DOORWAY INFORMATION
Opening Scenario
Kathleen Moore, a 33-year-old female, comes to the clinic complaining of knee pain.
Vital Signs
BP: 130/80 mm Hg Temp: 99.9°F (37.7°C)
RR: 16/minute HR: 76/minute, regular
Examinee Tasks
1. Take a focused history.
2. Perform a focused physical exam (do not perform rectal, genitourinary, or female breast exam).
3. Explain your clinical impression and workup plan to the patient.
4. Write the patient note after leaving the room.
Checklist/SP Sheet
Patient Description
Patient is a 33 yo F, divorced with 2 daughters.
Notes for the SP
■ Pretend to have pain when the examinee moves your left knee in all directions.
■ Do not allow the examinee to fully flex or extend your left knee.
■ Paint your left knee red to make it look inflamed.
Challenging Questions to Ask
“Do you think I will be able to walk on my knee like before?”
Sample Examinee Response
“Most likely, but that depends on the underlying problem and your response to treatment. I need to perform a physical examination before we can figure out an appropriate course of treatment.”
Examinee Checklist
Building the Doctor-Patient Relationship Entrance
□ Examinee knocked on the door before entering.
□ Examinee introduced self by name.
□ Examinee identified his/her role or position.
□ Examinee correctly used patient’s name.
□ Examinee made eye contact with the SP.
Reflective Listening
□ Examinee asked an open-ended question and actively listened to the response.
□ Examinee asked the SP to list his/her concerns and listened to the response without interrupting.
□ Examinee summarized the SP’s concerns, often using the SP’s own words.
Information Gathering
□ Examinee elicited data efficiently and accurately.
Connecting with the Patient
□ Examinee recognized the SP’s emotions and responded with PEARLS.
Physical Examination
□ Examinee washed his/her hands.
□ Examinee asked permission to start the exam.
□ Examinee used respectful draping.
□ Examinee did not repeat painful maneuvers.
Closure
□ Examinee discussed initial diagnostic impressions.
□ Examinee discussed initial management plans:
□ Follow-up tests: Examinee mentioned the need for a pelvic exam.
□ Examinee discussed safe sex practices.
□ Examinee asked if the SP had any other questions or concerns.
Sample Closure
Ms. Moore, there are a few things that could be causing your knee pain, such as gout, an infection, or rheumatoid arthritis. To find out, I would like to obtain fluid from your knee and then draw some blood. Sometimes infections from the pelvis can spread to other parts of your body, such as your knee, and for that reason I would also like to do a pelvic exam. These tests will likely reveal the source of your pain. You mentioned earlier that you don’t always use condoms. I know condoms may be difficult to use regularly, but they are important in helping control the spread of STDs. Do you have any questions for me?
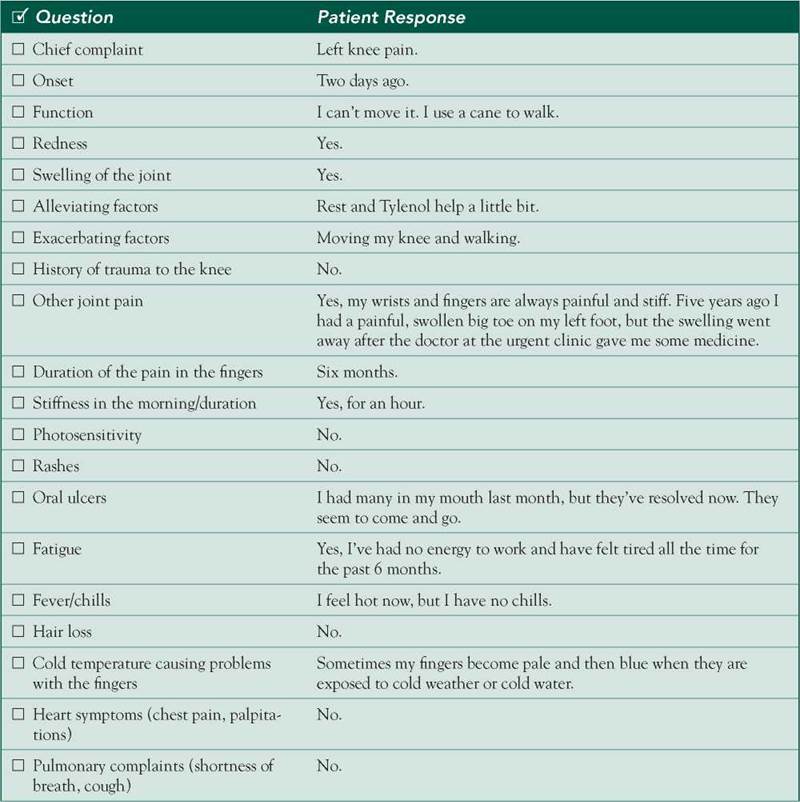
History
HPI: 33 yo F c/o left knee pain that started 2 days ago and is causing difficulty walking. She has swelling and redness in her left knee and mild fever but no chills. She denies trauma. She has a history of fatigue and painful wrists and fingers and has experienced 1-hour morning stiffness over the past 6 months. She also recalls multiple oral ulcers that resolved last month. She describes Raynaud's phenomenon but denies rash, photosensitivity, hair loss, or recent tick bites. She recalls a 10-lb weight loss over the past 6 months and has no appetite.
ROS: Negative except as above.
Allergies: NKDA.
Medications: Tylenol.
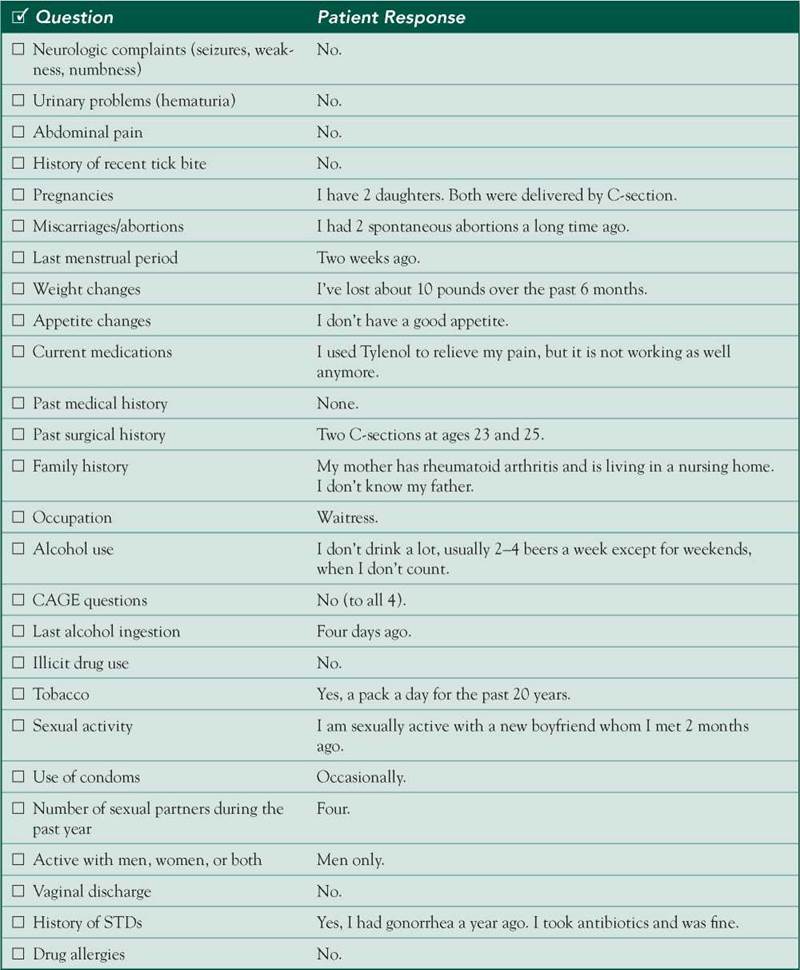
PMH: Episode of acute left big toe arthritis 5 years ago; gonorrhea 1 year ago.
PSH: Two C-sections, 2 spontaneous abortions.
SH: 1 PPD for 20 years. Usually drinks 2-4 beers/week; on weekends drinks more; last ingestion 4 days ago; CAGE 0/4. No illicit drugs. Sexually active with multiple partners; inconsistent condom use.
FH: Mother has rheumatoid arthritis and lives in a nursing home.
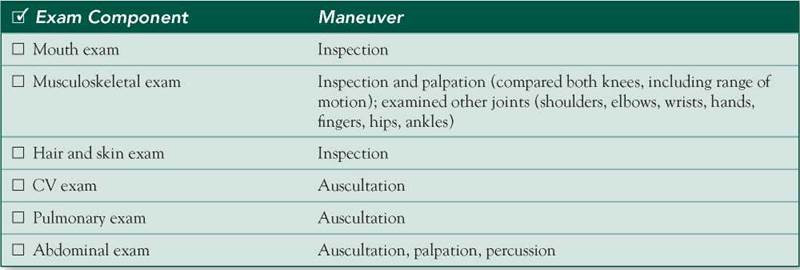
Physical Examination
Patient is in no acute distress but favors the left knee.
VS: WNL except for low-grade fever.
HEENT: No oral lesions.
Chest: Clear breath sounds bilaterally.
Heart: RRR; normal S1/S2; no murmurs, rubs, or gallops.
Abdomen: Soft, nondistended,![]() BS, no hepatosplenomegaly
BS, no hepatosplenomegaly
Extremities: Erythema, tenderness, pain, and restricted range of motion on flexion and extension of left knee compared to right knee.![]() swelling at left knee. Fingers and hands with stiffness bilaterally. Shoulder, elbow, wrist, hip, and ankle joints WNL bilaterally.
swelling at left knee. Fingers and hands with stiffness bilaterally. Shoulder, elbow, wrist, hip, and ankle joints WNL bilaterally.
Differential Diagnosis

CASE DISCUSSION
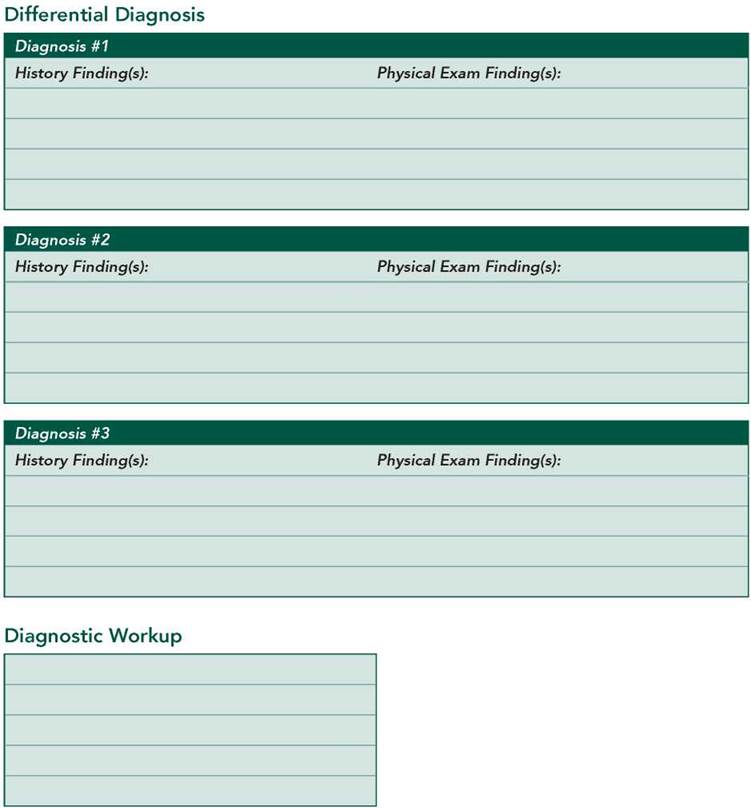
Patient Note Differential Diagnoses
■ Gout: This acute, usually monoarticular, crystal-induced arthritis rarely occurs in premenopausal women, but the patient’s history of first MTP arthritis (“podagra”) is classic for gout. Alcohol ingestion causes hyperuricemia and may precipitate an acute attack. Foot, ankle, and knee joints are also commonly affected. Gout does not explain her hand arthralgias, but osteoarthritis is common and may coexist.
■ Rheumatoid arthritis (RA): This is suggested in a patient with a positive family history, symmetric small joint arthritis (eg, fingers, wrists), prolonged morning stiffness, and systemic symptoms (low-grade fever, anorexia, weight loss, fatigue, and weakness). However, this patient’s hand joints were not red, warm, swollen, or tender on exam. Monoarthritis is also uncommon but is occasionally seen early in the course of the disease.
■ Systemic lupus erythematosus (SLE): Joint symptoms (usually symmetric peripheral arthralgias), constitutional symptoms, and Raynaud’s phenomenon may be early manifestations of this disease. Unilateral knee involvement is not typical. The diagnosis requires at least four of the following 11 criteria: malar (“butterfly”) rash, discoid rash, symmetric arthritis, photosensitivity, oral ulcers, serositis, renal disease, CNS involvement, hematologic disorders (her fatigue may be due to anemia), immunologic abnormalities (her history of spontaneous abortions may signal the presence of antiphospholipid antibodies), or ANA positivity. More testing needs to be done before SLE can be diagnosed in this case.
Additional Differential Diagnoses
■ Pseudogout: Another crystal-induced arthritis, pseudogout frequently involves the knees and wrists but is usually seen in patients older than 60 years of age.
■ Gonococcal septic arthritis: This occurs in healthy hosts, most commonly young women (women are much more likely than men to have asymptomatic genitourinary gonococcal infection, which allows the bacteria to mutate and disseminate). The knee is the most frequently involved joint, but the monoarthritis (or tenosynovitis) is usually preceded by a few days of migratory polyarthralgias. Also, this patient does not have the characteristic rash, which consists of small necrotic pustules on the extremities (including the palms and soles).
■ Nongonococcal septic arthritis: This occurs suddenly, usually affects the knee or wrist, and is most commonly caused by S aureus. However, it is a disease of an abnormal host; previous joint damage and IV drug use are key risk factors not present in this case.
■ Osteoarthritis: Onset is insidious, joint stiffness brief, and joint inflammation minimal, all of which are incongruent with this patient’s presentation. Also, osteoarthritis spares the wrist and MCP joints and is not associated with constitutional symptoms.
Diagnostic Workup
■ CBC: To look for anemia, leukopenia, and/or thrombocytopenia in SLE or for leukocytosis in acute gout and septic arthritis.
■ Immunologic tests: ANA is a highly sensitive but nonspecific screening test for SLE. A negative test essentially excludes the disease. If ANA is positive, antibody against double-stranded DNA (anti-dsDNA), antibody against the Smith antigen, anticardiolipin antibodies, and lupus anticoagulant should be investigated to help confirm the diagnosis of SLE. RF is present in > 75% of patients with RA. Anti-cyclic citrullinated peptide (anti-CCP) antibody has high specificity (up to 96%) for RA and is frequently sent when RA is suspected as the diagnosis.
■ Knee aspiration, Gram stain, culture, and inspection for crystals: In most cases of acute monoarthritis, joint aspiration must be performed to rule out septic arthritis. Inflammatory joint synovial fluid contains > 3000 WBCs/L, and septic joint fluid often contains > 50,000 cells/L. The demonstration of needle-shaped, negatively birefringent crystals or rhomboid-shaped, weakly positively birefringent crystals confirms gout or pseudogout, respectively.
■ XR—left knee and both hands: Specific changes in RA include symmetric joint space narrowing, marginal bony erosions, and periarticular demineralization. However, x-rays are usually normal during the first six months of illness. In gout, look for punched-out cortical erosions and a sclerotic joint margin. In pseudogout, look for calcified articular cartilage (“chondrocalcinosis”). In osteoarthritis, look for joint space narrowing, marginal osteophytes, subchondral osteosclerosis, and occasionally subchondral cysts.
■ Pelvic exam and cervical cultures: Necessary to investigate gonococcal infection and often positive in the absence of symptoms (urine, anorectal, and throat cultures may also be necessary).
■ Blood culture: An important test in septic arthritis if systemic symptoms are present.