Opening Scenario
Joseph Short, a 46-year-old male, comes to the ED complaining of chest pain.
Vital Signs
BP: 165/85 mm Hg Temp: 98.6°F (37°C)
RR: 22/minute HR: 90/minute, regular
Examinee Tasks
1. Take a focused history.
2. Perform a focused physical exam (do not perform rectal, genitourinary, or female breast exam).
3. Explain your clinical impression and workup plan to the patient.
4. Write the patient note after leaving the room.
Checklist/SP Sheet
Patient Description
Patient is a 46 yo M.
Notes for the SP
■ Lie on the bed and exhibit pain.
■ Place your hands in the middle of your chest.
■ Exhibit difficulty breathing.
■ If ECG is mentioned by the examinee, ask, “What is an ECG?”
Challenging Questions to Ask
“Is this a heart attack? Am I going to die?”
Sample Examinee Response
“As you suspect, your symptoms are of significant concern. We need to learn more about what’s going on to know if your pain is life threatening.”
Examinee Checklist
Building the Doctor-Patient Relationship Entrance
□ Examinee knocked on the door before entering.
□ Examinee introduced self by name.
□ Examinee identified his/her role or position.
□ Examinee correctly used patient’s name.
□ Examinee made eye contact with the SP.
Reflective Listening
□ Examinee asked an open-ended question and actively listened to the response.
□ Examinee asked the SP to list his/her concerns and listened to the response without interrupting.
□ Examinee summarized the SP’s concerns, often using the SP’s own words.
Information Gathering
□ Examinee elicited data efficiently and accurately.
Connecting with the Patient
□ Examinee recognized the SP’s emotions and responded with PEARLS.
Physical Examination
□ Examinee washed his/her hands.
□ Examinee asked permission to start the exam.
□ Examinee used respectful draping.
□ Examinee did not repeat painful maneuvers.

Closure
□ Examinee discussed initial diagnostic impressions.
□ Examinee discussed initial management plans:
□ Follow-up tests.
□ Lifestyle modification (diet, exercise).
□ Examinee asked if the SP had any other questions or concerns.
Sample Closure
Mr. Short, the source of your pain can be a cardiac problem such as a heart attack or angina, or it may be due to acid reflux, lung problems, or disorders related to the large blood vessels in your chest. It is crucial that we perform some tests to identify the source of your problem. We will start with an ECG and some blood work, but more complex tests may be needed as well. In the meantime, I strongly recommend that you stop using cocaine, since use of this drug can lead to a variety of medical problems, including heart attacks. Do you have any questions for me?
USMLE STEP 2 CS Patient Note
History
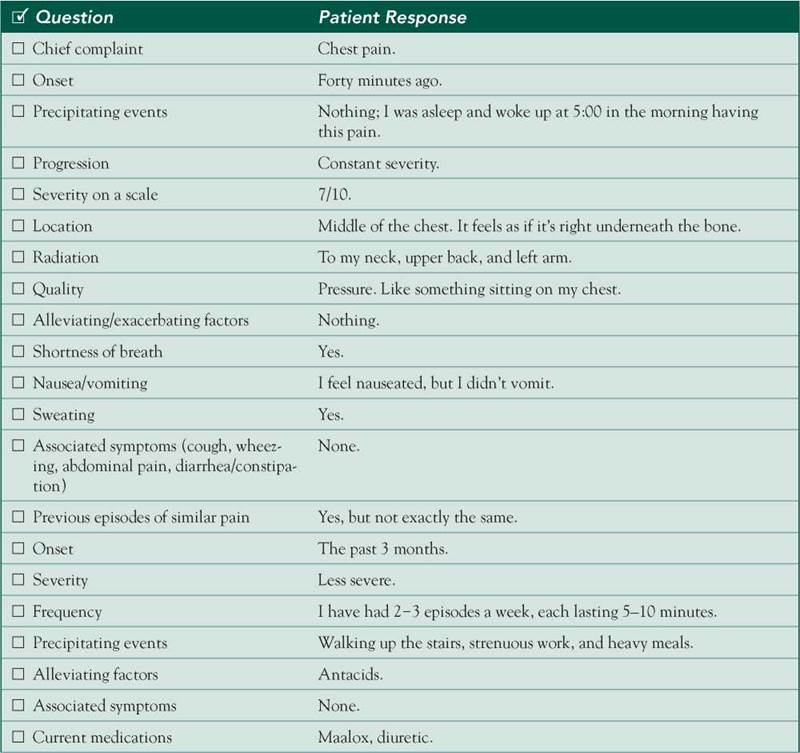
HPI: 46 yo M c/o substernal chest pain. The pain started 40 minutes before the patient presented to the ED. The pain woke the patient from sleep at 5:00 a.m. with a steady 7/10 pressure sensation in the middle of his chest that radiated to the left arm, upper back, and neck. Nothing makes it worse or better. Nausea, sweating, and dyspnea are also present. Similar episodes have occurred during the past 3 months, 2-3 times/week. These episodes were precipitated by walking up the stairs, strenuous work, sexual intercourse, and heavy meals. Pain during these episodes was less severe, lasted for 5-10 minutes, and disappeared spontaneously or after taking antacids.
ROS: Negative except as above.
Allergies: NKDA.
Medications: Maalox, diuretic.
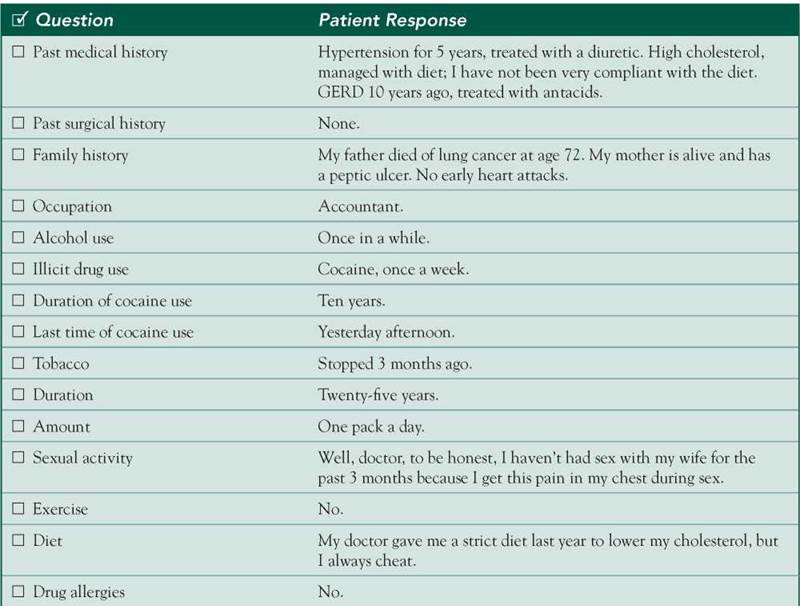
PMH: Hypertension for 5 years, treated with a diuretic. High cholesterol, managed with diet. GERD 10 years ago, treated with antacids.
SH: 1 PPD for 25 years; stopped 3 months ago. Occasional EtOH, occasional cocaine for 10 years (last used yesterday afternoon). No regular exercise; poorly adherent to diet.
FH: Father died of lung cancer at age 72. Mother has peptic ulcers. No early coronary disease.
Physical Examination
Patient is in severe pain.
VS: BP 165/85 mm Hg (both arms), RR 22/minute.
Neck: No JVD, no bruits.
Chest: No tenderness, clear symmetric breath sounds bilaterally.
Heart: Apical impulse not displaced; RRR; normal S1/S2; no murmurs, rubs, or gallops.
Abdomen: Soft, nondistended, nontender, © BS, no hepatosplenomegaly Extremities: No edema, peripheral pulses 2+ and symmetric.
Differential Diagnosis
CASE DISCUSSION
Patient Note Differential Diagnoses
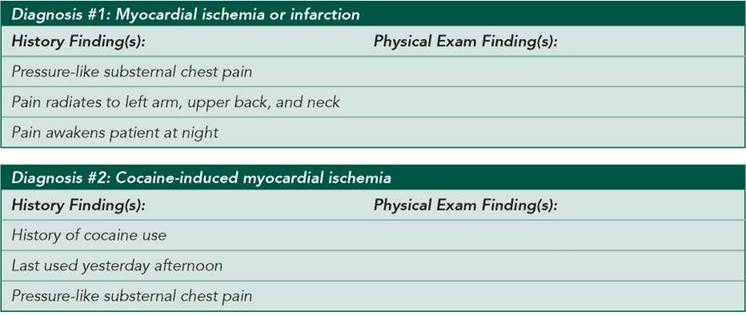
■ Myocardial ischemia or infarction: The patient has multiple cardiac risk factors, including smoking, hypertension, and hyperlipidemia, and his symptoms are classic for cardiac ischemia.
■ Cocaine-induced myocardial ischemia: Cocaine can predispose to premature atherosclerosis and can induce myocardial ischemia and infarction either by causing coronary artery vasoconstriction or by increasing myocardial energy requirements.
■ GERD: Severe chest pain is atypical but not uncommon for GERD and may worsen with recumbency overnight. Other atypical symptoms include chronic cough, wheezing, and dysphagia. The classic symptom of GERD is heartburn, which may be exacerbated by meals.
Additional Differential Diagnoses
■ Aortic dissection: With the sudden onset of severe chest pain, aortic dissection should be suspected given the high potential for death if missed (and the potential for harm if mistaken for acute MI and treated with thrombolytic therapy). However, the patient’s pain is not the classic sudden, tearing chest pain that radiates to the back. In addition, his peripheral pulses and blood pressures are not diminished or unequal, and there is no aortic regurgitant murmur (although physical exam findings have poor sensitivity and specificity to diagnose aortic dissection).
■ Pericarditis: The absence of pain that changes with position or respiration and the absence of a pericardial friction rub make pericarditis less likely.
■ Pneumothorax: This diagnosis should be considered in a patient with acute chest pain and difficulty breathing, but it is less likely in this case given that breath sounds are symmetric.
■ Pulmonary embolism: As above, this is on the differential for acute chest pain and difficulty breathing, but this patient has no apparent risk factors for pulmonary embolism.
■ Costochondritis (or other musculoskeletal chest pain): This is more typically associated with pain on palpation or pleuritic pain.
Diagnostic Workup
■ ECG: Acute myocardial ischemia, infarction, and pericarditis have characteristic changes on ECG.
■ Cardiac enzymes (CPK, CPK-MB, troponin): Specific tests for myocardial tissue necrosis that can turn positive as early as 4-6 hours after onset of pain.
■ Transthoracic echocardiography (TTE): Can demonstrate segmental wall motion abnormalities in suspected acute MI (infarction is unlikely in the absence of wall motion abnormalities).
■ Upper endoscopy: Can be used to document tissue damage characteristic of GERD. However, it can be normal in up to one-half of symptomatic patients; esophageal probe (pH and manometry measurements) together with endoscopic visualization constitutes an effective diagnostic technique.
■ Urine toxicology: To help confirm the patient’s history of recent cocaine use.
■ Cardiac catheterization: Can diagnose and treat coronary artery disease.
■ Transesophageal echocardiography (TEE): Highly specific and sensitive for aortic dissection, and can be done rapidly at the bedside.
■ CXR: A widened mediastinum suggests aortic dissection and may reveal other causes of chest pain, including pneumothorax and pneumonia.
■ CT—chest with IV contrast: Another rapidly available diagnostic study that can rule out aortic dissection or pulmonary embolism.
■ Cholesterol panel: Can identify a critical risk factor for cardiovascular disease.