Jeahan H. Colletti and James E. Colletti
Diarrheal illness continues to be a significant cause of pediatric morbidity and mortality. Worldwide diarrheal illnesses are the second leading cause of mortality in children under 5 years of age, accounting for approximately 1.5 million deaths per year (1).
CLINICAL PRESENTATION
The most common presenting etiology of diarrhea in children is infectious gastroenteritis, with viral agents accounting for 75% of cases. Acute diarrhea typically lasts less than 2 weeks, and the history is one of a distinct change in stool frequency, volume, and color. The stools may be less well-formed and yellowish, loose and green, or watery and voluminous. The presence of bloody, mucoid stools increases the possibility of a bacterial cause. Vomiting is common, especially with viral disorders. However, bilious vomiting requires close attention and raises the possibility of intestinal obstruction. Intussusception may complicate an otherwise mild gastroenteritis. Low-grade fever is common, but fever in excess of 40°C suggests a bacterial etiology.
Important history includes antibiotic use, recent travel, or other exposures such as daycare, pets, or an unsanitary water supply. The patient’s prior weight, duration of illness, and associated signs and symptoms, such as fever, abdominal pain, vomiting, rash, seizures, and activity level, can aid in determining the degree and severity of dehydration. A vital component of the history is the type of oral intake given to the child. The use of hyperosmolar fluids, such as carbonated soft drinks, apple juice, or excess sodium due to improper formula preparation, can result in hypernatremia, whereas hypotonic fluid replacement can result in hyponatremia.
Assessment for signs of dehydration is of vital importance Infants may become critically dehydrated over a period of only a few hours and present with shock. As the vascular space contracts, the extremities become cool with decreased distal pulses, and alterations in mental status occur. Gorelick et al. (2) discovered that the findings of three or fewer of the clinical signs of dehydration correlated with a 5% fluid deficit, three to five signs correlated with 5% to 9% dehydration, and more than six signs with a fluid deficit of 10% or greater. In general, the diagnosis of dehydration is improved by the presence of multiple signs or through the use of clinical scales.
Parental reporting has been found to accurately predict degree of dehydration as well as clinically significant acidosis (3). A parental report of a normal tearing state is associated with a reduced likelihood of significant dehydration and acidosis. Moreover, parental reporting of a sunken fontanelle and decreased tears are associated with an increased likelihood of hospital admission (3).
DIFFERENTIAL DIAGNOSIS
The differential diagnosis of diarrheal illness is broad. Diarrhea may accompany almost any pediatric illness at any given point in its course. The differential diagnosis may be categorized as acute or chronic. There may be important diagnostic clues based on the child’s age, character of the stool, associated symptoms, and effect on the child’s general health.
The most common causes of acute and chronic diarrheal disease are listed in Table 224.1. The vast majority of acute diarrheal illnesses are viral. Before the introduction of the rotavirus vaccines, rotavirus was the leading cause of severe acute gastroenteritis (AGE) in US children less than 5 years of age. Since the introduction of the vaccines in 2006, there has been a significant (60% to 65%) reduction in the number of rotavirus-associated hospitalizations (4). With the reduction in rotavirus-associated diarrhea, the Noroviruses have become the leading cause of AGE in children.
TABLE 224.1
Common Causes of Acute and Chronic Diarrheal Illness

ED EVALUATION AND MANAGEMENT
The goals of diarrhea management include prevention of dehydration by early fluid administration, treatment of dehydration with an oral rehydration solution (ORS), continued feeding during the diarrhea, selective use of antibiotics, and avoidance of antidiarrheal medications (5,6).
A thorough history should determine acute or chronic status. Preliminary studies that may be indicated for chronic diarrhea include a stool examination for blood, parasites, culture, Sudan fat stain, and alpha-1-antitrypsin. If there is significant dehydration or failure to thrive, the child should be hospitalized. Otherwise, the patient should be referred to a pediatrician for further evaluation.
If the diarrhea is acute, the primary concern is for dehydration, acidosis, electrolyte disturbances, shock, or associated sepsis. The physical examination indicates the degree of dehydration (Table 224.2). The serum bicarbonate level may occasionally also prove useful. A bicarbonate concentration of <17 mEq/L, when considered along with clinical parameters may improve accuracy in determining the presence of moderate to severe dehydration (7,8). Conversely, a bicarbonate concentration of >15 or 17 mEq/L decreases the likelihood of dehydration (9). Furthermore, a bicarbonate of ≤13 mEq/L is associated with a need for prolonged IV fluid replacement (3,10). Other than a guaiac test or culture, stool studies such as fecal leukocytes, Rotazyme, pH, reducing substances, and ova and parasites are usually not helpful in the emergent setting.
TABLE 224.2
Estimating Degree of Dehydration

KEY TESTING
• Well-appearing child with minimal or no dehydration—no testing
• Ill-appearing child or signs of significant dehydration— electrolytes (serum bicarbonate and glucose levels of particular interest)
• Febrile child with bloody stools—stool culture
Dehydration exceeding 5% to 10%, or significant electrolyte disturbances, are considerations for admission. Rehydration should begin in the emergency department (ED). In children who are mildly to moderately dehydrated and refusing oral intake, a nasogastric tube can be placed to initiate replacement therapy. An investigation by Nager and Wang (11) examined rapid nasogastric hydration and rapid intravenous hydration and determined them to be safe, efficacious, and cost-effective alternatives to standard therapy for moderately dehydrated children. When rapid nasogastric hydration was compared to rapid intravenous hydration, there was no significant difference. In this trial, rapid nasogastric hydration was achieved by administering a continuous infusion of 50 mL/kg of Pedialyte over 3 hours, and rapid intravenous hydration was performed by a continuous infusion of 50 mL/kg of normal saline over 3 hours.
In severely dehydrated children, intravenous normal saline boluses of 20 cc/kg should be initiated, with repeat boluses as needed to restore intravascular volume. It is common to administer 60 to 80 cc/kg in the initial phase of fluid resuscitation. Close monitoring of the pulmonary status and urine output is important in children with underlying cardiac or pulmonary conditions. Once intravascular volume has been restored, dextrose-containing maintenance fluid should be initiated. Potassium replacement should continue until the patient is spontaneously voiding and is known to have normal renal function.
In mild to moderate dehydration, oral rehydration therapy (ORT) should begin with a commercially available ORS. ORT is an inexpensive, effective therapy for dehydration that is underutilized in the United States (12). In mildly to moderately dehydrated children, ORT is as effective as IV therapy. Furthermore, ORT has been found to be associated with higher parental satisfaction and decreases in both length of stay and staff time (6,12).
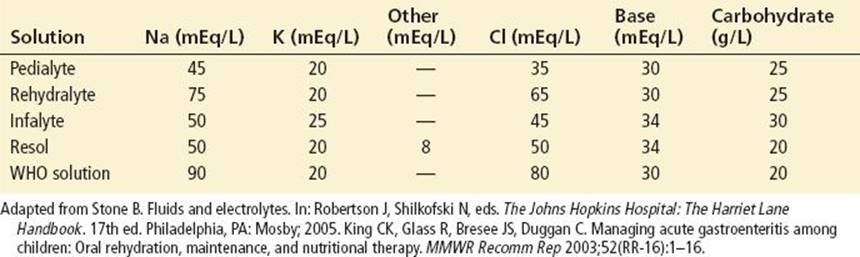
Homemade solutions and electrolyte-glucose beverages for athletes should be avoided the former because serious errors may be made in preparation and the latter because they contain too little sodium, too much sugar, and almost no potassium. The use of carbonated beverages, apple juice, and Jello water should also be discouraged, as they consist of high concentrations of carbohydrates and low concentrations of required electrolytes. The high osmotic load of these fluids often results in an increase in stool output, and their low sodium content may contribute to hyponatremia (13,14). Each liter of a commercial ORS contains about 45 to 75 mEq sodium, 20 to 25 mEq potassium, 2% glucose, and a mixture of chloride and base as anions (Table 224.3). This ratio of electrolytes and glucose promotes the coupled mucosal transport of sodium and glucose, with water absorption following.
TABLE 224.3
Contents of Commercial Oral Rehydration Solutions
If oral rehydration is chosen, it is best started during an extended period of monitored therapy in the ED, and it may be implemented in any child who can drink and is not in shock. The efficacy of ORT has been established even in the child with emesis accompanying diarrhea. In these children, ORT should be administered in small frequent doses (5 mL q1–2 min) (13,14). Table 224.4 lists a program for mild to moderate dehydration. Table 224.5 lists contraindications to ORT.
TABLE 224.4
Emergency Department (ED) Management of Acute Diarrhea with Mild to Moderate Dehydration

TABLE 224.5
Restrictions to ORT Administration

ORT consists of two phases of therapy. The first is the rehydration phase, in which fluid and electrolytes are restored. Ideally the first phase is completed within a 3- to 4-hour period. The second phase is the maintenance phase, which includes the replacement of ongoing electrolyte and fluid losses as well as ensuring dietary intake.
After successful oral rehydration, a prompt return to age-appropriate diet is indicated. It should be stressed to parents that the objective is to “feed through” the diarrhea, and that loose stools will persist for a few days but should decrease in volume and frequency (15). Continued feeding is safe and may reduce the duration and volume of diarrhea (14). Early refeeding has not been shown to increase the risk of unscheduled parenteral fluid administration, emesis episodes, or the development of persistent diarrhea (16). In general, smaller but more frequent feedings should be given so that the total daily intake approaches normal (5).
Restricted and progressive diets are no longer recommended (17). Breast-fed infants may continue to feed on demand through both the rehydration and maintenance phases of management. Infants who are bottle-fed should stop feeds during rehydration but should restart them with full-strength formula once the rehydration phase is complete. Restarting full-strength formula allows for a return to full caloric intake. Lactose-free formulas are generally not necessary but may be useful in children who are malnourished, have a severe enteropathy, or have persistent lactose intolerance (17). For older children on a mixed diet, the traditional bland diet of bananas, rice or rice cereal, applesauce, and toast (commonly called the BRAT diet) is no longer recommended. To date, there are no studies to support the use of a bland diet and moreover, the BRAT diet is unnecessarily restrictive and provides suboptimal nutrition (17). Therefore, once hydration has been reestablished, the child’s usual preferred and age-appropriate diet should be resumed, although the BRAT diet may be incorporated into the child’s regular diet if desired. Carbonated soft drinks, juice, gelatin desserts, and foods with significant amounts of simple sugars should be avoided, as the osmotic load may increase the diarrhea.
Most episodes of diarrhea do not require antimicrobial therapy, as the predominant cause of acute diarrhea is viral. Moreover, even when a bacterial etiology is responsible, the majority of acute diarrheal cases are self-limited, and the duration of illness is not shortened by antibiotic therapy. However, antimicrobial therapy should be considered in immunosuppressed children, premature infants, septic infants, those with a toxic appearance, or children with underlying disorders (17).
Bloody diarrhea with PMNs probably represents a bacterial cause, and antibiotic therapy may be considered if Escherichia coli O157:H7 and Salmonella have been excluded. The association of antibiotic therapy in children with E. coli 0157:H7 and the development of hemolytic uremic syndrome (HUS) is controversial. It is currently unknown whether empiric antibiotic therapy increases the risk of HUS (18). A few investigations have reported an increased risk of HUS with empiric antibiotic therapy (19,20). In contrast, others have reported a protective effect or a lack of association (21–23). Therefore, the physician contemplating empiric antibiotic therapy for bloody diarrhea should give careful consideration to the possibility of E. coli 0157:H7 infection and the potential for an increased risk of HUS with antibiotics.
Generally, antibiotics should be avoided in Salmonella gastroenteritis, but exceptions include certain populations prone to Salmonella bacteremia, such as in infants younger than 3 months old and in patients with immunodeficiency, a history of chronic gastrointestinal tract disease, or hemoglobinopathies (5). These high-risk patients should be admitted and given intravenous antibiotics.
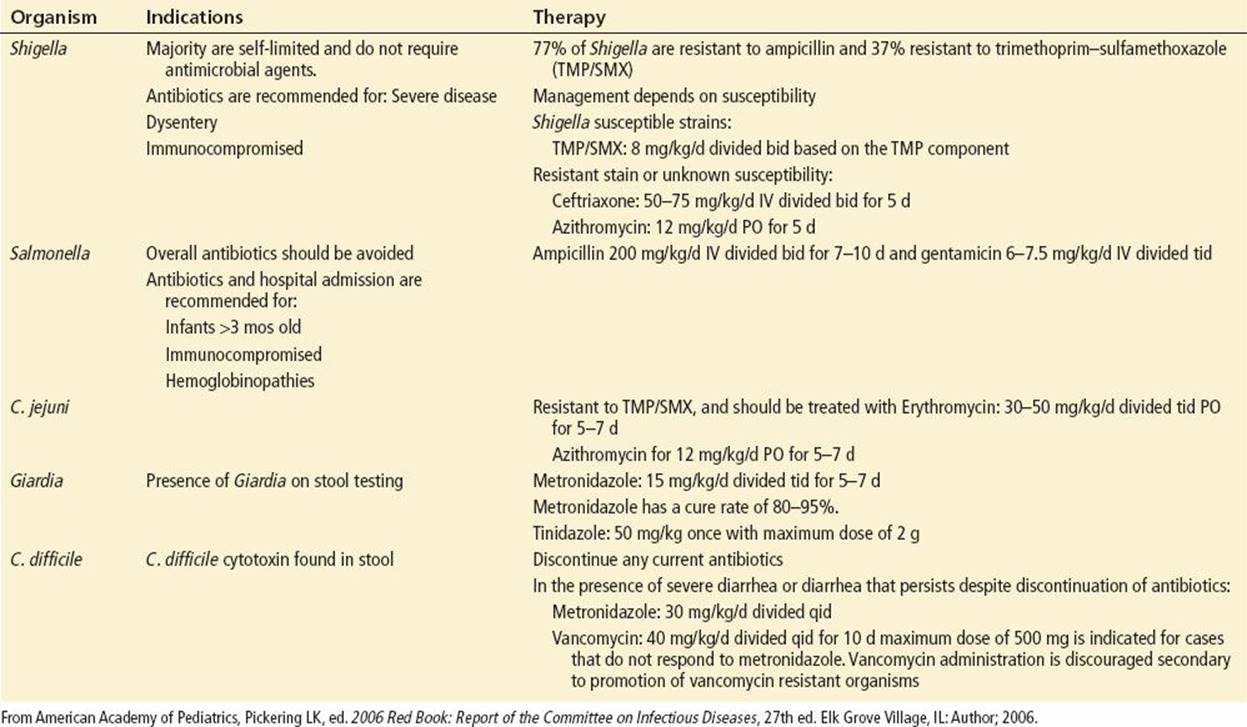
In cases where E. Coli 0157:H7 and Salmonella have been excluded and antimicrobial therapy is required, initial antibiotic selection should be adjusted based on stool culture and sensitivity results (Table 224.6).
TABLE 224.6
Antibiotic Therapy Based on Etiology
The American Academy of Pediatrics does not recommend the use of antiemetic, antisecretory, or antiperistaltic drugs (6). There is a growing body of evidence that selective use of antiemetics (particularly ondansetron) may be effective in decreasing the rate of vomiting, improving the success rate of oral hydration, preventing the need for IV hydration, and preventing the need for hospital admission in those receiving IV hydration (see Chapter 223).
The use of narcotic-based agents is specifically contraindicated in bacterial gastroenteritis because they may induce bowel stasis and promote more aggressive bacterial invasion. Some of the adverse events associated with use of such antidiarrhea agents in the pediatric population are ileus, lethargy, and death. A systematic review and meta-analysis found the risks to outweigh the benefits of loperamide, specifically in children less than 3 years of age, in those that are malnourished, moderately or severely dehydrated, or systemically ill, and in the presence of dysentery (24).
Parents should be instructed on hygienic precautions for diaper handling and good hand-washing practices. Strict hand-washing techniques have been demonstrated to reduce the incidence of acute infectious diarrhea in daycare facilities (25). The child should be excluded from the daycare center if there is diarrhea not contained by diaper or toilet use, if stools contain mucus or blood, or if there is associated fever.
CRITICAL INTERVENTIONS
• Recognition and correction of dehydration, acidosis, electrolyte disturbances, hypoglycemia, shock, or associated sepsis
• ORT should be administered over a period of 3 to 4 hours.
• Additional ORS should be administered for ongoing losses.
• Prompt return to an age-appropriate diet once rehydration is achieved
• Selective utilization of antibiotics based on exclusion of E. Coli 0157:H7 and Salmonella by culture as well as by the criteria listed in Table 224.6
• Avoidance of antisecretory or antiperistaltic medications
• Instruction of parents on hygienic precautions.
DISPOSITION
If more than 5% dehydration is present, a pediatrician should be consulted for probable admission, with rehydration efforts beginning in the ED. With chronic diarrhea, consultation with a pediatrician or pediatric gastroenterologist is in order. Diarrhea may paradoxically complicate surgical conditions (e.g., Hirschsprung disease), in which case a pediatric surgeon should be consulted.
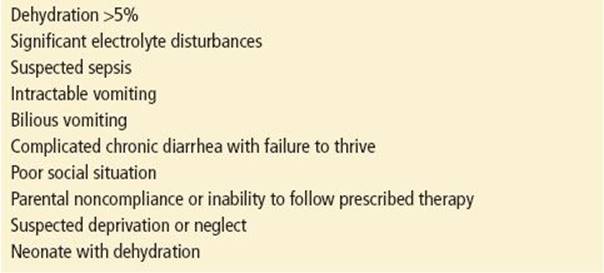
Indications for hospitalization are listed in Table 224.7. Sepsis and serious illness in infants younger than 1 month old may be clinically subtle or occult. Even mild dehydration in young infants deserves careful consideration for admission.
TABLE 224.7
Indications for Admission
Simple diarrhea with dehydration requires only judicious oral or intravenous rehydration and rarely requires transfer unless there are no inpatient pediatric services. Complicated cases of dehydration (e.g., those associated with hypernatremia) or those of chronic duration usually require specific pediatric expertise.
Common Pitfalls
• Failure to appreciate that the young infant with diarrhea may initially appear well but develop serious dehydration over a short period
• Use of restrictive or progressive diets
• Failure to rely on the caregiver’s history of decreased or absent urine output, lethargy, or inability to tolerate fluids may lead to inappropriate management and disposition.
• Underestimation of the degree of hypovolemia and failing to identify subtle signs of shock
• Failure to follow strict hand hygiene
ACKNOWLEDGMENTS
The authors gratefully acknowledge the contributions of Lowell Clark and Ghazala Sharieff to the content of this chapter.
REFERENCES
1. Bryce J, Boschi-Pinto C, Shibuya K, et al. WHO estimates of the causes of death in children. Lancet. 2005;365:1147–1152.
2. Gorelick MH, Shaw KN, Murphy K. Validity and reliability of clinical significance in the diagnosis of dehydration in children. Pediatrics. 1997;99(5):E6.
3. Porter SC, Fleisher GR, Kohane IS, et al. The value of parental report for diagnosis and management of dehydration in the emergency department. Ann Emerg Med. 2003;41:196–205.
4. Cortes JE, Curns AT, Tate JE, et al. Rotavirus vaccine and health care utilization for diarrhea in U.S. children. N Engl J Med. 2011;365(12):1108–1117.
5. Gastanaduy AS, Begue RE. Acute gastroenteritis. Clin Pediatr. 1999;38:1–12.
6. Provisional Committee on Quality Improvement, Subcommittee on Acute Gastroenteritis, American Academy of Pediatrics Practice parameter. The management of acute gastroenteritis in young children. Pediatrics. 1996;97:424–435.
7. Vega RM, Avner JR. A prospective study of the usefulness of clinical and laboratory parameters for predicting percentage of dehydration in children. Pediatr Emerg Care. 1997;13:179–182.
9. Steiner MJ, DeWalt DA, Byerley JS. Is this child dehydrated? JAMA. 2004;291(22):2746–2754.
10. Reid SR, Bonadio WA. Outpatient rapid intravenous rehydration to correct dehydration and resolve vomiting in children with acute gastroenteritis. Ann Emerg Med. 1996;28:318–323.
11. Nager AL, Wang VJ. Comparison of nasogastric and intravenous methods of rehydration in pediatric patients with acute dehydration. Pediatrics. 2002;109:566–572.
12. Conners GP, Barker WH, Mushlin AI, et al. Oral versus intravenous: Rehydration preferences of pediatric emergency medicine fellowship directors. Pediatr Emerg Care. 2000;16:335–338.
13. Burkhart DM. Management of acute gastroenteritis in children. Am Fam Physician. 1999;60:2555–2566.
14. Santosham M. Oral rehydration therapy: Reverse transfer of technology. Arch Pediatr Adolesc Med. 2002;156:1177–1179.
15. Sullivan PB. Nutritional management of acute diarrhea. Nutrition. 1998;14:758–762.
16. Gregorio GV, Dans LF, Silvestre MA. Early versus delayed refeeding for children with acute diarrhoea. Cochrane Database Syst Rev. 2011;(7):CD007296.`
17. King CK, Glass R, Bresee JS, et al. Managing acute gastroenteritis among children: Oral rehydration, maintenance, and nutritional therapy. MMWR Recomm Rep. 2003;52(RR-16):1–16.
18. Molbak K, Mead PS, Griffin PM. Risk of hemolytic uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 Infection. JAMA. 2002;288:1014–1016.
19. Slutsker L, Ries AA, Maloney K, et al. A nationwide case-control study of Escherichia coli O157:H7 infection in the United States. J Infect Dis. 1998;177:962–966.
20. Wong CS, Jelacic S, Habeeb RL, et al. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;342:1930–1936.
21. Ikeda K, Ida O, Kimoto K, et al. Effect of early fosfomycin treatment on prevention of hemolytic uremic syndrome accompanying Escherichia coli O157:H7 infection. Clin Nephrol. 1999;52:357–362.
22. Proulx F, Turgeon JP, Delage G, et al. Randomized, controlled trial of antibiotic therapy for Escherichia coli O157:H7 enteritis. J Pediatr. 1992;121:299–303.
23. Safdar N, Said A, Gangnon RE, et al. Risk of hemolytic uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 enteritis: A meta-analysis. JAMA. 2002;288:996–1001.
24. Li ST, Grossman DC, Cummings P. Loperamide therapy for acute diarrhea in children: Systematic review and meta-analysis. PLoS Med. 2007;4(3):e98.
25. Roberts L, Jorm L, Patel M, et al. Effect of infection control measures on the frequency of diarrheal episodes in child care: A randomized, controlled trial. Pediatrics. 2000;105:743–746.