Edited by George Jelinek
OUTLINE
26.1 Pre-hospital emergency medicine 841
26.2 Retrieval 846
26.3 Medical issues in disasters 852
26.4 Triage 861
26.5 Emergency care in a humanitarian crisis 865
26.6 Emergency department observation wards 869
26.7 Overcrowding 872
26.8 Rapid response systems and the emergency department 875
26.9 Public health and emergency medicine 881
26.1 Pre-hospital emergency medicine
Stephen A Bernard and Paul A Jennings
Essentials
1 Ambulance dispatch is increasingly becoming computerized and this allows for medical determination of response speed and skill set, as well as telephone instructions for cardiopulmonary resuscitation and first aid.
2 Paramedic care of the critically ill or injured patient is similar to initial evaluation and management by an emergency physician.
3 The role of advanced life-support measures, such as endotracheal intubation and intravenous fluid therapy, in patients with severe trauma or cardiac arrest is uncertain.
4 Patients with chest pain and ST segment elevation on 12-lead electrocardiogram should be triaged to a centre with facilities for percutaneous cardiological intervention. If this transfer cannot be achieved with 1 hour, then pre-hospital thrombolysis should be considered.
5 Paramedics have effective treatment for other medical emergencies including cardiac arrhythmias, acute pulmonary oedema, narcotic drug overdose, seizures, hypoglycaemia and anaphylaxis.
Introduction
Ambulance services have the primary role of providing rapid stretcher transport of patients to an emergency department (ED). Increasingly, paramedics are also trained to provide emergency medical care prior to hospital arrival in a wide range of life-threatening illnesses with the expectation that earlier treatment will improve patient outcomes.
Dispatch
Many countries have a single telephone number for immediate access to the ambulance service in cases of emergency, such as 911 in North America, 999 in the United Kingdom and 000 in Australasia. However, the accurate dispatch of the correct ambulance skill set in the optimal time frame is complex. It is inappropriate to dispatch all ambulances on a ‘code 1’ (lights and sirens) response, since this entails some level of risk to the paramedics and other road users. On the other hand, it may be difficult to identify accurately life-threatening illnesses or injuries using information gained from telephone communication alone, especially from bystanders. Also, it may be inappropriate to dispatch paramedics with advanced life-support training to routine cases where these skills are not required since they then become unavailable for a subsequent call.
In order to have consistent, accurate dispatch of the appropriate skill set in the optimal time frame, many ambulance services are now using computer-aided dispatch programs. These computer programs have structured questions for use by call-takers with limited medical training. Pivotal to accurate telephone dispatch is identification of the chief complaint, followed by subsequent structured questions to determine the severity of the illness. The answers to these questions allow the computerized system to recommend the optimal paramedic skill set and priority of response. This computer algorithm is medically determined according to local protocols and practices and provides consistency of dispatch.
Most ambulance services generally have at least four dispatch codes. A code 1 (or local equivalent terminology) is used for conditions that are considered immediately life threatening. For these, emergency warning devices (lights and sirens) are routinely used. The possibility of life-saving therapy arriving as soon as possible is judged as outweighing the potential hazard of a rapid response. In a code 2 (or equivalent) response, the condition is regarded as being urgent and emergency warning devices may be used only when traffic is heavy. In a code 3 response, an attendance by ambulance within an hour is deemed medically appropriate. Finally, a non-emergency or ‘booked’ call is a transport arranged at a designated time negotiated by the caller and the ambulance service.
Despite continuous developments in computer algorithms, accurate telephone identification of life-threatening conditions may be difficult. For example, identification of patients who are deceased (beyond resuscitation) [1], in cardiac arrest [2], or suffering acute coronary syndrome [3] has been shown to lack the very high sensitivity and specificity that might be expected.
The dispatch centre also has a role for telephone instructions on bystander cardiopulmonary resuscitation [4] and first aid. For conditions that are regarded as non-urgent, the dispatch centre may transfer the call to a ‘referral service’ for the provision of a medical response other than an emergency ambulance. This might include dispatch of a district nurse for a home visit or the provision of simple medical advice with instructions to see a family physician or attend an emergency department if symptoms persist.
Clinical skills
Ambulance treatment protocols vary considerably around the world. Since there are few randomized, controlled trials to provide high quality evidence-based guidance for pre-hospital care, there is still much controversy and considerable variation in the ambulance skill set in different ambulance services.
Many ambulance services provide a number of varying levels of skill set, dispatching ambulance officers trained in basic life support (including defibrillation) to non-emergency or urgent cases (ambulance paramedics) and more highly trained officers (designated as advanced life-support paramedics or intensive-care paramedics) to patients with an immediately life-threatening condition for which advanced life-support skills may be appropriate [5]. In addition, ambulance services may co-respond with other emergency services (such as fire fighters) to provide rapid-response defibrillation.
The evidence for some of the more common pre-hospital interventions is outlined in the following sections.
Trauma care
Pre-hospital trauma care may be considered as either basic trauma life support (clearing of the airway, assisted ventilation with a bag/mask, administration of supplemental oxygen, control of external haemorrhage, spinal immobilization, splinting of fractures and the administration of inhaled analgesics) or advanced trauma life support (ATLS) including intubation of the trachea, intravenous (IV) fluid therapy, decompression of tension pneumothorax and the administration of intravenous analgesia.
Basic trauma life support
On arrival at the scene of the patient with suspected major trauma, paramedics are trained to perform an initial ‘DR-ABCDE’ evaluation which is similar to the approach that has been developed for physicians, namely consideration of dangers, response, airway, breathing, circulation, disability and exposure. Of particular importance in the pre-hospital trauma setting are dangers to paramedics from passing traffic, fallen electrical wires and fire from spillage of fuel.
The initial assessment of the airway and breathing includes the application of cervical immobilization in patients who have a mechanism of injury that suggests a risk of spinal column instability. Although decision instruments have been developed to identify patients in the emergency department who require radiographic imaging [6], the accuracy of these guidelines in the pre-hospital setting is uncertain. Spinal immobilization of many patients with minimal risk of spinal cord injury is uncomfortable and may lead to unnecessary radiographic studies [7]. Therefore, the recommendation to immobilize the neck in all cases of suspected spinal-column injury based on mechanism of injury alone is currently being challenged [8]. On the other hand, if spinal cord injury is suspected, patients should be transported with full spine immobilization [9].
Accurate triage of major trauma patients is an important component of trauma care in cities with designated major trauma centres. Triage tools based on vital signs, injuries and modifying factors, such as age, co-morbidities and mechanism of injury, are used [10]. Paramedic judgement may also have a role, although some injuries, such as occult intra-abdominal injuries, are difficult to detect on clinical grounds [11].
Advanced trauma life support
The role of ATLS by paramedics, particularly intubation of the trachea in comatose patients and intravenous cannulation for fluid therapy in hypotensive patients, is controversial. Although these interventions are routinely used in critically injured patients after hospital admission, studies to date indicate that the provision of ATLS provided by paramedics may not improve outcomes [5,12]. On the other hand, few studies conducted to date have been sufficiently rigorous to allow definitive conclusions and many were conducted in an urban setting with predominantly penetrating trauma rather than blunt trauma. Therefore, many ambulance services continue to authorize advanced airway management and intravenous fluid resuscitation in selected trauma patients, particularly those who are injured some distance from a trauma service.
Intubation
Following severe head injury, many unconscious patients have decreased oxygenation and ventilation during pre-hospital care and this secondary brain injury is associated with worse neurological outcome [13]. In addition, a depressed gag or cough reflex may lead to aspiration of vomit and this may cause a pneumonitis, which may be fatal or result in a prolonged stay in an intensive care unit. To prevent these complications of severe head injury, endotracheal intubation may be performed. This facilitates control of oxygen and carbon dioxide, provides airway protection and is routinely performed in patients with Glasgow coma score<9 following severe head injury after hospital arrival [14].
Most patients with severe head injury maintain a gag or cough reflex and successful intubation requires the use of drugs to facilitate laryngoscopy and placement of the endotracheal tube. The usual approach in the emergency department involves rapid sequence intubation (RSI), which is the administration of both a sedative drug and a rapidly acting muscle-relaxant, such as suxamethonium. It is unclear from the literature as to whether RSI should be performed pre-hospital by paramedics or, alternatively, be performed in an emergency department by appropriately trained physicians.
Pre-hospital RSI performed by paramedics has been reported in numerous studies as having a high success rate [15]. However, it is uncertain whether this procedure is associated with improved outcomes [16]. Recently, a prospective, randomized, trial in adult patients with severe traumatic brain injury reported that paramedic RSI increased the rate of favourable neurological outcome at 6 months when compared to intubation in the hospital by physicians [17]. On the other hand, this study also showed a relatively high incidence of cardiac arrest in the patients who underwent paramedic RSI. Therefore, some uncertainty remains as to the efficacy of this procedure.
Intravenous fluid
Intravenous fluid resuscitation has been shown to worsen outcome in patients with penetrating trauma and hypotension [18]. However, most major trauma in Australasia and Europe is blunt rather than penetrating and few patients require urgent surgical control of haemorrhage. Therefore, the issue of pre-hospital IV fluid for the treatment of hypotension remains the subject of debate.
Supporters of pre-hospital IV fluid therapy suggest that this treatment is intuitively beneficial and that any delay of this therapy increases the adverse effects of prolonged hypotension, which may result in end-organ ischaemia, leading to multiorgan system failure and increased morbidity and mortality. On the other hand, opponents of pre-hospital IV fluid therapy suggest that this therapy prior to surgical control in patients with uncontrolled bleeding increases blood loss due to increased blood pressure, dilution coagulopathy and hypothermia from large volumes of unwarmed IV fluid. Any additional blood loss would increase transfusion requirements and could be associated with increased morbidity and mortality.
There is no evidence from clinical trials for benefit of the administration of IV fluid to bleeding patients in the pre-hospital setting. A meta-analysis of the studies to date suggests that pre-hospital IV fluid does not improve outcomes [5]. Nevertheless, if intravenous fluid is given to patients with hypotension and severe head injury, crystalloid rather than colloid should be given, particularly in hypotensive patients with severe traumatic brain injury [19].
Analgesia
The administration of effective analgesia in the pre-hospital setting for traumatic pain remains a difficult issue for ambulance services. Many paramedics are not trained to administer IV therapy and treatment options are, therefore, limited to inhaled therapy.
Inhaled analgesic treatments include methoxyflurane and oxygen/nitrous oxide. However, while the former is reasonably effective [20], there are concerns with the administration of this agent in an enclosed space, such as the rear of an ambulance, because of the perceived risk of repeated exposures of these analgesics to the paramedics.
Alternatively, the training of paramedics in the insertion of an IV cannula and administration of small increments of IV morphine is increasingly regarded as a feasible alternative to inhalation analgesia. Alternative routes of narcotic administration, such as intranasal administration, are the subject of current studies. For example, the use of intranasal fentanyl has been shown to be equivalent to intravenous morphine [21].
An alternative analgesic agent for paramedic use is ketamine. Ketamine, in addition to morphine, has been shown to be superior to morphine alone for traumatic pain. In a randomized, controlled trial, adult patients with moderate to severe traumatic pain were randomized to receive either 5 mg of morphine followed by ketamine, or morphine alone [22]. Those who received morphine and ketamine reported a significant pain score reduction compared to those who received morphine alone. However, the rate of adverse effects, such as nausea and dysphoria, was higher following ketamine compared with morphine.
Cardiac care
Cardiac arrest
In 1966, external defibrillation was introduced into pre-hospital care and this led to the development of ‘mobile coronary care units’ in many countries for the delivery of advanced cardiac care for the patient with suspected myocardial ischaemia [23]. This approach was subsequently extended to rapid response for defibrillation of patients in cardiac arrest. Protocols for the management of pre-hospital cardiac arrest are based on the concept of the ‘chain of survival’, which includes an immediate call to the ambulance service, the initiation of bystander CPR, early defibrillation and advanced cardiac life support (intubation and drug therapy).
The patient in cardiac arrest represents the most time-critical patient attended by ambulance services. For the patient with ventricular fibrillation, each minute increase from time of collapse to defibrillation is associated with an increase in mortality of approximately 10%. However, most ambulance services have urban response times that average 8–9 minutes. Since there may be 2 minutes between collapse and dispatch and 1 minute between arrival at the scene to delivery of the first defibrillation, total time from collapse to defibrillation would usually be approximately 12 minutes. Therefore, current survival rates for witnessed cardiac arrest in urban areas are low [24] and there are even fewer survivors in rural areas [25].
The most effective strategy to improve outcomes would be to decrease ambulance response times. However, this would require very significant increases in ambulance resources and would be an expensive strategy in terms of cost per life saved. Alternatively, response times to cardiac arrest patients may be reduced with the use of co-response by first responders equipped with defibrillators. Such a first responder programme has been introduced in Melbourne, Australia with promising results [26].
The role of advanced cardiac life support (ACLS) during cardiac arrest remains controversial [27]. For example, in a randomized, controlled trial comparing a basic life-support approach with an advanced life-support approach, the rate of survival to hospital discharge was 10.5% for the ACLS group compared with 9.2% for the no ACLS group (P=0.61) [28]. This finding of a lack of efficacy of ACLS during cardiac arrest remained after adjustment for underlying differences between the groups in the rates of ventricular fibrillation, response interval, witnessed arrest or arrest in a public location.
Therapeutic hypothermia after resuscitation from cardiac arrest is used in many hospitals, particularly when the initial cardiac arrest rhythm is ventricular fibrillation. A number of clinical trials have tested whether therapeutic hypothermia should be initiated by paramedics after resuscitation using a bolus of cold IV fluid [29,30] or intranasal cooling [31]; however, the results of these studies do not currently support this therapy prior to hospital arrival.
Acute coronary syndromes
Most ambulance services have protocols for the management of the patient with chest pain where the cause is suspected as an acute coronary syndrome. These protocols usually include administration of aspirin and sublingual trinitrates followed by rapid transfer to an emergency department for definitive diagnosis and management. In addition, pain relief using intravenous morphine may be given by advanced life-support paramedics. The role of supplemental oxygen in patients with ST segment elevation myocardial ischaemia (STEMI) but without hypoxia remains uncertain [32].
While these interventions may decrease symptoms, more recent strategies to improve overall outcomes involve triage by paramedics of patients with STEMI using 12-lead electrocardiography to centres for interventional cardiology [33]. For patients with STEMI who are greater than 1 hour to a cardiac catheterization laboratory (i.e. rural patients), pre- hospital thrombolysis may be considered. In a recent European trial, patients with STEMI who presented within 3 hours after symptom onset but who were unable to undergo primary percutaneous coronary intervention (PCI) within 1 hour were assigned to undergo either primary PCI or fibrinolytic therapy [34]. The primary endpoint of death, shock, congestive heart failure or reinfarction occurred in 12.4% of patients in the pre-hospital fibrinolysis group and in 14.3% of patients in the primary PCI group (relative risk in the fibrinolysis group, 0.86; 95% confidence interval, 0.68 to 1.09; P=0.21). The rates of intracranial bleeding were similar in the two groups (after the dose of fibrinolysis was halved in the over 75 years patients). These data suggest that pre-hospital thrombolytic therapy is appropriate if there is a delay of greater than 1 hour in transport to a definitive centre for PCI.
Cardiac arrhythmias
Some patients with an acute coronary syndrome develop a cardiac arrhythmia during ambulance care. Pulseless ventricular tachycardia is treated with immediate defibrillation and amiodarone by slow IV infusion is recommended for ventricular tachycardia where a pulse is palpable and the patient is alert [35]. However, the pre-hospital drug treatment of supraventricular tachycardia is more controversial. While the use of verapamil or adenosine appears to be equivalent in efficacy [36], many ambulance services require the patient to be transported for 12-lead electrocardiography and management of the supraventricular tachyarrhythmia in an emergency department.
Pulmonary oedema
During myocardial ischaemia, the patient may develop pulmonary oedema and, in these patients, the use of oxygen and glyceryl trinitrates is regarded as useful [37]. Despite common use of non-invasive ventilation (NIV) in the emergency department for patients with acute pulmonarty oedema, pre-hospital continuous positive airway pressure for this indication has not been widely adopted, since the equipment is expensive and oxygen consumption is high. Nevertheless, there is some evidence that continuous positive airway pressure is feasible in the pre-hospital setting, may reduce the need for intubation and may reduce short-term morbidity [38].
Other medical emergencies
Stroke
Early identification and effective management of stroke aims to promote optimal recovery. The ambulance plays an important role in stroke management by triaging patients with suspected stroke to an appropriate hospital. Use of a validated stroke screen tool has been shown to increase diagnostic accuracy in identifying stoke and thus facilitate transfer to a stroke centre. There are a number of published stroke screening tools for paramedic use such as the Los Angeles Motor Score (LAMS) [39] and the Melbourne Ambulance Stroke Score [40] that have been shown to be effective in accurately identifying stroke. Patients suspected to be suffering from a stroke should be preferentially transported to a facility with stroke expertise.
Hypoglycaemia
The patient with hypoglycaemia due to relative excess of exogenous injected insulin will suffer neurological injury unless the blood glucose level is promptly corrected. Treatment of the conscious patient involves orally administered dextrose. For unconscious patients, intravenous 20% dextrose should be administered. For paramedics who are not trained to insert IV cannulae or where IV access is not possible, the administration of intramuscular glucagon is also effective, although this is associated with an increase in the time to full consciousness [41].
Patients who respond to treatment may refuse transport to hospital since they feel they have recovered. However, patients on oral hypoglycaemic agents may later develop recurrent hypoglycaemia [42]. Therefore, transport to hospital in this patient group is recommended.
Narcotic overdose
Patients who inject narcotic drugs may suffer coma and respiratory depression which is readily reversed by naloxone. However, the administration of IV naloxone by paramedics is somewhat problematic, since IV access may be difficult and the half-life of IV naloxone (approximately 20 minutes) may be shorter than the injected narcotic. If the patient awakens and leaves medical care, there may also be a recurrence of sedation. Therefore, many ambulance services administer naloxone via the intramuscular or subcutaneous route. While the absorption via this route may be slower, overall, the time to return of normal respirations is equivalent. To avoid the use of needles, naloxone may also be administered via the intranasal route and this has an equivalent onset time to intramuscular naloxone [43].
Anaphylaxis
Many patients with known severe anaphylaxis are prescribed adrenaline (epinephrine) by their physician for self-administration. The use of intramuscular adrenaline (epinephrine) by paramedics is a safe and effective pre-hospital therapy [44]. Generally, a dose of adrenaline 0.3 mg IM together with IV fluid therapy is recommended as first-line therapy for anaphylaxis with intravenous adrenaline reserved for patients who become severely hypotensive.
Seizures
Out-of-hospital status epilepticus is also regarded as a time-critical medical emergency. The first-line treatment of status epilepticus is usually a benzodiazepine. For many years, this was provided using the IV or rectal route of administration. More recently, there are supportive data that intramuscular midazolam is equally effective to intravenous benzodiazepine [45]. Many ambulance services therefore now authorize midazolam 0.1 mg/kg in the adult patient with seizure, with a half dose considered in older patients.
Controversies and future directions
![]() Computer-aided dispatch algorithms require further improvement to increase the sensitivity and specificity for the detection of life-threatening emergencies.
Computer-aided dispatch algorithms require further improvement to increase the sensitivity and specificity for the detection of life-threatening emergencies.
![]() Advanced life support, including intubation and intravenous fluid therapy, by ambulance paramedics for the severe trauma and cardiac arrest patient is unproven and expensive. Further randomized, controlled trials are required to justify these interventions.
Advanced life support, including intubation and intravenous fluid therapy, by ambulance paramedics for the severe trauma and cardiac arrest patient is unproven and expensive. Further randomized, controlled trials are required to justify these interventions.
![]() Patients with chest pain and ST segment elevation myocardial ischaemia should be identified with 12-lead electrocardiography and triaged to a centre with facilities for interventional cardiology. There is a possible role for pre-hospital thrombolysis if time to a cardiac catheterization exceeds 1 hour.
Patients with chest pain and ST segment elevation myocardial ischaemia should be identified with 12-lead electrocardiography and triaged to a centre with facilities for interventional cardiology. There is a possible role for pre-hospital thrombolysis if time to a cardiac catheterization exceeds 1 hour.
![]() Routine application of cervical spine immobilization interventions on the basis of mechanism of injury alone is being challenged. The utility of clinical examination and decision support tools to identify accurately those at increased risk of spinal injury requires further research.
Routine application of cervical spine immobilization interventions on the basis of mechanism of injury alone is being challenged. The utility of clinical examination and decision support tools to identify accurately those at increased risk of spinal injury requires further research.
References
1. Harvey L, Woollard M. Outcome of patients identified as dead (beyond resuscitation) at the point of the emergency call. Emerg Med J. 2004;21:367–369.
2. Flynn J, Archer F, Morgans A. Sensitivity and specificity of the medical priority dispatch system in detecting cardiac arrest emergency calls in Melbourne. Prehosp Disaster Med. 2006;21:72–76.
3. Deakin CD, Sherwood DM, Smith A, Cassidy M. Does telephone triage of emergency (999) calls using advanced medical priority dispatch (AMPDS) with Department of Health (DH) call prioritisation effectively identify patients with an acute coronary syndrome? An audit of 42,657 emergency calls to Hampshire Ambulance Service NHS Trust. Emerg Med J. 2006;23:232–235.
4. Lerner EB, Rea TD, Bobrow BJ, et al. American Heart Association Emergency Cardiovascular Care Committee; Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation Emergency medical service dispatch cardiopulmonary resuscitation prearrival instructions to improve survival from out-of-hospital cardiac arrest: a scientific statement from the American Heart Association. Circulation. 2012;125:648–655.
5. Ryynänen OP, Iirola T, Reitala J. Is advanced life support better than basic life support in prehospital care? A systematic review. Scand J Trauma Resusc Emerg Med. 2010;18:62–65.
6. Hoffman JR, Mower WR, Wolfson AB, et al. Validity of a set of clinical criteria to rule out injury to the cervical spine in patients with blunt trauma National Emergency X-Radiography Utilization study (NEXUS) Group. N Engl J Med. 2000;343:94–99.
7. Armstrong BP, Simpson HK, Crouch R, Deakin CD. Prehospital clearance of the cervical spine: does it need to be a pain in the neck? Emerg Med J. 2007;24:501–503.
8. Haut ER, Kalish BT, Efron DT, et al. Spine immobilization in penetrating trauma: more harm than good? J Trauma. 2010;68:115–120.
9. Ahn H, Singh J, Nathens A, et al. Pre-hospital care management of a potential spinal cord injured patient: a systematic review of the literature and evidence-based guidelines. J Neurotrauma. 2011;28:1341–1361.
10. Sartorius D, Le Manach Y, David JS, et al. Mechanism, Glasgow coma scale, age, and arterial pressure (MGAP): a new simple prehospital triage score to predict mortality in trauma patients. Crit Care Med. 2010;38:831–837.
11. Mulholland SA, Gabbe BJ, Cameron P, Victorian State Trauma Outcomes Registry and Monitoring Group (VSTORM). Is paramedic judgement useful in prehospital trauma triage? Injury. 2005;36:1298–1305.
12. Seamon MJ, Doane SM, Gaughan JP, et al. Prehospital interventions for penetrating trauma victims: a prospective comparison between advanced life support and basic life support. Injury 4 Feb 2013; [Epub ahead of print.].
13. Chi JH, Knudson MM, Vassar MJ, et al. Prehospital hypoxia affects outcome in patients with traumatic brain injury: a prospective multicenter study. J Trauma. 2006;61:1134–1141.
14. <https://www.braintrauma.org/coma-guidelines> [Accessed Mar. 2013].
15. Hubble MW, Brown L, Wilfong DA, et al. A meta-analysis of prehospital airway control techniques part I: orotracheal and nasotracheal intubation success rates. Prehosp Emerg Care. 2010;14:377–401.
16. Bernard SA. Paramedic intubation of patients with severe head injury: a review of current Australian practice and recommendations for change. Emerg Med Australas. 2006;18:221–228.
17. Bernard SA, Nguyen V, Cameron P, et al. Prehospital rapid sequence intubation improves functional outcome for patients with severe traumatic brain injury: a randomized controlled trial. Ann Surg. 2010;252:959–965.
18. Bickell W, Pepe P, Mattox K, et al. Immediate versus delayed fluid resuscitation for hypotensive patients with penetrating torso injuries. N Engl J Med. 1994;331:1105–1108.
19. Cooper DJ, Myburgh J, Heritier S, et al. Albumin resuscitation for traumatic brain injury: is intracranial hypertension the cause of increased mortality?. J Neurotrauma 21 Mar. 2013; [Epub ahead of print.].
20. Buntine P, Thom O, Babl F. Prehospital analgesia in adults using inhaled methoxyflurane. Emerg Med Australas. 2007;19:509–514.
21. Rickard C, O’Meara P, McGrail M. A randomized controlled trial of intranasal fentanyl vs intravenous morphine for analgesia in the prehospital setting. Am J Emerg Med. 2007;25:911–917.
22. Jennings P, Cameron P, Bernard SA, Fitzgerald M. Morphine and ketamine is superior to morphine alone for prehospital trauma analgesia: a randomized controlled trial. Ann Emerg Med. 2012;59:497–503.
23. Eisenberg MS. The C J Shanaberger lecture: the evolution of prehospital cardiac care: 1966–2006 and beyond. Prehosp Emerg Care. 2006;10:411–417.
24. Fridman M, Barnes V, Whyman A, et al. A model of survival following pre-hospital cardiac arrest based on the Victorian Ambulance Cardiac Arrest Register. Resuscitation. 2007;75:311–322.
25. Jennings PA, Cameron P, Walker T. Out-of-hospital cardiac arrest in Victoria: rural and urban outcomes. Med J Aust. 2006;185:135–139.
26. Smith KL, McNeill JJ, the Emergency Medical Response Steering Committee. Cardiac arrests treated by ambulance paramedics and fire fighters. Med J Aust. 2002;177:305–309.
27. Stiell IG, Wells GA, Field B, et al. Advanced cardiac life support in out-of-hospital cardiac arrest. N Engl J Med. 2004;351:647–656.
28. Olasveengen TM, Sunde K, Brunborg C, et al. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trial. J Am Med Assoc. 2009;302:2222–2229.
29. Bernard SA, Smith K, Cameron P, Rapid Infusion of Cold Hartmanns (RICH) Investigators, et al. Induction of therapeutic hypothermia by paramedics after resuscitation from out-of-hospital ventricular fibrillation cardiac arrest. A randomized controlled trial Circulation. 2010;122:737–742.
30. Bernard SA, Smith K, Cameron P, Rapid Infusion of Cold Hartmanns (RICH) Investigators, et al. Induction of therapeutic hypothermia by paramedics after resuscitation from out-of-hospital non-ventricular fibrillation cardiac arrest. Crit Care Med. 2012;40:747–753.
31. Castrén M, Nordberg P, Svensson L. Intra-arrest transnasal evaporative cooling: a randomized, prehospital, multicenter study (PRINCE: Pre-ROSC IntraNasal Cooling Effectiveness). Circulation. 2010;122:729–736.
32. Stub D, Smith K, Bernard S, AVOID Investigators, et al. A randomised controlled trial of air verses oxygen in myocardial infarction study (AVOID Study). Am Heart J. 2012;163:339–345.
33. Le May MR, Davies RF, Dionne R, et al. Comparison of early mortality of paramedic-diagnosed ST-segment elevation myocardial infarction with immediate transport to a designated primary percutaneous coronary intervention center to that of similar patients transported to the nearest hospital. Am J Cardiol. 2006;98:1329–1333.
34. Armstrong PW, Gershlick AH. Fibrinolysis or primary PCI in ST-segment elevation myocardial infarction. N Engl J Med 2013; In: http://dx.doi.org/10.1056/NEJMoa1301092; 2013.
35. Neumar RW, Otto CW, Link MS, et al. American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care part 8: adult advanced cardiovascular life support. Circulation. 2010;122:S729–S767.
36. Delaney B, Loy J, Kelly AM. The relative efficacy of adenosine versus verapamil for the treatment of stable paroxysmal supraventricular tachycardia in adults: a meta-analysis. Eur J Emerg Med. 2011;18:148–152.
37. Stiell IG, Spaite DW, Field B, et al. Advanced life support for out-of-hospital respiratory distress. N Engl J Med. 2007;356:2156–2164.
38. Plaisance P, Pirracchio R, Berton C. A randomized study of out-of-hospital continuous positive airway pressure for acute cardiogenic pulmoinary oedema: physiology and clinical effects. Eur Heart J. 2007;28:2895–2901.
39. Nazliel B, Starkman S, Liebeskind DS, et al. A brief prehospital stroke severity scale identifies ischemic stroke patients harboring persisting large arterial occlusions. Stroke. 2008;39:2264–2267.
40. Bray JE, Coughlan K, Barger B, Bladin C. Paramedic diagnosis of stroke: examining long-term use of the Melbourne Ambulance Stroke Screen (MASS) in the field. Stroke. 2010;41:1363–1366.
41. Howell MA, Guly HR. A comparison of glucagon and glucose in prehospital hypoglycaemia. J Accid Emerg Med. 1997;14:30–32.
42. Fitzpatrick D, Duncan EA. Improving post-hypoglycaemic patient safety in the prehospital environment: a systematic review. Emerg Med J. 2009;26:472–478.
43. Kelly AM, Kerr D, Dietze P. Randomised trial of intranasal versus intramuscular naloxone in prehospital treatment for suspected opioid overdose. Med J Aust. 2005;182:24–27.
44. Jacobsen RC, Millin MG. The use of epinephrine for out-of-hospital treatment of anaphylaxis: resource document for the National Association of EMS Physicians position statement. Prehosp Emerg Care. 2011;15:570–576.
45. Silbergleit R, Durkalski V, Lowenstein D, NETT Investigators, et al. Intramuscular versus intravenous therapy for prehospital status epilepticus. N Engl J Med. 2012;366:591–600.
26.2 Retrieval
Marcus Kennedy
Essentials
1 Mature retrieval systems act as a single point of entry for the referrer, preferably providing services by initiation of a single call to a system-wide phone number.
2 Retrieved patients are often unstable, at the margin of physiological compensation and in need of specialized investigation and intervention. They are often at that phase of an emergency presentation where diagnosis is incomplete, treatment is problem-focused and risk is high. This setting therefore requires special expertise, risk-averse processes and fail-safe systems characterized by anticipation, redundancy, rapid response and reliability.
3 The retrieval environment poses particular risk and technical training regarding platforms, procedures, relevant legislation, communication methods, rescue and escape procedures and equipment performance characteristics is needed.
4 Retrieval crew members must be trained to critical care standard. The skill set they provide must meet the clinical needs of the patient.
5 It is likely that the most complex patients receiving the highest levels of support are also the most likely to be exposed to in-transit critical incidents or equipment failure. Clinical practice in this setting requires the anticipation of such events, vigilance to detect them and rehearsed and standardized problem-solving algorithms to rectify them.
Retrieval systems
The definition of retrieval varies by jurisdiction, however, it includes the interhospital transfer of critical patients using specialized clinical staff, transport platforms and equipment. In most regions, this definition extends to the pre-hospital environment when medical staff crewing is deployed and, in this setting, is termed primary retrieval. In various systems, staff may include medical, nursing, advanced life support (ALS) paramedic or intensive care paramedic (or equivalents) in a range of combinations or crew-mix. Retrieval generally involves the transfer of patients with critical illness or life-threatening injury: situations where the patient requires the highest levels of clinical care and vigilance. Retrieved patients are often unstable, at the margin of physiological compensation and in need of specialized investigation and intervention. They are often at that phase of an emergency presentation where diagnosis is incomplete, treatment is problem-focused and risk is high. This setting therefore requires special expertise, risk-averse processes and fail-safe systems characterized by anticipation, redundancy, rapid response and reliability.
Retrieval is a coordinated process that provides specialized assessment and management, prior to and during transfer of critically ill patients from situations where resources or services are inadequate, to a destination where definitive care can be provided. It aims to deliver the same or higher level of clinical care as that available at the point of referral, thus ensuring that the patient is not exposed to any reduction in the quality of clinical care, despite the inherent risks of the transport environment.
The need for retrieval is related to the limitations of health facilities and the geography of populations. It is a reasonable premise that rural communities have a right to equitable and timely access to critical care medicine; however, it is recognized that there is often an urban/rural divide in regard to the accessibility of healthcare generally and to specialized critical care in particular. Key clinical ‘gap’ areas exist at both urban and rural and regional levels in regard to trauma, neurosurgery, cardiac and neonatal and paediatric critical care. Advances in medicine and technology are inevitably (at least initially) usually concentrated in major metropolitan centres, thus increasing the need for critical patient transport (e.g. coronary percutaneous procedures, interventional radiology, such as angio-embolization, major trauma centres and paediatric tertiary and quaternary care hospitals. Given that such divides exist and that critical-care transfer is inevitable, retrieval medicine aims to ensure quality of care in transfer in distinction to the somewhat ad hoc approach to irregular critical-care transfers that otherwise may be the case in less systematized approaches.
Retrieval systems are often a product of their geography and some services have evolved due to their unique environment. Examples include Nordic systems and alpine systems that have emerged from the demands of challenging altitude and temperature extremes, urban trauma service (such as HEMS London) and systems driven by the tyranny of distance, such as the Queensland retrieval system.
Retrieval systems vary by state and internationally. There are no uniform system designs or standards and, consequently, services vary in their use of transport platforms and crew types (nurse, paramedic, doctor). Staff may be employed by a health department, ambulance service, by contract with a private provider or a retrieval service may utilize hospital personnel. A state service may incorporate several retrieval service providers with central coordination; alternately, systems exist with local governance and responsibility at a district or area level. Transport platforms are generally state owned and operated or contracted; however, non-government-owned helicopters may be part of a state system (and have historically received both benevolent and state funding). In the past, such services were the mainstay of retrieval practice and were often initiated by passionate volunteers, being funded by community donations, corporate sponsorship and government grants. Governance systems for such services and their coordination and performance responsibilities were typically variable. Consequently, retrieval systems have evolved, leading to increased systematization and corporate and clinical governance, aiming at reduction in variation, greater accountability and increased reliability at the system level.
Most countries have progressively moved towards centralized state systems. These are characterized by central coordination centres that use nurses, paramedics and doctors who work together utilizing their complementary skills and experience. Neonatal, paediatric, perinatal and adult retrieval services may be integrated, co-located or separate; however, the trend of recent years is to co-locate these services with common governance, to allow synergies to be realized in regard to operational processes, infrastructure, management, education, research, response platforms and clinical staff.
Most retrieval services have developed similar systems for management of the generic operational processes of: patient referral, case coordination, response and logistics, clinical intervention, and destination determination (Table 26.2.1). In addition, these are usually supported by a formal array of governance elements (Table 26.2.2).
Table 26.2.1
Elements of operational management of retrieval services
Programme guidelines
Quality reporting
Reporting to Medical Standards Committee
Management guidelines
Data management
Organizational structure
Contracts and memoranda of understanding
Budget and financial system
Annual and strategic planning
Management and data reports
Table 26.2.2
Elements of clinical governance of retrieval services
Guidelines for coordinators
Guidelines for retrieval clinicians
Support staff guidelines
Equipment management systems
Orientation and training
Professional development
Clinical documentation
Case follow up and feedback
Case review and audit
Incident management
Indicator measurement
Credentialling
Performance management
In addition, states may legislate [1] or learned and academic bodies may publish guidelines and standards to promote safe systems of patient transfer, particularly in the critical-care sector [2].
Retrieval processes
Retrieval coordination
Case coordination is at the heart of all retrieval systems. As a process it commences with the initiation of contact from a referral site. It is important for referrers to understand the indications for retrieval and to have clear guidelines (both system and local) to encourage early referral and good decision making. Statewide trauma systems and neonatal paediatric care systems often have well established transfer criteria; however, processes for other clinical groups are often less developed and may be ad hoc. Mature retrieval systems act as a single point of entry for the referrer, preferably providing services by initiation of a single call to a system-wide phone number. Coordination staff are appropriately qualified senior clinicians, with specialized training and knowledge. Case coordination fundamentally answers: what are the needs of the referrer and their patient? Are the needs for clinical advice, for organization of transport and crew or for assistance in obtaining an appropriate destination for a critical patient? The coordinator must determine quickly and efficiently the planning and intervention priorities for each case. These may be for immediate care or advice, immediate response, destination planning or consideration of complex decisions involving logistics, crew or transport platforms. Coordinators need to display leadership while at all times taking a systems perspective and avoiding tunnel vision or task fixation.
Coordination must be provided through high performance organizations and, typically, utilizes sophisticated communication technologies, such as multiparty conference calls, telehealth videoconferencing, case recording and comprehensive data management systems.
Coordination of retrieval also implies an ongoing process of communication and feedback with the referrer of case progress, estimated response times and knowledge of patient status changes. During the response and transfer phase the coordination centre maintains communication with response teams, providing logistic support and mission oversight.
Transport platforms
Retrieval services generally use road, rotary wing (helicopter), or fixed wing aircraft response and transport platforms. For international retrieval missions, commercial larger jet transport is used and, in uncommon settings, aquatic transport platforms may be used. In consideration of platform selection for a mission, clinical factors must be factored first; these will include need for pressurization, need for space for specialized crew or equipment and patient size. Further to these factors, urgency (of response or return leg or both outbound and return components), distance to referral hospital, availability of helipads at referral and destination hospitals and need to minimize the out-of-hospital time for the patient. Heightened risk for patients in transit is experienced during platform transfers (from bed to trolley to ambulance to aircraft stretcher and so on) and, in general terms, in the out-of-hospital setting. Minimization of number of patient transfers and the out-of-hospital time for the critical care retrieval patient are important principles.
Road transport platforms should be specifically designed and fitted out for retrieval purposes to minimize variation (improving crew performance and safety) and the risk of ad hoc unsecured equipment placement. Use of helicopters (with crews of appropriate skill mix) in retrieval response has been demonstrated to improve patient outcomes [3,4], particularly patients with severe trauma and others with a need for time-critical interventions. In general, helicopter transfer is considered for retrieval of patients approximately 75–175 km from base, with road response used for shorter transfers and fixed wing for longer. These broad recommendations vary depending on road, geography and climatic conditions and on the performance characteristics and landing options for individual aircraft. Fixed wing transfers have the advantage of providing a (usually) pressurized aircraft, greater speed and comfort, more space and a controlled temperature. Rotary wing aircraft have advantages of door-to-door transfer where helipads exist at referral and destination sites, the primary response capability and the potential to avoid road transport legs, and multiple patient transfers. Road transfer offers spatial flexibility, door-to-door transfer and cost efficiency (Fig. 26.2.1).

FIG. 26.2.1 Retrieval transport platform allocation grid for fixed wing, helicopter and road transport based on distance vs transport urgency of either the response leg or the patient transfer leg of the retrieval mission.
Crew
Staff selected for roles in retrieval must meet required professional and personal standards. Critical-care capability is essential and medical staff specialist training in a critical-care specialty is desirable. Similarly, nursing and paramedic staff must be trained to intensive care practitioner level. In addition, all staff must have specific training in management of the retrieval environment, clinical care in transport settings and personal and crew behaviours.
The retrieval environment poses particular risk and technical training regarding platforms, procedures, relevant legislation, communication methods, rescue and escape procedures and equipment performance characteristics is needed. Training in clinical care during retrieval needs to ensure capability in management of the complete range of critical care, trauma and intensive care scenarios and an ability to apply depth of clinical knowledge to the relatively compact window of patient care that the retrieval mission represents. Practitioners need to understand in a retrieval setting that an intervention may be possible and ideal while also being inappropriate and inefficient or, that an intervention may be desirable but not be possible or practical. Compromise and pragmatism have a role in pre- and interhospital transfer particularly where priority exists for reaching a definitive care destination. Training in personal and crew behaviours is necessary to optimize the cohesiveness and functionality of the retrieval team – formal exposure to crisis resource management tools is a standard component of aeromedical and road-based retrieval education [5]. In interaction with referring practitioners and primary responders, the retrieval team needs to exhibit empathy, listening skills and professional behaviours – avoiding arrogance, premature conclusions or judgemental behaviour. The training and knowledge base required is significant, therefore training processes must be formalized and must be supported by ongoing professional development and regular credentialling in addition to compliance with relevant regulations.
Crew safety is paramount, so personal protective equipment and clothing which meets aviation and ambulance service standards is mandatory. Safety risk arises also in long and overnight missions and crewing must be adequate to allow sharing of clinical vigilance duties and patient interventions at times of fatigue and to allow for adequate breaks and rest.
Retrieval services play a major role in disaster response and management and generally provide a significant component of the early response to such incidents. Retrieval services and, in particular, their coordination processes are also key to the distribution and reception phase of the disaster response – providing system overview of capability and capacity of health services to receive victims. Retrieval staff must therefore be trained to expert status in this discipline [2,6].
Skill sets
Retrieval medicine and primary response aeromedical settings provide the most challenging of all clinical environments and, therefore, choice of staff skill sets and professional team makeup is fundamental to optimizing clinical outcomes. The central tenets of this clinical environment are that a critical-care retrieval team must consist of (at least) two professionals [6]. They must be trained to critical-care standard and work within their core scope of practice. The skill set they provide must meet the clinical needs of the patient. In most national and international jurisdictions, blended medical practitioner and paramedic or nursing crews satisfy these tenets. Significant literature supports the role of medical practitioners in this environment due to the additional diagnostic capability, procedural range, extent of knowledge and depth of clinical understanding they contribute [7]. Such skills are complemented by the skill set of critical-care-trained nursing staff. Paramedic staff contribute substantial critical-care capability (depending on individual jurisdictional training levels) together with expertise in the transport and pre-hospital scene environments. Crews comprised of paramedic or nursing staff paired in various combinations and without a medical crew member are appropriate for lower risk critical-care transfers, or for non-critical-care retrieval. Skill set needs to match the requirements of the patient in the basic dimensions of clinical complexity and physiological stability; the more unstable and complex patient clearly requiring a higher skill mix in the retrieval team. In rare situations, and where life-saving intervention may be possible, the transport of highly specialized clinical staff to the patient may be appropriate and should be considered, for example, transporting a surgeon to perform an infield amputation on an entrapped patient (Fig. 26.2.2).

FIG. 26.2.2 Crew skill set matches the clinical requirements of the patient.
Equipment
Within a retrieval service, equipment should be standardized as far as possible. Response kits and platform layouts will then be familiar to all practitioners at all times, including at night and during uncontrolled clinical emergencies. Equipment must meet the needs of the patient population or therapeutic interventions and must consider the operating environment, mission duration, availability of electrical power in transport platforms, oxygen consumption and standard oxygen supplies available in vehicles. Stretchers and equipment bridges must meet aviation engineering standards, as must all electrical equipment that may be used in aircraft.
On all missions, the retrieval practitioner must have access to the complete range of airway management equipment including a difficult airway kit, cardiac monitor defibrillator pacer, multiple infusion pumps appropriate for inotrope infusions, a transport ventilator capable of complex respiratory support, invasive pressure monitoring, temperature monitoring, capnography and oximetry. All equipment must be maintained to the highest level of biomedical support and be fitted with appropriate auditory and visual alert systems. A comprehensive range of drugs is necessary to cover the spectrum of clinical presentations and scenarios encountered in the retrieval setting. These should be maintained in sealed drug kits, with attention paid to expiry dates and to temperature control where relevant. The retrievalist will also require access to antivenoms, thrombolytics, blood and blood products and other specialized agents at times – systems must be in place to ensure timely access to uncommonly used pharmacological agents.
Clinical principles in retrieval and pre-hospital medicine
Preparation for transport
In many cases, the referral of a patient for retrieval is an uncommon event that may occur at one site perhaps once or twice each month and which may involve individual staff members only once or twice per year. Therefore, clear understanding and communication of the needs of the critical-care patient for transfer must be in place. Common dilemmas are faced:
![]() Does the patient require intubation for transfer?
Does the patient require intubation for transfer?
![]() If so, should the patient be intubated now, later or wait for the retrieval team to arrive to intubate?
If so, should the patient be intubated now, later or wait for the retrieval team to arrive to intubate?
![]() What IV access does the patient require? CVC? Arterial line?
What IV access does the patient require? CVC? Arterial line?
![]() Drug and equipment compatibility – what will the retrieval team expect? What will they want to take with them?
Drug and equipment compatibility – what will the retrieval team expect? What will they want to take with them?
![]() What if the patient’s clinical status changes?
What if the patient’s clinical status changes?
Airway management is perhaps the greatest risk in the critical-care retrieval setting. The need for intubation for transfer should be discussed between the retrieval coordinator, referring staff and the retrieval team. In general terms, the patient should be intubated if needed for respiratory failure or, if significantly aggressive, agitated or obtunded, or if their clinical condition makes it likely that they will deteriorate en route, e.g. large intracranial haemorrhage, complete cervical cord injury, or if they have threatened airway obstruction, e.g. burns, epiglottitis which would present a high risk in-transit intubation.
The general principles that should be applied systematically in the preparation of patients for retrieval are given in Box 26.2.1.
Box 26.2.1
General principles to be applied in preparation of patients for retrieval
Airway
1. Assess airway stability for all patients, particularly those with compromise in conscious state or risk of deterioration
2. If an endotracheal tube is in place, record laryngoscopic grade during intubation, note any intubation difficulties and record ETT size and lip length
3. Secure endotracheal tube
4. Insert an orogastric tube unless there is a major contraindication
5. Perform a CXR to confirm position of endotracheal tube
Breathing
1. Observe respiratory rate and character
2. Measure SpO2 and ETCO2
3. Administer oxygen using the correct delivery device
4. Check ABGs if indicated/possible
5. Secure intercostal catheters if present
Circulation
1. Insert two peripheral IV lines
2. Secure all lines – ensure injection ports are accessible
3. Prepare drug infusions in 50 mL syringes (or other standard as used by the regional retrieval or ambulance service)
4. For advice on standard infusion concentrations discuss with the retrieval coordinator
5. Record all IV fluids and consider insertion of a urinary catheter (mandatory in intubated patients)
6. Transduce all arterial and central lines
Documentation
1. Complete standard referral forms if available
2. Provide copies of all patient charts
3. Investigation results – pathology & ECG
4. Imaging – films/scan/MRI
5. Advise any ‘limitation of treatment’ orders
6. Notify any infectious disease risk/contagious disease risk or exposure
Other priorities
1. Monitor and maintain body temperature
2. Empty drainage bags prior to transport
3. Administer antiemetic in conscious patients
4. Maintain spinal precautions if indicated
5. Splints and pressure care
6. Remove possible contaminants, such as glass, dirt, etc.
7. Notify significant deterioration in conscious state, blood pressure, heart rate, respiratory status, oxygenation; or any major clinical developments, such as significantly abnormal diagnostic tests, new clinical signs or the need for major interventions prior to the retrieval team arriving (e.g. intubation, surgery)
Monitoring
Monitoring equipment used in transport should be in accordance with recommended jurisdictional standards. Most patients require at least continuous ECG, pulse oximetry and blood pressure monitoring. In addition, capnography, invasive pressure monitoring, temperature, ventilation and other monitoring may be required. Equipment must be selected carefully and, where possible, be integrated. Sophisticated light, transport-specific, multimodal monitoring units are now available which include the above components plus defibrillation and external pacing capability. Display screens must be visible in daylight and battery life must be appropriate for duration of transport. Equipment alarms must be clearly visible as auditory alarms are difficult or impossible to hear in moving vehicles, especially aircraft. A major component of any monitoring system is the observer and, in the retrieval setting, the need for vigilance is paramount; at all times at least one of the retrieval crew members must be absolutely focused on the patient and monitors, continually scanning measured parameters and clinical status (including temperature, peripheral circulation, urine output, conscious state and respiratory oscillation).
Environmental impacts
Transport environments are usually confined and limited in space, which may present hazards for all staff, the patient and equipment. Care, deliberate planned actions and vigilance are important as is the need to ensure all equipment is secured (and equipment that is needed is accessible). Planned exercise, movement, nourishment, breaks and fatigue avoidance must be considered, depending on the mission characteristics. Aircraft retrieval presents particular challenges [8]. Altitude results in reduction in barometric pressure and associated reduction in partial pressure of oxygen and expansion of gas within enclosed spaces. Expansion of gas (such as in an undrained pneumothorax or in a distended bowel) may result in pain or significant worsening of underlying pathology. In a normal person with sea level SpO2 of 98% and without supplemental oxygen, SpO2 decreases to about 90% at 3000 m altitude (10 000 ft). Most passenger jet aircraft are routinely pressurized to around 8000 ft; however, some aeromedical platforms may be able to be pressurized to sea level, while some (including most helicopters) cannot be pressurized at all. In patients with respiratory and cardiac disease, impacts are felt at lower altitudes. During descent, trapped gas will occupy less space causing contraction of flexible tissues, such as membranes and mucosal surfaces – this may cause pain, for example when middle ear or sinus space pressures cannot be equalized with the rising external atmospheric pressure. Air transport of patients with decompression sickness requires particular planning and care, since the condition may be significantly worsened at altitude as gas solubility in blood decreases with altitude (due to reduced barometric pressure) and dissolved gas comes out of solution in the circulation, forming nitrogen bubbles with devastating consequences.
Other impacts of flight include those due to noise, vibration, humidity, gravity, acceleration and deceleration, third space effects (swelling) and fatigue.
Critical incidents
It is likely that the most complex patients receiving the highest levels of support are also most likely to be exposed to in-transit critical incidents or equipment failure. A component of clinical practice in this setting is therefore the anticipation of such events, vigilance to detect them and rehearsed and standardized problem-solving algorithms to rectify them (Fig. 26.2.3). Examples include ventilator failure, unexpected hypoxia, high airway pressures, cardiac arrest in flight, etc. Such approaches are routine in the aviation industry, from which retrieval and pre-hospital medicine draws much at a cultural level, and have been applied commonly in anaesthesia [9].
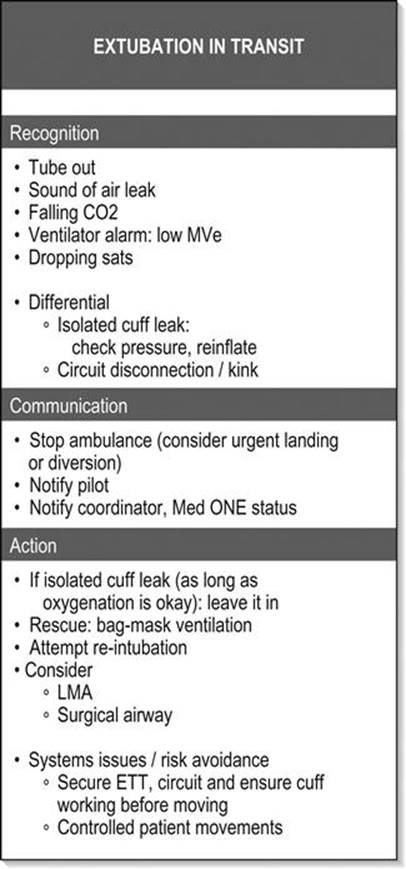
FIG. 26.2.3 Example of a critical incident algorithmic prompt card.
Respiratory support
Provision of appropriate oxygen therapy via correct delivery systems will be required for most retrieval patients. Oxygen supplies vary on different patient transport platforms and these must be checked prior to transport. Assisted ventilation is a frequent intervention in critical-care retrieval and must be approached with discipline. A reliable and capable transport ventilator will provide suitable ventilation mode options including intermittent positive pressure ventilation (IPPV), synchronized intermittent mandatory ventilation (SIMV) and pressure support. Non-invasive ventilation (NIV) methods are not commonly utilized in air transport; however, may be valuable in road transfer and in retrieval of patients in whom intubation and assisted ventilation may be undesirable or contraindicated or in patients for whom short-term assisted ventilation is indicated. Ventilators are almost universally power dependent so back-up ventilation systems (manual self-inflating bag/valve system) must be available at all times in the patient cabin to allow management of power, gas or mechanical failure.
Circulatory support and infusions
Intravenous infusions are best delivered using simple and compact syringe drivers. These are available in various sizes and configurations, including banks of multiple syringes. Each retrieval service and, preferably the jurisdiction in which it operates, should maintain standard infusion protocols for preparation, labelling and administration of therapeutic agents and, in particular, inotropes. Use of syringe systems that have error reducing software and programs integrated in them reduces risk of adverse events and patient harm. The retrieval environment is dynamic and attention must be paid to maintenance of infusion rates during transfer and power interruption. Critical patients are often highly dependent on inotropic support and brief periods of interruption of infusions may be associated with catastrophic circulatory collapse. Adequate fluid volumes and spare syringes which are pre-prepared for longer transfers must be planned for, as must the availability of blood and blood products which may need significant coordination.
Infectious risk
The proximity of the retrieval environment means that patients with infectious diseases may present hazards to medical crew, flight crew including pilots and other patients or passengers. Clearly, the application of universal precautions against infectious diseases is applicable as in all clinical settings; however, other measures may be important, such as use of ventilator expiratory filters, avoidance of use of nebulizers which may, for instance, aerosolize influenza, use of prophylactic medications, such as rifampicin, after prolonged exposure to meningococcal disease, barrier precautions in patients with vancomycin-resistant enterococci (VRE) and so on.
Highly-specialized retrieval
Neonatal, obstetric and paediatric specialized retrieval systems have been a part of many health systems for decades. While the clinical demands of these systems require particular sets of knowledge, the retrieval frameworks required are complementary and intersect with the larger and higher volume world of adult retrieval and pre-hospital care. Consequently, blending, collocating or integrating retrieval services is seen as a sustainable model and has become more common. Technical advances in critical care, such as increased use of extracorporeal membrane oxygenation (ECMO) support in severe respiratory failure for example in influenza, have promoted the development of specialized retrieval systems to manage these highly fragile patients [10]. Interestingly, in response to these needs, technology has evolved rapidly to offer lighter, smaller, less invasive and simpler ECMO systems.
Controversies/emerging issues
![]() Increased centralization is a consistent feature in Australian retrieval (and internationally). Where states and regions previously may have had multiple systems for retrieval, it is more common now to see single coordinated systems with improved governance. In addition, there is a nationally progressing movement for co-location of adult and paediatric services, integration of these services and for the increased formalization of the role of retrieval and pre-hospital medical services in disaster medicine.
Increased centralization is a consistent feature in Australian retrieval (and internationally). Where states and regions previously may have had multiple systems for retrieval, it is more common now to see single coordinated systems with improved governance. In addition, there is a nationally progressing movement for co-location of adult and paediatric services, integration of these services and for the increased formalization of the role of retrieval and pre-hospital medical services in disaster medicine.
![]() Building economy and efficiency from such commonality in systems is a driver for these developments; however, such benefits and advantages often require cultural and system readjustment and therefore may remain unrealized while change is managed.
Building economy and efficiency from such commonality in systems is a driver for these developments; however, such benefits and advantages often require cultural and system readjustment and therefore may remain unrealized while change is managed.
![]() Building on relevant interfaces which are a strong part of retrieval work is a common theme so that movement of retrieval services into management of critical and acute care bed flow and access management, outreach and support, telehealth and education is being seen.
Building on relevant interfaces which are a strong part of retrieval work is a common theme so that movement of retrieval services into management of critical and acute care bed flow and access management, outreach and support, telehealth and education is being seen.
![]() Retrieval and pre-hospital medicine in Australia is moving progressively to specialist status within academic colleges and has fully reached this point in some countries [11]. Formal training systems and qualifications are evolving in both the tertiary education sector and in specialist medical college settings.
Retrieval and pre-hospital medicine in Australia is moving progressively to specialist status within academic colleges and has fully reached this point in some countries [11]. Formal training systems and qualifications are evolving in both the tertiary education sector and in specialist medical college settings.
References
1. Hedges JR, Newgard CD, Mullins RJ. Emergency medical treatment and active labor act and trauma triage. Prehosp Emerg Care. 2006;10:332–339.
2. Australasian College for Emergency Medicine, Joint faculty of Intensive Care Medicine, Australian and New Zealand College of Anaesthetists. Minimum standards for transport of critically ill patients.<http://www.acem.org.au/media/policies_and_guidelines/min_standard_crit_ill.pdf>; 2003 [Accessed Nov. 2012].
3. Brown JB, Stassen NA, Bankey PE, et al. J Trauma Injury Infect Crit Care. 2011;70:310–314.
4. Brown JB, Stassen NA, Bankey PE, et al. Helicopters and the civilian trauma system: national utilization patterns demonstrate improved outcomes after traumatic injury. J Trauma Injury Infect Crit Care. 2010;69:1030–1036.
5. Carne B, Kennedy M, Gray T. Crisis resource management in emergency medicine. Emerg Med Australas. 2012;24:7–13.
6. Intensive Care Society UK. Guidelines for the transport of the critically ill adult, 3rd ed.<http://www.ics.ac.uk/professional/standards_and_guidelines/transport_of_the_critically_ill_adult>; 2011 [Accessed Nov. 2012].
7. Garner A. The role of physician staffing of helicopter emergency medical services in prehospital trauma response. Emerg Med Australas. 2004;16:318–323.
8. Martin T. Clinical considerations in transport of the sick and injured. Aeromedical transportation – a clinical guide 2nd edn. Aldershot: Ashgate; 2006.
9. Runciman W, Merry A. Crises in clinical care: an approach to management. Qual Saf Hlth Care. 2005;14:156–163.
10. Forrest P, Ratchford J, Burns B, et al. Retrieval of critically ill adults using ECMO: an Australian experience. Intens Care Med. 2011;37:824–830.
11. Intercollegiate Board for Training in Pre-hospital Emergency Medicine. Subspecialty training in prehospital and retrieval medicine – a guide for trainees, trainers, local education providers, employers and deaneries. London: College of Emergency Medicine; 2012.
Further reading
1. Ellis D, Hooper M. Cases in pre-hospital and retrieval medicine Sydney: Elsevier; 2010.
2. Martin T. Aeromedical transportation – a clinical guide 2nd edn. Aldershot: Ashgate; 2006.
26.3 Medical issues in disasters
Richard J Brennan, David A Bradt and Jonathan Abrahams
Essentials
1 The incidence of natural and technological disasters has increased exponentially from 1960 to the present.
2 Disaster deaths steadily declined over the last half of the 20th century, but numbers of disaster-affected populations continue to rise, encompassing 40% of the world’s population over the last decade.
3 Economic damage from natural disasters commonly surpasses $US100 b/yr.
4 Effective disaster planning requires knowledge of a community’s major hazards, vulnerabilities and capabilities, disaster history and disaster-associated patterns of morbidity and mortality. Disaster management is 80% generic for all hazards, 15% hazard-specific and 5% unique to the event.
5 Public health interventions are high priorities following disasters that disrupt environmental health infrastructure (e.g. water supply, sewerage), disasters that result in significant population displacement (e.g. conflict), disasters associated with epidemics and pandemics and disasters that involve the unintentional or deliberate release of chemical, biological or radiological agents.
6 Emergency physicians and other health professionals have a vital role in disaster management including prevention, mitigation, preparedness, response and recovery operations.
7 Continuing disaster losses have led to calls for community resilience as a cornerstone of national disaster management strategies.
8 The disasters most likely to confront emergency physicians are domestic transportation disasters associated with trauma-associated multiple casualties.
9 Effective management of mass casualty incidents requires knowledge of local and regional disaster response plans, scene assessment issues, site management, communications, casualty flow plans, field triage and the clinical management of hazard-specific conditions, such as crush injury and blast injury.
Introduction
Disaster management involves a complex, multidisciplinary process of which emergency medicine comprises one component. Domestically, fire fighters, law enforcement, ambulance services, civil defence, State Emergency Services, Red Cross national society, defence forces and other aid organizations commonly play major roles. Internationally, governmental and non-governmental organizations, International Federation of the Red Cross and Red Crescent Societies and United Nations agencies are frequently involved. The health and medical management of disasters can also cut across healthcare disciplines, requiring contributions from emergency medicine, public health, primary care, surgery, anaesthetics and intensive care.
From the health perspective, certain types of disasters are usually associated with well-described patterns of morbidity and mortality. The clinical and public health needs of an affected community therefore also vary according to the type and extent of disaster. Emergency physicians should understand the public health and medical consequences of the various types of disasters in order to determine their own roles in preparedness and response. In practice, emergency physicians are most actively involved in the response to an acute-onset disaster that involves multiple casualties, such as a transportation incident. Several other types of disasters, including floods and cyclones, are generally associated with few, if any, casualties. The health and medical needs in these settings usually involve augmenting public health and primary care services.
Emergency physicians should be familiar with disaster epidemiology and disaster management arrangements and understand the medical response to a disaster involving multiple casualties.
The differential effects of disasters on communities in all countries are associated with risk factors which make some communities and subpopulations more vulnerable and less capable of dealing with the risks than others. Apart from health and medical issues, the impact of disasters is often widespread and long term. Disasters can cause significant social, economic and environmental losses that may have devastating effects on the general well-being of the affected community. They may set back years of development progress in poorer countries, including disruption of health systems, such as the Pakistan floods of 2010. Their effects may be felt well beyond the borders of the first affected country. Epidemics, for example, may be prone to widespread international spread, with a broad range economic and sociopolitical consequences, for example, the H1N1 pandemic of 2009.
Definitions and classification
There is no internationally agreed definition of disaster or disaster classification. There are increasingly consistent uses of disaster terms among stakeholder organizations. Common to most definitions is the concept that, following a disaster, the capacity of the impacted community to respond is exceeded and there is, therefore, a need for external assistance.
The United Nations Office for Disaster Risk Reduction (UNISDR), defines a disaster as: ‘a serious disruption of the functioning of a community or a society causing widespread human, material, economic or environmental losses which exceed the ability of the affected community or society to cope using its own resources’ [1]. This definition is also one of several recognized by the World Health Organization (WHO).
The Australian Emergency Management Glossary defines disaster as: ‘a serious disruption to community life which threatens or causes death or injury in that community and/or damage to property which is beyond the day-to-day capacity of the prescribed statutory authorities and which requires special mobilization and organization of resources other than those normally available to those authorities’ [2].
The Center for Research on the Epidemiology of Disasters (CRED), which compiles the data behind the annual World Disasters Report of the International Federation of Red Cross and Red Crescent Societies, stipulates a quantitative surveillance definition involving one of the following: 10 or more people killed; 100 or more people affected; declaration of state of emergency; or an appeal for international assistance [3].
Disaster risk management is the range of activities designed to establish and maintain control over disaster and emergency situations and to provide a framework for helping at-risk populations avoid or recover from the impact of a disaster. It addresses a much broader array of issues than health alone, including a multisectoral approach to hazard identification, vulnerability analysis, risk assessment, risk evaluation and risk treatments [4].
Disaster medicine can be defined as the study and application of clinical care, public health, mental health and disaster management to the prevention, preparedness, response and recovery from the health problems arising from disasters [5]. This must be achieved in cooperation with other agencies and disciplines involved in comprehensive disaster management. In practice, emergency medicine and public health are the two specialties most intimately involved in disaster medicine.
A mass casualty incident is an event causing illness or injury among multiple patients simultaneously through a similar mechanism, such as a major vehicular crash, structural collapse, explosion or exposure to a hazardous material. A complex disaster is a disaster complicated by civil conflict, government instability, macroeconomic collapse, population migration and an elusive political solution.
Disasters are commonly classified as natural versus technological/human-generated (Box 26.3.1) [3]. Disasters may also be classified according to other characteristics, including sudden versus slow onset, short versus long duration, unifocal versus multifocal distribution and primary versus secondary. Classifications of disaster magnitude exist for selected natural hazards, such as earthquakes and hurricanes/cyclones; however, there is currently no standard classification of severity of disaster impact.
Box 26.3.1
Classification of disasters
|
Natural |
Technological/human-generated |
|
Hydrological |
Technological |
|
Floods (waves and surges) |
Industrial accidents: |
|
Wet mass movements |
Chemical spills |
|
Meteorological |
Building collapses |
|
Storms |
Explosions |
|
Climatological |
Fires |
|
Extreme temperatures |
Gas leaks |
|
Wildfires |
Poisoning |
|
Droughts |
Radiation |
|
Geophysical |
Transportation accidents: |
|
Earthquakes |
Air |
|
Tsunamis |
Rail |
|
Volcanic eruptions |
Road |
|
Dry mass movements |
Water |
|
Biological |
Miscellaneous accidents: |
|
Insect/pest infestations |
Domestic building collapses, fires and explosions |
|
Epidemics |
War/terrorism/complex emergencies |
Epidemiology
Globally, the types of disasters associated with the greatest numbers of deaths are complex emergencies (CEs). These are crises characterized by political instability, armed conflict, large population displacements, food shortages and collapse of public health infrastructure. Because of insecurity and poor access to the affected population, aggregate epidemiological data for CEs are somewhat limited. However, between 1998 and 2007 in the Democratic Republic of Congo, it is estimated that 5.4 million people lost their lives due to the consequences of the major humanitarian crisis afflicting that country [6]. This was four times the UNISDR estimate of deaths globally due to natural and technological disasters during the 20 years between 1992 and 2012.
According to information compiled by the International Federation of the Red Cross, there has been a significant increase in the total number of natural and technological disasters worldwide during the past 50 years. From 1960 to 2010, the annual number of disasters rose from 50 per year to approximately 700 per year peaking at 810 in 2005. While the total number of people killed by natural and technological disasters is currently approximately 150 000 per year, there is a wide annual range (17 660 in 2009 to 304 476 in 2010 due to the Haiti earthquake and the Russian heatwave). Moreover, the total number affected has almost quadrupled over the past three decades. It is estimated that approximately 200 million people are directly affected on an annual basis. Selected data are presented in Figures 26.3.1 and 26.3.2[3].

FIG. 26.3.1 Global disasters incidence by hazard 2001–2010 [3].

FIG. 26.3.2 Global disasters death by hazard 2001–2010 [3].
The commonest types of disasters across the globe are: transportation incidents, floods, windstorms, industrial incidents, building collapses, droughts, and earthquakes/tsunamis (see Fig. 26.3.1). Asia is the region of the world most prone to natural and technological disasters, recording 41% of such incidents between 2001 and 2010. It is followed by Africa (24%), the Americas (19%), Europe (14%) and Oceania (2%). Compared with other regions of the world, Australasia and Oceania have a relatively low incidence of disasters. Nonetheless, the World Risk Index (WRI) Report of 2012 included Vanuatu, Tonga and the Solomon Islands among the 10 countries most at risk to natural hazards [7].
Over the past 10 years, the commonest causes of disasters in Australia have been severe storms, including hail, transportation events and bushfires. Historically, the leading cause of death from natural disasters in Australia have been heatwaves (438 killed in 1939, 404 killed in 2009), followed by cyclone and bushfire. Human-generated disasters resulting in multiple casualties have occurred more frequently in Australia in recent years. The commonest causes of mass casualty incidents have been bus crashes, structural fires, mining incidents, aviation incidents and train crashes.
The impact of disasters has been less in New Zealand, where only 75 lives were lost among 307 000 persons affected over the period 2001–2010. However, 2011 brought the Christchurch earthquake with 185 deaths surpassing the death toll of the previous decade. The incidence of disasters also differs, with the commonest major events being transportation disasters, industrial disasters and earthquakes. Data reporting on the incidence of armed conflict is complicated by varying and changing definitions and political motivations of the reporting agencies. The Uppsala Conflict Database Program identified 37 on-going conflicts on five continents in 2011 [8].
The regions recording the highest number of terrorist attacks over the past decade have been Afghanistan and Iraq. Excluding those countries, the number of terrorist attacks worldwide resulting in the death of at least 10 persons, has ranged between 193 and 353 events per year [9]. Overall, this is just a very small fraction of the total number deaths attributed to natural and technological disasters and complex emergencies.
Disaster epidemiology globally, including the Australasian region, is being affected by climate change. Global warming has already been associated with an increase in the frequency, severity, and unpredictability of weather-related disasters, such as heatwaves, floods and droughts. Rising temperatures have been implicated in the spread of infectious disease, such as malaria and dengue, through increases in vector populations, such as mosquitoes. Other important diseases are also sensitive to changing temperatures and rainfall, including malnutrition and diarrhoea. The health-related and other impacts of climate change will not be evenly distributed. Disasters associated with global warming are particularly likely to threaten the lives and livelihoods of coastal communities, those living in low-lying islands (e.g. due to rising sea levels) and in arid and high mountain zones.
Socioeconomic impact
Disasters have the potential for major socioeconomic impact of direct damages plus economic losses, costing the host countries and international community billions of dollars annually. In developing countries, years of development work and investment can be devastated by a single disaster. During the decade 2000–2010, disasters caused a global average of approximately $US107 billion damage per year. Windstorms were the costliest disaster over the decade accounting for 49% of disaster-associated costs led by Hurricane Katrina with over $200 billion in damage. Terrorist attacks on major financial centres, such as the World Trade Center in New York, have demonstrated the potential for tens of billions of direct economic impact, enormous social consequences and political repercussions. These figures may be overshadowed by pandemic disease, such as from avian influenza, for which economic cost estimates range to upwards of $US1 trillion [10].
In Australia over the past 30 years, floods, storms, then cyclones have caused the greatest disaster-related economic losses with an average of approximately $AUS1 billion annually. The most economically costly disaster was the 2010–2011 Queensland floods exceeding $A7 billion in damages and losses.
Economic estimates, of course, are unable to reflect the true scale of human suffering associated with disasters. While we can often document the mortality, morbidity and financial losses associated with disasters, it is impossible to quantify the associated personal, psychological, social, cultural and political losses.
Disaster management/emergency management
As emergency physicians play a vital role in the medical aspects of disaster management, they should be familiar with the underlying concepts on which these arrangements are based [11].
Integrated approach
The basis for the Australian system for managing disasters is a partnership between the Commonwealth, State/Territory local governments, the private sector and the community. Under legislation, State and Territory governments have the primary responsibility for coordinating disaster-management activities and maintain government and statutory agencies that provide emergency services to the community. Local governments play an active role in risk assessments, land-use planning, public education and awareness, local emergency planning and providing local resources in emergency relief and recovery. The major roles of the Australian Federal Government are to support State and Territory governments in coordinating national strategic policy, to assist with disaster information and knowledge management (e.g. meteorological and geological data to support risk assessments and early warnings), to provide financial resources on a cost-sharing basis with States and Territories and to provide operational support in the event that a disaster exceeds the affected State or Territory’s response capability [12]. Federal assistance in the area of health would most likely be medical resources provided by the Australian Defence Force (ADF). The ADF also has special expertise in the management of incidents involving chemical and biological agents.
Comprehensive approach
The comprehensive approach to disaster management encompasses prevention, preparedness, response and recovery. The traditional view is that health and medical professionals contribute most significantly to disaster preparedness and response. A broader appreciation of the factors that enable communities to be more disaster resilient would further recognize the role of the health sector in prevention and mitigation – specifically, by improving overall health, immunization rates and nutritional status of individuals, as measures to reduce vulnerabilities and strengthen resilience. The disaster equivalent of primary prevention activities includes regulatory and physical measures that prevent or mitigate the effects of hazards and to reduce community exposure to these hazards. Preparedness involves arrangements to ensure that resources and services that may be needed can be rapidly mobilized and deployed. Response activities are those actions taken during and immediately after impact to ensure that the disaster’s effects are minimized. Recovery involves strategies and services that support affected communities in reconstructing their physical infrastructure and restoration of their social, economic, physical and emotional well-being.
All-hazards approach
Different types of disasters can cause similar problems. Therefore, disaster management plans are based on a core set of arrangements and measures that can be applied to all hazards. Many risks, however, including acts of terrorism, also require specific prevention, preparedness, response and recovery measures.
The prepared community
The prepared community is the foundation of Australia’s disaster management arrangements. Local governments, voluntary organizations and individuals all play a critical role in this area. Individuals can reduce their own risks by being aware of the local hazards and taking appropriate precautions. Experience has demonstrated that individual and community self-help can often provide the most immediate, decisive and effective relief following a disaster, as it cannot be assumed that assistance from external sources always arrives promptly, particularly in remote area communities.
Risk management
From 1996, following the endorsement of the National Emergency Management Committee, the principles and processes of the joint Australian and New Zealand Standard for Risk Management have been adopted by the Australian emergency management community. The risk management methodology embraces the key approaches identified above and ensures a greater focus on reducing vulnerability of communities, as well as hazard prevention, emergency response and recovery measures [13].
Disaster resilience
Against the background of disasters, climate change and a myriad of social, economic and environmental factors, the Council of Australian Governments adopted the National Strategy for Disaster Resilience in 2011. The Strategy emphasizes the shared responsibility of individuals, households, community organizations, businesses and governments to enhance Australia’s capacity to prepare for, withstand and recover from disasters. According to the Strategy, a disaster-resilient community has the characteristics of: functioning well while under stress, successful adaptation, self-reliance and social capacity. The Strategy provides high-level direction and guidance on how to achieve disaster-resilient communities through a long-term commitment to a broad range of measures including understanding risks, communicating and educating about risks, reducing risks and supporting capacities for resilience [14].
Disaster response planning
Disaster response planning is the process by which a community develops a comprehensive strategy effectively to manage and respond to disasters. It is a collaborative effort that requires cooperation among government agencies, community services and private organizations. The objectives of the planning process include identification of the main hazards facing the community; clarification of the capabilities, roles and responsibilities of responding agencies; and the strengthening of emergency networks. Other operational issues, such as emergency communications and public warning systems, should also be addressed.
All-hazards planning for response and recovery remains fundamental to disaster preparedness. To that end, disaster experience to date reveals a generic set of issues that disaster planners must address in the management of any hazard. These include risk assessment, incident management, on-scene and overall disaster command, control and coordination, relief operations, risk communication and media management, reconstruction, and community recovery. By contrast, the nature of the hazard imposes specific implications for epidemiology, search and rescue, medical care and consequences of contamination and communicable diseases. To this end, governments have elaborated all hazards disaster response planning including hazard-specific disaster subplans (e.g. mass casualty management for burns).
Finally, the circumstances of time, place, climate, geography, politics and security are unique for each disaster and challenge disaster planners to anticipate the issues arising from those specific circumstances.
Several high-profile terrorist events (e.g. World Trade Center attack in New York City) and important gatherings (e.g. London Olympic Games) have highlighted the need for specific planning for terrorist events. Such planning frequently involves collaboration with relevant military, security and intelligence agencies and a consideration of the tactics used by terrorists. The majority of terrorist attacks have employed conventional weapons, including explosives and small arms. Other terrorist tactics include assassinations, hijacking and kidnapping. Unconventional attacks, including those using jet airliners as weapons of mass destruction, or chemical, biological and radiological weapons have constituted only a tiny fraction of international terrorist attacks.
Disaster exercises must be conducted regularly to test the response and recovery aspects of the plan. Exercises range from desktop simulations to realistic scenarios with moulaged patients in the field. If conducted appropriately, they demonstrate strengths and weaknesses of the plan and highlight any need for an updating of response procedures. They are also considered to provide the most practice-based form of disaster response training. Disaster planning is a continuous process and plans need to be regularly reviewed and updated.
Planning and responding for international disasters has become more relevant for Australasian health professionals in light of the terrorist attacks in Bali (2002 and 2005), the Indian Ocean tsunami (2004), the earthquake in Pakistan and India (2005) and the Pakistan floods (2010), including through the deployment of Australian medical response teams (AusMATs) [15]. Such planning and response can be advised by the internationally-recognized Sphere Minimum Standards in Disaster Response [16] and in collaboration with important international agencies, such as the United Nation’s Office for Coordination of Humanitarian Affairs. Sphere specifies standards in six sectors of disaster response: water and sanitation, food security, food aid, nutrition, shelter and health services. These standards are relevant for all disasters and represent an extremely useful reference to guide planning and response for domestic incidents as well.
A major reform of the international humanitarian system was initiated at the end of 2011 under the leadership of the UN’s Office for Coordination of Humanitarian Assistance (OCHA) and involving all major relief agencies through the UN’s Inter-agency Standing Committee (IASC). This reform process, known as the IASC Transformative Agenda, includes a broad range of policy and procedural measures to improve the leadership, coordination, predictability and effectiveness of international disaster response. It also aims to increase the accountability of responding agencies, especially to the affected populations.
Domestic disaster response activities
Disaster management is increasingly seen as a cardinal sign of good governance in civil society. Healthcare systems have become mandated to undertake a range of health emergency and disaster risk management actions, with a focus on disaster preparedness, including disaster planning, training and exercises and response. Specific to emergency medicine, mass casualty management is the subject of well-developed training packages, such as Emergotrain, Major Incident Medical Management and Support (MIMMS), Basic Disaster Life Support (BDLS) and Advanced Disaster Life Support (ADLS).
Incident management
Scene assessment and stabilization
The initial scene assessment is conducted by first responders, such as police, fire or ambulance personnel. It is important for the first medical responder, generally an ambulance officer, rapidly to report findings to the Ambulance Communications Centre. An accurate, timely assessment is critical to initiating an appropriate and effective response. Key information that should be relayed from the scene includes the nature and magnitude of the disaster, the presence of ongoing hazards, the estimated number of deaths and injuries, the need for further assistance and the most appropriate routes of access to the scene. In large-scale disasters that affect entire populations, such as cyclone or earthquake, a rapid multisectoral assessment followed by broader epidemiological assessments is required, including an evaluation of the impact on the health infrastructure, health services, public utilities and shelter.
Site security and safety procedures must be observed to ensure that rescuers and bystanders do not become victims. This is particularly relevant in chemical and radiological incidents or when a terrorist incident is suspected, because of the threats posed by a secondary attack on responders or the potential use of weapons of mass destruction. The police should establish a perimeter around the scene of a multiple casualty incident and allow access only to authorized personnel. If a hazardous material is involved, rescuers may be required to wear specialized personal protective equipment (PPE) to protect their airways, eyes and skin. Electrical hazards, fires, explosions, leaking gases and unstable structures may all pose significant threats to rescue personnel. These hazards must be eliminated or controlled prior to initiating rescue operations.
Hazard-specific issues
While the all-hazards approach remains fundamental to disaster management, a unifying approach for undifferentiated hazards has been developed for the management of incidents involving chemical, biological or radiological agents. Basic principles of awareness include: recognition of potential terrorist events; avoidance of the affected area; isolation of the affected area; and notification of proper authorities. Basic principles for first responders include the four don’ts: don’t become a victim, don’t rush in, don’t TEST (taste, eat, smell, touch) anything, and don’t assume anything. Only properly trained and equipped hazardous material personnel should be in contaminated areas.
Site arrangements
Regardless of the nature of the incident, a Forward Command Post should be set up at or near the disaster site at the beginning of the emergency operation. The Command Post has representatives from the major responding services and reports back to the regional or State Emergency Operations Centre. The function of the Command Post is to coordinate the activities of the various services during the rescue operations. It also provides a central point for the submission of requests for assistance by each of the responding services. Medical and ambulance commanders are located at the Command Post to direct and coordinate medical care to victims at the scene, patient transportation, hospital communications, provision of medical supplies and medical air operations.
Communications
Good communications are vital to ensure appropriate command, control and coordination during a disaster. Communication problems are often cited as a major cause of suboptimal disaster response. There are many factors that may contribute to poor communications at the scene. Damaged equipment and overloaded telephone systems indicate the need for back-up systems, including reserved cellular phone lines. The use of different radio frequencies by different agencies may lead to poor coordination and an inability to communicate vital information. Compatible frequencies need to be identified and utilized. Megaphones may be required to overcome noise at the scene due to heavy extrication equipment, helicopters and general rescue activities. Information overload may also hamper the rescue effort. Radio and telephone reports should be kept brief, relevant and succinct. Professional jargon is frequently misunderstood or misinterpreted by other agencies and is best avoided.
Hospitals must also have reliable communications systems. Designated phone lines, cellular phones and back-up radio networks may augment the existing system during a disaster. It is essential for hospitals to remain in regular contact with the incident medical director, to provide information regarding medical capabilities, bed capacity and bed availability.
Medical management
Personnel
Provider roles in disasters continue to evolve. Dedicated disaster medical response teams have been extensively studied [17]. These teams form an integral part of national response plans in many developed countries notwithstanding lack of data attesting to any reduction in disaster-associated mortality associated with their deployments [18]. At international level, standards and procedures for foreign medical teams are currently being developed, after the poor experiences with many clinical teams following the Haiti earthquake in 2010.
Emergency responders generally respond best when their disaster roles are similar to their daily professional practice. Medical and nursing personnel are best suited to staffing emergency rooms and hospitals, where they have the advantage of working in a familiar, more stable environment. Ambulance personnel have more experience in pre-hospital settings and are usually responsible for conducting the initial on-site medical assessment and triage. In situations where there are multiple casualties, it may be appropriate to send a hospital team to the scene of a disaster, where their main functions are to perform primary and secondary triage and to provide medical care at the Patient Treatment Post. The science and practice of disaster medicine has progressed substantially. Therefore, only doctors and nurses specifically trained to work in the field environment and familiar with the relevant best practices and standards should be deployed to the disaster scene, as inexperienced personnel may well hinder the medical response.
Pre-hospital mass casualty management
Disaster epidemiology has refined the expectations of casualty flow plans. Current epidemiological evidence indicates that 50–80% of people acutely injured in a mass casualty disaster arrive at the closest medical facilities generally within 90 minutes after the event [19]. Moreover, the vast majority of disaster- affected patients self-evacuate without benefit of pre-hospital triage, transport or decontamination. A casualty-flow plan remains crucial to optimize patient care and transportation of those remaining at the scene.
A Casualty Collection Area should be established at a site that is close enough to the disaster scene to allow easy access, but far enough away to ensure protection from potential hazards. Patients are assembled and triaged here prior to transfer to a nearby Patient Treatment Post, where they are once again triaged and basic medical care provided. An Ambulance Loading Point and Ambulance Holding Point also need to be clearly marked so that patient transportation is conducted efficiently and to ensure that scene convergence and congestion is minimized. Landing zones for helicopters are established away from the incident site for safety reasons, to limit noise and to reduce down-wash from rotor blades. A temporary morgue may need to be established in a nearby area when many fatalities have occurred.
Triage
The aim of triage is to allocate medical resources, including personnel, supplies and facilities, in a manner that provides the greatest good to the greatest number of patients. The emphasis is not on providing optimal care to each individual patient, but rather on directing limited medical resources to those who are most likely to benefit. Triage is the single most important medical activity at the disaster site. It is a dynamic, ongoing process that occurs at every stage of patient management, from the disaster site, to the Casualty Collection Area, Patient Treatment Post and again at the hospital. Patients are rapidly assessed and categorized according to priority of treatment and transport. The condition of patients frequently changes and repeated examinations are required so that patients may be moved up or down in the order of priority. Triage is a learned skill and should be conducted by the most experienced medical or ambulance officer at the scene.
Different triage systems have emerged in different parts of the world. In British and Australasian health systems, ‘sieve and sort’ triage processes have become the preferred approach through MIMMS training courses [20]. In North America, ‘start and save’ triage processes have become incorporated into the National Disaster Medical System [21]. More recently, a National Disaster Life Support Consortium in the USA has promulgated a triage approach based on ‘move, assess, sort and send’ [22]. These different systems rely on different assessment approaches with different vital sign thresholds to assign triage priority.
In general, most systems recognize that there are categories of patients who require immediate care, delayed care, minimal care and those that are expectant or unsalvageable. Patients requiring immediate care are individuals in critical condition, but to whom simple life-saving procedures may be successfully applied, such as the manual clearing of the airway. Patients classified as requiring delayed care may have significant injuries, such as major fractures, but are likely to survive if treatment is postponed for several hours. Minimal care patients are generally ambulatory and their treatment may be delayed until other patients have been appropriately treated. Expectant or unsalvageable patients are those that have acutely life-threatening injuries requiring advanced resuscitation, or those that have non-survivable injuries, such as massive head trauma. Advanced life support measures, such as cardiopulmonary resuscitation, are rarely indicated at a scene with multiple casualties. Instead, these patients generally receive palliative care, but only after patients in the immediate category have received appropriate treatment.
Stabilization
Following triage of the affected patients, rapid stabilization of airway, breathing and circulation is provided to those with the greatest potential for survival. Definitive care is not generally provided at the scene. On-scene medical care concentrates on securing the airway, administration of oxygen, external pressure to control haemorrhage and insertion of intravenous catheters for volume expansion prior to hospital transportation. Medical care should generally be provided at the Patient Treatment Post but, during prolonged rescues, resuscitative procedures may be required prior to extrication. Appropriate use of analgesia, including parenteral narcotics and regional nerve blocks, may assist with the extrication of trapped individuals. Special on-scene procedures are sometimes required for those with crush injury, blast injury, burns or hypothermia. Amputation of a mangled limb, although rarely indicated, may be a life-saving procedure for an entrapped patient.
Decontamination
Chemical, biological, radiological and nuclear (CBRN) agents have the potential to contaminate individuals, property and the general environment. In practice, industrial accidents represent by far the most common cause of exposure to hazardous materials that may require decontamination. A small number of high-profile chemical–biological terrorist incidents over the past 20 years have also prompted medical as well as lay attention to this potential threat. Regardless of the cause, the principles guiding the process of decontamination remain consistent.
Decontamination is the process of removing or neutralizing a hazard from the victim or environment. Detailed management protocols exist for these hazards [23–25]. Fundamental principles involve:
![]() staff and site preparation with establishment of hot/warm/cold zones
staff and site preparation with establishment of hot/warm/cold zones
![]() casualty, staff and crowd protection
casualty, staff and crowd protection
![]() decontamination procedures
decontamination procedures
![]() clinical treatment of contaminated patients and transport to definitive care
clinical treatment of contaminated patients and transport to definitive care
![]() recovery of environment.
recovery of environment.
Removal of contaminated clothes should be conducted as a matter of urgency. Rapid decontamination of the skin is especially necessary following exposure to the liquid or aerosolized form of an agent. It is most useful when conducted within 1 minute of exposure but, in practice, this is rarely possible. When indicated, decontamination should be conducted close to the scene (i.e. in the ‘warm zone’) and, ideally, prior to transportation. Commonly used agents for decontamination include soap and water and hypochlorite (household bleach) in concentrations of 0.5–2.0%. Steps must be taken to ensure that emergency responders, health personnel and other patients are not at risk of secondary exposure to the chemical agent. Decontamination after exposure to a biological agent is less important, as most biological agents are not dermally active. But decontamination may be an effective way to limit the spread of the agent from potential secondary aerosolization.
Transportation
Efficient and rational transportation of patients to appropriate health facilities is dependent on good communications between hospitals and the incident Transport Officer. Capabilities of the affected community’s hospitals should be identified and documented in the regional disaster plan. Hospitals are required regularly to update the Incident Commander and Transport Officer of their bed availability status. The closest hospitals may be flooded by ‘walking wounded’ who have made their own way from the scene and by victims transported by well-meaning civilians. This has the potential of overwhelming local emergency departments and the Transport Officer must take this into consideration when determining the appropriate distribution of patients. It is essential that the disaster scene not be relocated to the nearest hospitals.
A number of factors need to be considered when determining the most appropriate hospital for a particular patient, including the patient’s triage category, the hospital’s capabilities (e.g. trauma, burns), transportation times, distance from the scene and the available transportation modalities. Medical helicopters may be able to transport patients to more distant hospitals, to relieve pressure on nearby facilities.
Health facility management
Guidance on hospital planning for disaster management has become widely available from the World Health Organization [26] as well as domestic stakeholders [27]. Emergency physicians are expected to be familiar with their own hospital disaster plan and have contributed significantly to its development. The plan should address both internal and external disasters. Surge strategies for hospitals and emergency departments have become well elaborated [28].
The emergency department needs to be cleared of non-critical patients and steps taken to expedite appropriate discharge of stable ward patients, so that bed capacity may be optimized. The emergency department should be well stocked with supplies and have arrangements with suppliers for rapid replenishment. A recall system for additional medical and nursing staff mobilized in a disaster needs to be incorporated into the plan. Extra security staff should be on standby to assist with the management of patients, families, friends, onlookers and the media.
Patients require re-triage by a senior medical officer as they arrive at the emergency department. Those with acutely life-threatening injuries are immediately resuscitated. Less severely injured patients need to be regularly reviewed while awaiting definitive care, to monitor for a potential deterioration in their condition. Expectant, unsalvageable patients are provided appropriate palliative care and their condition clearly explained to their relatives. Documentation is kept succinct and should generally be limited to the essential points about each patient’s condition and treatment. Any forensic investigations are likely to require the cooperation of emergency physicians and other health personnel. Cultural and religious needs associated with the management of dead bodies and in communication with relatives should be respected at all times.
Urban search and rescue
Urban search and rescue (USAR) is the science of locating, reaching, treating and safely extricating survivors who remain trapped following a structural collapse. Search and rescue response capabilities have increased significantly, due to advances in rescue technology and in emergency services.
In the period immediately following a structural collapse, many survivors are rescued by uninjured bystanders. Those who remain trapped generally require the assistance of specially trained and equipped units from fire, ambulance or police services in order to be safely extricated. Medical members of search and rescue teams are tasked to provide medical care to the victims and medical support to the rescuers. They are not usually involved in the actual extrication process. Potential hazards to victims and rescuers are numerous and scene safety is of critical importance. The identification and extrication of victims following a major structural collapse is one of the most physically and emotionally challenging tasks of any rescue operation. The shock of dealing with scenes of carnage and mutilation may render some rescue personnel ineffective. These teams must therefore be trained and prepared to deal with the emotional strains of working in such a demanding environment.
Mental health
It is easy to overlook the mental health needs of affected individuals during the emergency response, when rescue and life-saving interventions receive top priority. Emergency physicians should be aware of the significant psychological impact of disasters on victims, families and rescue personnel. Psychological support is recommended as first-level assistance to disaster-affected communities and personnel [29]. Mental health consequences, such as depression, anxiety states and post-traumatic stress syndrome, are well described following disasters and need to be considered when developing the disaster plan. Crisis counselling may play an important role in the overall medical care provided to patients following a disaster. In addition, rescue personnel may well suffer psychological consequences from their own involvement in the disaster response and should therefore be provided with access to appropriate support and services.
Mass gatherings
Social and cultural events can result in the gathering of many people in one place at a particular time, sometimes over several days. Common examples include religious events, music festivals, sporting events, fairs and parades. The organization of medical services for mass gatherings is generally designed to address minor medical needs, but must also take into consideration medical emergencies, such as cardiac arrests, and disaster planning, for incidents such as extreme weather, fire, structural collapse or terrorism. Medical services developed for the mass gathering must be linked to local emergency medical systems. Public health and occupational health regulations, including food safety and environmental health measures, must be observed.
Public health issues in disasters
Public health professionals are involved in all phases of disaster risk management and it is important for emergency physicians to understand the role of public health in disaster medicine and disaster risk management. Epidemiological studies that have identified risk factors for illness and injury following disasters have contributed greatly to disaster risk assessments, prevention, mitigation, preparedness (including planning), response and recovery. These investigations have been central to the development of the science of disaster medicine. They have led to key strategies that have been effective in reducing disaster-related morbidity and mortality.
Public health interventions become high priorities following disasters that disrupt the social infrastructure (for instance, cyclone, flooding, earthquake) and disasters that result in significant population displacement (such as complex emergencies). Priorities for the affected population include the provision of adequate water quantity and quality, sanitation, food, shelter, infectious disease control and disease surveillance. The role of public health following a mass casualty incident includes injury control, occupational health and safety measures for responders and injury surveillance.
The interface between emergency medicine and public health becomes increasingly important following technological disasters or terrorist events involving biological, chemical or nuclear agents. The terrorist attacks with anthrax in the USA during 2001 and their aftermath demonstrated the vital importance of key public health tools, such as disease surveillance and outbreak investigation and control. Following incidents with chemical or radiological agents, public health officials may be required to provide guidance on issues, such as evacuation of the public, mass decontamination and the mass distribution of iodine. Emergency physicians should become more familiar with the skills, roles and responsibilities of their public health colleagues, especially as they relate to disaster management and infectious disease control.
Conclusion
State-of-the-art in contemporary disaster management emerges from interdisciplinary, interagency and international best practices. Curative medical skills and public health skills are both fundamental to the comprehensive management of a community affected by a disaster. Emergency physicians contribute most significantly to the preparedness and response aspects of disaster management. Emergency physicians should plan and build capacities for disasters based on an assessment of the major risks that their communities face and those which are most likely to result in multiple casualties. These include the risks associated with natural, technological, biological and societal hazards. The increased risks posed by climate change and terrorists require the continuing review and revision of disaster risk-assessment processes and disaster planning. Disasters associated with multiple casualties provide unique challenges to the health and medical communities. Short courses in disaster management are widely available and should be part of every emergency physician’s training.
Likely developments
![]() Increasing frequency, severity and unpredictability of natural disasters.
Increasing frequency, severity and unpredictability of natural disasters.
![]() Increasing standardization in international response mechanisms, including foreign medical teams.
Increasing standardization in international response mechanisms, including foreign medical teams.
![]() Increasing accountability of health factors for disaster clinical interventions and their outcomes.
Increasing accountability of health factors for disaster clinical interventions and their outcomes.
![]() Strengthened mechanisms for the leadership, coordination and effectiveness of international disaster response, in line with recent reform measures.
Strengthened mechanisms for the leadership, coordination and effectiveness of international disaster response, in line with recent reform measures.
Controversies and future directions
![]() The fields of disaster management and disaster medicine continue to professionalize. There are updated standards, best practices and trainings for most aspects of disaster response. There has also been significant progress in managing the risks posed by various hazards prior to disasters striking. Emergency physicians should familiarize themselves with these developments so that they are better able to respond to both small- and large-scale disasters.
The fields of disaster management and disaster medicine continue to professionalize. There are updated standards, best practices and trainings for most aspects of disaster response. There has also been significant progress in managing the risks posed by various hazards prior to disasters striking. Emergency physicians should familiarize themselves with these developments so that they are better able to respond to both small- and large-scale disasters.
![]() Disaster planning and preparedness must address the most common hazards and vulnerabilities within a community, while still including a prudent approach to high profile events that have low probability and high consequences, such as terrorist attacks with CBRN agents. The all-hazards approach provides appropriate guiding principles for such planning.
Disaster planning and preparedness must address the most common hazards and vulnerabilities within a community, while still including a prudent approach to high profile events that have low probability and high consequences, such as terrorist attacks with CBRN agents. The all-hazards approach provides appropriate guiding principles for such planning.
![]() The threat of pandemic influenza and other potential epidemics must also be considered in disaster planning and preparedness. Emergency physicians should increase their familiarity with important concepts, such as infectious disease surveillance, case detection and outbreak investigation and response. They should also become more familiar with the skills, roles and responsibilities of their public health colleagues, especially as they relate to disaster management and infectious disease control.
The threat of pandemic influenza and other potential epidemics must also be considered in disaster planning and preparedness. Emergency physicians should increase their familiarity with important concepts, such as infectious disease surveillance, case detection and outbreak investigation and response. They should also become more familiar with the skills, roles and responsibilities of their public health colleagues, especially as they relate to disaster management and infectious disease control.
![]() The recently developed Australian medical response teams (AusMATs) and the Australian Civilian Corps provide opportunities for civilian specialists, including emergency physicians, to be deployed to countries experiencing or emerging from natural disaster or conflict. Opportunities also exist with a range of non-governmental organizations and UN agencies. Emergency physicians wishing to take advantage of these opportunities need to be familiar with specific clinical and public health issues, security considerations and international disaster response architecture and procedures.
The recently developed Australian medical response teams (AusMATs) and the Australian Civilian Corps provide opportunities for civilian specialists, including emergency physicians, to be deployed to countries experiencing or emerging from natural disaster or conflict. Opportunities also exist with a range of non-governmental organizations and UN agencies. Emergency physicians wishing to take advantage of these opportunities need to be familiar with specific clinical and public health issues, security considerations and international disaster response architecture and procedures.
References
1. International Strategy for Disaster Reduction. UNISDR terminology on disaster risk reduction Geneva: UNISDR; 2009.
2. Australian Government Attorney-General’s Department. Australian emergency management handbook series. Disaster health handbook. vol. 1 Barton, ACT: Australian Emergency Management Institute; 2011.
3. International Federation of Red Cross and Red Crescent Societies. World disasters report Geneva: International Federation of Red Cross and Red Crescent Societies; 2011; p. 203.
4. Keim MJ, Abrahams J. Health and disaster. In: Wisner B, Gaillard JC, Kelman I, eds. The Routledge handbook of hazards and disaster risk reduction. Oxford/New York: Routledge; 2012.
5. Murray V, Clifford J, Seynaeve G, Fisher J. Disaster health education and training: a pilot questionnaire to understand current status. Prehosp Disast Med. 2006;21:156–167.
6. International Rescue Committee. Mortality in the democratic republic of Congo: an ongoing crisis New York: International Rescue Committee; 2007.
7. Alliance Development Works, United Nations University Institute for Environment and Human Security (UNU-EHS), The Nature Conservancy Trust. World Risk Report 2012. Berlin: Bündnis Entwicklung Hilft (Alliance Development Works); 2012.
8. Uppsala Conflict Data Program. Uppsala Conflict Data Program.<http://www.pcr.uu.se/research/ucdp/>[Accessed Dec. 2012].
9. US Department of State, National Counterterrorism Center: Annex of Statistical Information. Country reports on terrorism 2011.<http://www.state.gov/j/ct/rls/crt/2011/195555.htm>[Accessed Nov. 2012].
10. Brahmbhatt M. Avian influenza: economic and social impacts.<http://web.worldbank.org/WBSITE/EXTERNAL/NEWS/0,contentMDK:20663668~pagePK:34370~piPK:42770~theSitePK:4607,00.html>[Accessed Jan. 2012].
11. Australian Government Australian Emergency Manuals. Principles and reference series. Emergency management concepts and principles Canberra: Emergency Management Australia; 2004.
12. Australian Government Attorney General’s Department. Australian emergency management arrangements Canberra: Australian Attorney-General’s Department; 2009.
13. Australian Government Australian Emergency Manuals. Principles and reference series. Emergency risk management applications guide 2nd edn. Canberra: Emergency Management Australia; 2004.
14. Council of Australian Governments. National strategy for disaster resilience: building the resilience of our nation to disasters Canberra: Commonwealth of Australia; 2011.
15. National Critical Care and Trauma Response Centre.<http://www.nationaltraumacentre.nt.gov.au/disaster>[Accessed Feb. 2013].
16. Sphere Project. Humanitarian charter and minimum standards in humanitarian response Rugby, United Kingdom: Practical Action Publishing; 2011.
17. Anton Breil Centre for Public Health and Tropical Medicine, James Cook University. Disaster Medical Assistance Teams: a literature review; 2006. Available from the Health Protection Group, Department of Health, Western Australia, Australia.
18. Bradt DA. Site management of health issues in the 2001 World Trade Center disaster. Acad Emerg Med. 2003;10:650–660.
19. US Centers for Disease Control and Prevention. Mass trauma casualty predictor.<http://www.bt.cdc.gov/masscasualties/predictor.asp>[Accessed Feb. 2013].
20. Advanced Life Support Group. Major incident medical management and support – the practical approach 3rd edn. UK: John Wiley & Sons; 2012.
21. Benson M, Koenig KL, Schultz CH. Disaster triage: START, then SAVE – a new method of dynamic triage for victims of a catastrophic earthquake. Prehosp Disaster Med. 1996;11:117–124.
22. American Medical Association. Basic disaster life support provider manual (Ver 2.6) American Medical Association 2007.
23. US Department of Health and Human Services Public Health Service Agency for Toxic Substances and Disease Registry Hospital Emergency Departments: a planning guide for the management of contaminated patients (Volume 2). December 2012. CreateSpace Independent Publishing Platform.<http://www.atsdr.cdc.gov>.
24. US Army Medical Research Institute of Infectious Diseases. Medical management of biological casualties handbook, 7th edn. September 2011.<http://www.usamriid.army.mil/education/bluebookpdf/USAMRIID%20BlueBook%207th%20Edition%20-%20Sep%202011.pdf>[Accessed Feb. 2013].
25. US Army Medical Research Institute of Chemical Defense. Medical management of chemical casualties handbook, 4th edn. February 2007.<http://www.globalsecurity.org/wmd/library/policy/army/other/mmcc-hbk_4th-ed.pdf>[Accessed Feb. 2013].
26. World Health Organization Western Pacific Region. Field manual for capacity assessment of health facilities in responding to emergencies, 2006. Available from the WHO Western Pacific Regional Publications Office, WHO Regional Office for the Western Pacific.
27. Qureshi K, Gebbie KM, Gebbie EN. Public Health Incident Command System: a guide for the management of emergencies or other unusual incidents within public health agencies, Volumes 1 & 2. August 2006.<http://www.ualbanycphp.org/pinata/phics/default.cfm>.
28. Bradt DA, Aitken P, Fitzgerald G. Augmentation of hospital emergency department surge capacity: recommendations of the Australasian Surge Strategy Working Group. Acad Emerg Med. 2009;16:1350–1358.
29. Interagency Standing Committee. IASC guidelines on mental health and psychosocial support in emergency settings Geneva: IASC; 2007.
26.4 Triage
Drew Richardson
Essentials
1 Triage is the ongoing process of sorting patients on the basis of the urgency of their need for medical care.
2 Urgency is distinct from both severity and complexity.
3 Triage categorization has been found to relate strongly to both resource use and patient outcome in the near term.
4 The 5-level Australasian Triage Scale (ATS) forms the basis of emergency department triage in Australasia.
5 The ATS is also used in case mix funding models and important performance measures.
6 The ‘treatment strategy’ by which the next patient to be seen is chosen from the various treatment queues continues to evolve in the face of increasing demand and ‘streaming’ according to likely therapeutic need.
7 Similar triage scales have been developed and adopted in other jurisdictions.
Introduction
Provision of high-availability quality medical care is expensive and has been traditionally limited to the very wealthy or to situations of great demand, such as the military in battle. Even today, well-organized emergency medical systems are concentrated in societies sufficiently affluent to spend 5% or more of GDP on health. Some form of rationing is required whenever an expensive resource is coupled with fluctuating demand. Price, queuing and denial are all used in different areas of medicine. Simple application of any of these methods in emergency medicine would not be efficient nor equitable, so the majority of emergency medical systems use a triage process to sort patients into a number of queues.
Triage, the sorting of patients on the basis of urgency, is an ongoing process that nevertheless requires formal structures at different points within the continuum of care. In the emergency department (ED) setting there is considerable evidence that urgency can be assigned reliably and distinctly on a five level scale and that this categorization is applicable and useful beyond the concept of ‘urgency’ into other aspects of hospital care.
Origins of triage
The word ‘triage’, arising from the French ‘trier’ meaning ‘to sort’ has its origins in Latin. It has entered English at least three times: from the 18th century wood industry, the 19th century coffee industry and from 20th century emergency medicine. The process understood today as triage was first described by Baron Dominique Jean-Larrey (1766–1842) [1], the surgeon to Napoleon, who also developed the ambulance volante, the first field ambulance. This delivered large numbers of injured but salvageable cases to medical units, mandating a more efficient system than treatment in order of military rank. Jean-Larrey’s ‘order of dressing and arrangement’ by urgency was also in keeping with the egalitarian spirit of the French revolution, although there is no evidence that he actually used the word triage. His concept was embraced and refined by military surgeons over the next 150 years, usually with the primary intent of returning soldiers to battle in the most efficient manner.
Civilian triage developments
There was certainly some sorting of patients from the moment ‘casual wards’ opened in 19th century hospitals, but the first systematic description in civilian medicine was by E. Richard Weinerman in Baltimore in 1966 [2]. Since that time, there has been a huge growth in emergency medicine as a specialty and a number of workers have undertaken formal investigation of triage, particularly in Australasia. The Australasian experience formed the basis of ED triage development in Canada and the UK, while some other jurisdictions have developed systems independently.
Process of triage
The underlying principles of triage are those of equity (or justice) and efficiency. EDs experience potentially overwhelming demand from patients with an enormous range of conditions. Equity demands that the distribution of resources for treatment is fair in the broadest sense. The concept of urgency is well understood by the population who generally accept that it is fair to treat those in the greatest need ahead of those who arrived before them. Efficiency demands that best use is made of available resources. In the setting of ED, cost and resource pressures prevent all demand being satisfied simultaneously. The overall philosophy of ‘doing the greatest good for the greatest number’ requires resource allocation on the basis of need which, in turn, requires a process to identify and prioritize the needs of the presenting population.
In the ED, urgency is distinct from severity, prognosis, complexity and case mix, although a correlation exists. Some urgent problems (for example, upper airway obstruction) have a poor outcome without rapid intervention but are not severe in the sense of requiring long-term care, other severe problems (for example, life-threatening malignancy) may not require any treatment in the ED time frame. Complexity is reflected in the number of interventions, such as investigations or consultations required, whereas case mix is an indication of the resources required to provide care.
Triage is an ongoing process that may change in response to alterations in patient status and resource availability, but it is efficient to undertake a formal process once, early in the patient’s encounter, and then review only as necessary. ED triage is normally undertaken by trained nursing staff at the time of arrival and the assigned urgency is then used to guide treatment order. ‘Triage’, used as a noun, is now regarded as the first point of patient contact in EDs.
The overall efficiency and effectiveness of such a system depends not only on the allocated priority but also on the treatment strategy, that is, the way in which the next patient is chosen from the different queues. A more urgent case should wait less time than a less urgent case but, when resources become available to treat the next patient, choice may still be required between a new arrival and a slightly less urgent patient who has already been waiting for some time. It may also be a more efficient strategy in terms of both waiting time and patient care time to ‘stream’ particular patients to particular providers, for example uncomplicated muscular injuries to a physiotherapist.
Australasian triage development
The first Australasian description was of the Box Hill Triage Scale by Pink and Brentnall in 1977 [3]. They used verbal descriptions without time consideration and classified patients into five categories: immediate, urgent, prompt, non-urgent and routine. Fitzgerald modified this scale in 1989 [4], to produce the Ipswich Triage Scale. This used five colours to categorize patients according to the question: ‘This patient should under optimal circumstances be seen within…’. The five categories were seconds, minutes, an hour, hours and days. Fitzgerald found his triage scale to have good interobserver reliability on formal testing and to be a practical predictor of ED outcome and length of ICU stay, but a relatively poor predictor of outcome at hospital discharge.
Jelinek [5] investigated the relationship between the Ipswich Triage Scale and case mix, observing a strong correlation between triage categorization and overall use of resources in the ED and validated possible funding models. He proposed two possible case mix classifications: urgency and disposition groups (UDGs – 12 groups) and urgency related groups (URGs – 73 groups) based on urgency, disposition and diagnosis. After trimming for outliers, these were found to account for 47% and 58% of the cost variance in large hospitals.
In 1994, the Australasian College for Emergency Medicine formalized the National Triage Scale [6], derived from the Ipswich Triage Scale. This used colours, names or numerical categories to represent five groups, based on the answer to the question ‘This patient should wait for medical care no longer than…’. The categories were: immediate, 10 minutes, 30 minutes, 1 hour and 2 hours. The definition document also proposed Jelinek’s concept [5] of performance indicators based on the proportion of patients whose care fell within the desired time threshold and audit by means of admission rates and sentinel diagnoses. It influenced treatment strategies by indicating the need to achieve performance indicators in a high proportion of patients in every category (higher in the more urgent) and it clearly established the need for EDs to employ systematic, accountable and audited triage processes.
Over the next few years, the National Triage Scale was widely accepted and recognized by all Australian State Governments as an appropriate measure of access to emergency care. It was also adopted in the performance indicators promulgated by the Australian Council on Healthcare Standards [7]. Research repeated the findings of Fitzgerald and Jelinek with reference to the new 5-point scale and investigated many more of the subtleties of triage scale use.
The Australasian Triage Scale
The Australasian Triage Scale (ATS) [8] is the current refinement of the National Triage Scale (NTS). It has been jointly developed by the Australasian College for Emergency Medicine, emergency nursing organizations and other interested parties. For practical purposes, the scale concept itself is unchanged, but the ATS uses numeric classification only, better defines waiting time and includes associated implementation guidelines and educational material, partly derived from work on the NTS in areas such as mental health triage [9]. Further training packages have subsequently been developed [10], secondary to concerns about variation in triage training [11].
The ATS categorizes patients presenting to EDs in response to the question: ‘This patient should wait for medical assessment and treatment no longer than…’ (Table 26.4.1)
Table 26.4.1
The ATS categorization of patients presenting to EDs
|
ATS category |
Treatment acuity (maximum waiting time) |
|
ATS 1 |
Immediate |
|
ATS 2 |
10 minutes |
|
ATS 3 |
30 minutes |
|
ATS 4 |
60 minutes |
|
ATS 5 |
120 minutes |
Other triage scales
The concept of desirable waiting time must include some subjective component but has, nevertheless, been found to be reliable and reproducible. Achievement of ATS waiting times has proven to be a useful performance indicator, but remains a measure of process rather than ED outcome. Concerns have been expressed in some jurisdictions about the medicolegal implications of a time-based threshold which will not always be met and other systems have taken different approaches in development of their own ED triage systems. Nevertheless, most have developed five-level triage systems along the Australasian model. Major validated triage scales include:
![]() the Canadian Emergency Department Triage and Acuity Scale (CTAS) [12]: derived from the ATS but using a 15-minute threshold in category 2
the Canadian Emergency Department Triage and Acuity Scale (CTAS) [12]: derived from the ATS but using a 15-minute threshold in category 2
![]() the Manchester Triage Scale [13]: uses an algorithmic approach to the UK Triage scale, similar to the ATS but with longer thresholds in the lower acuity categories
the Manchester Triage Scale [13]: uses an algorithmic approach to the UK Triage scale, similar to the ATS but with longer thresholds in the lower acuity categories
![]() the ESI Triage Algorithm [14]: developed in the USA without any time thresholds, but using a simple approach to classifying urgency.
the ESI Triage Algorithm [14]: developed in the USA without any time thresholds, but using a simple approach to classifying urgency.
Use beyond waiting time
Triage is based on a brief assessment and an individual triage categorization can reflect only the probability of certain outcomes. Large populations of triaged patients, however, exhibit predictable patterns. There is a very strong, almost linear relationship between triage category and total rate of admission, transfer or death, ranging from 80–100% in ATS 1 to 0–20% in ATS 5 [15]. This pattern is repeated across hospitals of different size and different patient mix. Admission rates by triage category follow the pattern of overall admission rates in relation to age, giving a flattened ‘U-shaped’ distribution. The inter-rater reliability studies performed using the Ipswich Triage Scale have been repeated using the NTS/ATS, which has been found to be slightly better [16]. Further, admission rates by triage category have been shown to be constant over time in individual institutions [17].
The NTS/ATS has been extensively studied as a case-mix tool. ED outcome (admission/transfer/death versus discharge) accounts for the largest variance in cost, but triage categorization comes a close second, with age third. The mean cost of care for a category 1 patient is approximately 10 times that of a category 5 patient. Urgency and Disposition Groups (UDGs), described by Jelinek using the Ipswich Triage Scale, have been validated using the National Triage Scale on large samples [18]. Age has been included to derive urgency, disposition and age groups (UDAGs – 32 groups), which account for 51% of the cost variance and are not susceptible to different diagnostic approaches [19]. The relativities derived in these studies should no longer be considered valid in the era of overcrowding and access block, because staff costs for admitted patients reflect length of time in the ED, which may now be driven by outside factors. Further, the costs for discharged patients are becoming skewed by increased pressure to keep complex patients out of hospital.
Triage categorization is a very strong predictor of ED outcome and a good predictor of utilization of critical care resources. However, it is a relatively poor predictor of outcome at hospital discharge [20,21]. Many patients with chronic or subacute conditions that frequently cause death are triaged to less urgent categories because there is no benefit from earlier treatment within the time scales available in the ED.
Attainment of performance indicators for patients seen within triage thresholds has been shown to be a measure of resource allocation within the ED. A longitudinal comparative study has demonstrated a significant improvement with an increase in ED staff and funding [22].
Triage staff are well able to assess complexity [23] and so initial triage is also the appropriate point to start streaming decisions, for example to a ‘fast track’ area for low-complexity patients [24]. Although streaming can be seen as decreasing equity because the less urgent patients achieve shorter waiting times than more urgent, in practice, this is compensated by the gain in overall efficiency [25–27]. Like the triage process itself, changes to the treatment strategy, such as streaming, can and should be ongoing, reflecting not the urgency of the patients, but the best distribution of the resources available at that moment.
Structure and function of a triage system
The exact requirements for triage vary with the role, location and size of the hospital, but effective systems share a number of important features, mostly derived from experience:
![]() A single point in the ED near the entrance where triage is undertaken so that all patients will be exposed to the nurse(s) undertaking triage.
A single point in the ED near the entrance where triage is undertaken so that all patients will be exposed to the nurse(s) undertaking triage.
![]() Appropriate facilities for undertaking brief assessment and limited treatment (first aid) including relevant equipment and washing facilities for staff and patients.
Appropriate facilities for undertaking brief assessment and limited treatment (first aid) including relevant equipment and washing facilities for staff and patients.
![]() A balance between competing concerns of accessibility, confidentiality and security.
A balance between competing concerns of accessibility, confidentiality and security.
![]() A means of recording assessment and triage categorization that will ‘follow’ the patient through their time in the ED and be available for review afterwards. In most departments, this is now a computerized information system.
A means of recording assessment and triage categorization that will ‘follow’ the patient through their time in the ED and be available for review afterwards. In most departments, this is now a computerized information system.
![]() Contemporary data on the state of the ED and the expected patients, such as the information system and ambulance and police radio systems.
Contemporary data on the state of the ED and the expected patients, such as the information system and ambulance and police radio systems.
Pre-hospital triage
The principle of making best use of available resources to maximize patient outcome remains the basis of triage in any setting. Relatively less therapeutic options are available to pre-hospital providers and patient disposition is generally limited to transport and sometimes choice of hospitals. The initial pre-hospital phase, the travel to the patient, must be undertaken on the basis of minimal information. Most pre-hospital systems are strongly protocol driven and tend towards three or four level assessment: rapid response (lights and sirens), immediate response, routine response or no transport. Once the patient is assessed in the field, there is patient benefit in triaging to the most appropriate hospital for tertiary-level conditions, such as major trauma [28] or ST-elevation myocardial infarction [29].
Military and disaster triage
In situations of overwhelming imbalance between resources and demand, triage remains critical in ensuring that available resources are used to achieve the greatest good. The principles of rapid assessment, documentation and multiple queues for care remain the same, but competing demands on resources may mean triaging cases to receive minimal or no care or treating first those who can return to work or duty. The need for both human and physical resources for more important tasks may profoundly limit individual patient care.
Military and disaster triage require seniority and experience (which by definition is rarely available), the ability to make and defend rapid decisions and a successful liaison with other players outside the medical or nursing hierarchy. Senior personnel with significant experience and preferably with additional training should be chosen for this role if possible. Formal triage and documentation must be brief and will use different scales from those appropriate in the ED.
Controversies and future directions
![]() The research base undertaken on the National Triage Scale has shown it to be relatively reliable and reproducible, but identified some areas for improvement. The Australasian Triage Scale and its associated guidelines and educational materials were designed to address some of the recognized problems with the NTS, but revision and improvement of the Scale will continue. Further study is required on issues including:
The research base undertaken on the National Triage Scale has shown it to be relatively reliable and reproducible, but identified some areas for improvement. The Australasian Triage Scale and its associated guidelines and educational materials were designed to address some of the recognized problems with the NTS, but revision and improvement of the Scale will continue. Further study is required on issues including:
![]() variation in implementation between sites, particularly hospitals of different role delineation
variation in implementation between sites, particularly hospitals of different role delineation
![]() the most appropriate ‘treatment strategy’, that is, how the next patient to be treated is chosen from the various queues, in both normal and overcrowded conditions
the most appropriate ‘treatment strategy’, that is, how the next patient to be treated is chosen from the various queues, in both normal and overcrowded conditions
![]() variation associated with activity or overcrowding – there is evidence of consistency in some hospitals but changes in others
variation associated with activity or overcrowding – there is evidence of consistency in some hospitals but changes in others
![]() variation in approach to paediatric triage, especially between mixed and paediatric EDs and to psychiatric triage
variation in approach to paediatric triage, especially between mixed and paediatric EDs and to psychiatric triage
![]() whether the ATS has any role outside its design base of EDs with 24-hour medical staffing, for example in smaller hospitals and pre-hospital settings.
whether the ATS has any role outside its design base of EDs with 24-hour medical staffing, for example in smaller hospitals and pre-hospital settings.
References
1. Larrey DJ. Surgical memoirs of the campaigns in Russia, Germany, and France. Translated Mercer JC. Philadelphia: Carey and Lea; 1832. Cited in Winslow G. Triage and justice. University of California Press.
2. Weinerman ER, Rateen RS, Robbins A. Yale studies in ambulatory care V Determinants of use of hospital emergency services. Am J Publ Hlth Nations Hlth. 1966;56:1037–1056.
3. Pink N. Triage in the accident and emergency department. Aust Nurses J. 1977;6:35–36.
4. Fitzgerald GJ. Emergency department triage. Doctor of Medicine Thesis. University of Queensland; 1989.
5. Jelinek GA. Casemix classification of patients attending hospital emergency departments in Perth, Western Australia. Doctor of Medicine Thesis. University of Western Australia; 1995.
6. Australasian College for Emergency Medicine: National Triage Scale. Emerg Med (Aust) 1994; 6:145–46.
7. Australian Council on Healthcare Standards. Clinical indicators – a user’s manual. Zetland NSW: ACHS; 1996.
8. Australasian College for Emergency Medicine: Australasian Triage Scale. Emerg Med (Aust) 2002; 14:335–36.
9. Smart D, Pollard C, Walpole B. Mental health triage in emergency medicine. Aust NZ J Psychiatr. 1999;33:57–66.
10. Gerdtz MF, Considine J, Sands N, et al. Emergency triage education kit. In: Australian Commonwealth Department of Health Ageing. Canberra: Commonwealth Government of Australia; 2007;10–15.
11. Kelly AM, Richardson D. Training for the role of triage in Australasia. Emerg Med (Aust). 2001;13:230–232.
12. Beveridge R, Ducharme J, James L. Reliability of the Canadian Emergency Department Triage and acuity scale: interrater agreement. Ann Emerg Med. 1999;34:155–159.
13. Manchester Triage Group. Emergency triage London: Publishing Group; 1997.
14. Wuerz RC, Milne LW, Eitel DR. Reliability and validity of a new five-level triage instrument. Acad Emerg Med. 2000;7:236–242.
15. Whitby S, Leraci S, Johnson D, Mohsin M. Analysis of the process of triage: the use and outcome of the National Triage Scale Liverpool NSW: Liverpool Health Service; 1997.
16. Jelinek GA, Little M. Inter-rater reliability of the National Triage Scale over 11,500 simulated occasions of triage. Emerg Med (Aust). 1996;8:226–230.
17. Richardson DB. No relationship between emergency department activity and triage categorization. Acad Emerg Med. 1998;5:141–145.
18. Erwich MA, Bond MJ, Phillips DG, Baggoley CJ. The identification of costs associated with Emergency Department attendances. Emerg Med (Aust). 1997;9:181–187.
19. Erwich MA, Bond MJ, Baggoley CJ. Costings in the emergency department. Report to the Commonwealth Department of Health and Human Services (Australia); 1996.
20. Dent A, Rofe G, Sansom G. Which triage category patients die in hospital after being admitted through emergency departments? A study in one teaching hospital. Emerg Med (Aust). 1999;11:68–71.
21. Doherty SR, Hore CT, Curran SW. Inpatient mortality as related to triage category in three New South Wales regional base hospitals. Emerg Med (Aust). 2003;15:334–340.
22. Rogers IR, Evans L, Jelinek GA. Using clinical indicators in emergency medicine: documenting performance improvements to justify increased resource allocation. J Accid Emerg Med. 1999;16:319–321.
23. Vance J, Sprivulis P. Triage nurses validly and reliably estimate emergency department patient complexity. Emerg Med Australas. 2005;17:382–386.
24. King DL, Ben-Tovim DI, Bassham J. Redesigning emergency department patient flows: application of Lean Thinking to health care. Emerg Med Australas. 2006;18:391–397.
25. O’Brien D, Williams A, Blondell K, Jelinek GA. Impact of streaming ‘fast track’ emergency department patients. Aust Hlth Rev. 2006;30:525–532.
26. Kwa P, Blake D. Fast track: has it changed patient care in the emergency department? Emerg Med Australas. 2008;20:10–15.
27. Shetty A, Gunja N, Byth K, Vukasovic M. Senior streaming assessment further evaluation after triage zone: a novel model of care encompassing various emergency department throughput measures. Emerg Med Australas. 2012;24:374–382.
28. Cox S, Currell A, Harriss L. Evaluation of the Victorian state adult pre-hospital trauma triage criteria. Injury. 2012;43:573–581.
29. Carstensen S, Nelson GC, Hansen PS, et al. Field triage to primary angioplasty combined with emergency department bypass reduces treatment delays and is associated with improved outcome. Eur Heart J. 2007;28:2313–2319.
26.5 Emergency care in a humanitarian crisis
Angela Jackson and Mark Little
Essentials
1 The worldwide problem of displaced persons is massive and likely to increase. Millions more are displaced within their own countries compared to those refugees who have crossed international borders.
2 Overall responsibility for displaced persons lies with the United Nations High Commission for Refugees (UNHCR), although numerous other organizations also assist.
3 When people are displaced, they often establish alternate homes, usually tented, which increases the risks of disease, violence and social dislocation.
4 The UN has introduced the cluster system to improve communication and coordination of the humanitarian crisis. Involvement of the local community and displaced leaders is essential.
5 The basics of nutrition, shelter, clean water and sanitation are always the most important. Minimum standards (Sphere handbook) exist for the provision of care provided.
6 The four major health threats in a humanitarian crisis are malaria, measles, diarrhoeal illness and respiratory tract infections.
7 For those displaced, the durable solutions are resettlement in their country of origin, integration into the new host country or resettlement into a third country.
8 The ultimate solution to solving the problem of the world’s displaced population is political.
Introduction
Increasingly over the past few years, Australian health professionals, including emergency medicine staff, have responded to humanitarian crises due to conflict or natural disasters within our region. Caring for displaced persons is not a new problem. Since World War II up to 100 million civilians have been forced to flee their homes due to unrest. The major factors that cause people to flee their country include conflict, political repression and persecution, and are as old as humanity. In 1573, the term ‘refugee’ was first used for Calvinists fleeing political repression in the Spanish-controlled Netherlands.
The modern response to refugees started at the end of World War II and, in 1946, the International Refugee Organisation (IRO) was created. The United Nations High Commissioner for Refugees (UNHCR) replaced the IRO in 1951 and the Convention Relating to the Status of Refugees, came into being. This key legal document defines who is a refugee and sets out the rights of those who are granted asylum and the legal obligations of nations that grant it. It has been widely ratified to date and, notably, was signed by the President of Nauru, Marcus Stephen on 17 June 2011. With some fine-tuning over the years it remains the cornerstone of International Refugee Law. It defines a refugee as:
A person who owing to a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion, is outside the country of his nationality and is unable or, owing to such fear, is unwilling to avail himself of the protection of that country; or who, not having a nationality and being outside the country of his former habitual residence as a result of such events, is unable or, owing to such fear, is unwilling to return to it…
The UNHCR encourages countries to receive refugees and to provide them with assistance and protection. One of the major points of the Convention is the principle of ‘non-refoulement’, which means that refugees cannot be forcibly returned to their countries of origin if to do so would threaten their life or freedom.
Perhaps of more concern to the humanitarian community are the large numbers of Internally Displaced Persons (IDPs). IDPs are people displaced from their home but who have not crossed an international border. They are commonly fleeing situations such as internal armed conflict, communal violence and other human rights violations. Although the national government has a responsibility to care and protect IDPs, in many instances, state authorities may not only be the cause of displacement but may lack the will or capacity to address the IDPs’ needs which include, not only humanitarian relief assistance, but also protection. Where a state lacks capacity, it can request humanitarian relief assistance from UNHCR. Since 1992, UNHCR has been focusing more efforts to the protection of IDPs and, since 2007, has taken the lead in complex emergencies.
In 2011, according to UNHCR, there were 42.5 million people displaced worldwide. Of these, 15.2 million were refugees and 26.4 million were internally displaced persons (IDPs); 25.9 million were living under protection of the UNHCR mandate. Pakistan was hosting 1.7 million refugees. Up to 93% of all refugees were being hosted within the region of the country they had fled. The major sources of refugees in 2011 were Afghanistan (2.66 million), Iraq (1.43 million) and Somalia (1.07 million). Of all these refugees, 46% are less than 18 years of age.
There were 2.9 million newly displaced persons in 2011. The largest numbers of IDPs are found in the Democratic Republic of the Congo (DRC) 0.83 million and Pakistan 0.62 million. At the height of the crises in 2010, the floods in Pakistan saw 20 million people displaced. The worldwide problem is clearly significant.
The solution to any displacement problem is ultimately non-medical as the problem is commonly based on political instability. Even in the acute phases of refugee movement, the most important needs are basic and are commonly food, shelter and clean water. Physicians, however, can play a considerable role in relief efforts, particularly where they are adaptable and able to use simple, cheap and effective solutions to problems. Of particular importance, however, is that at all stages of relief assistance, the displaced population, sometimes referred to as ‘the beneficiaries’, must be actively involved in planning and delivery of aid. Affected communities themselves know what they need, who their leaders are and they speak the local language.
Emergency physicians need to have an understanding of the issues and possible solutions for those displaced, including links to appropriate organizations and information where necessary.
Responsibility for refugee care
Until the end of the World War I, the response to refugees was from philanthropic sections of the community. The formation of the League of Nations began the process of the international community assuming responsibility for refugees. In 1921, a High Commission for Refugees was established with a mandate to look after refugees fleeing the Russian and Armenian wars. Its first Commissioner was Fridtjof Nansen, who established a special identity document, the ‘Nansen Passport’, as refugees frequently had no means of identification.
In the wake of World War II, the United Nations (UN) established the International Refugee Organisation to assist the millions of displaced persons in Europe. Between 1947 and 1951, it helped 1.6 million people, mainly Germans and Austrians.
Coordination in a humanitarian crisis
Overcoming problems of poor planning and coordination has been the major thrust of more recent developments. After the Great Lakes Disaster in the early 1990s, it was decided in 1997 to establish a set of minimum standards and rights to which refugees were entitled. The collaborative project, called Sphere, was initiated in 1997 by a group of humanitarian non-government organizations (NGOs) and the International Red Cross and Red Crescent Movement with the overall aim of improving the quality of their actions and accountability during disaster response. The Sphere Project produced a manual that is available free from the website www.sphereproject.org. The Sphere Handbook is widely known and sets out common principles and universal minimum standards for humanitarian response. The Sphere Handbook was first published in 2000 with the most recent revision in 2010. Other organizations, such as Médecins Sans Frontières (MSF), UNHCR and the World Health Organization (WHO), also have several excellent manuals describing in detail the approach to humanitarian emergencies.
The Office for the Coordination of Humanitarian Affairs (OCHA) is the UN agency responsible for mobilizing and coordinating effective and principled humanitarian action in partnership with national and international factors. In 2005, realizing the need for improved coordination to humanitarian crises, OCHA initiated a review of its processes. This resulted in the introduction of the UN clusters with the aim of building sufficient response capacity, improving humanitarian coordination and leadership and building effective partnerships. Organizational leaders are responsible for nine themed clusters at both field and global level coordination. Table 26.5.1 shows the current clusters and their lead agencies.
Table 26.5.1
Clusters and cluster lead agencies

UNICEF: United Nations International Children’s Emergency Fund; WHO: World Health Organization; UNHCR: UN High Commissioner for Refugees; IFRC: International Federation of Red Cross; IOM: International Organization of Migration; OHCHR: Office of the High Commissioner for Human Rights; UNDP: UN Development Program; WFP : World Food Program; FAO: Food & Agriculture Organization; SCF UK: Save the Children Fund UK.
*Agriculture and education were the newer clusters established.
Global cluster leaders develop partnerships, humanitarian preparedness and set standards and policy. At a field level, the cluster lead ensures collaboration and coordination and is accountable to the senior UN person in the country coordinating the response, referred to as the Humanitarian Coordinator. The cluster lead is also the ‘provider of last resort’, which means they must do their utmost to ensure an adequate response and, if lacking resources, seek assistance to receive these resources from others higher up in the UN chain (such as the Humanitarian Coordinator). Any organization responding to a humanitarian crisis and working in a specified area of response (e.g. health) is welcome to attend any relevant cluster meeting.
Funding is another important issue. In 2006, the UN General Assembly established the Central Emergency Response Fund (CERF) to provide funds rapidly for the immediate assistance to a humanitarian crisis. It has a grant facility of $US450 M and a loan facility of $US30 M.
Before you go
The Internet and electronic media are increasingly being used in innovative ways by humanitarian agencies. It is now possible to follow evolving disasters on several websites, such as UN affiliated sites, Red Cross sites, major NGOs and MSF sites and explore what each particular organization is doing. OCHA has an excellent website called Reliefweb (www.reliefweb.int) which gives regular updates on all crises. Relevant data can also be sourced from gapminder (www.gapminder.org). In most humanitarian crises, the health issues are predictable (e.g. orthopaedic injuries with earthquakes). It is important to be aware of the literature and to scan previous reports of health issues within the region where you are intending to travel. As soon as clusters are operational, they will report recent data for the affected region, as will the local Ministry of Health. Where possible, it is preferable to be in contact with these organizations prior to departure. WHO publish on the Internet some excellent manuals on diagnosing and managing cases in humantarian crises and have prepacked medical kits (Interagency Emergency Medical Kits). The Sphere guidelines are an essential resource and the Australian Medical Assistance Team training manual is also helpful.
Personal attributes
Working under difficult conditions imposed by a humanitarian crisis demands special qualities. It is certainly not glamorous and often much of what has been learned from training and practice in the West is either irrelevant or needs modification to suit local conditions and resources. In general the main requirements are:
![]() flexibility, versatility and ability to improvise
flexibility, versatility and ability to improvise
![]() appropriate qualifications and sufficient experience along with the ability to work independently in extreme conditions
appropriate qualifications and sufficient experience along with the ability to work independently in extreme conditions
![]() cultural awareness and sensitivity
cultural awareness and sensitivity
![]() good interpersonal and communication skills and the personality to get along with all types of people
good interpersonal and communication skills and the personality to get along with all types of people
![]() willingness to follow leadership and direction
willingness to follow leadership and direction
![]() good pre-deployment preparation, including appropriate vaccinations and insurance arrangements
good pre-deployment preparation, including appropriate vaccinations and insurance arrangements
![]() acceptance of security and health risks both by the individual and their family.
acceptance of security and health risks both by the individual and their family.
Camps for refugees and IDPs
Persons fleeing war or persecution escape in a variety of ways. They may be integrated within the local community or be accommodated by friends and relatives. Typical, however, is the mass movement of populations either across a country or a border into temporary accommodations or camps. It is under these circumstances that the displaced are most at risk, as they are not accommodated in isolation. There are generally interactions with a local population, which are not necessarily cordial. There may also be important political and ethnic factors within the displaced population themselves, which can lead to tensions or even violence within the camps. This scenario was tragically demonstrated in the post-Rwandan holocaust camps in 1994. Camps themselves can sustain conflict in some areas, for example, the West Bank and the camps on the Thai–Cambodian border which were used as refuges by Khmer Rouge and became a platform from which they could carry on the war.
Responding to a crisis
Emergency phase
As a result of a crisis, due either to war or acts of nature, large populations can be displaced from their normal environment. This often results in large numbers of people, with minimal or no basic life needs, descending upon a region and where they stop is generally where a camp evolves. Most population movements into such camps occur in developing countries that already have limited resources with which to deal with such issues. Preplanning by the UN, aid agencies and host governments is essential to ensure a rapid and well-coordinated humanitarian response. Considerable expertise in responding to refugee emergencies has been gained and the main priorities are now well recognized. In accordance with Sphere guidelines the main priorities are as follows.
Initial assessment
A rapid assessment of the population structure, their medical and other needs, is essential in the very early stages to prioritize planning and allocate resources appropriately. It is essential to involve local leaders and population in assessing needs and planning priorities.
Measles immunization
Conditions in refugee camps can facilitate large-scale measles epidemics which, in an at-risk population, can have devastating consequences. In 2011, the UNHCR reported that in one of the Dollo Ado camps in Ethiopia – host to mainly Somali refugees – up to 10 children per day were dying, mainly due to measles and malnutrition. Combined with malnutrition, measles can have a case fatality rate as high as 33%. The detection of one case of measles in a camp is a public health emergency and requires urgent intervention. Mass vaccination of all children from 6 months to 15 years is essential and should be done as soon as possible. To increase vaccination efficacy, WHO recommend combining measles vaccination with the administration of vitamin A. According to WHO, vitamin A has been shown to reduce the burden of disease mortality and morbidity, particularly in children less than 5 years, by improving immune response. The dosing schedule for vitamin A administration is available from the WHO website and is age specific.
Water and sanitation
Poor water supply and sanitation play a major role in the spread of diarrhoeal diseases. Well-defined standards that can be checked with simple kits now exist for acceptable water quality. The Sphere guidelines stipulate minimum quantities of water in the emergency phase of a disaster are 5 L/person/day initially and rising to 15 L/person/day when possible. Sphere also set standards for the location, type and number of latrines and washing facilities per person in camp situations.
Food and nutrition
Malnutrition is common in refugee populations and particularly in the at-risk young and elderly groups. The initial food ration recommended is 2100 kcal/person/day. It is also important to undertake surveys to assess for specific micronutrient deficiencies, such as scurvy or pellagra, and treat accordingly. Measurement of mid-upper arm circumference (MUAC) in children between 6 months and 5 years is a common quick way to asses the overall nutritional status of a population.
Assessment of nutrition in the population is an ongoing process and special feeding programmes may need to be set up for at-risk groups. Generally, there are specific agencies, such as the UN World Food Program, which specialize in this area. It is therefore important that adverse findings are reported to the health cluster to determine who will be responsible for targeting the at-risk population.
Shelter and site planning
Proper shelter and adequate clothing are essential early priorities. Overcrowding can lead to or worsen disease outbreaks and may affect the mental health of the camp population. Protection from the elements is essential for well-being and particularly so in extreme climates. When planning camps, it is important to consider the size, terrain, security, access in and out, nearby water supply, distance to host community, etc. Again, well-defined standards for living space and shelter construction exist.
General healthcare
Organizing a system to deal with the health needs of a population is essential. Medical needs of a population are rapidly assessed and endemic diseases taken into account. There may be numerous organizations involved in health delivery activities. To avoid duplication and the waste of valuable resources, it is important for all providers to participate in ongoing communication and health planning. In disaster situations, this is best achieved by reporting to the health cluster, which has overall responsibility to coordinate the health response. Accurate data collection and reporting is necessary to monitor response progress. There are manuals and guidelines available to assist and WHO have created medical kits intended to cover the needs per 1000 refugees for a 3-month period.
Control of infectious disease
The four most frequent infectious diseases in the emergency phase are diarrhoea, malaria, respiratory infections and measles. Providing good basic living conditions will help ward off these and other illnesses; however, if an outbreak occurs, there is potential for high mortality rates. Aggressive treatment and decisive public health interventions are therefore essential. As diarrhoea is a major cause of death, the early establishment of oral rehydration centres is essential.
Public health surveillance
Collecting epidemiological data on a daily basis provides essential information to those in charge of a camp so that interventions can be planned and disease outbreaks rapidly recognized. The most useful health indicator is the daily crude mortality rate (CMR), which is normally expressed as deaths/10 000 population/day. The Sphere manual gives baseline CMRs for different regions worldwide. Double the baseline CMR is an indication the emergency threshold has been reached. If the baseline CMR is unknown then a CMR of over 1/10 000/day for adults (or 2/10 000/day for children less than 5 years) is an indicator of an emergency situation. Disease-specific mortality rates may also be useful.
Human resources and training
Administering a refugee camp is complex and requires a variety of skilled personnel who include doctors, nurses, water/sanitation experts, nutritionists, logisticians and others. The need for different types of personnel should be determined followed by appointment of the appropriate personnel – ideally from the local population where possible.
Post-emergency phase
This phase begins when the basic needs of the population are met (food, shelter, water and so on) and the CMR is either back to the baseline or less than 1 per day/10 000 for the adult population and 2 per day/10 000 for the under 5 year olds. The situation in the post-emergency phase is complex and fluid. Some of the displaced persons may become quite settled and start to work locally or farm some land. The health and nutritional status of refugees may even surpass those of the local population because of the availability of overseas aid. This may lead to resentment. Complex political issues may arise. Where a large population remains in place, descent back to the emergency phase is an ongoing possibility and may occur with epidemic outbreaks or fresh influxes of newly displaced people. In general, however, the post-emergency phase is concerned with consolidating earlier achievements, preparation for possible new emergencies and future sustainability. The continuation of water quality monitoring, public health surveillance and nutritional status assessment is important for early detection and intervention.
Healthcare delivery in the post-emergency phase is complex. Some issues that warrant consideration for planning purposes include:
![]() standardization of training, supervision and delivery of health services
standardization of training, supervision and delivery of health services
![]() curative healthcare services
curative healthcare services
![]() reproductive healthcare, including antenatal and delivery, postnatal and family planning, sexually transmitted infections (STIs) and HIV/AIDS
reproductive healthcare, including antenatal and delivery, postnatal and family planning, sexually transmitted infections (STIs) and HIV/AIDS
![]() child health activities, such as expanded programmes of immunization (EPIs)
child health activities, such as expanded programmes of immunization (EPIs)
![]() specific HIV/AIDS/STI programmes
specific HIV/AIDS/STI programmes
![]() tuberculosis programmes
tuberculosis programmes
![]() addressing psychosocial and mental health issues.
addressing psychosocial and mental health issues.
Permanent ‘durable’ solutions
There are three possible solutions to any displaced situation – repatriation, integration or resettlement in another country. Many displaced populations reside in countries neighbouring their own country and are thereby the responsibility of the UNHCR. Repatriation is the preferred option but is often quite complex. In 2011, UNHCR reported that 532 000 refugees were voluntarily repatriated. This will generally only occur where there is a solution to the problem that caused the refugees to leave initially. This can take years. People returning need a lot of extra support in order to rebuild their lives. At the time of repatriation, some families have lived in refugee camps for years and children and grandchildren have been born in camps in the host country. The newborns may have no link to the original country they fled and have more of a relationship with the host country and hence, some refugees remain in the host countries and integrate into local communities. In the past, integration into the host community was commonplace in African nations but, more recently, has become increasingly difficult, particularly when African governments see their Western counterparts’ increasing reluctance to accept refugees.
The minority of refugees who cannot return are resettled in third (mostly Western) countries. Many countries have quotas and will only admit those refugees determined by UNHCR as having a valid claim. In 2011, the UNHCR reported 80 000 refugees were resettled. Of these, the USA took 51 500, Canada took 12 900 and Australia received 9200.
Past problems
In the past, there have been important problems with the response to a refugee crisis. Often these have their root in poor coordination between agencies responding to a particular crisis. It is well documented that poor coordination has in the past led to inappropriate interventions and even frank competition. Often, in a dramatic disaster, such as an earthquake which has considerable media coverage, there is a frenzy of intervention as agencies attempt to get their image across to international viewers to assist in fundraising. In the 2001 earthquake in Gujarat province, India, it was estimated that there were as many as 200 different government and non-government agencies in the field. There is no doubt that such competition has resulted in unnecessary death, most notably in the great lakes region of Africa following the Rwandan genocide.
Controversies and future directions
![]() There is often a lack of coordination and communication between agencies involved in responding to a humanitarian crisis. The challenge is to coordinate the response and maximize efficiencies and outcomes.
There is often a lack of coordination and communication between agencies involved in responding to a humanitarian crisis. The challenge is to coordinate the response and maximize efficiencies and outcomes.
![]() Since the Haiti earthquake of 2010, there has been a call for the standardization and registration of foreign medical teams responding to humanitarian crises, the aim being to improve the quality and appropriateness of medical care.
Since the Haiti earthquake of 2010, there has been a call for the standardization and registration of foreign medical teams responding to humanitarian crises, the aim being to improve the quality and appropriateness of medical care.
![]() Developing durable solutions for the world’s displaced population that stands at 42.5 million is challenging. Part of the challenge is to change the attitude of many developed countries towards accepting these people for resettlement.
Developing durable solutions for the world’s displaced population that stands at 42.5 million is challenging. Part of the challenge is to change the attitude of many developed countries towards accepting these people for resettlement.
![]() Instead of spending millions of dollars each year on international staff to assist in humanitarian crises, would this money be better spent if given directly to those affected by the crisis?
Instead of spending millions of dollars each year on international staff to assist in humanitarian crises, would this money be better spent if given directly to those affected by the crisis?
![]() Although the UN cluster system has been established, there is a need to build resilience in this system.
Although the UN cluster system has been established, there is a need to build resilience in this system.
![]() Disaster risk reduction and mitigation is probably more important than humanitarian response and, in the long term, will be more effective. Unfortunately, this is an area that needs more support and planning, although there has recently been an increase in effort in this area.
Disaster risk reduction and mitigation is probably more important than humanitarian response and, in the long term, will be more effective. Unfortunately, this is an area that needs more support and planning, although there has recently been an increase in effort in this area.
Further reading
1. Emergency Relief Items. Vols 1 & 2. United Nations Development Program; 2000.
2. Hospitals for War Wounded 1998 International Committee of the Red Cross.<www.icrc.org/eng/assets/files/other/icrc_002_0714.pdf>This is the entry point into the UN agencies, such as OCHA and its various branches. Also publishes situation reports of evolving disasters.
3. International Committee of the Red Cross site.<www.icrc.org>. This is more concerned with war zones.
4. International Federation of Red Cross and Red Crescent societies.<www.ifrc.org>.
5. Médecins Sans Frontières (MSF)<www.msf.org>. The MSF website is a very useful resource with several free publications on refugee healthcare.
6. Médecins Sans Frontières. Refugee health, an approach to emergency situations. McMillan Education Ltd; 1997. This and many other invaluable MSF texts on treatment protocols, basic kits are all available free on the MSF website<www.msf.org>.
7. Oxfam.<www.oxfam.org>.
8. Relief Web.<www.reliefweb.int>. A UN website with information on humanitarian relief organizations. Information in what is happening in recent crises as well as job availablility.
9. The Sphere Project.<www.sphereproject.org>. The Sphere handbook and related resources.
10. UNHCR.<www.unhcr.org>. Refugee facts, figures and histories.
11. World Health Organisation.<www.who.int>. Health topics, data and programmes. Good information and publications.
26.6 Emergency department observation wards
Jessamine Soderstrom
Essentials
1 Observation wards play a key role in modern emergency departments.
2 They have an increasing role in improving patient flow while maintaining quality of care and safety in the era of National Emergency Access Target (NEAT).
3 Staffing is ideally by emergency department staff with defined admission criteria and a plan for disposition usually within 24 hours.
4 They offer time-limited intensive treatment with clear treatment and follow-up guidelines.
5 Observation wards reduce length of stay and cost compared to inpatient ward admissions.
Introduction
The observation ward is an essential part of an emergency department (ED) that has evolved over time to service changing needs. Its growth is a response to the emergency physician’s desire not to be forced into a dichotomous decision to admit or discharge patients. It provides a third option for medically complex patients who require more diagnostic testing and therapeutic intervention in a short time frame. Observation wards are defined by the following general characteristics [1–4]:
![]() discrete wards with 4–20 beds, located adjacent to or in close proximity to the main body of the ED
discrete wards with 4–20 beds, located adjacent to or in close proximity to the main body of the ED
![]() capacity to care for approximately 5–10% of the total ED volume
capacity to care for approximately 5–10% of the total ED volume
![]() staffed and run by ED personnel
staffed and run by ED personnel
![]() provide an area for patients who require further treatment or diagnostics before being safely discharged
provide an area for patients who require further treatment or diagnostics before being safely discharged
![]() the average length of stay is 10 hours and 80% of patients are discharged home.
the average length of stay is 10 hours and 80% of patients are discharged home.
Acute care hospitals are facing enormous pressures to improve patient access and flow while maintaining quality of care and patient satisfaction without increasing costs. In the era of improved patient flow and time targets (e.g. 4-hour rule or National Emergency Access Target [NEAT]), the observation ward provides a degree of control and flexibility to emergency physicians to extend investigation and care beyond the 4-hour targets. The benefits of having an observation ward adjacent to the emergency department include [1–4]:
![]() allowing patients to access investigations before leaving the emergency department, ensuring accurate diagnosis and formulation of a discharge plan
allowing patients to access investigations before leaving the emergency department, ensuring accurate diagnosis and formulation of a discharge plan
![]() admission to the correct inpatient service once an accurate diagnosis has been made
admission to the correct inpatient service once an accurate diagnosis has been made
![]() provides an alternative to inpatient hospital admission as a way to improve efficiency, clinical care and patient satisfaction, while minimizing the costs [1,3]
provides an alternative to inpatient hospital admission as a way to improve efficiency, clinical care and patient satisfaction, while minimizing the costs [1,3]
![]() reducing inpatient admissions [1,3]
reducing inpatient admissions [1,3]
![]() temporary holding areas for access blocked patients
temporary holding areas for access blocked patients
![]() temporary accommodation for patients (e.g. elderly or those with acute situational crisis) where discharge at an antisocial hour would be inappropriate
temporary accommodation for patients (e.g. elderly or those with acute situational crisis) where discharge at an antisocial hour would be inappropriate
![]() safeguard for junior medical staff who require assistance with disposition plans
safeguard for junior medical staff who require assistance with disposition plans
![]() shorter length of stay and cost compared to inpatient stay (Table 26.6.1) [1].
shorter length of stay and cost compared to inpatient stay (Table 26.6.1) [1].
Table 26.6.1
Cost and LOS comparisons for observation ward vs inpatient care

EDOU: Emergency department observation units; LOS: length of stay; TIA: transient ischaemic attack.
Adapted from Baugh C, Venkatesh A, Bohan J. Emergency department observation units: a clinical and financial benefit from hospitals. Hlth Care Manag Rev 2011;36:28-37 [1] with permission.
Observation ward policies and protocols
The overall function of the observation ward varies depending on the needs of the individual department. There are some common requirements essential to the smooth functioning of the ward [1–4].
Admission process
There must be clear medical governance and responsibility for the patient at all times. This will vary between institutions based on the functionality of the observation ward. Minimizing the number of handovers during the patient’s journey through the observation ward reduces medical errors. As an example, if the observation ward functions primarily as a clinical decision unit to await investigations, then the care should remain with the primary physician. The aim is to have a senior clinician making key decisions, minimizing handovers and ensuring nursing staff are aware of who to contact in the event of patient deterioration. All patients must have a treatment plan, defined objectives for admission and conditions to be met prior to discharge.
Admission criteria
Admission criteria need to be clear. Suitable patients require time limited intensive treatment or have single system problems with clear treatment and follow-up guidelines. It is useful to have pre-negotiated referral pathways to other inpatient teams in the event of failed discharge planning. The general principle of admission to the observation ward is an expectation by the admitting doctor that the patient will be discharged within a set time limit (usually within 24 hours). This will vary depending on the available resources of each department. Some examples of conditions that may be treated in an observation ward include the following [1–9]:
Time-limited intensive treatment:
![]() renal colic
renal colic
![]() mild to moderate asthma
mild to moderate asthma
![]() gastroenteritis
gastroenteritis
![]() migraines
migraines
![]() analgesia and mobilization after soft-tissue injuries
analgesia and mobilization after soft-tissue injuries
![]() commencement of therapy that will be continued out of hospital by hospital in the home services, general practitioners or home care nurses (e.g. intravenous antibiotics for cellulitis).
commencement of therapy that will be continued out of hospital by hospital in the home services, general practitioners or home care nurses (e.g. intravenous antibiotics for cellulitis).
Patients requiring a longer ED stay before a disposition decision can be made:
![]() requiring investigations before disposition planning (e.g. clinical decision unit)
requiring investigations before disposition planning (e.g. clinical decision unit)
![]() post-procedure observation (e.g. lumbar puncture or Bier’s block)
post-procedure observation (e.g. lumbar puncture or Bier’s block)
![]() alcohol and drug intoxication
alcohol and drug intoxication
![]() minor head injury with normal Glasgow coma scale (GCS) for neurological observation
minor head injury with normal Glasgow coma scale (GCS) for neurological observation
![]() envenoming requiring a period of investigation and treatment.
envenoming requiring a period of investigation and treatment.
Patients requiring input from allied health (e.g. physiotherapy, occupational therapy or social work), psychiatric services or where discharge after hours is not appropriate:
![]() elderly or other vulnerable patients to ensure safety for discharge, or where after hours discharge is inappropriate
elderly or other vulnerable patients to ensure safety for discharge, or where after hours discharge is inappropriate
![]() acute situational crisis where patients would benefit from psychiatric input.
acute situational crisis where patients would benefit from psychiatric input.
Other uses of an observation ward
![]() A ‘holding bay’ as a means of decanting access-blocked patients. This can be a useful means of decongesting the ED but can also impair the function of the observation ward (reducing capacity of the observation ward to accept observation ward patients)
A ‘holding bay’ as a means of decanting access-blocked patients. This can be a useful means of decongesting the ED but can also impair the function of the observation ward (reducing capacity of the observation ward to accept observation ward patients)
![]() Chest pain assessment unit – for low-risk chest pain patients [10–12]
Chest pain assessment unit – for low-risk chest pain patients [10–12]
![]() Toxicology unit – providing care for envenomed patients, acutely poisoned patients not requiring intensive care procedures and after intensive care (ICU) admission. Such units may be run by clinical toxicologists where present and have been demonstrated to be efficient, particularly in post-ICU care, reducing length of stay in the ICU [13].
Toxicology unit – providing care for envenomed patients, acutely poisoned patients not requiring intensive care procedures and after intensive care (ICU) admission. Such units may be run by clinical toxicologists where present and have been demonstrated to be efficient, particularly in post-ICU care, reducing length of stay in the ICU [13].
Exclusion criteria
Exclusion criteria will vary between institutions. There are some general themes [2]:
Patients who clearly require>24-hour admission:
![]() patients who have more than one or complex medical problems, especially the elderly
patients who have more than one or complex medical problems, especially the elderly
![]() patients without clear treatment plans or who will not meet conditions for discharge in a timely fashion.
patients without clear treatment plans or who will not meet conditions for discharge in a timely fashion.
Patients who require intensive nursing care:
![]() patients who are a heavy nursing load, e.g. those who are immobile, requiring full care with all their activities of daily living (ADLs)
patients who are a heavy nursing load, e.g. those who are immobile, requiring full care with all their activities of daily living (ADLs)
![]() patients who are violent, psychotic or disruptive.
patients who are violent, psychotic or disruptive.
Some patients are admitted to the observation ward pending review and opinions from inpatient teams where the expectation is that the patient will be discharged. It is important that inpatient treatment is not delayed unnecessarily.
Efficiency of patient care
The observation ward is an area of rapid patient turnover within a defined time frame. There are a number of factors that assist with the efficient running of the ward [1–4]:
![]() Senior clinician input is required for rapid decision making and referral as necessary. Ward rounds and presence of the senior decision maker is not affected by weekends or public holidays (as may be the case with other inpatient teams).
Senior clinician input is required for rapid decision making and referral as necessary. Ward rounds and presence of the senior decision maker is not affected by weekends or public holidays (as may be the case with other inpatient teams).
![]() Defined clinical pathways and referral process to facilitate patient disposition. This improves and streamlines the referral process. As an example, the management of renal colic should be a straightforward process with analgesia, imaging and referral to urology as required [7]. Efficiencies can be gained by negotiation with radiology for a streamlined process for appropriate imaging and admission, discharge and follow-up criteria with urology. These pathways need to be negotiated at a departmental level and this improves efficiency by streamlining the process and removing any inconsistencies in management.
Defined clinical pathways and referral process to facilitate patient disposition. This improves and streamlines the referral process. As an example, the management of renal colic should be a straightforward process with analgesia, imaging and referral to urology as required [7]. Efficiencies can be gained by negotiation with radiology for a streamlined process for appropriate imaging and admission, discharge and follow-up criteria with urology. These pathways need to be negotiated at a departmental level and this improves efficiency by streamlining the process and removing any inconsistencies in management.
![]() Access to allied health staff. In many hospitals, allied health teams have been established within the emergency department to reduce the number of admissions and expedite care in the community, especially in the elderly age group. They are an invaluable part of the team; this includes physiotherapist, social workers, discharge coordinators, occupational therapist, drug and alcohol counsellors and psychiatry liaison nurses.
Access to allied health staff. In many hospitals, allied health teams have been established within the emergency department to reduce the number of admissions and expedite care in the community, especially in the elderly age group. They are an invaluable part of the team; this includes physiotherapist, social workers, discharge coordinators, occupational therapist, drug and alcohol counsellors and psychiatry liaison nurses.
![]() Ten to 20% of patients in the observation ward will be further referred to inpatient teams for admission. This is a key performance indicator in most departments. For this group of patients, it is important to negotiate priority admission to inpatient wards so as not to impact on the efficiency of the ward.
Ten to 20% of patients in the observation ward will be further referred to inpatient teams for admission. This is a key performance indicator in most departments. For this group of patients, it is important to negotiate priority admission to inpatient wards so as not to impact on the efficiency of the ward.
Staffing
Observation wards are staffed by ED personnel. It is important to have defined medical governance. This means that there is a specified senior clinician who is responsible for the patients at all times. The precise detail varies between departments. The nursing staff usually rotate between the emergency department and the observation ward.
Audit and feedback
As the function of the observation ward evolves and matures, it is important to have some form of monitoring and auditing process. Some key performance indicators have been established. Examples of these include:
![]() number of observation ward patients transferred to the care of inpatient teams (internationally 10–20% is acceptable)
number of observation ward patients transferred to the care of inpatient teams (internationally 10–20% is acceptable)
![]() occupancy rates
occupancy rates
![]() length of stay
length of stay
![]() discharge to home rate
discharge to home rate
![]() representation rates within 48 hours
representation rates within 48 hours
![]() adverse events and outcomes
adverse events and outcomes
![]() complaints.
complaints.
Conclusions
The emergency observation unit is an integral extension of the emergency department. Its value is in improved clinical decision making and improved flow, especially in the overcrowded emergency department. There is increasing evidence for various discrete conditions where the role of the observation unit reduces hospital admission rates and length of stay.
As the emergency observation unit matures in some institutions, it has taken on the role as a defined diagnostic and therapeutic unit. It will be interesting to see how the emergency observation unit interacts with other short-stay units in the future. The role of the emergency physician in the care of patients beyond 24 hours is slowly expanding, with an increasing number developing an interest in short-stay medicine. This can only be a positive move, allowing emergency physicians to expand their interests, for job satisfaction and professional longevity, while meeting increasing demands for improved flow and throughput.
Controversies
The latest controversies relate to funding. With the introduction of activity-based funding and the 4-hour rule or NEAT:
![]() What is the definition of an admission? There is now a separate category of short-stay admission (with length of stay less than 8 hours) and an observation unit observation (with length of stay greater than 8 hours).
What is the definition of an admission? There is now a separate category of short-stay admission (with length of stay less than 8 hours) and an observation unit observation (with length of stay greater than 8 hours).
![]() There is a blurring of boundaries between acute assessment units, chest pain assessment units and observation medicine.
There is a blurring of boundaries between acute assessment units, chest pain assessment units and observation medicine.
![]() What is the true financial benefit of an observation ward: do such wards change emergency physicians’ behaviour by reducing the number of discharges? [3]
What is the true financial benefit of an observation ward: do such wards change emergency physicians’ behaviour by reducing the number of discharges? [3]
References
1. Baugh C, Venkatesh A, Bohan J. Emergency department observation units: a clinical and financial benefit from hospitals. Hlth Care Manage Rev. 2011;36:28–37.
2. Williams A, Jelinek GA, Rogers IR. The effect of establishment of an observation ward on hospital admission profiles. Med J Aust. 2000;173:411–414.
3. Ventakesh AK, Geisler BP, Gibson Chambers JJ, et al. Use of observation care in US emergency departments, 2001–2 to 9. PLos ONE. 2011;6:e24326.
4. Jagminas L, Partridge R. A comparison of emergency department versus in hospital chest pain observation units. Am J Emerg Med. 2005;2:111–113.
5. Wiler J, Ross MA, Ginde AA. National study of emergency department observation services. Acad Emerg Med. 2011;18:959–965.
6. McDermott MF, Murphy DG, Zalenski RJ, et al. A comparison of emergency department observation units between emergency diagnostic and treatment unit and in-patient care in the management of acute asthma. Arch Intern Med. 1997;157:2055–2062.
7. Ross MA, Compton S, Medado P. An emergency department diagnostic protocol for patients with transient ischemic attack: a randomized controlled trial. Ann Emerg Med. 2007;50:109–119.
8. Greenberg RA, Dudley NC, Rittichier KK. A reduction in hospitalization, length of stay, and hospital charges for croup with the institution of pediatric observation unit. Am J Emerg Med. 2006;7:818–821.
9. Schrock JW, Rezvikova S, Weller S. The effect of an observation unit on the rate of ED admission and discharge for pyelonephritis. Am J Emerg Med. 2010;28:682–688.
10. Grossman S, Shapiro N, et al. Is telemetry useful in evaluation chest pain patients in an observation unit. Intern Emerg Med. 2011;6:545–546.
11. Roberts RR, Zalenski RJ, Mensah EK, et al. Costs of an emergency department-based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial. J Am Med Assoc. 1997;278:1670–1676.
12. Goodacre S, Nicholl J, Dixon S, et al. Randomized controlled trial and economic evaluation of a chest pain observation unit compared with routine care. Br Med J. 2004;328:254.
13. Western Australia Toxicology Service (Royal Perth Hospital data) 2009–2012.
26.7 Overcrowding
Drew Richardson
Essentials
1 Overcrowding is the situation where emergency department (ED) function is impeded primarily by the excessive number of patients needing or receiving care.
2 Access block is excessive delay in accessing appropriate inpatient beds and, in Australasia, is defined as the proportion of patients with longer than 8 hours total ED time.
3 Access block is the principal cause of overcrowding but overall demand is also increasing.
4 Although multiple different definitions have been used in studying overcrowding and access block, there is clear evidence that both are associated with diminished quality of care and worse patient outcomes including mortality.
5 Changes to ED structure and function including senior staffing, increased size, fast-track observation units and multidisciplinary discharge procedures can to some extent improve the function of the ED in the face of overcrowding, but do not address the underlying causes and are easily overwhelmed by increasing access block.
6 The causes of overcrowding and hence the solutions lie largely outside the ED, especially in managing hospital bedstock in such a way that inpatient beds remain available.
Introduction
Wherever human beings gather there are fluctuations in number and, without outside control, numbers occasionally exceed the efficient maximum for a given purpose. Emergency departments (EDs) are designed largely for ongoing flow of patients rather than gathering, but even in systems designed purely for flow (such as roads) there are peaks and troughs of activity and occupancy sometimes exceeds the number able to move safely and smoothly.
Overcrowding to the point of dysfunction has gradually become the norm in Australasian EDs since the mid-1990s. The greatest contributing factor has been access block, the inability of patients requiring inpatient admission to access appropriate beds in a timely fashion, a phenomenon which is generally called ‘boarding’ in North America. There has additionally been some increase in demand on EDs in both number and complexity of patients resulting from the enlarging, ageing population and the growth in diagnostic and therapeutic choices. This has not been matched by growth in other services, especially outside office hours, increasing the burden on EDs.
Theoretical basis of overcrowding
Queuing theory indicates that the length of a queue and hence the waiting time to treatment is determined by the arrival rate, the treatment rate and the baulk rate (did not wait to be seen rate, which is usually dependent on the length of the queue). An individual patient’s access to emergency care is dependent first on their urgency (assuming the patient is triaged to the correct queue), secondly on the number of similar patients already waiting ahead and thirdly, on the rate and strategy of treatment. Treatment rate is dependent on staffing and on the number of patients already being treated (occupancy), which determines physical availability of resources and the competing demands on staff. On a daily basis, patient flow is significantly dependent on occupancy because even a small decrease in treatment rate has a cumulative effect: it further increases the number waiting ahead of each new arrival.
EDs can be considered as overcrowded when treatment is dysfunctional, that is, the treatment rate is reduced or the treatment quality suffers. Some authorities believe that an ED can be purely overcrowded with patients waiting to be seen while the treatment function remains optimal, others regard this situation as a ‘surge’ – a subset of disaster medicine, rather than an overcrowding problem.
Definition of overcrowding
The Australasian College for Emergency Medicine (ACEM) defines ED overcrowding [1] as the situation where ED function is impeded primarily because the number of patients waiting to be seen, undergoing assessment and treatment or waiting for departure exceeds either the physical or the staffing capacity of the ED. Access block is quantified as the proportion of admissions to hospital, transfers to other hospitals and deaths that have a total ED time of greater than 8 hours [1].
The American College of Emergency Physicians defines crowding [2] as occurring when the identified need for emergency services exceeds available resources for patient care in the ED, hospital, or both, a definition deliberately closer in spirit to that of disaster medicine. Most research on the subject, however, is concerned with the balance between daily fluctuations and ED occupancy, rather than the response to mass-casualty surges.
‘Crowding’ might be the more descriptive term, but ‘overcrowding’ is in common use and researchers have used multiple definitions in attempts to quantify the phenomenon. All major recognized definitions incorporate occupancy with patients under treatment, but many also include subjective factors and outcomes, such as ambulance bypass, which are not applicable to all EDs.
Retrospectively identified episodes of overcrowding tend to be reliable for research but are of only strategic significance in ED management. Real-time assessments may be correlated with patient service (number of patients waiting correlates well with waiting time for new arrivals) but are only useful if there is a managerial commitment to intervening. Predictive algorithms based on the number being treated suffer from false positives and again are only justified if interventions exist to prevent deterioration in flow.
Although there are multiple scales proposed and used to define overcrowding [3,4], recent research indicates that overcrowding to some extent is a local problem: variation in ED performance metrics between apparently similar departments cannot be easily explained in terms of routinely collected data [5]. Validation studies are difficult and many rely on ambulance diversion as an outcome measure, which is only suitable for multi-ED urban centres. The few Australasian studies have not shown US-derived scales to be clinically useful in real time [6].
Causes of overcrowding
The single most important factor affecting ED overcrowding is the availability of inpatient beds [7–9]. Bed availability depends not only on the number of physical beds but also on the way the bedstock is managed. Modelling of extensive hospital datasets has identified the importance of discharge practice [10], patient complexity [11] and even admission practice at off-peak times [12] to ED flow at peak times. ED overcrowding is best seen as a marker of whole-of-hospital dysfunction which requires a whole-of-hospital response [13].
Hospitals providing a local service in areas of significant demographic change, such as a large ageing cohort or rapid growth, may experience ED overcrowding simply through the pressure of presenting numbers exceeding appropriate ED changes. Although locally hospitals may rarely close when demand falls, overall ED demand continues to increase worldwide at rates well above population growth [14,15], reflecting both changing patient expectations and demographics. This will likely be exacerbated among Western cohorts with a large ageing ‘baby boomer’ population.
Development and adoption of new diagnostic and therapeutic approaches and therapies has contributed to increases in total ED time in some groups. Chest pain ‘rule-out’ protocols using delayed marker measurements and increasing use of computed tomography (CT) scans for conditions such as abdominal pain are two examples. These are only partly mitigated by shorter, protocol-driven care of other conditions, for example routine CT for minor head injury with immediate discharge after a normal result rather than observation. Substitution of hospital admission by longer ED stays is likely contributing to an increase in ED ‘practice intensity’ but admission numbers are rising as well [15].
Consequences of overcrowding
Adverse effects of hospital overcrowding have been described since the birth of modern medicine and ED overcrowding had been seen as undesirable since before the recognition of emergency medicine as a specialty. In Australasia, access block was recognized as a quality issue from 1998 [16], first shown to be associated with decreased ED function in 2000 [17] and defined by the ACEM from 2002 [1]. Worldwide, properly conducted research started in 2001 and, since that time, multiple studies in different centres have found an association between overcrowding and reduced access to care [17–19], decreased quality measures [19–22]and lesser outcomes [23–25]. This relationship is robust and applies both to patients who experience delay in obtaining an inpatient bed and to those who present to, or are unlucky enough to already be in, an overcrowded department.
The most important studies are those linking overcrowding with excess patient mortality. The first well-controlled studies were Australian [26,27] and they have been followed by multiple, large, well-designed international studies linking mortality with ED overcrowding in specific disease processes [28,29], patients who ‘board’ in ED [30], admissions [31], discharges [32] and in populations served by potentially overcrowded EDs [33,34]. Demonstration of the link with quality measures, widespread similar results and a dose–response effect have removed any doubt that the relationship between overcrowding and mortality is causative.
Strategies to deal with overcrowding
EDs have an obligation to reduce overcrowding and to mitigate its effects. Multiple successful strategies have been described at an individual ED level, although systematic reviews have tended to be critical of the quality of the evidence [35]. There is no doubt that overcrowding can be reduced, but single interventions may not be easily transferred between different EDs.
As noted, any reduction in overcrowding will be largely achieved through whole-of-hospital changes. Long time series suggest that, in the absence of hospital-wide changes, access block tends to continue to increase even after mitigation efforts within the ED [36]. However, long-term, jurisdiction-wide reports make it clear that overcrowding can be reduced by increasing hospital resources and provision of appropriate incentives [37–39].
Increases in the number and seniority of ED staff are associated with improvements in process measures [40,41] and are a widely used initial response to overcrowding. Physical rebuilding is used to increase patient care spaces but changes in flow dynamics are highly dependent on the rest of the hospital [42]. Analysis of flow and system redesign can allow better use of existing resources [43]. Use of senior medical staff earlier in the patient’s journey (at triage) [44], triage nurse ordering of investigations [45] and streaming of selected patients through a rapid assessment (‘fast track’) area [46] are all effective interventions in the ED. None of these responses can be used indefinitely if access block keeps increasing.
Mandated time targets for ED patients associated with appropriate hospital-wide incentives are effective at reducing overcrowding. Evidence from the British and Western Australian experience with a ‘4-hour rule’ has not shown a negative effect on quality, safety or use of tests [47]. There are early suggestions that patient mortality may be reduced with study ongoing [39]. It is worth noting that hospital commitment to aiming at such a target appears to have beneficial effects on ED function even if the target is not fully achieved.
Evidence is accumulating in favour of hospital enforced ‘overcapacity protocols’ which distribute the overcrowding burden between ED and inpatient areas [48]. Major success has been reported in Alberta, Canada, again without apparent detrimental effects on patient care [49].
Discretionary, low-complexity presentations by patients who might reasonably be managed elsewhere, often incorrectly called ‘GP-type’ patients, constitute a significant number but an insignificant workload in most EDs [50]. Such presentations have a short assessment and treatment time and do not need fixed capacity spaces, such as resuscitation rooms, so their contribution to occupancy with patients under treatment is low. However, being of lower triage urgency their contribution to the number waiting at any given time is relatively high. Use of Primary Care professionals in ED to provide non-urgent care has not been shown to be beneficial [51].
Telephone advice services have not been shown to reduce ED workload in Australasia [52,53] but are highly regarded by the public. Dedicated ED fast-track areas [46] address the management of low-complexity patients in an efficient manner and thus tend to improve overall waiting time performance and staff and patient satisfaction. Their contribution to reducing occupancy with patients under treatment, and hence improving ambulance offload, is low.
EDs also themselves have a small but significant role in reducing hospital occupancy. Observation medicine within the ED is a useful adjunct or alternative to formal inpatient admission [54]. Multidisciplinary assessment and discharge is effective at reducing representation at least in the elderly [55].
Conclusions
Overcrowding has changed the nature of emergency medicine practice. Access block represents a useful simple description of overcrowding because the fundamental issue is the availability of inpatient beds. There is a causal relationship between overcrowding and worse patient outcomes including mortality. Emergency physicians have a role to play in maintaining patient care function in the face of overcrowding, but most of the solutions lie outside the ED.
Future research
The relationship between overcrowding and adverse outcomes is accepted to be causal. Large, well-designed studies of hospital- or system-wide interventions to reduce overcrowding, with adequate follow up to detect improvements in outcome, especially mortality, are now being undertaken and will assist in clarifying barriers and enablers in improving ED overcrowding.
Controversies/future directions
There are medicopolitical, financial and ethical controversies related to ED overcrowding.
![]() Political dimension: ED overcrowding is the product of hospital overcrowding, that is lack of available inpatient beds. Hospital overcrowding is likely to continue while hospital funding schemes favour elective surgery over emergency cases and utilization over efficiency. Politically driven funding incentives can improve this situation but sufficiently robust change is not yet widespread.
Political dimension: ED overcrowding is the product of hospital overcrowding, that is lack of available inpatient beds. Hospital overcrowding is likely to continue while hospital funding schemes favour elective surgery over emergency cases and utilization over efficiency. Politically driven funding incentives can improve this situation but sufficiently robust change is not yet widespread.
![]() Financial dimension: demand for healthcare is effectively unlimited, but demand for current levels of care will grow as the cohort of ‘baby boomers’ age, meaning significant rationing is inevitable if health spending remains contained. Although EDs have a role to play in reducing admissions, the major change needs to be in increasing early discharges, as the inpatient bed-day is the largest driver of acute hospital costs.
Financial dimension: demand for healthcare is effectively unlimited, but demand for current levels of care will grow as the cohort of ‘baby boomers’ age, meaning significant rationing is inevitable if health spending remains contained. Although EDs have a role to play in reducing admissions, the major change needs to be in increasing early discharges, as the inpatient bed-day is the largest driver of acute hospital costs.
![]() Ethical dimension: emergency physicians are comfortable with rationing on the basis of need – it is the foundation of the triage system. However, rationing by queuing becomes fundamentally inefficient once the time in the queue starts to approach the time course of the disease. The current institutional culture of the majority of hospital units does not accept rationing of care to ward inpatients even when other patients with clearly greater medical needs are waiting for immediate access. These differences partly reflect ethical conflict between the principles of justice for all patients and beneficence for individual patients.
Ethical dimension: emergency physicians are comfortable with rationing on the basis of need – it is the foundation of the triage system. However, rationing by queuing becomes fundamentally inefficient once the time in the queue starts to approach the time course of the disease. The current institutional culture of the majority of hospital units does not accept rationing of care to ward inpatients even when other patients with clearly greater medical needs are waiting for immediate access. These differences partly reflect ethical conflict between the principles of justice for all patients and beneficence for individual patients.
References
1. Australasian College for Emergency Medicine. Policy document–standard terminology. Emerg Med (Aust). 2002;14:337–340.
2. American College of Emergency Physicians. Crowding. Ann Emerg Med. 2006;47:585.
3. Hwang U, Concato J. Care in the emergency department: how crowded is overcrowded? Acad Emerg Med. 2004;11:1097–1101.
4. Jones SS, Allen TL, Flottemesch TJ, et al. An independent evaluation of four quantitative emergency department crowding scales. Acad Emerg Med. 2006;13:1204–1211.
5. Pines JM, Decker SL, Hu T. Exogenous predictors of national performance measures for emergency department crowding. Ann Emerg Med. 2012;60:293–298.
6. Raj K, Baker K, Brierley S, et al. National emergency department overcrowding study tool is not useful in an Australian emergency department. Emerg Med Australas. 2006;18:282–288.
7. Hostetler MA, Mace S, Brown K, et al. Subcommittee on Emergency Department Overcrowding and Children, Section of Pediatric Emergency Medicine, American College of Emergency Physicians Emergency department overcrowding and children. Pediatr Emerg Care. 2007;23:507–515.
8. Trzeciak S, Rivers EP. Emergency department overcrowding in the United States: an emerging threat to patient safety and public health. Emerg Med J. 2003;20:402–405.
9. Crilly J, Keijzers G, Krahn D. The impact of a temporary medical ward closure on emergency department and hospital service delivery outcomes. Qual Manag Hlth Care. 2011;20:322–333.
10. Khanna S, Boyle J, Good N, Lind J. Unravelling relationships: hospital occupancy levels, discharge timing and emergency department access block. Emerg Med Australas. 2012;24:510–517.
11. Rathlev NK, Obendorfer D, White LF, et al. Time series analysis of emergency department length of stay per 8-hour shift. West J Emerg Med. 2012;13:163–168.
12. Luo W, Cao J, Gallagher M, Wiles J. Estimating the intensity of ward admission and its effect on emergency department access block. Stat Med 2012; In: http://dx.doi.org/10.1002/sim.5684; 2012.
13. Richardson DB. Reducing patient time in the emergency department. Med J Aust. 2003;179:516–517.
14. Pitts SR, Pines JM, Handrigan MT, Kellermann AL. National trends in emergency department occupancy, 2001 to 2008: effect of inpatient admissions versus emergency department practice intensity. Ann Emerg Med. 2012;60:679–686.
15. FitzGerald G, Toloo S, Rego J. Demand for public hospital emergency department services in Australia: 2000–2001 to 2009–2010. Emerg Med Australas. 2012;24:72–78.
16. Baggoley C. President’s message. Emerg Med (Aust). 1998;10:169–171.
17. Richardson DB. Quantifying the effects of access block [abstract]. Emerg Med (Aust). 2001;13:A10.
18. Fatovich DM, Nagree Y, Sprivulis P. Access block causes emergency department overcrowding and ambulance diversion in Perth, Western Australia. Emerg Med J. 2005;22:351–354.
19. Vieth TL, Rhodes KV. The effect of crowding on access and quality in an academic ED. Am J Emerg Med. 2006;24:787–794.
20. Dunn R. Reduced access block causes shorter emergency department waiting times: an historical control observational study. Emerg Med (Aust). 2003;15:232–238.
21. Schull MJ, Vermeulen MJ, Slaughter G, et al. Emergency department crowding and thrombolysis delays in acute myocardial infarction. Ann Emerg Med. 2004;44:577–585 Erratum in Ann Emerg Med 2005; 45:84.
22. Fee C, Weber EJ, Maak CA, et al. Effect of emergency department crowding on time to antibiotics in patients admitted with community-acquired pneumonia. Ann Emerg Med. 2007;50 501–9, 509.e1.
23. Carr BG, Kaye AJ, Wiebe DJ, et al. Emergency department length of stay: a major risk factor for pneumonia in intubated blunt trauma patients. J Trauma. 2007;63:9–12.
24. Liew D, Liew D, Kennedy MP. Emergency department length of stay independently predicts excess inpatient length of stay. Med J Aust. 2003;179:524–526.
25. Chalfin DB, Trzeciak S, Likourezos A, et al. DELAY-ED study group Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35:1477–1483.
26. Sprivulis PC, Da Silva JA, Jacobs IG, et al. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust. 2006;184:208–212.
27. Richardson DB. Increase in patient mortality at 10 days associated with emergency department overcrowding. Med J Aust. 2006;184:213–216.
28. Hong YC, Chou MH, Liu EH, et al. The effect of prolonged ED stay on outcome in patients with necrotising fasciitis. Am J Emerg Med. 2009;27:385–390.
29. Jo S, Kim K, Lee JH, et al. Emergency department crowding is associated with 28-day mortality in community-acquired pneumonia patients. J Infect. 2012;64:268–275.
30. Singer AJ, Thode Jr HC, Viccellio P, Pines JM. The association between length of emergency department boarding and mortality. Acad Emerg Med. 2011;18:1324–1329.
31. Sun BC, Hsia RY, Weiss RE, et al. Effect of emergency department crowding on outcomes of admitted patients. Ann Emerg Med. 2012;5 S0196-0644(12)01699-X.
32. Guttmann A, Schull MJ, Vermeulen MJ, Stukel TA. Association between waiting times and short term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario, Canada. Br Med J. 2011;342:d2983.
33. Shenoi RP, Ma L, Jones J. Ambulance diversion as a proxy for emergency department crowding: the effect on pediatric mortality in a metropolitan area. Acad Emerg Med. 2009;16:116–123.
34. Shen Y, Hsia RY. Association between ambulance diversion and survival among patients with acute myocardial infarction. J Am Med Assoc. 2011;305:2440–2447.
35. Morris ZS, Boyle A, Beniuk K, Robinson S. Emergency department crowding: towards an agenda for evidence-based intervention. Emerg Med J. 2012;29:460–466.
36. Richardson DB. Responses to access block in Australia: Australian Capital Territory. Med J Aust. 2003;178:103–104.
37. Weber EJ, Mason S, Carter A, Hew RL. Emptying the corridors of shame: organizational lessons from England’s 4-hour emergency throughput target. Ann Emerg Med. 2011;57:79–88 e1.
38. Richardson DB, Kelly A-M, Kerr D. Prevalence of access block in Australia 2004–8. Emerg Med Australas. 2009;21:472–478.
39. Geelhoed GC, de Klerk NH. Emergency department overcrowding, mortality and the 4-hour rule in Western Australia. Med J Aust. 2012;196:122–126.
40. Rogers IR, Evans L, Jelinek GA, et al. Using clinical indicators in emergency medicine: documenting performance improvements to justify increased resource allocation. J Accid Emerg Med. 1999;16:319–321.
41. Cardin S, Afilalo M, Lang E, et al. Intervention to decrease emergency department crowding: does it have an effect on return visits and hospital readmissions? Ann Emerg Med. 2003;41:173–185.
42. Han JH, Zhou C, France DJ, et al. The effect of emergency department expansion on emergency department overcrowding. Acad Emerg Med. 2007;14:338–343.
43. King DL, Ben-Tovim DI, Bassham J. Redesigning emergency department patient flows: application of Lean Thinking to health care. Emerg Med Australas. 2006;18:391–397.
44. Rowe BH, Guo X, Villa-Roel C, et al. The role of triage liaison physicians on mitigating overcrowding in emergency departments: a systematic review. Acad Emerg Med. 2011;18:111–120.
45. Rowe BH, Villa-Roel C, Guo X, et al. The role of triage nurse ordering on mitigating overcrowding in emergency departments: a systematic review. Acad Emerg Med. 2011;18:1349–1357.
46. Bullard MJ, Villa-Roel C, Guo X, et al. The role of a rapid assessment zone/pod on reducing overcrowding in emergency departments: a systematic review. Emerg Med J. 2012;29:372–378.
47. Weber EJ, Mason S, Freeman JV, Coster J. Implications of England’s four-hour target for quality of care and resource use in the emergency department. Ann Emerg Med. 2012;60:699–706.
48. Villa-Roel C, Guo X, Holroyd BR, et al. The role of full capacity protocols on mitigating overcrowding in EDs. Am J Emerg Med. 2012;30:412–420.
49. Innes G, McRae A, Holroyd B, et al. Policy-driven improvements in crowding: system-level changes introduced by a provincial health authority and its impact on emergency department operations in 15 centers [abstract]. Acad Emerg Med. 2012;19:s14.
50. Sprivulis P, Grainger S, Nagree Y. Ambulance diversion is not associated with low acuity patients attending Perth metropolitan emergency departments. Emerg Med Australas. 2005;17:11–15.
51. Khangura JK, Flodgren G, Perera R. Primary care professionals providing non-urgent care in hospital emergency departments. Cochrane Database Syst Rev 2012;11.
52. Graber DJ, Ardagh MW, O’Donovan P, et al. A telephone advice line does not decrease the number of presentations to Christchurch Emergency Department, but does decrease the number of phone callers seeking advice. NZ Med J. 2003;116:U495.
53. Sprivulis P, Carey M, Rouse I. Compliance with advice and appropriateness of emergency presentation following contact with the HealthDirect telephone triage service. Emerg Med Australas. 2004;16:35–40.
54. Williams AG, Jelinek GA, Rogers IR, et al. The effect on hospital admission profiles of establishing an emergency department observation ward. Med J Aust. 2000;173:411–414.
55. Caplan GA, Williams AJ, Daly BA. Randomized controlled trial of comprehensive geriatric assessment and multidisciplinary intervention after discharge of elderly from the emergency department – the DEED II study. J Am Geriatr Soc. 2004;52:1417–1423.
26.8 Rapid response systems and the emergency department
Daryl A Jones and Julie Considine
Essentials
1 Up to 17% of hospitalized ward patients suffer serious adverse events (SAEs), including cardiac arrest.
2 These events are often preceded by signs of physiological derangement for up to 24 hours prior to the event.
3 Rapid response systems (RRSs) are designed to review ward patients in the early phases of such deterioration.
4 There is increasing, but conflicting evidence supporting the effectiveness of RRSs in reducing cardiac arrests and unplanned intensive care unit (ICU) admissions in ward patients.
5 Increasing literature suggests that patients in the emergency department (ED) can experience clinical instability which predicts subsequent development of adverse events.
6 Single centre studies suggest that implementing a rapid response system into an ED is feasible.
7 Future research needs to validate activation criteria and response for an ED-specific RRS and to assess the potential benefits of such a system for deteriorating patients in the ED.
Introduction and definitions
Rapid response teams (RRTs) are composed of staff who review acutely unwell hospital ward patients in an attempt to reduce cardiac arrests and other serious adverse events (SAEs) [1]. When the team leader is a doctor, the RRT is called a medical emergency team (MET). A MET should have a number of competencies, including abilities in the following areas [1]:
![]() prescription of therapies
prescription of therapies
![]() advanced airway management skills
advanced airway management skills
![]() insertion of invasive vascular lines
insertion of invasive vascular lines
![]() commencement of intensive care level of care at the bedside.
commencement of intensive care level of care at the bedside.
The term ‘rapid response system’ (RRS) has been proposed to represent an entire system that provides both an ‘afferent’ component to identify patient deterioration and an ‘efferent’ component to assess and treat the patient. Other types of review team include the rapid response team and critical-care outreach team (CCO), which differ in their staff composition, skill set and mechanism of activation [1]. The remainder of this chapter will focus on the MET, which is the predominant model in hospitals in Australia and New Zealand.
Additional components of the RRS include quality improvement and clinical governance arms, which permit audit and evaluation of SAEs and implementation of hospital-wide strategies to prevent recurrence [1].
Epidemiology and principles underlying the MET
Several principles underpin the MET and RRS. In summary, SAEs are common in hospitalized patients and are often preceded by a period of instability of up to 24 h. The MET is summoned to review patients in the early phases of deterioration in an attempt to prevent further deterioration, morbidity and mortality.
SAEs are common in hospitalized patients
Studies in Australia [2], New Zealand [3,4], England [5] and Canada [6] have assessed the incidence of SAEs in hospitalized patients. These studies defined an SAE as ‘unintended injury or complication resulting from medical management rather than the underlying disease process’. They reported an incidence of SAEs ranging between 7.5% and 16.6% and suggested that 36.9–51% were preventable.
A single-centre study in an Australian hospital [7] found that 16.9% of 1125 patients undergoing major surgery suffered at least one of 11 predefined SAEs (which included myocardial infarction, stroke, arrest and respiratory failure).
SAEs are preceded by signs of clinical instability
At least four studies [8–11] have demonstrated that patients suffering SAEs develop new complaints, deterioration of commonly measured vital signs or derangement in laboratory investigations in up to 84% of cases prior to the event. It is for this reason that common triggers for MET activation are based on derangements in vital signs. More importantly, three studies [12–14] have confirmed that patients who develop vital signs that satisfy MET criteria are at increased risk of death.
Deterioration of the MET patient is typically gradual
Unexpected out-of-hospital cardiac arrest is usually sudden and due to cardiac arrhythmias, pulmonary embolism or major vascular catastrophe. In contrast, progression to in-hospital cardiac arrests and other SAEs is typically gradual [8]. This allows sufficient time for intervention and, potentially, prevention of the event.
Early intervention improves outcome
One of the tenets underlying the MET principle is that early intervention in the course of critical illness is associated with improved outcome. This observation has been made in patients suffering trauma [15,16], myocardial infarction [17] and in resuscitation of patients presenting to the emergency department (ED) with sepsis [18].
Skilled staff already exist in the hospital
METs are usually composed of critical-care staff with skills in advanced airway management, insertion of invasive vascular lines and with knowledge of therapies commonly used in acute care medicine (Table 26.8.1). Staff need to be available 24 hours per day, 7 days a week to manage acutely unwell patients anywhere in the hospital [19].
Table 26.8.1
MET staff members and their roles
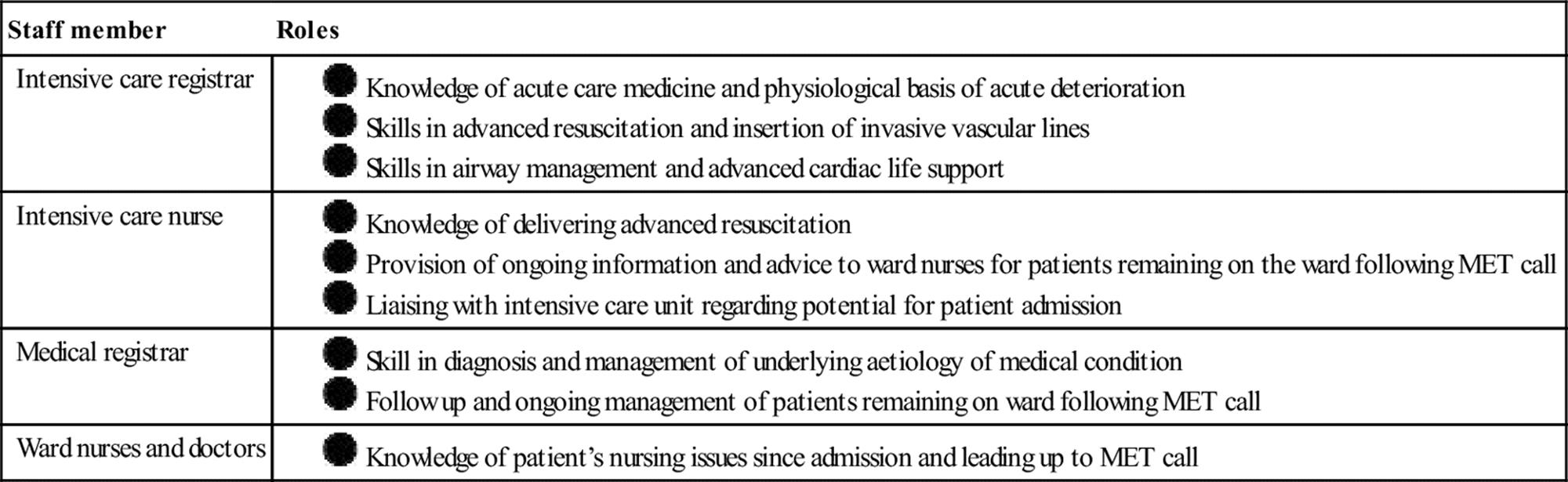
How MET services and RRSs work
Different roles of the MET
The MET was originally described in 1995 when Lee and coworkers reported the introduction of a MET service into Liverpool Hospital in Sydney, Australia [19]. The MET superseded the existing cardiac arrest team and was modelled on rapid detection and correction of abnormal vital signs indicative of trauma teams. In this model, the MET is merely an expansion of the existing cardiac arrest team and reviews all medical emergencies including arrests.
In other hospitals [20,21], two separate RRTs operate: a cardiac arrest team to review patients who have suffered cardiorespiratory arrest and a MET that reviews all medical emergencies other than cardiac arrest.
Activation of the MET – the afferent arm
The MET service is activated when one or more predefined criteria are reached. Typical criteria involve derangement of commonly measured vital signs (Table 26.8.2). Other criteria include conditions such as uncontrolled seizures or chest pain. Finally, some hospital MET criteria contain a ‘staff member worried’ criterion to permit activation of the MET service for any possible medical emergency.
Table 26.8.2
Commonly used MET calling criteria

RR: respiratory rate; BP: blood pressure; UO: urine output.
Composition of the MET – the effector arm
The precise composition of each MET varies between hospitals. Each member has a predefined role (see Table 26.8.1) and simulation or mock sessions may be held as part of training [22]. The teams typically bring their own equipment to the MET call, either on a trolley or in a carry bag, which includes equipment needed for endotracheal intubation, invasive vascular access and medicines and fluids used in advanced resuscitation.
Clinical features of MET patients
Characteristics of triggers leading to MET activation
A number of studies [13,21,23] have reported the relative frequency of MET call criteria leading to MET calls (Table 26.8.3). Variations between hospitals are likely to represent differences in the limits of the criteria as well as differences in local case mix. Hypoxaemia, hypotension and altered conscious state were the commonest causes of MET calls in these studies.
Table 26.8.3
Relative frequency (%) of MET triggers leading to MET calls

Medical conditions leading to MET calls
The clinical cause of MET calls has also been assessed in a number of studies and the concept of ‘MET syndromes’ (e.g. the ‘hypoxic MET syndrome’) has recently been raised [23,24]. Again, variations in case mix and MET calling criteria are likely to account for these differences. In the original description of the MET, Lee and coworkers reported that acute respiratory failure, status epilepticus, coma and pulmonary oedema were the most common causes of MET calls [19]. In a district general hospital, Daly and coworkers reported that chest pain, respiratory distress, seizures and cardiopulmonary arrest caused most MET calls [25]. Finally, a study of 400 MET calls at the Austin hospital [23] revealed that infections, pulmonary oedema and arrhythmias caused 53% of MET calls.
Management of MET call patients
One of the most underinvestigated aspects of the MET system is the details of the management undertaken by the staff during a MET call. De Vita and coworkers have recently reported that use of a detailed curriculum and a computerized human patient simulator resulted in increased task completion rate and improved survival of the simulated patient [22].
An analysis of the MET syndromes associated with 400 MET calls and an approach to their management has been reported [23]. The ‘A to G’ approach described can be used to manage any possible medical emergency and can be used in the management of specific MET syndromes (Table 26.8.4).
Table 26.8.4
A to G approach to management of a hypoxic MET call

MET: medical emergency team; ECG: electrocardiogram; CCF: congestive cardiac failure; COAD: chronic obstructive airways disease.
The MET and the ED
Hospital-wide MET services that involve ED staff and patients
In the original description of the MET system, the ED was one of the hospital areas serviced by the MET and, in fact, was the area that attracted the highest number of MET activations [19]. This approach involves review of ED patients by intensive care unit (ICU) staff and is most appropriate during periods when there are limited senior emergency medical staff, particularly out of hours. In contrast, Daly and coworkers described a MET model for a district general hospital in which staff from the ED formed the core of the MET and reviewed patients in the general wards when the MET service was activated [25].
The MET philosophy in the ED
The MET involves a coordinated multidisciplinary approach to the management of acute deterioration of hospital ward patients [1]. As outlined above (see Table 26.8.1), each member has a designated role coordinated by the team leader. This is similar to the team-based approach to trauma management seen in most EDs and trauma centres (Table 26.8.5).
Table 26.8.5
Similarities and differences between MET services and trauma teams
|
Variable |
Trauma team |
MET service |
|
Location of patient |
Emergency department or trauma centre |
Hospital ward |
|
Team leader |
Typically emergency department doctor |
Typically intensive care unit registrar |
|
Patient profile |
Young with few co-morbidities |
Elderly with multiple co-morbidities |
|
Presenting problem |
Trauma |
Hypoxia, hypotension and tachycardia |
|
Need for early intervention |
Concept of ‘golden hour’ |
Shown for sepsis, myocardial ischaemia, stroke |
The MET system principle is equally applicable in the ED as it is on the hospital ward. For example, a multidisciplinary programme was shown to reduce the hospital mortality rate of patients presenting to a community hospital with non-traumatic shock [26]. Coordinated team work is required for the management of acute myocardial ischaemia, severe sepsis, intracranial haemorrhage and ischaemic stroke. These are discrete clinical entities where the clinical diagnosis is rapidly determined and algorithmic- or guideline-based therapies exist.
How often do patients in ED develop clinical instability?
The epidemiology of deterioration in the ED is poorly understood. Unplanned ICU admission is a well documented largely preventable serious adverse event in general ward patients and is associated with up to a 10-fold increase in mortality [27,28]. It may be argued that there are ED patients in whom ICU admission is unplanned as these patients appear stable on ED arrival (indicated by allocation to lower acuity triage categories) but, subsequently, require ICU admission following clinical deterioration [29]. Australian data can be used to explore the prevalence of ICU admissions of ED patients. Of 6.2 million patients attending Australian EDs annually [30], more than 24 500 patients require ICU admission directly from the ED and over 2700 die [31]. Victorian Government data from 2010–11 show that of the 7220 (0.5%) admissions directly from ED to ICU, 70% (5088) were recognized as critically ill or injured on arrival to the ED (triage category 1 or 2). However, 30% (2132) were assessed as moderate or low acuity (triage category 3, 4 or 5) on ED arrival hence may have suffered an unplanned ICU admission [32].
There is even less information about early deterioration in ED patients. Recent single site pilot studies from Victoria, Australia suggest that approximately 1% of general ED patients (excluding patients in resuscitation areas) Fulfilled organizational MET criteria [33] and 1.5% of ED patients suffered clinical deterioration significant enough to warrant activation of a local ED rapid response system [34].
Clinical instability in ED predicts subsequent adverse outcomes
There is a body of evidence related to the predictors of deterioration in ED patients, the use of modified early warning score (MEWS) in ED and prediction of critical care or ICU admission in ED patients that may be used to inform a standardized approach to deteriorating ED patients. In a study of medical ED patients, Burch et al. [35] found systolic blood pressure≤100 mmHg, pulse rate≥130 per minute, respiratory rate≥30 breaths per minute, temperature≥38.5°C and decreased conscious state on ED arrival were independent predictors of hospital admission. Further, systolic blood pressure≤100 mmHg or≥200 mmHg, respiratory rate≥30 breaths per minute and decreased conscious state on ED arrival were independent predictors of in-hospital death [35]. In this same study, an increased MEWS score was associated with higher rates of hospital admission in medical patients, so MEWS may be used to identify medical patients who require hospital admission and who are at increased risk of hospital death [35]. Similarly, Groarke et al. [36] examined the predictive value of an EWS calculated on hospital presentation in medical patients. For each increase in score category, there was increased risk of ICU admission, CCU admission, death and hospital length of stay[36]. Groarke et al. concluded that early warning score is a potential triage tool for ED medical patients and that improved serial EWS within 4 hours of hospital presentation may be used to predict clinical outcomes.
Known predictors of unplanned ICU admission in patients admitted to hospital via the ED are older age, male gender, higher acuity triage category and a history of co-morbid conditions [37]. Further, diagnostic groups associated with higher incidence of unplanned ICU admission included sepsis, acute renal failure, lymphatic–haematopoietic tissue neoplasms, pneumonia, chronic obstructive pulmonary disease and bowel obstruction [37]. Clinical factors evident on ED arrival predictive of critical care admission (ICU and coronary care unit) in patients triaged as low to moderate acuity were chief complaint of nausea, vomiting and diarrhoea on ED arrival; heart rate or temperature abnormalities at triage; and respiratory rate or heart rate abnormalities at first ED nursing assessment [38]. Hypotension during ED care significantly increases risk of in-hospital death in both trauma [39] and non-trauma patients [40]. The results of these studies demonstrate relationships between mortality and morbidity and ED patient characteristics; physiological abnormalities present on ED arrival; or physiological abnormalities that occur during ED care [37–40] and may be used to inform ED systems for recognition of, and response to deteriorating ED patients. Further, parameters currently absent from inpatient MET criteria, such as advanced age and temperature abnormalities, have been linked to critical-care admission and death and therefore may have a place in increasing recognition of deteriorating ED patients and warrant further investigation [38,41].
Existing studies describing RRS in EDs
There are a number of studies describing RRS in EDs. A review of EWS from the UK showed that high EWS triggered review by senior ED staff in 71% of patients and critical-care input in 44% of patients [42]. However, there are no details of whether a structured approach to escalating care was used or the outcomes of patients not reviewed by senior clinicians or critical-care referral despite high EWS. One recently reported Australian model is a single trigger approach with escalation of care to the emergency physician and nurse in charge to ensure timely review of the patient by senior personnel and mobilization of ED resources as required by personnel who have a global overview of ED activity [34]. This model resulted in two to three early warning system activations per day so did not overburden ED clinicians and simple interventions, such as intravenous fluids and supplemental oxygen, restored physiological normality in most patients within 1 hour [34]. This same model also showed that nurses were well placed to identify deteriorating patients and rapidly escalate care within 5 minutes [34].
The ideal response to deteriorating ED patients is unknown and for many deteriorating patients, the ED response will be appropriate, albeit ad hoc. However, the advantages of a structured and consistent approach to escalation of care include further development of already positive multidisciplinary relationships and enhanced inter-professional communication, particularly for new or transient ED staff [43]. A systematic and ED-led approach to recognizing and responding to deteriorating ED patients is a logical progression, building on other patient safety systems, such as triage and systematized approaches to ED care of critically ill or injured patients. There is a need to develop and test ED-specific approaches to improve the sequential detection, recognition and timely escalation of care for ED patients who have deteriorated after initial triage and assessment [43].
Likely future developments
Despite the absence of level 1 evidence of the effectiveness of MET services, RRSs have been introduced into thousands of hospitals worldwide to manage deteriorating ward patients. RRSs are a key component of the Institute of Health Improvement’s 100 k campaign, which aims to save 100 000 lives across American hospitals [44]. RRSs are also an integral component of The Australian National Safety and Quality Health Service Standards [45]. For these reasons, it is unlikely that further randomized trails will be conducted to assess the effectiveness of METs in improving the outcome of acutely unwell hospitalized patients.
The most important questions that need addressing regarding rapid response systems for ward patients in the near future include:
![]() Why do patients need MET calls? – clinical, disease state and system factors.
Why do patients need MET calls? – clinical, disease state and system factors.
![]() What is the outcome of MET calls?
What is the outcome of MET calls?
![]() What are barriers to MET activation?
What are barriers to MET activation?
![]() How can MET be most effectively used to review patients most likely to benefit from MET service intervention?
How can MET be most effectively used to review patients most likely to benefit from MET service intervention?
![]() In the cases of RRSs in the ED, there is a need to better quantify the point prevalence and consequences of clinical instability and to validate activation criteria.
In the cases of RRSs in the ED, there is a need to better quantify the point prevalence and consequences of clinical instability and to validate activation criteria.
Controversies
The MET service and deskilling of ward staff
The increasing use of MET services to manage acutely unwell hospital ward patients has the potential to deskill ward nursing and medical staff [46]. However, in a survey conducted in hospitals with a well-established MET service, most of the nurses questioned stated that the MET actually taught them how better to manage sick ward patients [47,48].
Improved outcome is demonstrated only in single-centre studies
Reduction in cardiac arrests, unplanned ICU admission and other SAEs following introduction of MET services and RRSs has been shown in a number of single-centre studies [20,21,49–51]. A cluster randomized trial of 23 Australian hospitals was recently reported in which 12 hospitals introduced a MET system and 11 continued with usual care [52]. The study did not demonstrate that introduction of a MET service reduced the incidence of cardiac arrests, unplanned ICU admissions or unexpected deaths. While this finding may suggest that MET services do not improve the outcome of acutely unwell ward patients, the negative result is at least in part due to other factors. First, the education period preceding introduction of the MET was brief (4 months) and the subsequent call rate was only 8.3 calls/1000 admissions [52]. At the Austin hospital, a 1-year education period resulted in a progressive increase in the use of the MET to a call rate of>40 calls/1000 admissions [53].
Most importantly, only 30% of the patients admitted to the ICU who had MET criteria actually received a MET call [52]. Combined, these findings suggest that the negative result of the MERIT study was at least in part due to a failure of MET use as opposed to a failure of the process of MET review.
Other controversies
A number of other problems with the MET service have been proposed [46,54] including inappropriate patient management because the MET is unfamiliar with the patient, diversion of attention away from adequate ward staffing and development of other strategies that might benefit acutely ill ward patients, diversion of critical care staff from their usual duties and conflict between MET staff and the ward staff caring for the patient.
References
1. Devita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med. 2006;34:2463–2478.
2. Wilson RM, Runciman WB, Gibberd RW, et al. The quality in Australian health care study. Med J Aust. 1995;163:458–471.
3. Davis P, Lay-Yee R, Briant R, et al. Adverse events in New Zealand public hospitals I: occurrence and impact. NZ Med J. 2002;115:U271.
4. Davis P, Lay-Yee R, Briant R, et al. Adverse events in New Zealand public hospitals II: preventability and clinical context. NZ Med J. 2003;116:U624.
5. Vincent C, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. Br Med J. 2001;322:517–519.
6. Baker GR, Norton PG, Flintoft V, et al. The Canadian Adverse Events Study: the incidence of adverse events among hospital patients in Canada. Can Med Assoc J. 2004;170:1678–1686.
7. Bellomo R, Goldsmith D, Russell S, et al. Postoperative serious adverse events in a teaching hospital: a prospective study. Med J Aust. 2002;176:216–218.
8. Buist MD, Jarmolowski E, Burton PR, et al. Recognising clinical instability in hospital patients before cardiac arrest or unplanned admission to intensive care A pilot study in a tertiary-care hospital. Med J Aust. 1999;171:22–25.
9. Hodgetts TJ, Kenward G, Vlackonikolis I, et al. Incidence, location and reasons for avoidable in-hospital cardiac arrest in a district general hospital. Resuscitation. 2002;54:115–123.
10. Nurmi J, Harjola VP, Nolan J, et al. Observations and warning signs prior to cardiac arrest Should a medical emergency team intervene earlier? Acta Anaesthesiol Scand. 2005;49:702–706.
11. Schein RM, Hazday N, Pena M, et al. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest. 1990;98:1388–1392.
12. Bell MB, Konrad D, Granath F, et al. Prevalence and sensitivity of MET-criteria in a Scandinavian University Hospital. Resuscitation. 2006;70:66–73.
13. Buist M, Bernard S, Nguyen TV. Association between clinically abnormal observations and subsequent inhospital mortality: a prospective study. Resuscitation. 2004;62:137–141.
14. Goldhill DR, White SA, Sumner A. Physiological values and procedures in the 24 h before ICU admission from the ward. Anaesthesia. 1999;54:529–534.
15. Hedges J, Adams A. Gunnels M ATLS practices and survival at rural level trauma hospitals, 1995–1999. Prehosp Emerg Care. 2002;6:299–305.
16. Nardi G, Riccioni L, Cerchiari E, et al. Impact of an integrated treatment approach to the severely injured patients (ISS>16) on hospital mortality and quality of care. Minerva Anesthesiol. 2002;68:25–35.
17. Fresco C, Carinci F, Maggioni AP, et al. Very early assessment of risk for in-hospital death among 11,483 patients with acute myocardial infarction GISSI investigators. Am Heart J. 1999;138:1058–1064.
18. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–1377.
19. Lee A, Bishop G, Hillman KM. The medical emergency team. Anaesth Intens Care. 1995;23:183–186.
20. Bellomo R, Goldsmith D, Uchino S, et al. Prospective controlled trial of effect of medical emergency team on postoperative morbidity and mortality rates. Crit Care Med. 2004;32:916–921.
21. Bellomo R, Goldsmith D, Uchino S, et al. A prospective before-and-after trial of a medical emergency team. Med J Aust. 2003;179:283–287.
22. De Vita M, Schaefer J, Lutz J, et al. Improving medical emergency team (MET) performance using a novel curriculum and a computerized human simulator. Qual Safe Hlth Care. 2005;14:326–331.
23. Jones D, Duke G, Green J, et al. Medical emergency team syndromes and an approach to their management. Crit Care. 2006;10:R30.
24. DeVita M. Medical emergency teams: deciphering clues to crises in hospitals. Crit Care. 2005;9:325–326.
25. Daly FF, Sidney KL, Fatovich DM. The medical emergency team (MET): a model for the district general hospital. Aust NZ J Med. 1998;28:795–798.
26. Sebat F, Johnson D, Musthafa A, et al. A multidisciplinary community hospital program for early and rapid resuscitation of shock in non-trauma patients. Chest. 2005;127:1729–1743.
27. Haller G, Myles PS, Wolfe R. Validity of unplanned admission to an intensive care unit as a measure of patient safety in surgical patients. Anesthesiology. 2005;103:1121–1129.
28. Bristow P, Hillman K, Chey T, et al. Rates of in-hospital arrests, deaths and intensive care admissions: the effect of a medical emergency team. Med J Aust. 2000;173:236–240.
29. Kennedy M, Joyce N, Howell MD. Identifying infected emergency department patients admitted to the hospital ward at risk of clinical deterioration and intensive care unit transfer. Acad Emerg Med. 2010;17:1080–1085.
30. Australian Institute of Health and Welfare. Australian hospital statistics 2010–11: emergency department care and elective surgery waiting times. Canberra: Australian Institute of Health and Welfare. Health services series no. 41. Cat. no. HSE 115. Retrieved January 2012 from<http://www.aihw.gov.au/publication-detail/?id=6442472405>; 2011.
31. Drennan K, Hart G, Hicks P. Intensive care resources & activity: Australia and New Zealand 2006/2007. Carlton, Victoria Australia and New Zealand Intensive Care Society. Retrieved March 2011 from<http://www.anzics.com.au/core/reports>; 2009.
32. Victorian Health Information Reporting System. Victorian Emergency Department data, Victorian Government Department of Health 2010;2011.
33. Hosking J, Considine J, Sands N. Recognising clinical deterioration in the emergency department: point prevalence of emergency department patients fulfilling MET criteria and patient outcomes. In Tenth international conference for emergency nurses, Hotel Grand Chancellor: Hobart, Australia; October 2012.
34. Considine J, Lucas E, Wunderlich B. The uptake of an early warning system in one Australian emergency department: a pilot study. Crit Care Resus. 2012;14:135–141.
35. Burch VC, Tarr G, Morroni C. Modified early warning score predicts the need for hospital admission and inhospital mortality. Emerg Med J. 2008;25:674–678.
36. Groarke JD, Gallagher J, Stack J, et al. Use of an admission early warning score to predict patient morbidity and mortality and treatment success. Emerg Med J. 2008;25:803–806.
37. Frost SA, Alexandrou E, Bogdanovski T. Unplanned admission to intensive care after emergency hospitalisation: risk factors and development of a nomogram for individualising risk. resuscitation. 2009;80:224–230.
38. Considine J, Thomas S, Potter R. Predictors of critical care admission in emergency department patients triaged as low to moderate urgency. J Adv Nurs. 2009;65:818–827.
39. Sikorski TJ, Black L, Ho E, Mills T. Survival in posttraumatic hypotension. Ann Emerg Med. 2004;44:S128–S129.
40. Jones AE, Yiannibas V, Johnson C, Kline JA. Emergency department hypotension predicts sudden unexpected in-hospital mortality: a prospective cohort study. Chest. 2006;130:941–946.
41. Smith GB, Prytherch DR, Schmidt PE, et al. Should age be included as a component of track and trigger systems used to identify sick adult patients? Resuscitation. 2008;78:109–115.
42. Griffiths JR, Kidney EM. Current use of early warning scores in UK emergency departments. Emerg Med J. 2012;29:65–66.
43. Considine J, Jones DA, Bellomo R. Emergency Department Rapid Response Systems: The case for a standardised approach to deteriorating patients. Eur J Emerg Med. 2013;20:375–381.
44. Overview of the 100,000 Lives Campaign.<http://www.ihi.org/IHI/Programs/Campaign/100kCampaignOverviewArchive.htm>[Accessed Jan. 2007].
45. Australian Commission on Safety and Quality in Health Care. National consensus statement: essential elements for recognising and responding to clinical deterioration. Sydney: ACSQHC, 2010.<http://www.safetyandquality.gov.au/internet/safety/publishing.nsf/Content/F329E60CC4149933CA2577740009229C/$File/national_consensus_statement.pdf>[Accessed Nov. 2012].
46. Brown D, Bellomo R. Are medical emergency teams worth the cost? In: DeVita MA, Hillman K, Bellomo R, eds. Medical emergency teams: a guide to implementation and outcome measurement. New York: Springer; 2006.
47. Jones D, Baldwin I, McIntryre T, et al. Nurses’ attitudes to a medical emergency team service in a teaching hospital. Qual Safe Hlth Care. 2006;15:427–432.
48. Bagshaw SM, Mondor EE, Scouten C, Capital Health Medical Emergency Team Investigators, et al. A survey of nurses’ beliefs about the medical emergency team system in a Canadian tertiary hospital. Am J Crit Care. 2010;19:74–83.
49. Bristow PJ, Hillman KM, Chey T, et al. Rates of inhospital arrests, deaths and intensive care admissions: the effect of a medical emergency team. Med J Aust. 2000;173:236–240.
50. Buist MD, Moore GE, Bernard SA, et al. Effects of a medical emergency team on reduction of incidence of and mortality from unexpected cardiac arrests in hospital: preliminary study. Br Med J. 2002;324:387–390.
51. DeVita MA, Braithwaite RS, Mahidhara R, et al. Use of medical emergency team responses to reduce hospital cardiopulmonary arrests. Qual Safe Hlth Care. 2004;13:251–254.
52. Hillman K, Chen J, Cretikos M, et al. Introduction of the medical emergency team (MET) system: a cluster randomised controlled trial. Lancet. 2005;365:2091–2097.
53. Jones D, Bates S, Warrillow S, et al. Effect of an education programme on the utilization of a medical emergency team in a teaching hospital. Intern Med J. 2006;36:231–236.
54. Joyce C, McArthur C. Rapid response systems: have we MET the need? Crit Care Resus. 2007;9:127–128.
26.9 Public health and emergency medicine
Diana Egerton-Warburton, Jennie Hutton, Peter Aitken and Hilary Tyler
Essentials
1 Public health is a key component of a sustainable health system.
2 Emergency medicine has a mandate to advocate for public health initiatives.
3 Acute healthcare has limited opportunity to affect healthcare outcomes compared to public health.
4 Screening, brief intervention and referral for treatment (SBIRT) are the cornerstone of emergency department (ED) prevention.
5 Disease and injury surveillance is an important function for emergency departments including identification of emerging infectious diseases.
6 Emergency medicine can take a leadership role in highlighting and addressing socially determined health inequalities, particularly the healthcare gap of indigenous and other vulnerable populations.
Introduction
Public health (PH) is an organized attempt by society to ensure a healthy population. It is recognized as key to a sustainable and effective healthcare system. The UN Universal Declaration of Human Rights (1948) states that all people are equally entitled to good health and decent living conditions and it is this humanistic ideal that drives much of public health.
Emergency medicine (EM) is an important but under recognized and utilized player in public health. While at first glance it may appear an anathema to the practice of EM, PH and EM interact over a number of domains. These include: diseases surveillance, healthcare access, disease and injury prevention and advocacy. The International Federation for Emergency Medicine provides a clear mandate for public health in its definition of EM as: ‘A field of practice based on the knowledge and skills required for the prevention, diagnosis and management of acute and urgent aspects of illness and injury’.
Emergency departments (EDs) Australasia-wide see over 7 million attendances annually. This population is receptive to PH intervention in a concept described as the ‘teachable moment’. This has been described as a brief opportunity to intervene to change behaviour. This is particularly pertinent when patients present as a consequence of risky health behaviour. While patients are open to PH messages, providing them in the ED setting is challenging. EDs have limited resources and strive to provide safe and timely acute care. PH roles may be seen as simply adding to the burden. However, many emergency physicians (EP) see PH as part of their role as a healthcare advocate. This has been inculcated by the Australasian College for Emergency Medicine (ACEM) adopting the CanMEDS competency framework, which includes the role of health advocate.
A number of barriers exist to the introduction of PH measures into EDs. Lack of time and resources are almost universally cited and it is recognized that additional resources will be required for widespread adoption. PH roles within the ED are performed by a wide range of clinical and non-clinical staff members.
Increasingly, the social determinants of health affect individuals’ opportunity to have a healthy life. Examples include access to safe and affordable housing, education and exposure to violence. This is particularly the case in indigenous populations. Many ED patients have poor social determinants and limited access to alternate healthcare options. EM should, through its surveillance and advocacy role, help to highlight and address these issues at a community and policy level. Social and environmental factors can be influenced by advocacy both at a local and national level. EP and ACEM are credible and persuasive healthcare advocates to provide effective public health messages.
Disease and injury surveillance
Emergency departments play an ongoing and pivotal role in injury prevention through surveillance. ED surveillance plays an important role in injury campaigns, such as child drowning and road safety. In regards to road traffic accidents, EM has advocated for changes to seat-belt and helmet legislation.
Based upon figures from the World Health Organization (WHO), the health profile of many countries is changing. The burden of non-communicable diseases has risen and will increase further with ageing populations. Non-communicable diseases, mainly cardiovascular diseases, diabetes and cancers, were responsible for 63% of the 57 million deaths that occurred worldwide in 2008.
According to the Australian Institute of Health and Welfare, coronary heart disease, anxiety and depression and type II diabetes are the largest specific contributors to overall burden of disease. Within 15 years, type II diabetes and obesity will be the leading cause.
A small number of unhealthy lifestyle choices, described in Table 26.9.1, account for much of this disease burden. From an Australian perspective, while smoking rates are comparatively low, rates of drinking alcohol, obesity and sedentary lifestyles are relatively high.
Table 26.9.1
Health impact of main risk factors for non-communicable disease
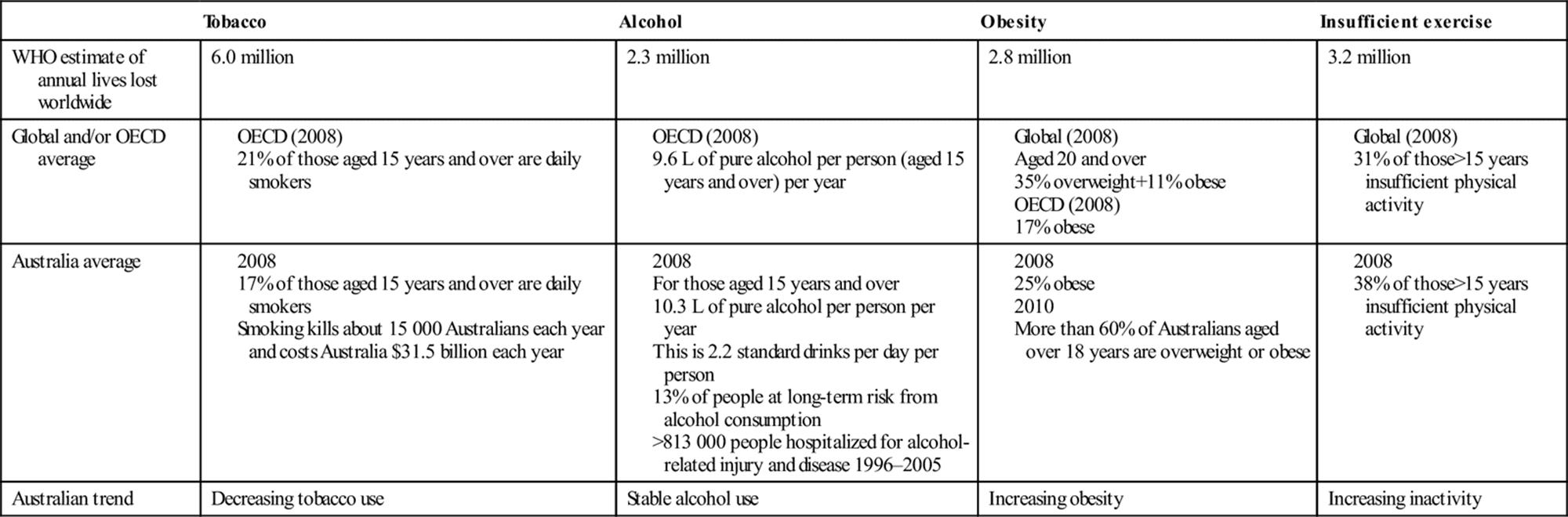
Potentially avoidable diseases account for at least 20% of healthcare expenditure. While Australia spent 8.7% of GDP on health in 2008, the Organization for Economic Cooperation and Development estimated that health spending will increase by 78% over the next four decades, partly due to the rise in preventable conditions. In response to this looming health burden, the WHO and many nations are working to endorse international strategies for health promotion and protection.
Emerging infectious diseases (EID) are increasing and becoming a significant burden on global economies and health [1]. The Institute of Medicine defines EID as: ‘infections whose incidence in humans has increased within the past two decades or whose incidence threatens to increase in the near future’. These may be new pathogens, such as sudden acute respiratory syndrome (SARS) or bat viruses; old pathogens expanding in range and incidence, such as dengue or ebola; and multidrug resistant tuberculosis strains. The majority of EID originates in wildlife and is correlated with socioeconomic, environmental and ecological factors[1]. Increasing temperatures, associated with climate change, may contribute to malaria and dengue extending to more temperate zones [2].
Increased global travel, coupled with the incubation periods of some diseases, such as SARS (2–10 days) or avian influenza (2–10 days), also means travellers may not become ill until returning home. Monitoring increases in ED visits for key ‘chief complaints’ has been shown to provide timely indicators for outbreaks and ED staff should be aware of EIDs and what tests to request. They should be suspected in patients: aged up to 49 years; with life-threatening illness of potentially infectious aetiology; and with no cause for illness identified by preliminary testing [3].
Both screening and diagnostic tests are needed. Screening tests help detect a disease early, often in relatively asymptomatic patients. They are sensitive but often less specific. Screening tests correctly identify those individuals who may have a given disease but often require more specific diagnostic testing to confirm or exclude this. Because screening tests are also performed on larger patient numbers, they should be cheap and simple to perform.
The ED is part of a system with integrated management and communication strategies needed rapidly to identify EID. Collaboration needs to occur locally, regionally, nationally and globally as well as between ED and multiple disciplines.
Disease prevention and control
The role of delivering preventive care may seem at first glance at odds with the normally very pragmatic function of an ED. In the current climate, where EDs are overcrowded and resources scarce, we are challenged to deliver the principal role of acute care. However, ED patients are often those that most need to be targeted for preventive measures and are least able to access it by other means. These populations include: the homeless, people on low incomes, people living with a disability, mental illness, refugees, migrants and indigenous populations. These populations have poor health literacy and limited health access.
There is a growing body of evidence that can guide us as to the optimum way to target our time and resources in the ED setting to deliver effective, efficient preventive care. Bernstein suggests that any intervention would be approached by asking the following questions [4]. Is the public health purpose clear? Is the screening appropriate and accurate? Will the intervention be effective and is this the best approach? Also the intervention needs to be assessed long term and an appropriate endpoint reached.
Prevention in the ED setting can be divided into primary, secondary and tertiary measures. Primary prevention involves intervention in a population prior to illness occurring. In the ED, this would include the routine vaccination of patients with the tetanus immunization and post-exposure prophylaxis for diseases such as rabies, hepatitis and HIV.
Secondary prevention involves an intervention in an at-risk population, early in the course of the disease. A good example in the emergency setting is that of screening for chlamydia. A further example would be a brief intervention for smoking cessation in a patient presenting for an unrelated issue.
Tertiary prevention involves an intervention in a population that is at risk and has experienced a resulting illness. This is treating an established disease which is core EM practice.
Screening, brief intervention and referral for treatment (SBIRT)
SBIRT has been described as the cornerstone of EM preventive care. There is some evidence that supports the use of SBIRT in the ED in family violence, risky alcohol use and smoking cessation. Much of this evidence comes from North America [5].
The methods that traditionally can be utilized for SBIRT include paper-based, computer questionnaire, video and a computer-based intervention. Innovations including the use of new technology and social media will provide many opportunities.
SBIRT need not be resource intensive for EDs, but additional resources are required to make them sustainable [5]. It also requires dedicated time for planning interventions and in measuring outcomes. Both the setting and the provider of the prevention activity may vary. It can occur at any opportune time in the patient’s journey though the ED and by all health workers in the ED.
The cost to Australian society of alcohol, tobacco and other drug misuse in 2004–05 was estimated at $56.1 billion, including costs to the health and hospital system, lost workplace productivity, road crashes and crime. Of this, tobacco accounted for $31.5 billion (56.2%), alcohol accounted for $15.3 billion (27.3%) and illegal drugs $8.2 billion (14.6%) [6].
The act of quitting smoking involves five stages of which a number can occur in an ED. A single physician encounter results in 2% of patients quitting. Routine physician screening and counselling may increase cessation from 3% (usual care) to 8–11% at 6–12 months [7]. Smoking cessation interventions are more cost-effective than other interventions, such as treatment of blood pressure or cholesterol and Pap smears. In one investigation, it was found that EPs were likely to gather information about smoking but not to counsel or educate patients to quit; 56% of discussions with current smokers contained advice to quit, 16% an assessment of readiness to quit and only 13% a referral to quit. Smoking was more likely to be discussed when the patient presented with a smoking-associated condition [7]. Smoking interventions in the ED, even if low efficiency, will have high reach due to the absolute number of smokers attending. This results in a high impact intervention, which is cost-effective.
Over 800 000 Australians aged 15 years or over were hospitalized for alcohol attributable disease or injury in the 10-year period up to 2006 and it is likely that this figure will increase in the following decade [6]. The risk of sustaining an injury increases with the quantity of alcohol consumed and that risk is significantly higher for women.
EDs are well placed to recognize patients with both binge and chronic drinking problems. Validated screening tools can be used. The general efficacy of brief alcohol interventions in these settings has been recognized, although the evidence has been mixed [2]. The effectiveness of brief interventions varies with patient populations and treatment contexts [2]. Some trials have demonstrated small effect sizes, but this may be the result of lack of a true control arm, which typically received more than current standard care.
Many ED-based SBIRT are disease or risk behaviour focused rather that patient centred. They fail to recognize that many risk behaviours interact and are synergistic. They also have limited capacity to consider health literacy and social and cultural determinants of health. Thus, paradoxically, the most vulnerable populations may be least likely to benefit from them. For example, a smoking intervention is not likely to be effective in a person with low health literacy and alcohol dependence. While a role exists for simple effective interventions, future research should be patient centred and take into consideration the social and cultural context. More rigorous multicentred research is required in the Australasian context to determine the effective of SBIRT before widespread introduction can be recommended.
Health of indigenous people and cultural safety
The first peoples of Australia and New Zealand have not fared well from the respective colonization of their countries and this is apparent in the health status of these people. Australia’s Aboriginal and Torres Strait Islander people have poor health outcomes, resulting from limited access to resources, such as adequate housing, education, employment, municipal infrastructure, health services and an enforced dismantling of cultural practice and community governance.
Many chronic diseases are the direct result of overcrowding and poverty. Post-streptococcal glomerulonephritis (PSGN) resulting in end-stage renal disease and high rates of type II diabetes are two striking examples of poverty-related disease. Recurrent streptococcal skin infections resulting in renal disease occurring at an early age is the direct result of poor living conditions. The risk and severity of type II diabetes is a consequence of limited access to affordable healthy food. Issues of alcoholism can be linked to dislocation, homelessness, experiences of racism and despair.
Aboriginal people living in poverty often access healthcare infrequently. Although many co-morbidities may appear to be peripheral to the prime reason for attendance, an opportunistic approach with this group of people and liaison with allied health services, including Aboriginal liaison officers and Aboriginal health services where available, can have long-term health benefits.
New Zealand’s Indigenous Maori have had very similar health issues to combat but there are encouraging signs of improvement in their general health status, although poverty and associated health issues continue in many communities, particularly rural.
Addressing issues of cultural safety and competency in EDs in Australia and New Zealand has the potential to improve healthcare and thus outcomes.
Australian Indigenous Aboriginal and Torres Strait Islanders
According to the Australian Bureau of Statistics in 2011, the median age of death for Australian indigenous men and women is around 20 years less than for non-indigenous Australians. Mortality from coronary artery disease is significantly higher in indigenous people. The overall incidence rate of end-stage renal disease is higher in Aboriginal and Torres Strait Islander people, with an age-standardized notification rate almost 10 times that of non-indigenous Australians. The mortality rate from respiratory disease in those aged 35–44 is 20 times that of other Australians. Infectious diseases, such as tuberculosis, hepatitis, sexually transmitted diseases including HIV/AIDS, Haemophilus influenzae type b and pneumococcal and meningococcal disease are common. The adjusted mortality rate from diabetes is almost seven times the rate for other Australians. These health outcomes are based upon figures from the Australian Institute of Health and Welfare.
Suicide is the third leading cause of death for indigenous males. Significant stressors, such as family death, unemployment, alcohol, trouble with police, overcrowding and discrimination, are common. Assault is the commonest cause of injury and the leading causes of death from injury are intentional self-harm and transport accidents. Overall, fewer Aboriginal and Torres Strait Island people drink alcohol than non-Aboriginal people; however, of those who do drink, more drink at harmful levels [8].
New Zealand’s indigenous Maori people
Even though life expectancy of Maori people has improved, it is still not level with non-Maori in New Zealand. Cardiovascular disease is the leading cause of mortality for Maori, with rates 2.5 times those of non-Maori. Maori and non-Maori have similar self-reported diabetes prevalence, but there are disparities in developing complications, such as renal failure and lower limb amputation. Maori female breast cancer registrations are 1.3 times that of non-Maori and breast cancer mortality is 1.8 times higher than that of non-Maori. Smoking rates are higher in this population with an estimated 50% of Maori female adults smoking.
New Zealand has moved to a focus on reducing inequality across all ethnicities by addressing the issues and barriers and by placing training in cultural safety high in health workforce priorities. Sir Mason Durie [9] gives wise guidance on the three principles that can be gained from the New Zealand experience and applied in Australia, these being integrated solutions, indigenous pathways and empowering relationships.
Cultural safety and cultural competency
To be able to have a positive impact on health status, practitioners working in Australasian EDs must be able to work in a culturally safe manner. This requires an understanding of the social, political, historical and cultural influences on the health of indigenous people.
While indigenous cultures are diverse, themes, such as the importance of customary law, the extended family and kinship obligations, the notion of reciprocity and a differing worldview are common. Identity is complex and it is essential that ED staff do not perpetuate notions of racial percentage and skin colour as determinants of someone’s identity.
It is critical for health professionals to understand and acknowledge the existence of racism and how it has affected the health of indigenous people. Institutional racism [10] relates to the systems, policies and processes that disadvantage indigenous people.
Cultural competence is ‘a set of behaviours and attitudes and a culture within business or system that respects and takes into account the person’s cultural background, cultural beliefs and their values and incorporates them in the way healthcare is delivered to that individual’ [11].
Similarly, cultural safety is defined as a way of practising in which the health professional undertakes a process of reflection on their own cultural identity and recognizes the impact of that culture on their professional practice. Unsafe cultural practice is any action which diminishes, demeans or disempowers the cultural identity and well-being of an individual [12]. A culturally safe health professional is one who knows what culture is, values their own culture, reflects on the interface between power and practice and acts to change unequal power relationships.
Acknowledgements
Hilary Tyler wishes to thank her colleagues, the members of the Indigenous Health Subcommittee.
Controversies/emerging issues
![]() New technologies and social media provide new opportunities in preventive health initiatives in the ED.
New technologies and social media provide new opportunities in preventive health initiatives in the ED.
![]() SBIRT should be rigorously evaluated prior to widespread introduction.
SBIRT should be rigorously evaluated prior to widespread introduction.
![]() PH interventions in the ED will require additional resources in order to be effective and sustainable.
PH interventions in the ED will require additional resources in order to be effective and sustainable.
![]() Smoking cessation and addressing risky alcohol use are priorities for EM.
Smoking cessation and addressing risky alcohol use are priorities for EM.
![]() Developing cultural competency and practising in a cultural safe manner is important for EPs.
Developing cultural competency and practising in a cultural safe manner is important for EPs.
References
1. Jones KE, Patel NG, Levy MA, et al. Trends in emerging infectious diseases. Nature. 2008;451:990–993.
2. Saniotis A, Bi P. Global warming and public health: reasons to be concerned. Aust Hlth Rev. 2009;33:611–617.
3. Perkins BA, Flood JM, Danila R, et al. Unexplained deaths due to possibly infectious causes in the United States: defining the problem and designing surveillance and laboratory approaches The Unexplained Deaths Working Group. Emerg Infect Dis. 1996;2:47–53.
4. Bernstein J, Haukoos J. Public health, prevention and emergency medicine: a critical juxtaposition. Acad Emerg Med. 2008;15:190–193.
5. Bernstein E, Bernstein J, Stein J. SBIRT in emergency care setting: are we ready to take the scale? Acad Emerg Med. 2009;16:1072–1077.
6. National Drug Strategy. Ministerial council on drug strategy Australian Government 2010–2015; <http://www.nationaldrugstrategy.gov.au/>[Accessed Jan. 2013].
7. Vokes N, Bailey J, Rhodes K. ‘Should I give you my smoking lecture now or later?’ Characterizing emergency physician smoking discussions and cesssation counseling. Ann Emerg Med. 2006;48:406–414.
8. Wilson M, Stearne A, Gray D, Saggers S. The harmful use of alcohol amongst indigenous Australians; 2010.<http://www.healthinfonet.ecu.edu.au/alcoholuse_review>[Accessed Jan. 2013].
9. Durie M. Indigenous health: the New Zealand experience. Med J Aust. 2012;197:10–11.
10. Henry BR, Houston S, Mooney GH. Institutional racism in Australian healthcare: a plea for decency. Med J Aust. 2004;180:517–520.
11. Betancourt. InThomson N. Cultural respect and related concepts: a brief summary of the literature. Aust Indig Hlth Bull. 2005;5:1–11.
12. Te Kaunihera Tapuhi o Aotearoa Nursing Council of New Zealand. Guidelines for cultural safety, the Treaty of Waitangi and Maori health in nursing education and practice. Nursing Council of New Zealand. 2011;<http://www.nursingcouncil.org.nz/download/97/cultural-safety11.pdf>[Accessed Jan. 2013].