Michael A. Cole and Sukhjit S. Takhar
Gastrointestinal (GI) bleeding is a common emergency, with a prevalence of 170 cases per 100,000 adults per year in America. In the majority of cases, the source is the upper GI tract, and the mortality from upper GI bleeding (UGIB) has remained at approximately 6% to 8% for three decades (1). Patients with GI hemorrhage often have coexisting serious illnesses, making their care even more challenging. The site of bleeding is usually predictable from the history and physical examination and is often confirmed and treated by endoscopy. Although there have been many advances in care, the fundamental goals of resuscitation and hemostasis remain the same.
UGIB is defined as a source of bleeding originating between the upper esophageal sphincter and the ligament of Treitz. Although peptic ulcer disease is the cause of more than 60% of UGIB cases, the highest mortality rates are associated with variceal bleeding. Due to the potential severity and unique pathophysiology and treatment of variceal bleeding, it is useful to divide UGIB into variceal and nonvariceal bleeding (1,2).
Causes of UGIB are listed in Table 99.1. UGIB may occur at any age but has a higher incidence in patients older than 40 years. It is more common in males than females. Elderly patients have less ability to compensate for acute hemorrhage and the majority of deaths occur in this subgroup. Mortality is also higher in those with multiple comorbidities (3,4).
TABLE 99.1
Causes of Upper Gastrointestinal Tract Bleeding

CLINICAL PRESENTATION
Patients present with a variety of GI symptoms, such as nausea, vomiting, and abdominal pain, as well as symptoms of acute blood loss, such as lightheadedness or syncope. UGIB classically presents with hematemesis and melena. Bright-red emesis suggests fresh blood with significant, ongoing hemorrhage. Both coffee-ground emesis and melenic stools signify a more subacute to chronic UGIB. Experienced clinicians sometimes make a presumptive diagnosis of UGIB based on the unique odor of melenic stool. Hematochezia is usually a result of lower GI hemorrhage but may occur in those with a massive UGIB and rapid GI transit (2,5,6). Furthermore, some patients with melena may have a lower GI source for their bleeding (7).
UGIB can result in varying degrees of blood loss, ranging from trivial, occult bleeding to fatal exsanguination. Patients may have underlying comorbid conditions that can complicate the interpretation of the vital signs. Hypovolemic patients often complain of thirst, apprehension, weakness, or lightheadedness. When reflex mechanisms can no longer fully compensate for volume loss, hypotension develops and organ perfusion is impaired. This can result in oliguria, altered mentation, metabolic acidosis, and dyspnea. Some patients may not recognize that a black stool is a sign of bleeding. Melena must also be differentiated from black stools due to iron or bismuth, which do not have the tarry consistency and are guaiac-negative.
DIFFERENTIAL DIAGNOSIS
If the clinician can appropriately categorize the bleeding as having an upper or lower source, the differential may be more focused. However, it is not always possible to establish the location of bleeding in the ED. The appearance of the stool is often helpful but is sometimes misleading. In one study, the ingestion of 1000 mL of blood led to hematochezia, demonstrating that an upper rather than lower source may be the cause of hematochezia (8). Conversely, melena may be produced by as little as 50 mL of blood from an upper GI source (9).
The most frequent cause of UGIB is peptic ulcer disease. Hemorrhage results from erosion into an underlying vascular structure. Predisposing factors for peptic ulcers include cigarette smoking, ingestion of alcohol, nonsteroidal anti-inflammatory (NSAID) use, hereditary factors, and colonization with Helicobacter pylori (10,11). The rate of hemorrhage from peptic ulcer disease appears to be decreasing in the United States, possibly due to increased use of proton pump inhibitors (PPIs) and treatment for H. pylori (11).
Erosive gastritis is also a common cause of UGIB. The resultant bleeding can range from minimal to life-threatening, and the clinical presentation is often indistinguishable from that of a peptic ulcer. The most common predisposing factor is the use of NSAIDs. Other risk factors include use of alcohol, prolonged corticosteroid use, age, major trauma, burns, or head injury.
Esophageal and gastric varices are two of the most dangerous causes of UGIB. Varices should be suspected in patients with a history of cirrhosis or with other stigmata of liver disease. The presence of hepatic dysfunction and other comorbidities further worsens the prognosis. Bleeding can be sudden and massive and is associated with an acute mortality rate between 15% and 53%. Patients with variceal hemorrhage also have a poor long-term prognosis, with a projected 1-year mortality of 70% (12).
Mallory–Weiss tears are longitudinal, nontransmural tears that occur at the gastroesophageal junction and are usually caused by recurrent forceful vomiting or retching. The history of sudden vomiting of bright-red blood after retching is characteristic, but this history is present in only one-half of patients with Mallory–Weiss tears. Risk factors include alcohol abuse, hiatal hernia, and underlying esophagitis. Bleeding usually stops spontaneously, and intervention is rarely required. Mallory–Weiss tears are differentiated from Boerhaave syndrome, which is a transmural tear of the esophagus that typically presents as chest pain, odynophagia, and pneumomediastinum without GI bleeding.
Other, less common conditions account for the remaining 10% of episodes of UGIB (see Table 99.1). Aortoenteric fistula occurs when an aortic aneurysm or a synthetic graft erodes into the small intestine, producing massive hemorrhage. Aortoenteric fistulas can occur within weeks to many years after the initial aneurysm repair, with one study reporting an average of 2.8 years (13).
Patients with small intestinal angiodysplasias may present with melena. This diagnosis is usually made on a small bowel examination after upper and lower endoscopies are negative.
ED EVALUATION
The first priority should be to identify and treat patients who are hemodynamically unstable. This assessment should start with the initial triage or in the prehospital setting. The goal is to rapidly assess the severity and location of bleeding and to determine whether the patient may have variceal bleeding.
Medications and allergies should be noted, with an emphasis on NSAIDs, acetylsalicylic acid, and anticoagulants. Patients who are anticoagulated have more severe bleeding and a higher mortality (3,11,14,15). Use of iron products or bismuth (Pepto-Bismol) should be noted, as their use may mimic melena. Severe abdominal pain is unusual, as many causes of UGIB are painless. The review of systems should include symptoms consistent with hypovolemia (e.g., chest pain, dyspnea, light-headedness, or syncope). Those with a history of cirrhosis or alcoholism should be assumed to have variceal bleeding (14,16).
The physical examination should focus on finding evidence of bleeding and attempting to localize and quantify the blood loss. Hypotension may not be present until 30% to 40% of the circulating blood volume has been lost, though orthostatic changes occur with more modest losses. In an adult, a supine systolic blood pressure of <100 mm Hg, or an orthostatic pulse increase of >20 to 30 beats per minute, suggests an acute blood loss of at least 1 L. However, orthostatic vital signs are not reliable, especially at the extremes of age. Although tachycardia is usually present after acute blood loss, it is not a reliable finding. Flat neck veins; cold, mottled extremities; altered mental status; or pallor are all suggestive of significant acute blood loss.
The nose and oropharynx should also be examined for potential bleeding sources. Stigmata of chronic liver disease ( jaundice, ascites, and spider angiomata) are concerning for variceal bleeding. Ecchymosis, gingival bleeding, and epistaxis suggest a coagulopathy or platelet deficit.
Digital rectal examination and stool appearance are important parts of the early evaluation. The presence of gross blood should be noted. Not all black stool is melena, so it should be tested to confirm the presence of blood. Abdominal tenderness can be associated with perforated peptic ulcer or gastritis.
Initial laboratory evaluation should include a complete blood count, electrolyte panel, blood urea nitrogen (BUN), creatinine levels, liver function tests, and coagulation studies. Unless the bleeding seems minimal, patients should also have a type and screen or crossmatch for blood. An elevated BUN is often seen in the setting of a UGIB, and a BUN-to-creatinine ratio of >30 increases the likelihood of UGIB (17,18). The hemoglobin and hematocrit can be normal immediately after massive blood loss. Elderly patients should be evaluated for myocardial ischemia. A chest radiograph is indicated if aspiration, esophageal rupture, or cardiopulmonary complications are suspected. Abdominal films may be helpful in the subset of patients with suspected perforation or bowel obstruction, but computed tomography scan is more definitive.
The placement of a nasogastric (NG) tube may be considered in select patients with UGIB; however, routine placement is controversial (1,11,19). NG tube placement has been reported to be one of the most painful procedures performed in the ED (20). More importantly, a negative aspirate does not rule out a significant source of bleeding. NG placement may provoke vomiting, and aspiration and a recent study demonstrates that NG tube placement does not decrease mortality or the length of stay in a hospital (17,21,22). The poor sensitivity and specificity of an NG tube aspirate has been well described (1). In patients with melena but no hematemesis, the finding of fresh blood may be useful, but this information comes at the expense of significant discomfort to the patient (19). The early use of endoscopy can provide much more information. NG aspiration also misses up to 25% of bleeding duodenal ulcers, because it does not reliably sample material past the pylorus. Thus, making disposition decisions based on a negative aspirate is risky. Of note, varices are not a contraindication to NG tube placement.
KEY TESTING
• CBC, platelets, coagulation studies, type, and screen
• Stool guaiac test
ED MANAGEMENT
Initial resuscitation efforts should be guided by the estimated severity of bleeding. Patients with significant bleeding should be placed on a cardiac monitor, receive supplemental oxygen, and have intravenous access established with two large-bore catheters. Close attention to airway, breathing, and circulation is paramount. Critically ill patients, those with massive bleeding or altered mental status, usually need endotracheal intubation (2,5).
Intravenous fluid resuscitation to maintain blood pressure is essential. If the patient’s condition has not substantially improved after IV fluids and ongoing hemorrhage is suspected, blood transfusion is indicated. Crossmatched blood is preferred, but those in extremis may require type-specific or type O blood. The appropriate transfusion thresholds and targets during emergency care have not been established, and in acute hemorrhage, hemoglobin values can be misleading since compensatory hemodilution may lag by several hours. A normal hemoglobin concentration thus does not exclude an acute massive hemorrhage. After admission, a restrictive approach involving blood transfusion below hemoglobin levels of 7 g per dL improves clinical outcomes, although this benefit has not been demonstrated in the emergency setting (23). The decision to transfuse should also take into account the patient’s symptoms and hemodynamics, and the physician’s estimate of ongoing blood loss. Warmed blood should be used in patients who require massive transfusion, and if a large number of packed red blood cells (PRBCs) have been transfused one may consider initiating a “massive transfusion protocol” involving administration of blood, platelets, and fresh frozen plasma (FFP) in a 1:1:1 ratio. Massive transfusion protocols may help prevent the dilutional coagulopathy that results from the administration of large quantities of packed red blood cells, although evidence for improved outcomes in UGIB is lacking.
Coagulopathy and thrombocytopenia should be corrected as needed. Current recommendations are to resuscitate with FFP until the patient reaches an INR <2.7 and to maintain the platelet count above 50 × 109/L (24,25). Platelet transfusion may also be considered in the presence of qualitative platelet defects due to NSAID or aspirin use. There is no current evidence to justify the routine use of factor VII or tranexamic acid (TXA) in UGIB (25–27). In a stable, coagulopathic UGIB patient the decision to use plasma or vitamin K should be based on the medical cause of coagulopathy (e.g., warfarin for chronic atrial fibrillation versus cirrhosis) (28). An ongoing assessment of vital signs, general clinical status, and urine output will help to guide resuscitative efforts. In patients with massive bleeding, early consultation with a gastroenterologist, an intensivist, and possibly a surgeon or an interventional radiologist should be arranged. Further treatment of UGIB depends on whether the bleeding is nonvariceal or variceal.
Nonvariceal Bleeding
Pharmacologic therapy in nonvariceal UGIB centers on acid suppression. Gastric acid impairs clot formation, and many common causes of UGIB (e.g., ulcers, gastritis, esophagitis, and duodenitis) respond well to PPIs. High-dose intravenous PPIs decrease the need for endoscopic therapy, and consensus guidelines recommend starting high-dose PPI therapy prior to endoscopy (1). Nevertheless, no current evidence demonstrates that PPIs decrease mortality, risk of rebleeding at 30 days, or risk of surgery in patients with UGIB (29). A commonly recommended regimen is omeprazole 80 mg as an IV bolus, followed by 8 mg/hr for 3 days (11). H2 blockers have no role in the treatment of acute UGIB since they do not consistently raise the pH, and studies have failed to show any benefits (1).
Endoscopy is the most important diagnostic and therapeutic tool in UGIB. Endoscopy can identify the cause of bleeding, may provide prognostic information, and allows for the administration of endoscopic therapy (3,5,30,31). Patients with high-risk endoscopic findings such as active bleeding or a visible vessel require emergent endoscopic therapy (1), the main techniques being thermocoagulation and injection therapy. Patients with low-risk endoscopic findings (e.g., flat-based ulcer) do not require endoscopic treatment or high-dose PPI therapy but may benefit from standard oral PPI therapy as outpatients. Occasionally, endoscopy and pharmacologic therapy fail to stop the bleeding, and emergent surgery or angiography must then be considered (1,4). Angiographic therapy is gaining popularity for high-risk patients who cannot tolerate a major surgical procedure.
Variceal Bleeding
Variceal bleeding occurs mainly in patients with advanced cirrhosis and is associated with complications related to hepatic dysfunction such as coagulopathy, sepsis, renal failure, and hepatic encephalopathy. Overresuscitation is also a concern, as this increases portal pressure and may increase the risk of rebleeding.
Early endoscopy is critical in these high-risk patients since it may enable definitive therapy. However, endoscopy is often delayed due to logistical issues or patient instability. Pharmacologic therapy is utilized to decrease portal pressures. Octreotide, a synthetic analog of somatostatin, reduces portal hypertension. Although no mortality benefit has been established, octreotide improves endoscopic visualization and hemostasis (32,33). It has largely replaced vasopressin due to its better safety profile (32). The dose is 25 to 50 μg/hr by infusion.
Patients with variceal hemorrhage are also susceptible to bacteremia and infections such as pneumonia, spontaneous bacterial peritonitis, and urinary tract infection. Empiric treatment with a third-generation cephalosporin or a fluoroquinolone improves outcomes (34,35).
Endoscopic therapy for varices is divided into two types: sclerotherapy and band ligation. In the former, sclerosing agents are injected into the esophageal vessels, causing thrombosis and eventual necrosis. Band ligation involves endoscopic placement of a rubber band around the varix, inducing obstruction and eventual tissue necrosis that obliterates the varix. This is the preferred endoscopic approach, though it is technically more difficult (14,16). Gastric varices are deeper and more difficult to treat. The direct injection of tissue adhesive is becoming more widely used.
When endoscopy and pharmacologic therapy have been unsuccessful or unavailable, balloon tamponade can be a lifesaving measure. The Sengstaken-Blakemore tube, the Minnesota tube, and the Linton tubeare specialized inflatable NG tubes that apply direct pressure to the bleeding varix. However, the use of these tubes is associated with a number of complications, including esophageal rupture, pulmonary aspiration, and airway compromise. The tubes come with an explicit list of instructions that should be reviewed prior to their use, and they are best placed by an experienced practitioner. The Linton tube does not have an esophageal balloon, but it may be better at controlling gastric varices. Endotracheal intubation is recommended prior to placement (12,16).
More drastic measures are sometimes needed to reduce portal pressure. Transjugular intrahepatic portosystemic shunt is extremely effective at controlling refractory variceal bleeding. This involves the placement, by an interventional radiologist, of an expandable metal stent across a tract between a hepatic vein and a hepatic branch of the portal vein. Surgical treatment of variceal bleeding is much less common since the advent of transjugular intrahepatic portosystemic shunt and is now typically limited to portocaval shunts in patients with very-well-compensated stable liver disease. Orthotopic liver transplantation is considered in selected patients (12,14,16).
CRITICAL INTERVENTIONS
• Aggressively volume resuscitate patients with UGIB and clinical signs of shock.
• Consider early blood transfusion.
• Reverse coagulopathy as needed (platelets, FFP, and vitamin K).
DISPOSITION
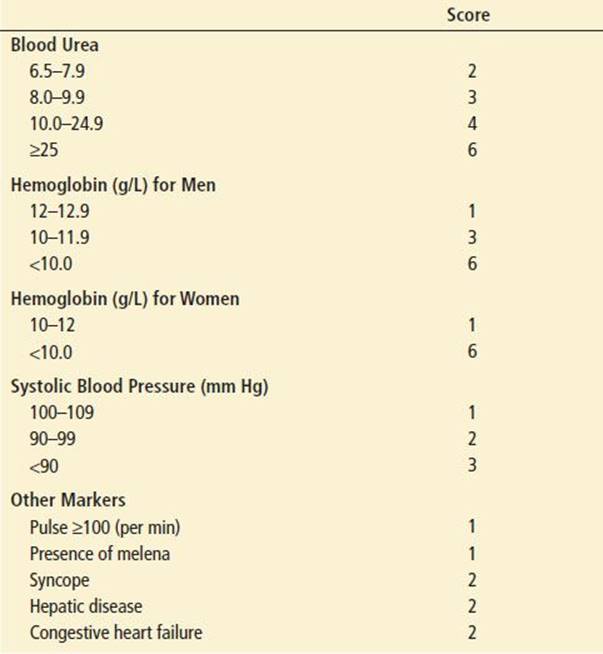
Risk scores have been designed to predict rebleeding and mortality in UGIB. Commonly used scores include the Rockall score and the Glasgow–Blatchford Bleeding Score (GBS). The GBS has been more extensively used (Table 99.2). An advantage of the GBS is that it does not require NG aspirate or endoscopy (17). A GBS of 0 is seen in up to 22% of UGIB patients and predicts that emergent medical care is not required; outpatient evaluation may thus be considered (17,36,37). Most other risk stratification models rely on the endoscopic appearance of the culprit lesion, which typically cannot be obtained in the ED.
TABLE 99.2
Glasgow–Blatchford Score
Nonvariceal Bleeding
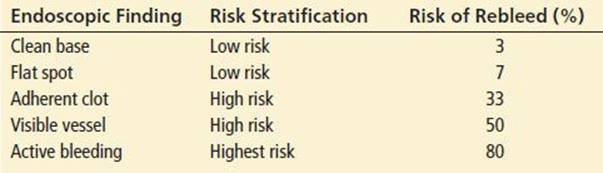
Most patients with UGIB due to a nonvariceal source should be admitted to the hospital, but carefully selected, stable patients with minimal blood loss may be safely discharged from the ED with close follow-up (Table 99.2). Endoscopic criteria can help to identify patients who can be safely managed as outpatients, since the risk of rebleeding is associated with certain endoscopic findings (Table 99.3) (38). This approach has the potential to identify a large subset of patients who may be discharged. Candidates for outpatient management must have reliable access to close outpatient follow-up and a demonstrated history of compliance with medical instructions. They should receive an oral PPI, should be told to avoid NSAIDs, and should be given clear instructions on reasons to return immediately for further medical attention.
TABLE 99.3
Endoscopic Appearance of Ulcers and Risk of Rebleeding (5)
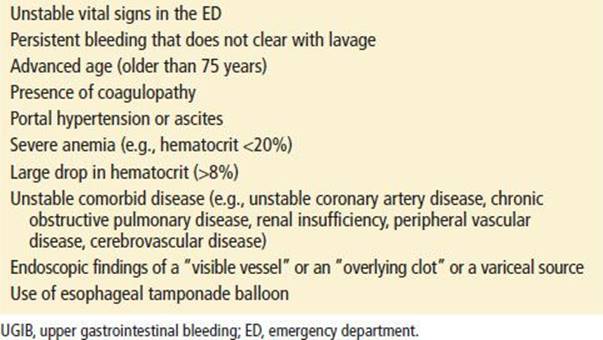
Patients who are unstable or have multiple adverse prognostic factors should be admitted to the ICU (Table 99.4). Although UGIB will stop spontaneously in many cases, up to 20% of patients may have continued or recurrent bleeding, with the risk of rebleeding being highest in the first 72 hours (1,38).
TABLE 99.4
Intensive Care Unit Admission Guidelines for Patients with Upper GI Bleed
Variceal Bleeding
The prognosis of patients with variceal bleeding is usually related to the severity of associated liver disease, and all such patients should be admitted. These patients frequently require critical care services. Early consultation with a gastroenterologist is imperative (12,14,16).
If the necessary critical care and consultant services are not readily available, the UGIB patient should be transferred to a facility with the necessary resources.
Common Pitfalls
• Underestimation of blood loss. Some patients can lose up to 20% to 30% of their blood volume and yet maintain a relatively normal blood pressure in the supine position. Moreover, patients with significant bleeding can have a normal initial hematocrit.
• Overreliance on a negative NG aspirate.
• Failure to recognize aortoenteric fistula as a cause of sudden massive hematemesis.
• Failure to involve a surgeon and/or interventional radiology in cases of massive hemorrhage with failed endoscopy.
• Treatment of hypovolemic shock with vasopressors instead of volume resuscitation.
REFERENCES
1. Barkun AN, Bardou M, Kuipers EJ, et al. International consensus recommendations on the management of patients with nonvariceal upper gastrointestinal bleeding. Ann Intern Med. 2010;152(2):101–113. doi:10.1059/0003-4819-152-2-201001190-00009.
2. Cappell MS, Friedel D. Initial management of acute upper gastrointestinal bleeding: From initial evaluation up to gastrointestinal endoscopy. Med Clin North Am. 2008;92(3):491–509, xi. doi:10.1016/j.mcna.2008.01.005.
3. Esrailian E, Gralnek IM. Nonvariceal upper gastrointestinal bleeding: Epidemiology and diagnosis. Gastroenterol Clin North Am. 2005;34(4):589–605. doi:10.1016/j.gtc.2005.08.006.
4. Marmo R, Koch M, Cipolletta L, et al. Predictive factors of mortality from nonvariceal upper gastrointestinal hemorrhage: A multicenter study. Am J Gastroenterol. 2008;103(7):1639–1647; quiz 1648. doi:10.1111/j.1572-0241.
2008.01865.x.
5. Palmer K. Acute upper gastrointestinal haemorrhage. Br Med Bull. 2007;83:307–324. doi:10.1093/bmb/ldm023.
6. Rockey DC. Gastrointestinal bleeding. Gastroenterol Clin North Am. 2005;34(4):581–588. doi:10.1016/j.gtc.2005.08.002.
7. Thompson HL, McGuffin DW. Melena; a study of underlying causes. J Am Med Assoc. 1949;141(17):1208–1213; Disc, 1217.
8. Schiff L, Stevens RJ, Shapiro N, et al. Observations on the oral administration of citrated blood in man. The effect on the stools. Am J Med Sci. 1942;203:409–412.
9. Daniel WA Jr, Egan S. The quantity of blood required to produce a tarry stool. JAMA. 1939;113:2232–2232.
10. Garrow D, Delegge MH. Risk factors for gastrointestinal ulcer disease in the US population. Dig Dis Sci. 2010;55(1):66–72. doi:10.1007/s10620-008-0708-x.
11. Gralnek IM, Barkun AN, Bardou M. Management of acute bleeding from a peptic ulcer. N Engl J Med. 2008;359(9):928–937. doi:10.1056/NEJMra0706113.
12. Toubia N, Sanyal AJ. Portal hypertension and variceal hemorrhage. Med Clin North Am. 2008;92(3):551–574, viii. doi:10.1016/j.mcna.2007.12.003.
13. O’Mara CS, Williams GM, Ernst CB. Secondary aortoenteric fistula. A 20 year experience. Am J Surg. 1981;142(2):203–209.
14. Jalan R, Hayes PC. UK guidelines on the management of variceal haemorrhage in cirrhotic patients. British Society of Gastroenterology. Gut. 2000;46(suppl 3–4):III1–III15.
15. Laine L, Peterson WL. Bleeding peptic ulcer. N Engl J Med. 1994;331(11):717–727. doi:10.1056/NEJM199409153311107.
16. Sharara AI, Rockey DC. Gastroesophageal variceal hemorrhage. N Engl J Med. 2001;345(9):669–681. doi:10.1056/NEJMra003007.
17. Srygley FD, Gerardo CJ, Tran T, et al. Does this patient have a severe upper gastrointestinal bleed? JAMA. 2012;307(10):1072–1079. doi:10.1001/jama.2012.253.
18. Ernst AA, Haynes ML, Nick TG, et al. Usefulness of the blood urea nitrogen/creatinine ratio in gastrointestinal bleeding. Am J Emerg Med. 1999;17(1):70–72.
19. Witting MD. “You wanna do what?!” Modern indications for nasogastric intubation. J Emerg Med. 2007;33(1):61–64. doi:10.1016/j.jemermed.2007.02.017.
20. Singer AJ, Richman PB, Kowalska A, et al. Comparison of patient and practitioner assessments of pain from commonly performed emergency department procedures. Ann Emerg Med. 1999;33(6):652–658.
21. Pallin DJ, Saltzman JR. Is nasogastric tube lavage in patients with acute upper GI bleeding indicated or antiquated? Gastrointest Endosc. 2011;74(5):981–984. doi:10.1016/j.gie.2011.07.007.
22. Huang ES, Karsan S, Kanwal F, et al. Impact of nasogastric lavage on outcomes in acute GI bleeding. Gastrointest Endosc. 2011;74(5):971–980. doi:10.1016/j.gie.2011.04.045.
23. Villanueva C, Colomo A, Bosch A, et al. Transfusion strategies for acute upper gastrointestinal bleeding. N Engl J Med. 2013;368(1):11–21. doi:10.1056/NEJMoa1211801.
24. Wolf AT, Wasan SK, Saltzman JR. Impact of anticoagulation on rebleeding following endoscopic therapy for nonvariceal upper gastrointestinal hemorrhage. Am J Gastroenterol. 2007;102(2):290–296. doi:10.1111/j.1572-0241.2006.00969.x.
25. Dworzynski K, Pollit V, Kelsey A, et al.; Guideline Development Group. Management of acute upper gastrointestinal bleeding: Summary of NICE guidance. BMJ. 2012;344:e3412.
26. Martí-Carvajal AJ, Karakitsiou DE, Salanti G. Human recombinant activated factor VII for upper gastrointestinal bleeding in patients with liver diseases. Cochrane Database Syst Rev. 2012;3:CD004887. doi:10.1002/14651858.CD004887.pub3.
27. Gluud LL, Klingenberg SL, Langholz E. Tranexamic acid for upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2012;1:CD006640. doi:10.1002/14651858.CD006640.pub2.
28. Martí-Carvajal AJ, Solà I. Vitamin K for upper gastrointestinal bleeding in patients with acute or chronic liver diseases. Cochrane Database Syst Rev. 2012;9:CD004792. doi:10.1002/14651858.CD004792.pub4.
29. Sreedharan A, Martin J, Leontiadis GI, et al. Proton pump inhibitor treatment initiated prior to endoscopic diagnosis in upper gastrointestinal bleeding. Cochrane Database Syst Rev. 2010;(7):CD005415. doi:10.1002/14651858.CD005415.pub3.
30. Gralnek IM, Dulai GS. Incremental value of upper endoscopy for triage of patients with acute non-variceal upper-GI hemorrhage. Gastrointest Endosc. 2004;60(1):9–14.
31. Spiegel BM, Vakil NB, Ofman JJ. Endoscopy for acute nonvariceal upper gastrointestinal tract hemorrhage: Is sooner better? A systematic review. Arch Intern Med. 2001;161(11):1393–1404.
32. Gøtzsche PC, Hróbjartsson A. Somatostatin analogues for acute bleeding oesophageal varices. Cochrane Database Syst Rev. 2008;(3):CD000193. doi:10.1002/14651858.CD000193.pub3.
33. Bañares R, Albillos A, Rincón D, et al. Endoscopic treatment versus endoscopic plus pharmacologic treatment for acute variceal bleeding: A meta-analysis. Hepatology. 2002;35(3):609–615. doi:10.1053/jhep.2002.31354.
34. Garcia-Tsao G, Sanyal AJ, Grace ND, et al.; Practice Guidelines Committee of the American Association for the Study of Liver Diseases, Practice Parameters Committee of the American College of Gastroenterology. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46(3):922–938. doi:10.1002/hep.21907.
35. Fernández J, Ruiz del Arbol L, Gómez C, et al. Norfloxacin vs ceftriaxone in the prophylaxis of infections in patients with advanced cirrhosis and hemorrhage. Gastroenterology. 2006;131(4):1049–1056; quiz 1285. doi:10.1053/j.gastro.2006.07.010.
36. Chen I-C, Hung M-S, Chiu T-F, et al. Risk scoring systems to predict need for clinical intervention for patients with nonvariceal upper gastrointestinal tract bleeding. Am J Emerg Med. 2007;25(7):774–779. doi:10.1016/j.ajem.2006.12.024.
37. Stanley AJ, Ashley D, Dalton HR, et al. Outpatient management of patients with low-risk upper-gastrointestinal haemorrhage: Multicentre validation and prospective evaluation. Lancet.2009;373(9657):42–47. doi:10.1016/S0140-6736(08)61769-9.
38. Corley DA, Stefan AM, Wolf M, et al. Early indicators of prognosis in upper gastrointestinal hemorrhage. Am J Gastroenterol. 1998;93(3):336–340. doi:10.1111/j.1572-0241.1998.00336.x.