactions
Drug reactions
![]() Postpartum
Postpartum
Inhibitors cause prolongation of the PT, the aPTT, or both. If the abnormal coagulation studies do not correct with mixing, an inhibitor is likely, and the Bethesda assay can be run to quantify the inhibitor (see Chap. 5 for details). If antiphospholipid antibodies are suspected, a source of phospholipids (such as dilute Russell’s viper venom) can be added to mixed plasma. Correction of the abnormal coagulation tests suggests the presence of antiphospholipid antibodies (see Chap. 6 for more information on antiphospholipid syndrome).
Patients may present with bleeding diathesis, which can be severe and life threatening. Treatment varies depending on the type of inhibitor and severity of bleeding. Therapeutic options include recombinant factor VIIa, immunosuppression with corticosteroids and/or cyclophosphamide, plasma exchange, and intravenous immunoglobulin.
REFERENCES
1. Sadler JE, Budde U, Eikenboom JC, et al. Update on the pathophysiology and classification of von Willebrand disease: a report of the subcommittee on von Willebrand factor. J Thromb Haemost. 2006; 4: 2103–2114.
2. Budde U. Laboratory diagnosis of congenital von Willebrand disease. Semin Thromb Hemost. 2002;28:173–189.
3. Favaloro EJ. Laboratory assessment as a critical component of the appropriate diagnosis and sub-classification of von Willebrand’s disease. Blood Rev. 1999;13:185–204.
4. Mannucci PM. Treatment of von Willebrand’s disease. N Engl J Med. 2004;351:683–694.
5. Mannucci PM. Desmopressin (DDAVP) in the treatment of bleeding disorders: the first 20 years. Blood. 1997;90:2515–2521.
6. Hoyer L. Hemophilia A. N Engl J Med. 1994;330:38–47.
7. Bolton-Maggs PH, Perry DJ, Chalmers EA, et al. The rare coagulation disorders—review with guidelines for management from the United Kingdom Haemophilia Centre Doctors’Organization. Haemophilia. 2004;10:593–628.
8. Butenas S, Brummel KE, Branda RF, Paradis SG, Mann KG, et al. Mechanism of factor VIIa-dependent coagulation in hemophilia blood. Blood. 2002;99:923–930.
9. Sahud MA. Laboratory diagnosis of inhibitors. Semin Thromb Hemost. 2000;26:195–203.
10. Lechner K, Niessner H, Thaler E. Coagulation abnormalities in liver disease. Semin Thromb Hemost. 1977;4:40–56.
11. Levi M, Ten Cate H. Disseminated intravascular coagulation. N Engl J Med. 1999;341:586–592.