Syana Sarnaik
Pediatric patients present with three basic categories of rhythm disturbance—fast, slow, or absent. Asystole and bradyarrhythmias are primarily seen in resuscitation settings and are discussed in Chapter 217. This chapter discusses dysrhythmias unique to pediatric patients outside the realm of critical resuscitation.
SUPRAVENTRICULAR TACHYCARDIA
Paroxysmal supraventricular tachycardia (SVT) is the most common pediatric tachydysrhythmia, and may present to the emergency department (ED) in children of almost any age. Infants may tolerate SVT well for 12 to 24 hours, but if the rhythm is sustained for longer periods, signs of congestive heart failure (CHF) may develop (1). Manifestations of CHF in infants include irritability, tachypnea, and poor feeding and, in more severe cases, mottling and cyanosis. Once CHF develops, the infant’s ability to compensate is compromised, and the condition can deteriorate rapidly. Older children may have chest pain, palpitations, syncope, fatigue, and dyspnea. In general, the longer SVT continues, the more severe the symptoms. Because of decreased diastolic filling time, tachycardia can lead to decreased stroke volume and therefore decreased cardiac output. Sustained tachycardia is also associated with increased myocardial oxygen demand and decreased time for diastolic myocardial perfusion. Thus, SVT can lead to CHF even after the tachycardia has resolved.
There are three main categories of SVT: AV reentrant tachycardia; atrial tachycardia; and junctional tachycardia. The majority of SVTs are due to reentrant tachycardia. Atrial tachycardias include atrial flutter (characterized by reentrant circuits within the atria), atrial fibrillation, and ectopic atrial tachycardia. Junctional tachycardia is exceedingly rare outside the immediate postoperative phase of open heart surgery.
The etiology of the SVT varies by age group. In infants, more than 50% is idiopathic, and 10% to 20% is associated with Wolff–Parkinson–White (WPW) syndrome (2). The remainder of cases occur after cardiac surgery or in association with congenital heart defects that predispose to SVT, such as Ebstein anomaly, single ventricle physiology, and congenitally corrected transposition of the great arteries. Older children are more likely to have WPW, concealed bypass tracts, or congenital heart disease. Young infants are more likely to present with CHF.
Electrocardiographic Findings
The typical electrocardiogram (ECG) of a patient with SVT shows a rapid rate, a narrow QRS complex, and an absence of identifiable P-waves (Fig. 266.1). In reentrant SVT, the circuit is usually too short to generate a substantial P-wave deflection or the P-wave may be buried in the QRS or T-wave. However, when P-waves are visible, the P-axis is usually abnormal. In reentrant tachycardia, the rhythm is usually regular, with a rate of 220 to 320 beats/min in infants and 150 to 250 beats/min in older children. If the rate varies over time, the rhythm is less likely to be reentrant and more likely to be sinus tachycardia secondary to fever, pain, agitation, dehydration, or possibly an ectopic atrial tachycardia.
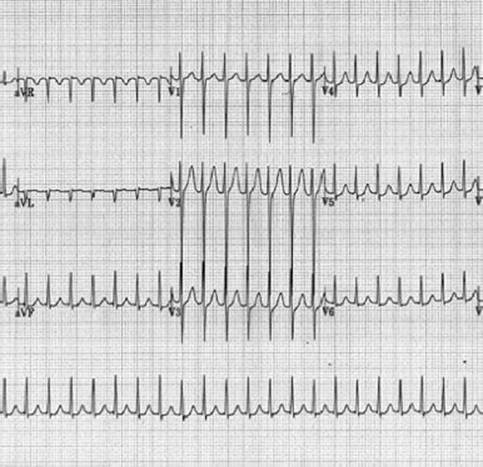
FIGURE 266.1 Supraventricular tachycardia.
ED MANAGEMENT
In an asymptomatic hemodynamically stable patient, the initial approach is to perform vagal maneuvers, followed if necessary by pharmacologic or electrical cardioversion. The effectiveness of vagal maneuvers is related to the patient’s age, with the success rate lower in infants and young children (3,4). Nevertheless, the occasional conversion justifies their initial trial. For infants and young children, the application of a bag of crushed ice to the face (to induce the diving reflex) for up to 30 seconds is an effective vagal stimulus. Older children may be asked to blow into an occluded straw or to perform a Valsalva maneuver, which requires cooperation and usually a sustained effort of 15 seconds. Because of the risk of retinal detachment, ocular compression is not a recommended vagal maneuver. The majority of SVTs are reentrant and respond to intravenous adenosine (5). Since its hemodynamic side effects are typically mild and very brief, a diagnostic dose of adenosine can be given safely if the type of underlying rhythm is not clear (Fig. 266.2).
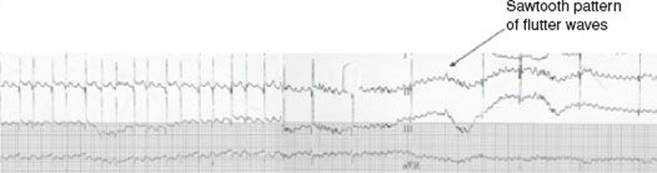
FIGURE 266.2 Adenosine dose uncovering atrial flutter.
Adenosine causes transient AV block by hyperpolarizing the AV node. This may cause some patients to have an uncomfortable sensation but lasts only a few seconds. The initial recommended dose of adenosine is 0.1 mg/kg (initial maximum of 6 mg, followed by repeat doses of 12 mg) as a rapid bolus, followed immediately by a rapid flush of 5 to 10 mL of normal saline. Given adenosine’s very short half-life of <1.5 seconds, it is important to use a three-way stopcock for a rapid flush immediately after the drug is administered. When administering adenosine, an ECG should be obtained prior to, and during, the conversion so as to document the underlying rhythm.
The patient may have a short break in the tachycardia due to adenosine followed by early recurrence requiring additional doses of adenosine. Infants may require up to 0.3 mg/kg by rapid intravenous push in a peripheral intravenous line, preferably positioned in the right arm. The adenosine dose can generally be lower if central venous access is obtained.
In general, calcium channel blockers are contraindicated in infants, as they may produce extreme bradycardia and hypotension in children younger than 1 year (6). In stable patients, other medications can be used, with input from a pediatric cardiologist. These include amiodarone (5 mg/kg), which slows AV nodal conduction and interrupts reentrant circuits, and procainamide (15 mg/kg over 15 minutes). Amiodarone and procainamide should not routinely be given together, as hypotension and QT prolongation may occur. A pediatric cardiologist should also be involved after successful conversion of SVT for further management and prevention of recurrence. Since patients with SVT by definition have an acquired or anatomic defect of the conduction system, and since they may deteriorate rapidly, it is prudent to have equipment immediately available for airway management and defibrillation.
Immediate synchronized cardioversion with 0.5 to 1 J/kg is indicated if the patient is hemodynamically unstable. Cardioversion may not be successful in the presence of hypoxia or an acid–base disorder, so there should be careful attention to concurrent management of airway, breathing, and circulation (ABCs). Cardioversion can induce ventricular dysrhythmias in patients who are taking digoxin. In cases of digoxin-related ventricular arrhythmia, lidocaine can be used (1).
COMPLETE HEART BLOCK
Complete heart block may be either congenital or acquired. It may be associated with structural heart defects or occur postoperatively after repair of a congenital heart lesion, especially Tetralogy of Fallot (TOF) or ventricular septal defect (VSD). Maternal collagen vascular disease (e.g., lupus) may also result in transplacental passage of maternal immunoglobulins that result in an abnormal fetal conduction system. Infants typically present with bradycardia and a ventricular rate usually less than 75 beats/min. ECG findings include dissociation between atrial and ventricular depolarization and either a wide or a narrow QRS, depending on whether the escape beats are junctional or ventricular. The clinical presentation in infants may range from asymptomatic to frank CHF. Older children may have syncope, fatigue, and decreased exercise tolerance. In unstable patients, management focuses on stabilization of the ABCs and consideration of an infusion of isoproterenol (0.02 to 0.5 μg/kg/min) or epinephrine (0.05 to 0.5 μg/kg/min) to increase the junctional or ventricular escape rate, pending pacemaker placement. Improving AV nodal conduction with atropine can be considered in first- and second-degree heart block but is not helpful in third-degree heart block. An external pacer should be applied while awaiting more definitive management.
VENTRICULAR DYSRHYTHMIAS
Isolated premature ventricular contractions (PVCs) may occur in up to 15% of normal newborns, 33% of normal adolescents, and 66% of patients with repaired heart disease (e.g., TOF, VSD, AV canal defects, transposition of the great vessels, and aortic stenosis) (7). An incidental finding of isolated PVCs is not worrisome, provided the remainder of the ECG is normal and the frequency of PVCs decreases with bedside exercise. However, multiform or complex ectopy (couplets, triplets), especially in an ill-appearing or febrile child, can be a presenting sign of myocarditis.
Ventricular tachycardia (VT) is defined as a series of three or more PVCs at a rate of 120 to 200 beats/min. QRS complexes are wide, and T waves have a polarity opposite the QRS. VT does not occur in children with normal hearts and usually indicates serious underlying myocardial pathology, dysfunction, or toxicity. Although uncommon, hemodynamically unstable ventricular arrhythmia requires immediate aggressive treatment. Cardiac output is seriously compromised in VT, and the rhythm is vulnerable to rapid deterioration to ventricular fibrillation. In the occasional patient who is stable, amiodarone should be given slowly, at a dose of 5 mg/kg over 20 to 30 minutes to avoid hypotension.
Unstable patients with VT require immediate synchronized cardioversion with 2 to 4 J/kg. Patients with pulseless VT require immediate defibrillation starting at 2 J/kg.
Electrolyte abnormalities should be considered in patients who are refractory to cardioversion. Drug ingestions causing dysrhythmias may require specific therapy (e.g., bicarbonate in patients with tricyclic overdose). In patients with digoxin toxicity, synchronized cardioversion should be avoided and treatment with digoxin-specific Fab fragments initiated.
ATRIAL FIBRILLATION
Atrial fibrillation is usually associated with structural heart disease such as dilated atria, myocarditis, digitalis toxicity, or previous intra-atrial surgery (e.g., Fontan procedure for hypoplastic left heart syndrome).
The ECG is characterized by an extremely fast atrial rate or a lack of recognizable atrial activity and an irregularly irregular ventricular response with narrow QRS complexes. Rate control can be accomplished by cautious administration of a beta blocker or calcium channel blocker. Digoxin may be started for longer-term control but is not effective acutely. In patients with atrial fibrillation and WPW syndrome, there may be rapid conduction to the ventricles and a risk of deterioration with drugs that preferentially slow AV node conduction, such as calcium channel blockers. Consultation with a cardiologist is strongly recommended (2).
For rhythm conversion, class I antiarrhythmic agents (i.e., quinidine, procainamide, flecainide) or the class III agent amiodarone may be used. Unstable patients require synchronized cardioversion, using 0.5 J/kg.
CRITICAL INTERVENTIONS
• Stabilize ABCs.
• Run a rhythm strip while administering adenosine to convert SVT.
• Be prepared for deterioration of dysrhythmia or patient’s overall condition.
Common Pitfalls
• Rapid administration of amiodarone in stable patients.
• Failure to recognize complete heart block and failure to place a pacemaker as needed.
• Intravenous calcium channel blockers are almost always contraindicated in infants.
ACKNOWLEDGMENTS
The author gratefully acknowledges the contributions of Syana Sarnaik and Ajit Sarnaik to the content of this chapter.
REFERENCES
1. Gewitz MH, Woolf PK. In: Fleisher GR, Ludwig S, eds Textbook of Pediatric Emergency Medicine. 6th ed. Lippincott Williams & Wilkins, 2010.
2. Binder LS, Boeche R, Atkinson D. Evaluation and management of supraventricular tachycardia in children. Ann Emerg Med. 1991;20(1):51–54.
3. Fulton DR, Grodin M. Pediatric cardiac emergencies. Emerg Med Clin North Am. 1983;1(1):45–61.
4. Garson A Jr, Gillette PC, McNamara DG. Supraventricular tachycardia in children: Clinical features, response to treatment, and long-term follow-up in 217 patients. J Pediatr. 1981;98(6):875–882.
5. Lee C, Mason LJ. Pediatric cardiac emergencies. Anesth Clin North Am. 2001; 19(2):287–308.
6. Epstein ML, Kiel EA, Victorica BE. Cardiac decompensation following verapamil therapy in infants with supraventricular tachycardia. Pediatrics. 1985;75(4):
737–740.
7. Park MK. Pediatric Cardiology for Practitioners. 4th ed. St. Louis, MO: Mosby, 2002.