Arteries of the Upper Limb
Fig. 22.1 Arteries of the upper limb
Right side, anterior view.

Fig. 22.2 Branches of the subclavian artery
Right side, posterior view.
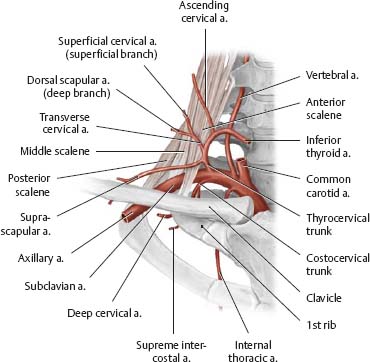
Fig. 22.3 Scapular arcade
Right side, posterior view.
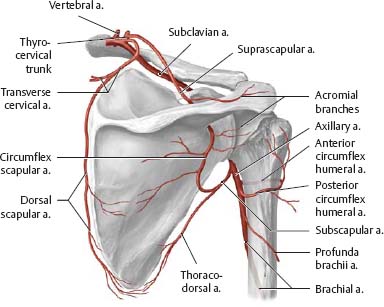
Fig. 22.4 Arteries of the forearm and hand
Right limb. The ulnar and radial arteries are interconnected by the superficial and deep palmar arches, the perforating branches, and the dorsal carpal network.

Veins & Lymphatics of the Upper Limb
Fig. 22.5 Veins of the upper limb
Right limb, anterior view.
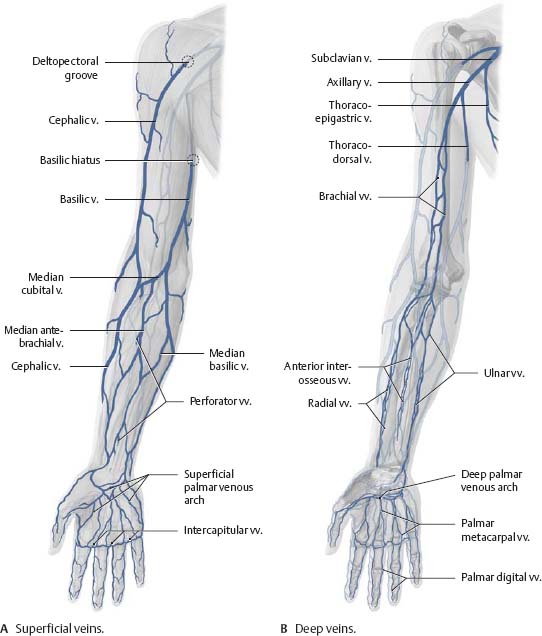
Fig. 22.6 Veins of the dorsum
Right hand, posterior view.

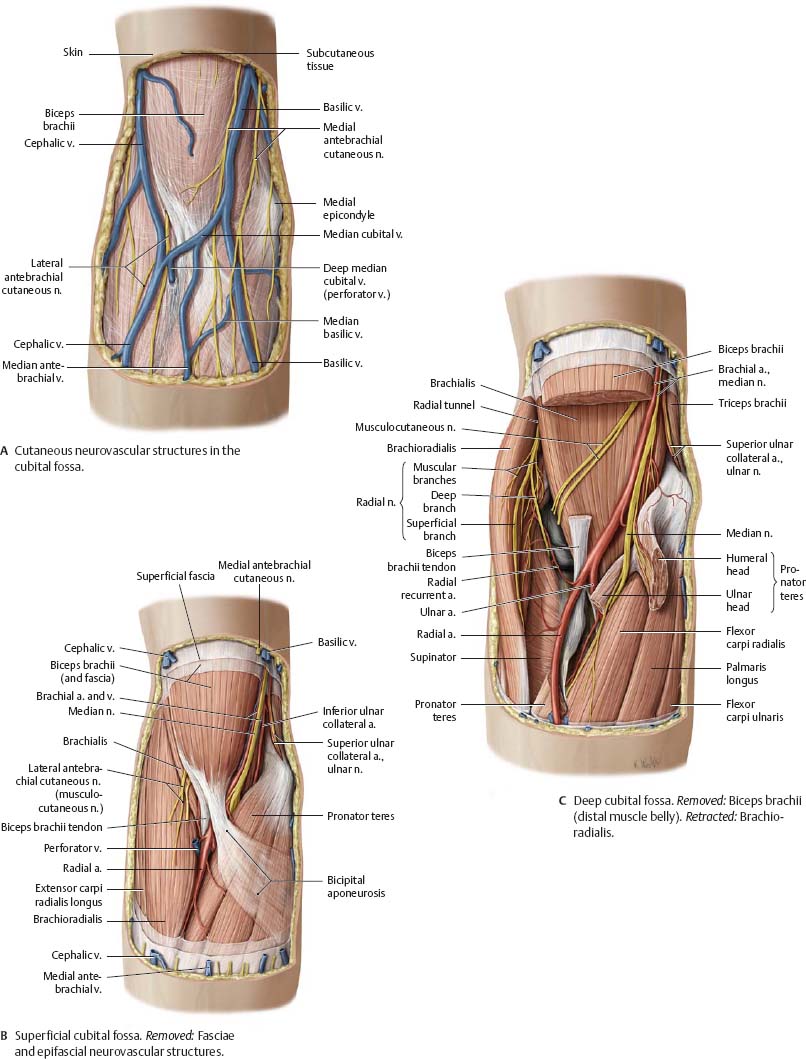
Fig. 22.7 Cubital fossa
Right limb, anterior view. The subcutaneous veins of the cubital fossa have a highly variable course.

![]() Clinical
Clinical
Venipuncture
The veins of the cubital fossa are frequently used when drawing blood. In preparation, a tourniquet is applied. This allows arterial blood to flow, but blocks the return of venous blood. The resulting swelling makes the veins more visible and palpable.
![]() Lymph from the upper limb and breast drains to the axillary lymph nodes. The superficial lymphatics of the upper limb lie in the subcutaneous tissue, while the deep lymphatics accompany the arteries and deep veins. Numerous anastomoses exist between the two systems.
Lymph from the upper limb and breast drains to the axillary lymph nodes. The superficial lymphatics of the upper limb lie in the subcutaneous tissue, while the deep lymphatics accompany the arteries and deep veins. Numerous anastomoses exist between the two systems.
Fig. 22.8 Lymph vessels of the upper limb
Right limb.

Fig. 22.9 Lymphatic drainage of the hand
Right hand, radial view. Most of the hand drains to the axillary nodes via cubital nodes. However, the thumb, index finger, and dorsumofthe hand drain directly.
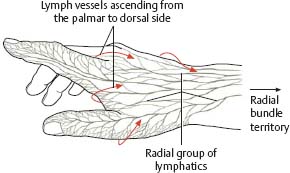
Fig. 22.10 Axillary lymph nodes
Right side, anterior view. The axillary lymph nodes are divided into three levels with respect to the pectoralis minor. They have major clinical importance in breast cancer (see p. 65).

Nerves of the Brachial Plexus
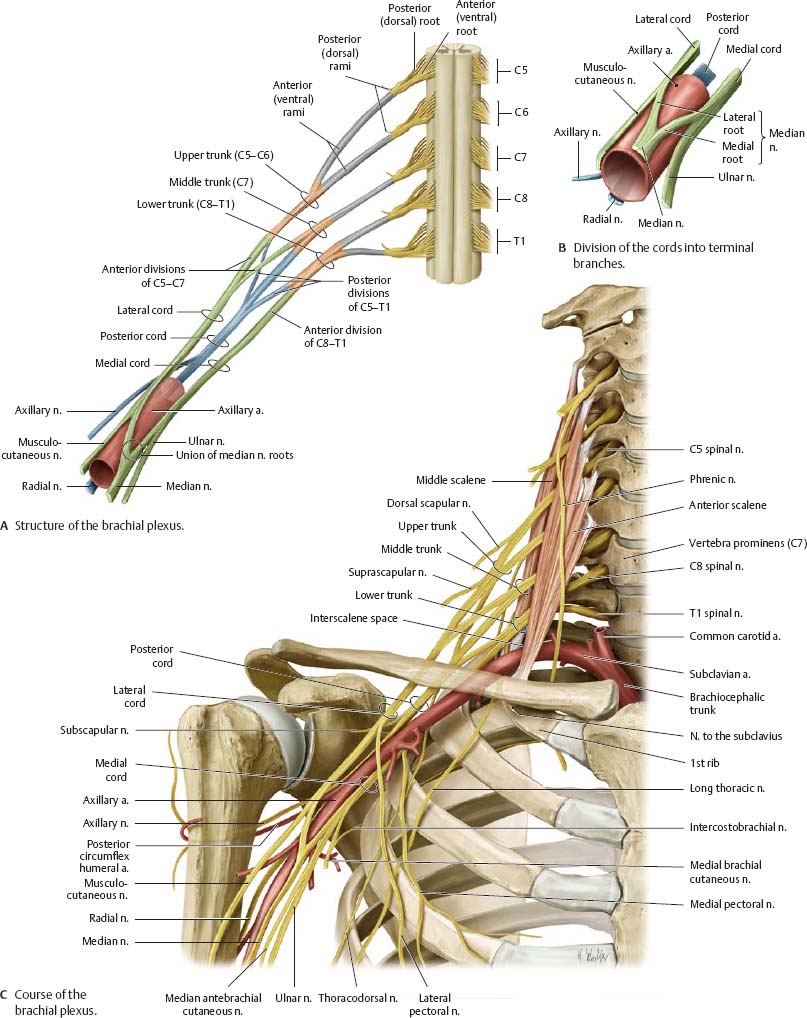
![]() Almost all muscles in the upper limb are innervated by the brachial plexus, which arises from spinal cord segments C5 to T1. The anterior rami of the spinal nerves give off direct branches (supraclavicular part of the brachial plexus) and merge to form three trunks, six divisions (three anterior and three posterior), and three cords. The infraclavicular part of the brachial plexus consists of short branches that arise directly from the cords and long (terminal) branches that traverse the limb.
Almost all muscles in the upper limb are innervated by the brachial plexus, which arises from spinal cord segments C5 to T1. The anterior rami of the spinal nerves give off direct branches (supraclavicular part of the brachial plexus) and merge to form three trunks, six divisions (three anterior and three posterior), and three cords. The infraclavicular part of the brachial plexus consists of short branches that arise directly from the cords and long (terminal) branches that traverse the limb.

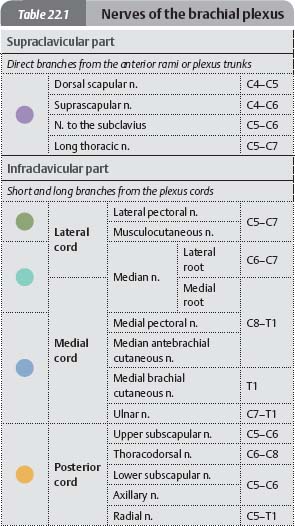
Fig. 22.11 Brachial plexus
Right side, anterior view.
Supraclavicular Branches & Posterior Cord
Fig. 22.12 Supraclavicular branches
Right shoulder.

![]() The supraclavicular branches of the brachial plexus arise directly from the plexus roots (anterior rami of the spinal nerves) orfrom the plexus trunks in the lateral cervical triangle.
The supraclavicular branches of the brachial plexus arise directly from the plexus roots (anterior rami of the spinal nerves) orfrom the plexus trunks in the lateral cervical triangle.
|
Table 22.2 Supraclavicular branches |
||
|
Nerve |
Level |
Innervated muscle |
|
Dorsal scapular n. |
C4–C5 |
Levator scapulae |
|
Suprascapular n. |
C4–C6 |
Supraspinatus |
|
Nerve to the subclavius |
C5–C6 |
Subclavius |
|
Long thoracic n. |
C5–C7 |
Serratus anterior |
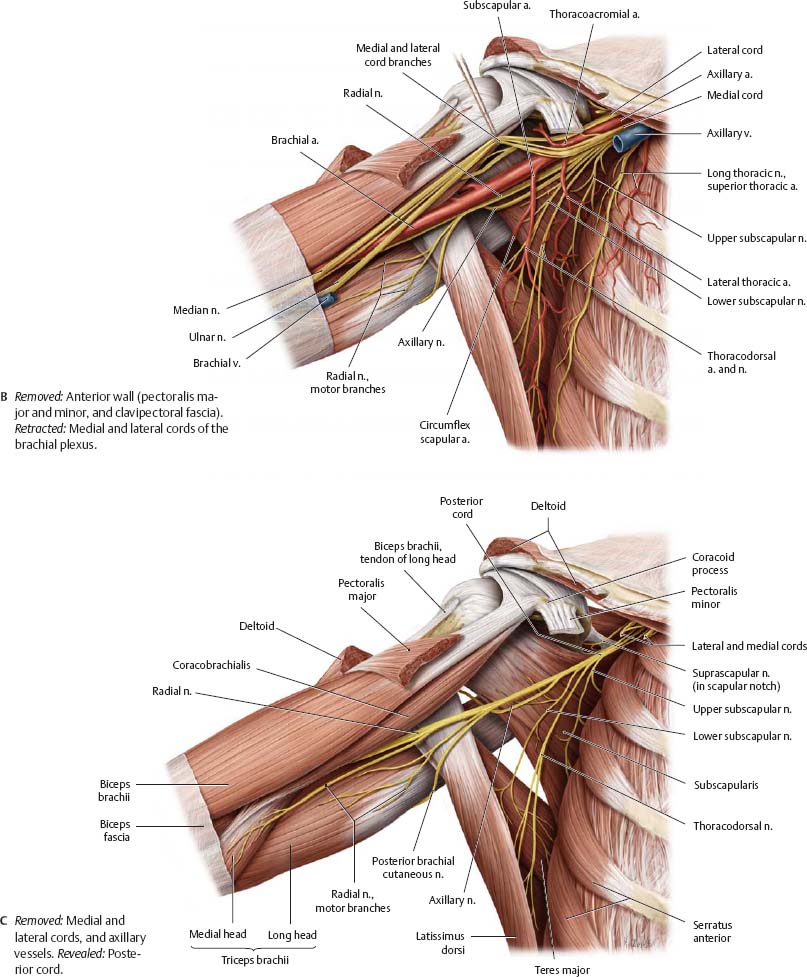
Fig. 22.13 Posterior cord: Short branches
Right shoulder.
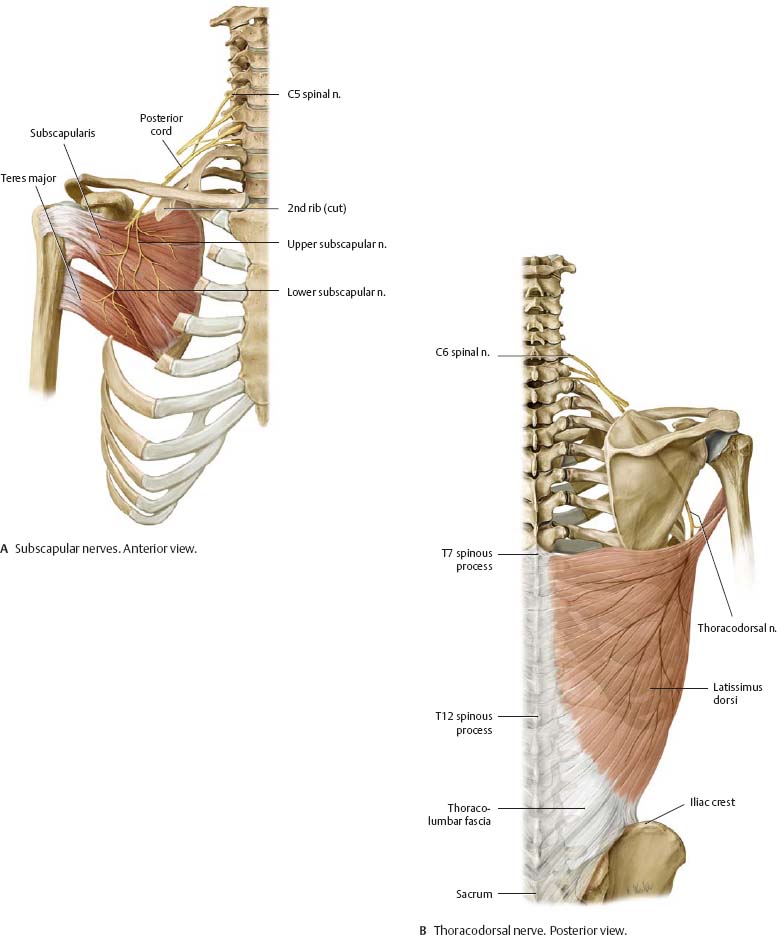
![]() The posterior cord gives off three short branches (arising at the level of the plexus cords) and two long branches (terminal nerves, see pp. 324–325).
The posterior cord gives off three short branches (arising at the level of the plexus cords) and two long branches (terminal nerves, see pp. 324–325).
|
Table 22.3 Branches of the posterior cord |
||
|
Nerve |
Level |
Innervated muscle |
|
Short branches |
||
|
Upper subscapular n. |
C5–C6 |
Subscapularis |
|
Lower subscapular n. |
Subscapularis Teres major |
|
|
Thoracodorsal n. |
C6–C8 |
Latissimus dorsi |
|
Long (terminal) branches |
||
|
Axillary n. |
C5–C6 |
Seep. 324 |
|
Radial n. |
C5–T1 |
Seep. 325 |
Posterior Cord: Axillary & Radial Nerves
Fig. 22.14 Axillary nerve: Sensory distribution
Right limb.
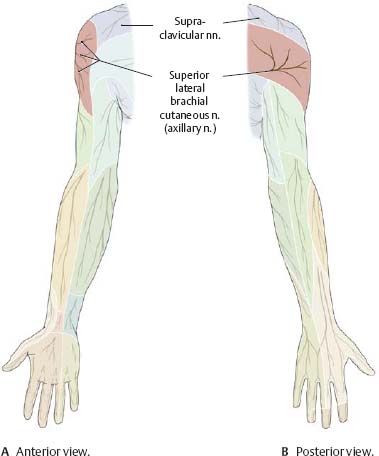
![]() Clinical
Clinical
The axillary nerve may be damaged in a fracture of the proximal humerus. This results in limited ability to abduct the arm, and may cause a loss of profile of the shoulder.
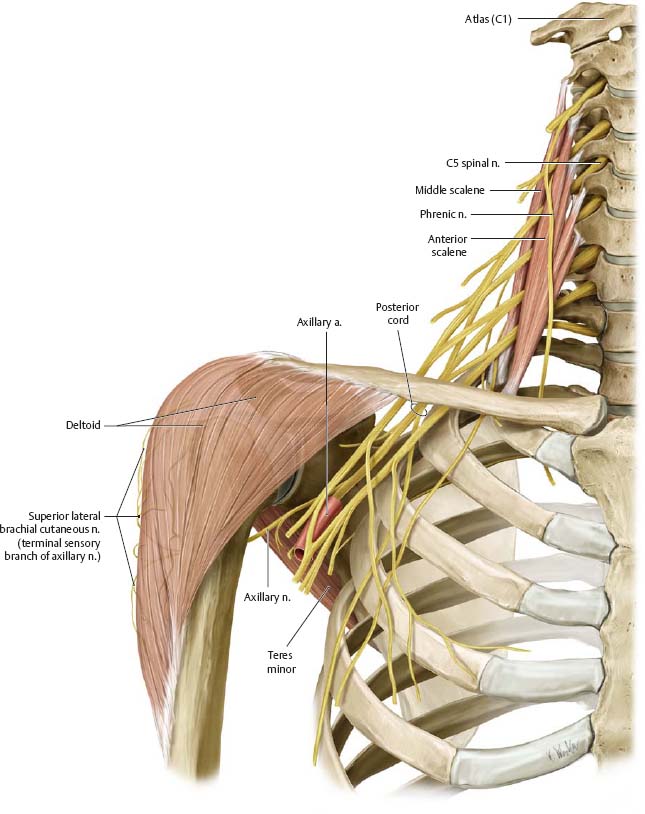
Fig. 22.15 Axillary nerve
Right side, anterior view.
|
Table 22.4 Axillary nerve (C5–C6) |
|
|
Motor branches |
Innervated muscles |
|
Muscular branches |
Deltoid |
|
Sensory branch |
|
|
Superior lateral cutaneous n. |
|
Fig. 22.16 Radial nerve: Sensory distribution

|
Table 22.5 Radial nerve (C5–T1) |
|
|
Motor branches |
Innervated muscles |
|
Muscular branches |
Brachialis (partial) |
|
Triceps brachii |
|
|
Anconeus |
|
|
Brachioradialis |
|
|
Extensors carpi radialis longus and brevis |
|
|
Deep branch (terminal branch: posterior interosseous n.) |
Supinator |
|
Extensor digitorum |
|
|
Extensor digiti minimi |
|
|
Extensor carpi ulnaris |
|
|
Extensors pollicis brevis and longus |
|
|
Extensor indicis |
|
|
Abductor pollicis longus |
|
|
Sensory branches |
|
|
Articular branches from radial n.: Capsule of the shoulder joint |
|
|
Articular branches from posterior interosseousn.: Joint capsule of the wrist and four radial metacarpophalangeal joints |
|
|
Posterior brachial cutaneous n. |
|
|
Inferior lateral brachial cutaneous n. |
|
|
Posterior antebrachial cutaneous n. |
|
|
Superficial branches |
Dorsal digital nn. |
|
Ulnar communicating branch |
|
Fig. 22.17 Radial nerve
Right limb, anteriorviewwith forearm pronated.
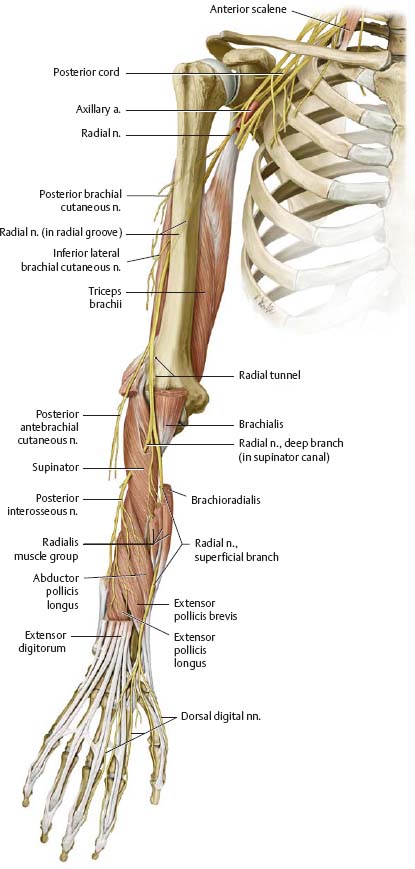
![]() Clinical
Clinical
Chronic radial nerve compression in the axilla (e.g., due to extended/ improper crutch use) may cause loss of sensation or motor function in the hand, forearm, and posterior arm. More distal injuries (e.g., during anesthesia) affect fewer muscles, potentially resulting in wrist drop with intact triceps brachii function.
Medial & Lateral Cords
![]() The medial and lateral cords give off four short branches. The intercostobrachial nerves are included with the short branches of the brachial plexus, although they are actually the cutaneous branches of the 2nd and 3rd intercostal nerves.
The medial and lateral cords give off four short branches. The intercostobrachial nerves are included with the short branches of the brachial plexus, although they are actually the cutaneous branches of the 2nd and 3rd intercostal nerves.

Fig. 22.18 Medial and lateral cords: Short branches
Right side, anterior view.
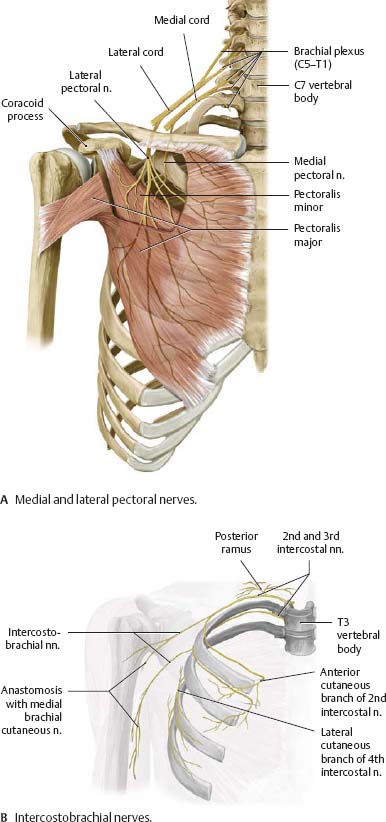
Fig. 22.19 Short branches: Sensory distribution
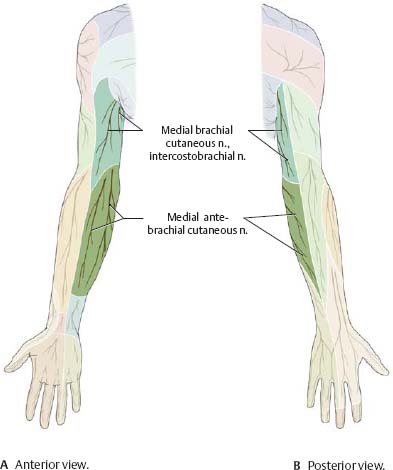
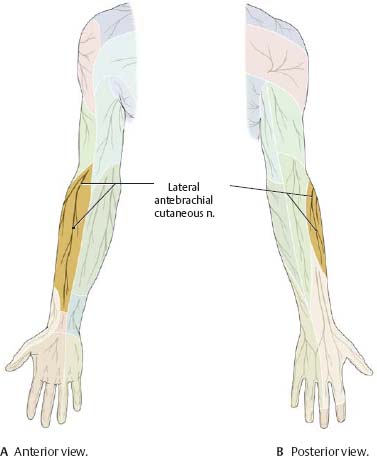
Fig. 22.20 Musculocutaneous nerve
Right limb, anterior view.

|
Table 22.7 Musculocutaneous nerve(C5–C7) |
|
|
Motor branches |
Innervated muscles |
|
Muscular branches |
Coracobrachialis |
|
Biceps brachii |
|
|
Brachialis |
|
|
Sensory branches |
|
|
Lateral antebrachial cutaneous n. |
|
|
Articular branches: Joint capsule of the elbow (anterior part) |
|
|
Note: Musculocutaneous nerve innervation of the arm is purely motor; innervation of the forearm is purely sensory. |
|
Fig. 22.21 Musculocutaneous nerve: Sensory distribution
Median & Ulnar Nerves
![]() The median nerve is a terminal branch arising from both the medial and lateral cords. The ulnar nerve arises exclusively from the medial cord.
The median nerve is a terminal branch arising from both the medial and lateral cords. The ulnar nerve arises exclusively from the medial cord.
Fig. 22.22 Median nerve
Right limb, anterior view.

![]() Clinical
Clinical
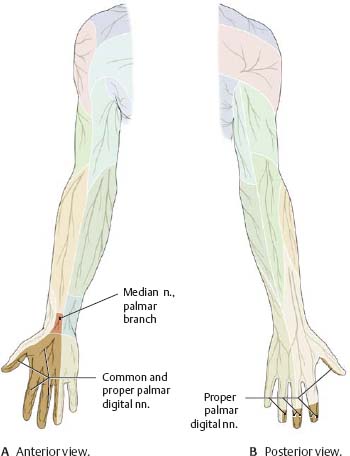
Median nerve injury caused by fracture/ dislocation of the elbow joint may result in compromised grasping ability and sensory loss in the fingertips (see Fig. 22.23 forterritories). See also carpal tunnel syndrome (p. 343).
Fig. 22.23 Median nerve: Sensory distribution
|
Table 22.8 Median nerve (C6–T1) |
|
|
Motor branches |
Innervated muscles |
|
Direct muscular branches |
Pronator teres |
|
Flexor carpi radialis |
|
|
Palmaris longus |
|
|
Flexor digitorum superficialis |
|
|
Muscular branches Pronator from anterior antebrachial Interosseous n. |
Pronator quadratus |
|
Flexor pollicis longus |
|
|
Flexor digitorum profundus (radial half) |
|
|
Thenar muscular branch |
Abductor pollicis brevis |
|
Flexor pollicis brevis (superficial head) |
|
|
Opponens pollicis |
|
|
Muscular branches from common palmar digital nn. |
1st and 2nd lumbricals |
|
Sensory branches |
|
|
Articular branches: Capsules of the elbow and wrist joints |
|
|
Palmar branch of median n. (thenar eminence) |
|
|
Communicating branch to ulnar n. |
|
|
Common palmar digital nn. |
|
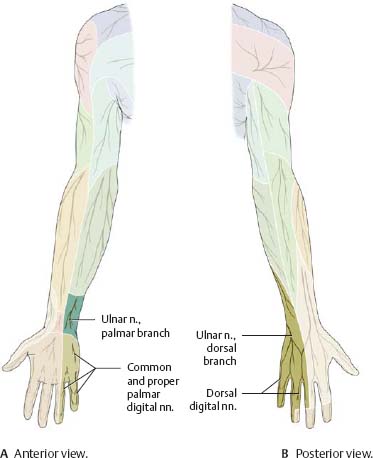
Fig. 22.24 Ulnar nerve: Sensory distribution
|
Table 22.9 Ulnar nerve (C7–T1) |
|
|
Motor branches |
Innervated muscles |
|
Direct muscular branches |
Flexor carpl ulnaris |
|
Flexor digitorum profundus (ulnar half) |
|
|
Muscular branch from superior ulnar n. |
Palmaris brevis |
|
Muscular branches from deep ulnar n. |
Abductor digiti miniml |
|
Flexor digiti minimi |
|
|
Opponens digiti miniml |
|
|
3 rd and 4th lumbricals |
|
|
Palmar and dorsal interosseous muscles |
|
|
Adductor policis |
|
|
Flexor policis brevis (deep head) |
|
|
Sensory branches |
|
|
Articular branches: Capsules of the elbow, carpal, and metacarpophalangeal joints |
|
|
Dorsal branch (terminal branches: dorsal digital nn.) |
|
|
Palmar branch |
|
|
Proper palmar digital n. (from superficial branch |
|
|
Common palmar digital n. (from superficial branch; terminal braches; proper palmar digital nn.) |
|
Fig. 22.25 Ulnar nerve
Right limb, anteriorview.
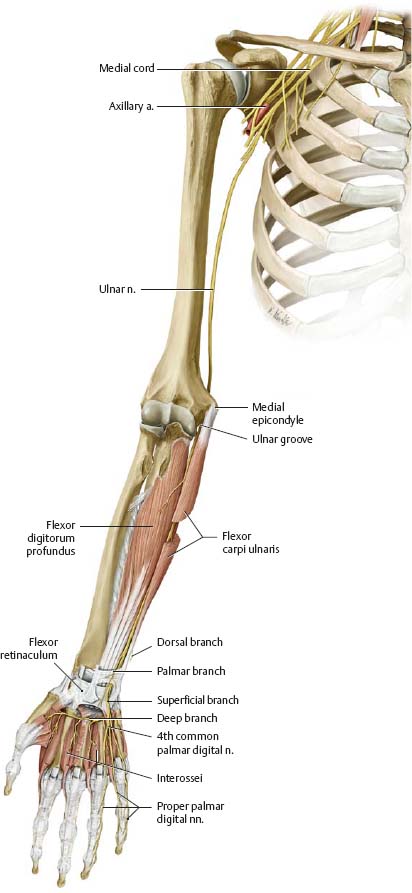
![]() Clinical
Clinical
Ulnar nerve palsy is the most common peripheral nerve damage. The ulnar nerve is most vulnerable to trauma or chronic compression in the elbow joint and ulnar tunnel (see p. 343). Nerve damage causes "clawing" of the hand and atrophy of the interossei. Sensory losses are often limited to the 5th digit.
Superficial Veins & Nerves of the Upper Limb
Fig. 22.26 Cutaneous innervation of the upper limb: Anterior view
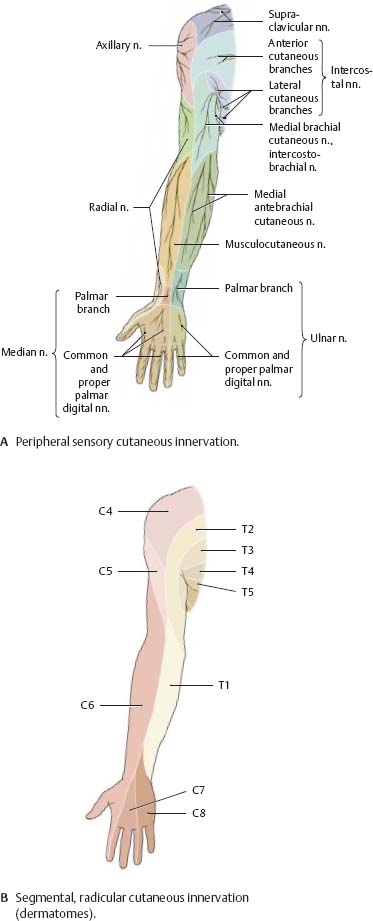
Fig. 22.27 Superficial cutaneous veins and nerves of the upper limb
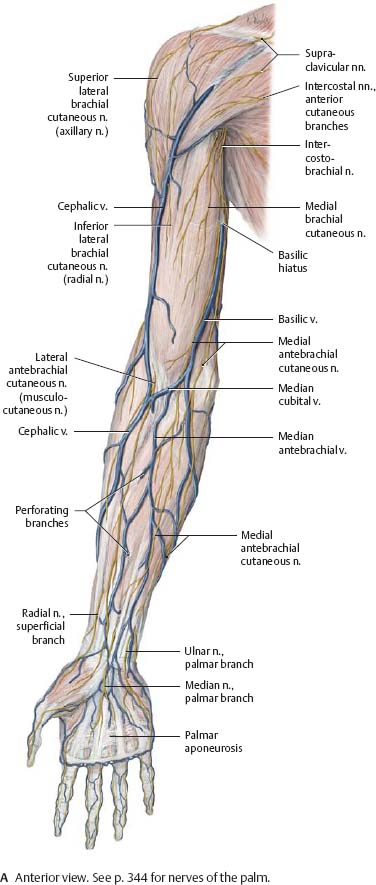
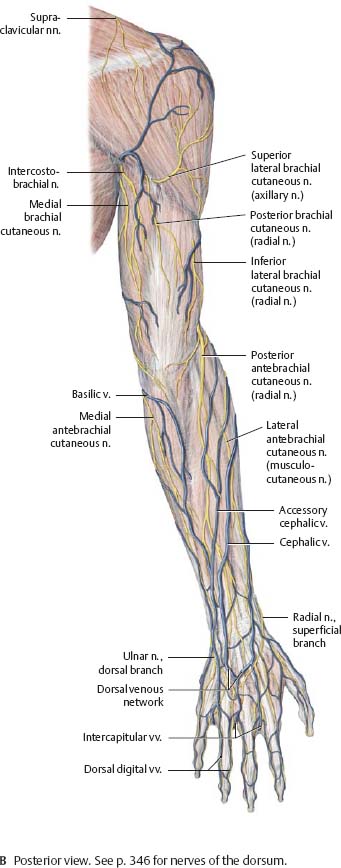
Fig. 22.28 Cutaneous innervation of the upper limb: Posterior view

Posterior Shoulder & Axilla
Fig. 22.29 Posterior shoulder
Right shoulder, posterior view. Ro/sed:Trapezius (transverse part). Windowed: Supraspinatus. Revealed: Suprascapular region.
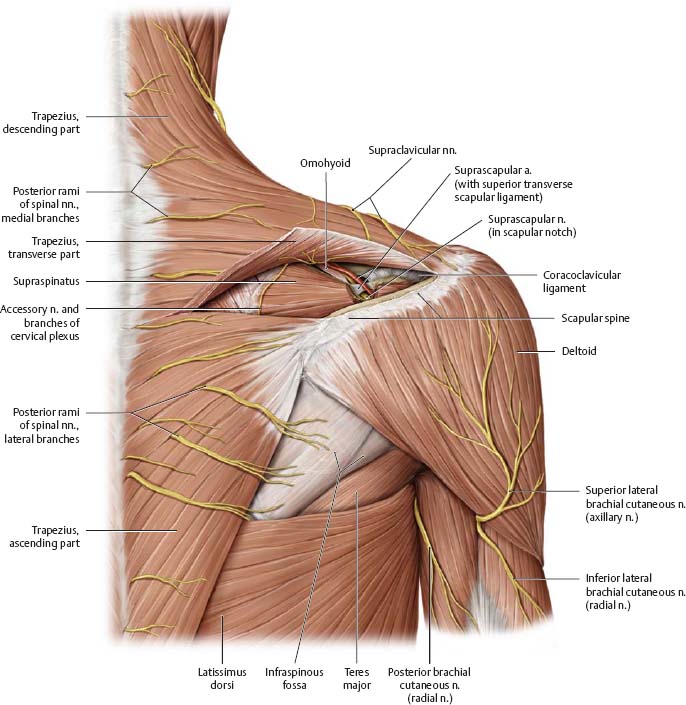

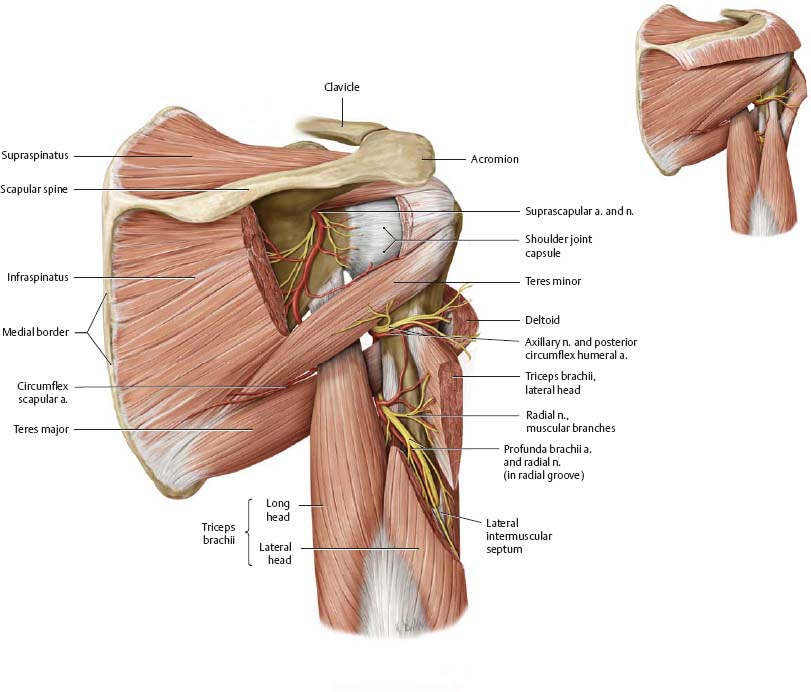
Fig. 22.30 Axilla: Triangular and quadrangular spaces
Right shoulder, posterior view.
Anterior Shoulder
Fig. 22.31 Anterior shoulder: Superficial dissection
Right shoulder.
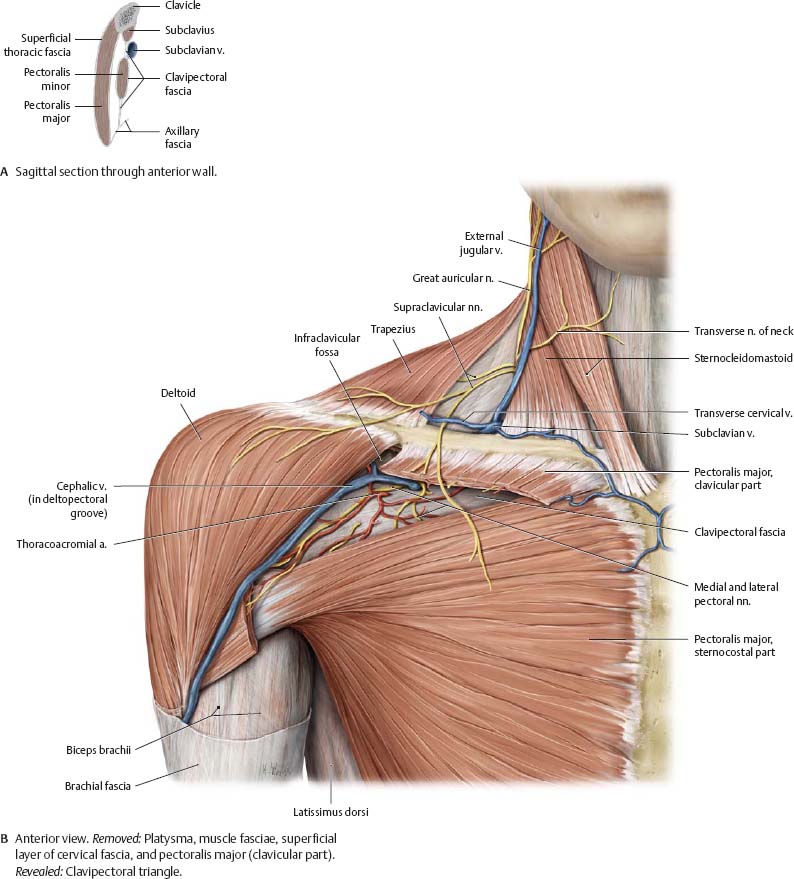
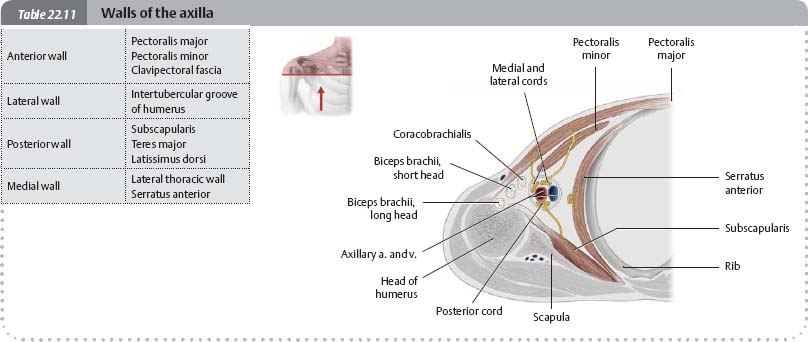
Fig. 22.32 Shoulder: Transverse section
Right shoulder, inferior view.

Fig. 22.33 Anterior shoulder: Deep dissection
Right limb, anterior view. Removed: Sternocleidomastoid, omohyoid, and pectoralis major. This dissection reveals the neurovascular contents of the lateral cervical triangle (see pp. 580–581) and axilla (seepp. 336–337).
Topography of the Axilla
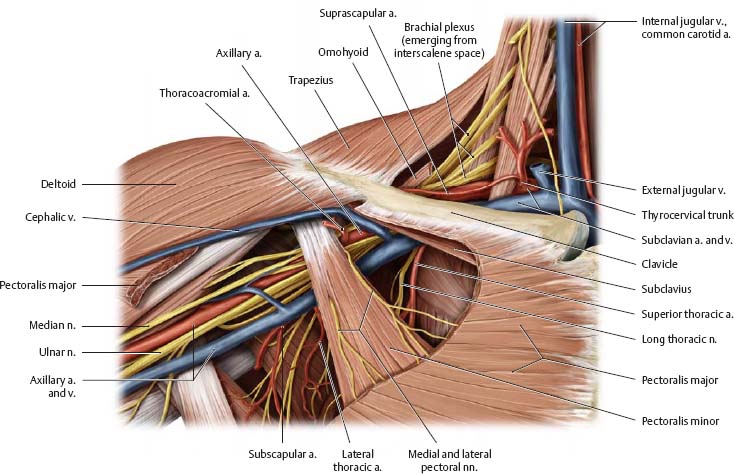
Fig. 22.34 Dissection of the axilla
Right shoulder, anterior view.

Topography of the Brachial & Cubital Regions
Fig. 22.35 Brachial region
Right arm, anterior view. Removed: Deltoid, pectoralis major and minor. Revealed: Medial bicipital groove.

Fig. 22.36 Cubital region
Right elbow, anterior view.
Topography of the Forearm
Fig. 22.37 Anterior forearm
Right forearm, anterior view.
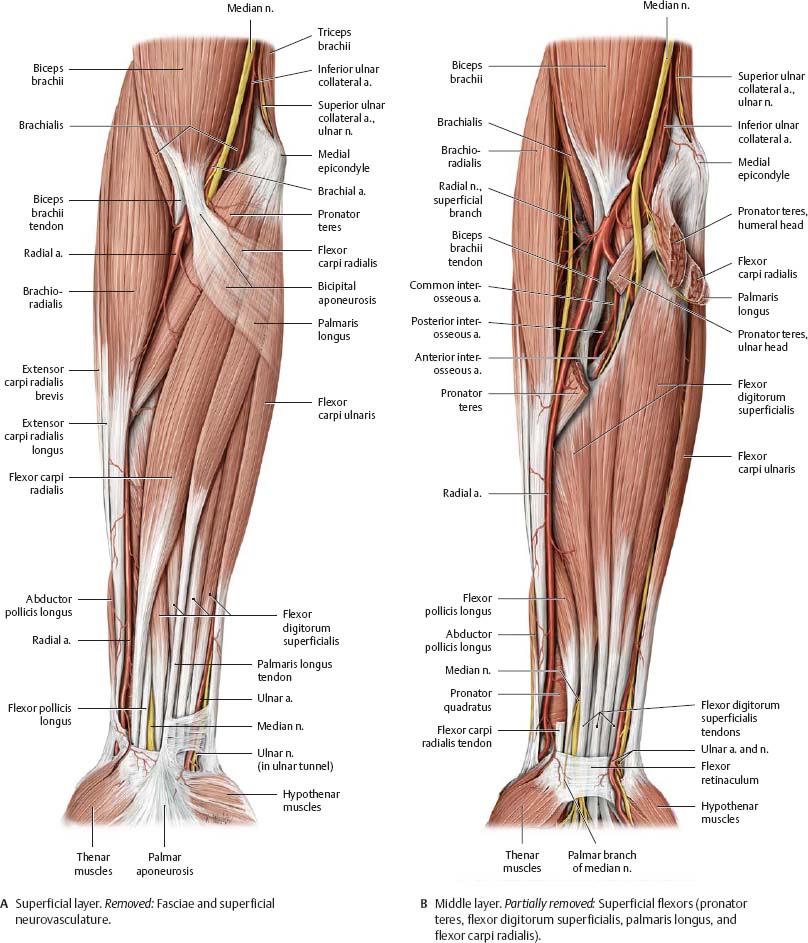
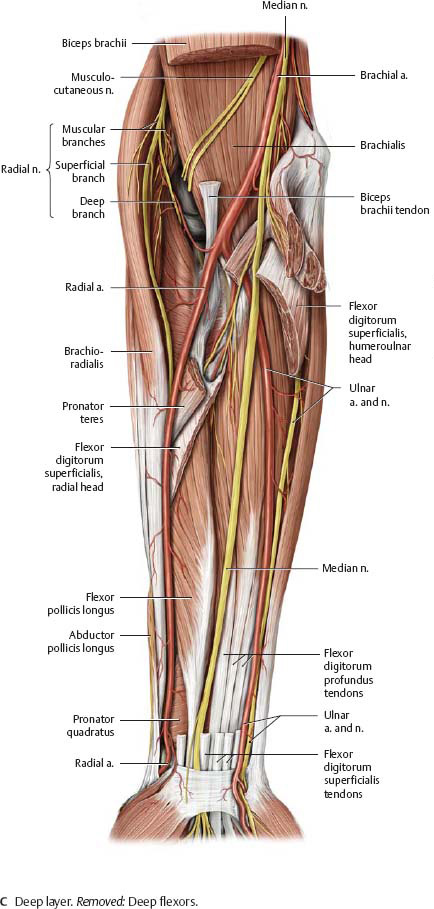
Fig. 22.38 Posterior forearm
Right forearm, anterior view during pronation. Reflected: Anconeus and triceps brachii. Resected: Extensor carpi ulnaris and extensor digitorum.

Topography of the Carpal Region
Fig. 22.39 Anterior carpal region
Right hand, anterior (palmar) view.
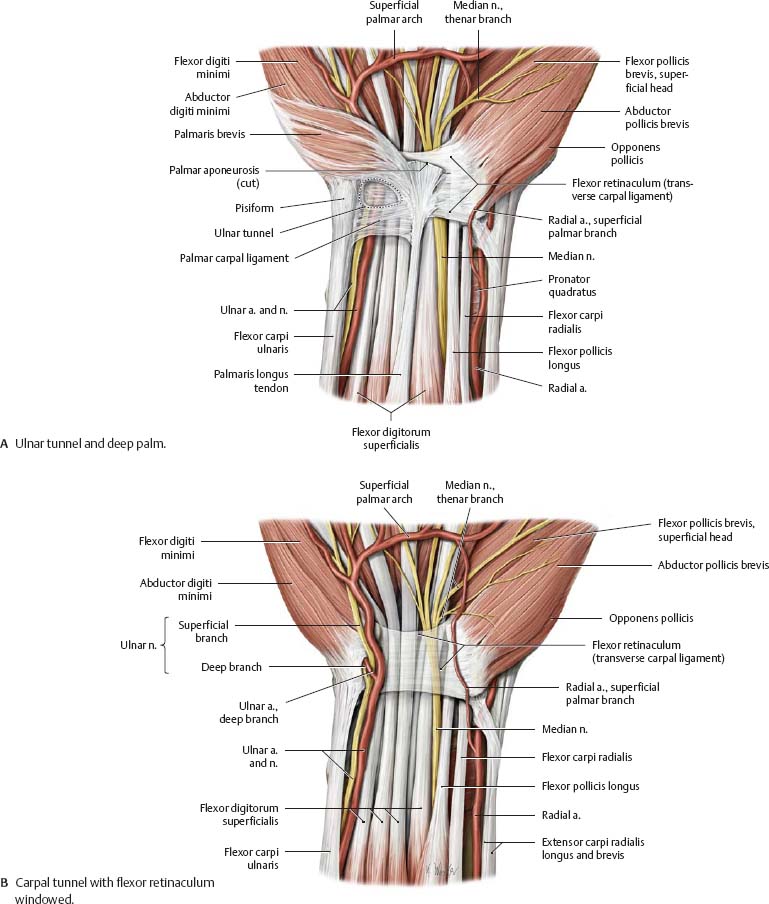
Fig. 22.40 Ulnar tunnel
Right hand, anterior (palmar) view.
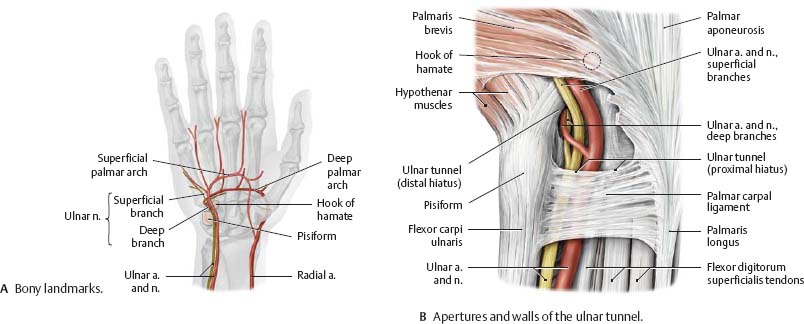
Fig. 22.41 Carpal tunnel: Cross section
Right hand, proximal view. The tight fit of sensitive neurovascular structures with closely apposed, frequently moving tendons in the carpal tunnel often causes problems (carpal tunnel syndrome) when any of the structures swell or degenerate.

Topography of the Palm of the Hand
Fig. 22.42 Superficial neurovascular structures of the palm
Right hand, anteriorview.
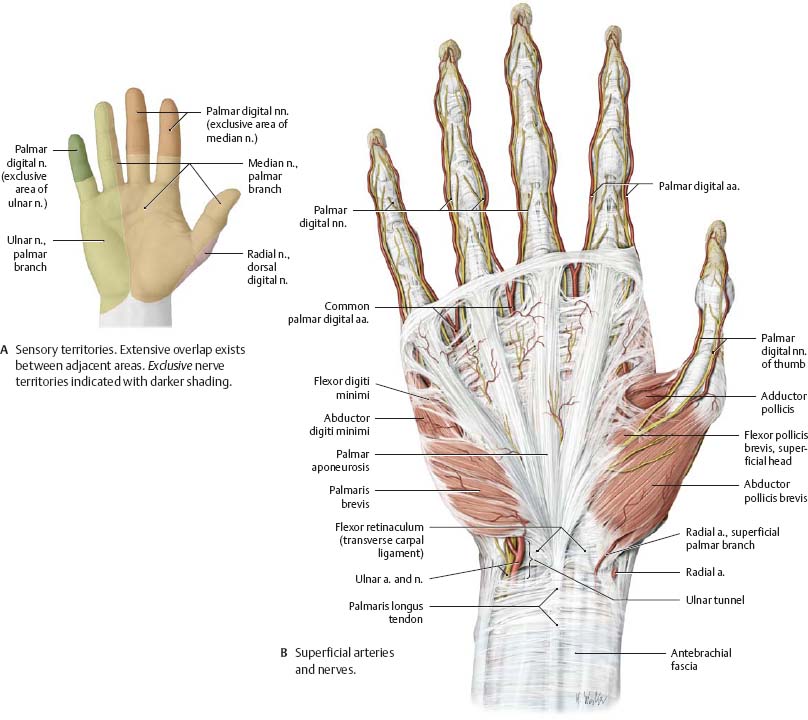
Fig. 22.43 Neurovasculature of the finger
Right middle finger, lateral view.
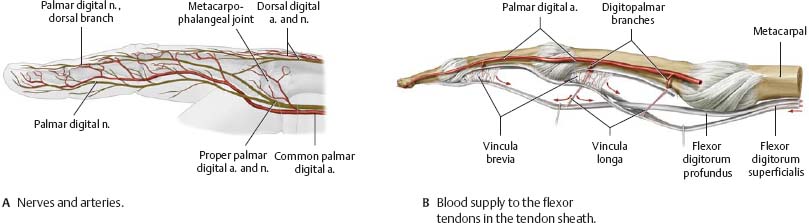
Fig. 22.44 Deep neuro-vascular structures of the palm
Right hand, anterior view.

Fig. 22.45 Innervation patterns in the palm
Right hand, anterior view.

Topography of the Dorsum of the Hand
Fig. 22.46 Sensory innervation of the dorsum
Right hand, posterior view.

Fig. 22.47 Anatomic snuffbox
Right hand, radial view. The three-sided "anatomic snuffbox" is bounded by the tendons of insertion of the abductor pollicis longus and extensors pollicis brevis and longus.
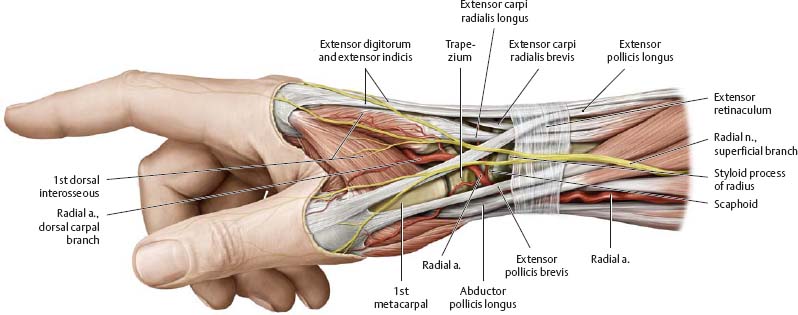
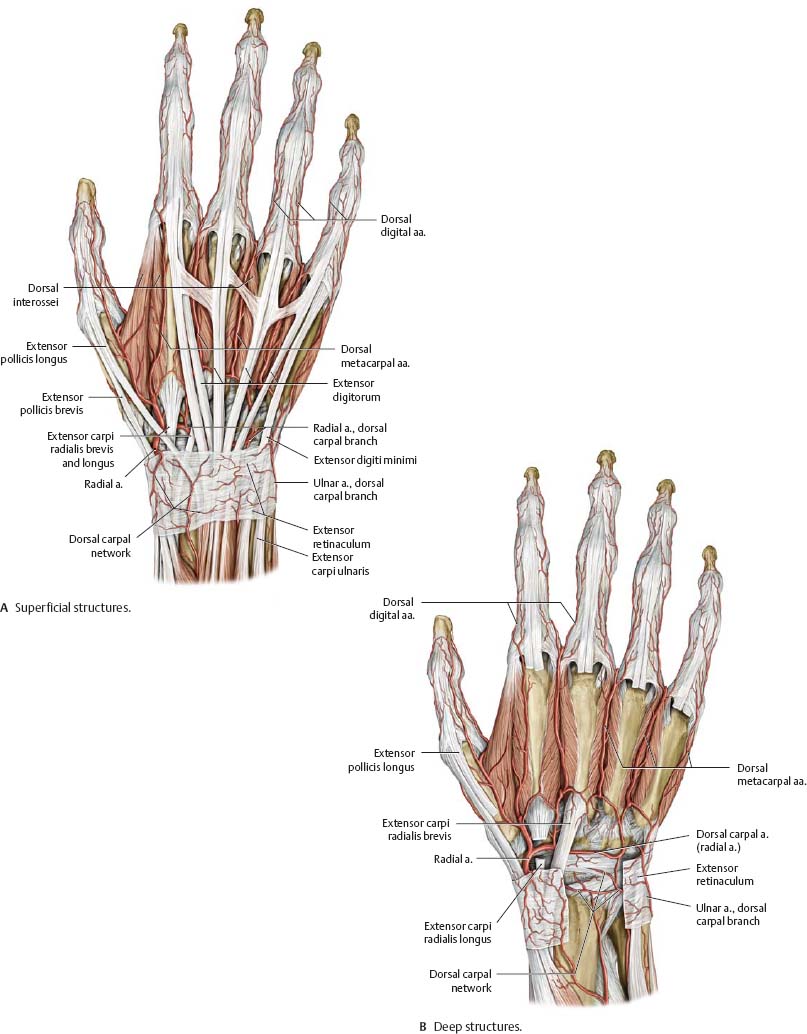
Fig. 22.48 Neurovascular structures of the dorsum
Transverse Sections
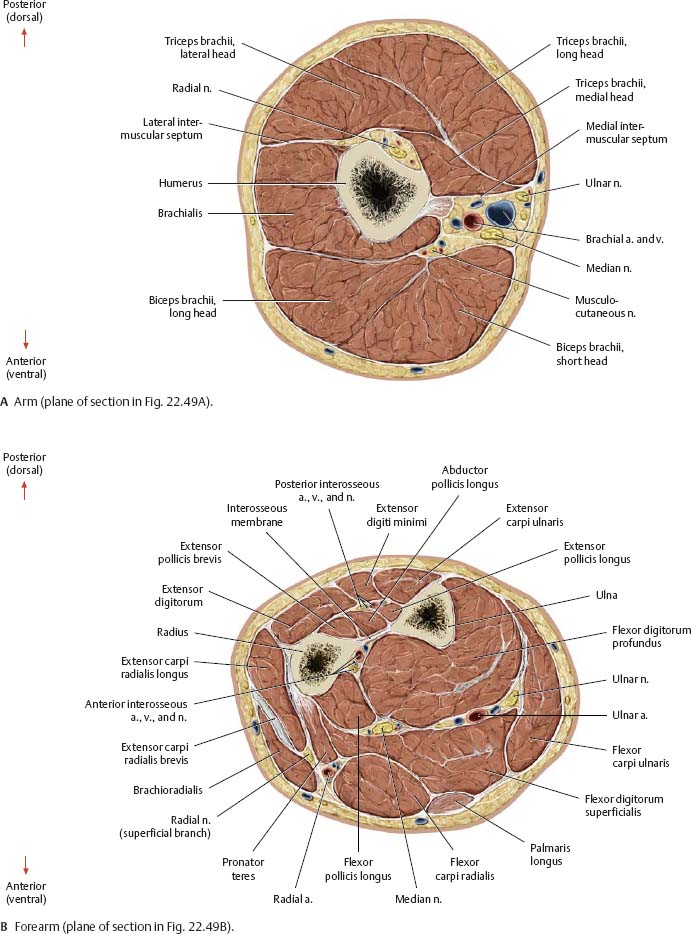
Fig. 22.49 Windowed dissection
Right limb, anterior view.
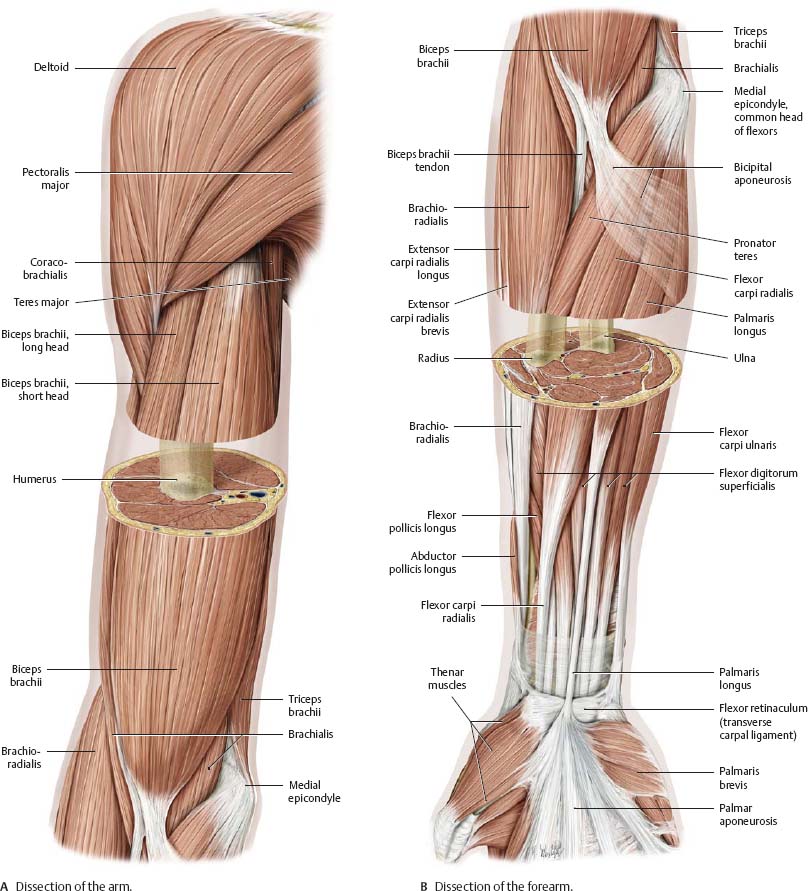
Fig. 22.50 Transverse sections
Right limb, proximal (superior) view.