
Pyoderma Gangrenosum (PG) ICD-9: 686.01 ![]() ICD-10:L88
ICD-10:L88 ![]()
![]() PG is an idiopathic, either acute or chronic, severely debilitating skin disease.
PG is an idiopathic, either acute or chronic, severely debilitating skin disease.
![]() It is characterized by neutrophilic infiltration, destruction of tissue, and ulceration.
It is characterized by neutrophilic infiltration, destruction of tissue, and ulceration.
![]() It occurs most commonly in association with a systemic disease, especially arthritis, inflammatory bowel disease, hematologic dyscrasias, and malignancy, but may also occur alone.
It occurs most commonly in association with a systemic disease, especially arthritis, inflammatory bowel disease, hematologic dyscrasias, and malignancy, but may also occur alone.
![]() Characterized by the presence of painful, irregular, boggy, blue-red ulcers with undermined borders and purulent necrotic bases.
Characterized by the presence of painful, irregular, boggy, blue-red ulcers with undermined borders and purulent necrotic bases.
![]() There is no laboratory test that establishes the diagnosis.
There is no laboratory test that establishes the diagnosis.
![]() The mainstays of treatment are immunosuppressive or modulating agents.
The mainstays of treatment are immunosuppressive or modulating agents.
![]() Relapses occur in most patients and there is significant morbidity.
Relapses occur in most patients and there is significant morbidity.
Epidemiology
Rare, prevalence unknown. All age groups affected with a peak between 40 and 60 years. Slight preponderance of females.
Etiology and Pathogenesis
Unknown. Although called pyoderma, it does not have a microbial etiology. PG is counted among the neutrophilic dermatoses because of the massive neutrophilic infiltrates within the skin.
Clinical Manifestation
Three Types. Acute. Acute onset with painful hemorrhagic pustule or painful nodule either de novo or after trauma. There is the phenomenon of pathergy, where a needle stick, insect bite, biopsy, or other minimal trauma can trigger a lesion. Chronic: slow progression with granulation and hyperkeratosis. Less painful. Bullous: true blisters often hemorrhagic and associated with hematologic disease.
Skin Lesions. Acute. Superficial hemorrhagic pustule surrounded by erythematous halo; very painful (Fig. 7-1). Breakdown occurs with ulcer formation, whereby ulcer borders are dusky-red or purple, irregular and raised, undermined, boggy with perforations that drain pus (Fig. 7-2). The base of the ulcer is purulent with hemorrhagic exudate, partially covered by necrotic eschar (Fig. 7-3), with or without granulation tissue. Pustules both at the advancing border and in the ulcer base; a halo of erythema spreads centrifugally at the advancing edge of the ulcer (Fig. 7-3). Chronic: lesions may slowly progress, grazing over large areas of the body and exhibiting massive granulation within the ulcer from the outset (Fig. 7-4) and crusting and even hyperkeratosis on the margins (Fig. 7-5). Lesions are usually solitary but may be multiple and form clusters that coalesce. Most common sites: lower extremities (Figs. 7-2 and 7-5) > buttocks > abdomen (Fig. 7-3) > face (Fig. 7-4). Healing of ulcers results in thin atrophic cribriform scars. Bullous: blisters from the outset, often hemorrhagic, followed by ulceration.

Figure 7-1. Pyoderma gangrenosum The initial lesion is a rapidly enlarging hemorrhagic nonfollicular pustule surrounded by an erythematous halo and is very painful.

Figure 7-2. Pyoderma gangrenosum Lesions rapidly break down in the center and become boggy, hemorrhagic, and purulent ulcers. Note small abscesses at base of ulcer on left leg.

Figure 7-3. Pyoderma gangrenosum A very large ulcer with raised bullous undermined borders covered with hemorrhagic and fibrinous exudate. The arrow indicates erythema surrounding advancing borders of the lesion. When the bullae are opened, pus is drained. This lesion arose acutely and spread rapidly after laparatomy for an ovarian carcinoma.

Figure 7-4. Pyoderma gangrenosum: chronic type The lesion involves the upper eyelid and represents an ulcer with elevated granulating base with multiple abscesses. The lesion later spread slowly to involve the temporal and zygomatic regions and eventually healed under systemic glucocorticoid treatment, leaving a thin cribriform scar that did not impair the function of the eyelid.

Figure 7-5. Pyoderma gangrenosum: chronic type This lesion, which appears like a plaque, spread only slowly but was also surrounded by an erythematous border. The lesion is crusted and hyperkeratotic and is less painful than the lesions in acute pyoderma gangrenosum.
Mucous Membranes. Rarely, aphthous stomatitis–like lesions; massive ulceration of oral mucosa and conjunctivae.
General Examination
Patient may appear ill.
Associated Systemic Diseases
Up to 50% of cases occur without associated disease. Remainder of cases associated with arthritis, large- and small-bowel disease (Crohn disease, ulcerative colitis), diverticulosis (diverticulitis), paraproteinemia and myeloma, leukemia, active chronic hepatitis, Behçet syndrome (which is also a disease with pathergy).
Laboratory Examinations
There is no single diagnostic test.
ESR. Variably elevated.
Dermatopathology. Not diagnostic. Neutrophilic inflammation with abscess formation and necrosis.
Diagnosis and Differential Diagnosis
Clinical findings plus history and course; confirmed by compatible dermatopathology. Differential diagnosis: ecthyma and ecthyma gangrenosum, atypical mycobacterial infection, clostridial infection, deep mycoses, amebiasis, leishmaniasis, bromoderma, pemphigus veg-etans, stasis ulcers, Wegener granulomatosis.
Course and Prognosis
Untreated, course may last months to years, but spontaneous healing can occur. Ulceration may extend rapidly within a few days or slowly. Healing occurs centrally with peripheral extension. New ulcers may appear as older lesions resolve. Pathergy.
Management
With Associated Underlying Disease. Treat underlying disease.
Systemic Treatment. High doses of oral glucocorticoids or IV glucocorticoid pulse therapy (1–2 g/d prednisolone) may be required. Sulfasalazine (particularly in cases associated with Crohn disease), sulfones, cyclosporine, and, more recently, infliximab, etanercept, adalimumab.
Topical. In singular small lesion, topical tacrolimus ointment or intralesional triamcinolone.
Sweet Syndrome (SS) ICD-9: 695.89 ![]() ICD-10: L98.2
ICD-10: L98.2 ![]()
![]() An uncommon, acute and recurrent, cytokine-induced skin reaction associated with various etiologies.
An uncommon, acute and recurrent, cytokine-induced skin reaction associated with various etiologies.
![]() Painful plaque-forming inflammatory papules, often with massive exudations giving the appearance of vesiculation (pseudovesiculation).
Painful plaque-forming inflammatory papules, often with massive exudations giving the appearance of vesiculation (pseudovesiculation).
![]() Accompanied by fever, arthralgia, and peripheral leukocytosis.
Accompanied by fever, arthralgia, and peripheral leukocytosis.
![]() Associated with infection, malignancy, or drugs.
Associated with infection, malignancy, or drugs.
![]() Treatment: systemic glucocorticoids, potassium iodide, dapsone, or colchicine.
Treatment: systemic glucocorticoids, potassium iodide, dapsone, or colchicine.
![]() Synonym: Acute febrile neutrophilic dermatosis.
Synonym: Acute febrile neutrophilic dermatosis.
Epidemiology and Etiology
Age of Onset. Most 30–60 years.
Sex. Women > men.
Etiology. Unknown, possibly hypersensitivity reaction.
Associated Disorders. Febrile upper respiratory tract infection. In some cases, associated with Yersinia infection. Hematologic malignancy; drugs: granulocyte colony-stimulating factor (G-GSF).
Clinical Manifestation
Prodromes are febrile upper respiratory tract infections. Gastrointestinal symptoms (diarrhea), tonsillitis, influenza-like illness, 1–3 weeks before skin lesions. Lesions tender/painful. Fever (not always present), headache, arthralgia, general malaise.
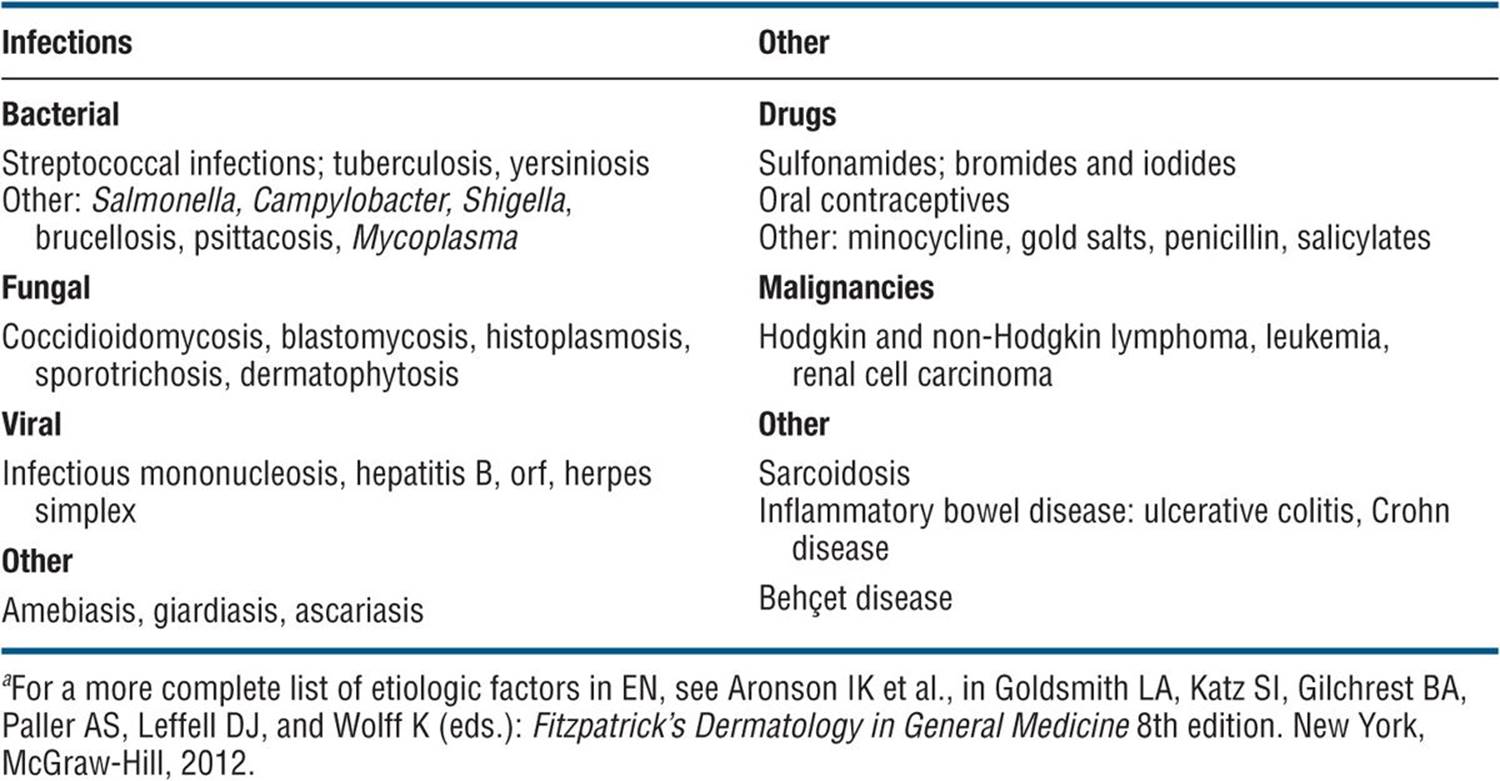
Skin Lesions. Bright red, smooth, tender papules (2–4 mm in diameter) that coalesce to form irregular, sharply bordered, inflammatory plaques (Fig. 7-6A). Pseudovesiculation: intense edema gives the appearance of vesiculation (Figs. 7-6A and 7-7A). Lesions arise rapidly, and as they evolve, central clearing may lead to annular or arcuate patterns. Tiny, superficial pustules may occur. May present as a single lesion or multiple lesions, asymmetrically or symmetrically distributed. Most common on face (Fig. 7-6A), neck (Fig. 7-6B), and upper extremities but also on lower extremities, where lesions may be deep in the fat and thus mimic panniculitis or erythema nodosum. Truncal lesions are uncommon but widespread, and generalized forms occur. If associated with leukemia, bullous lesions may occur (Fig. 7-7B) and lesions may mimic bullous PG.
Mucous Membranes. ± Conjunctivitis, episcleritis.
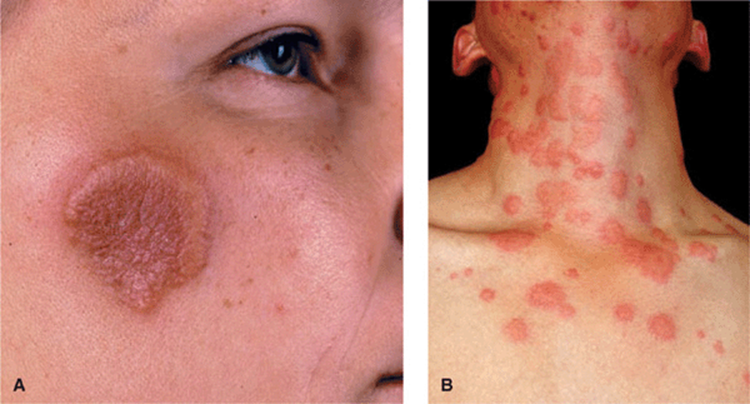
Figure 7-6. Sweet syndrome (A) An erythematous, edematous plaque that has formed from coalescing papules on the right cheek. The border of the plaque looks as if composed of vesicles, but palpation reveals that it is solid (pseudovesiculation). This lesion occurred in a 26-year-old female following an upper respiratory infection, and the patient also had fever and leukocytosis. (B) A more exanthematic eruption in a 23-year-old female. There are multiple, coalescing, inflammatory and very exudative papules with a wheal-like appearance on the neck. This patient also had leukocytosis and fever.

Figure 7-7. Sweet syndrome (A) Coalescing exudative papules that look like vesicles. Upon palpation lesions were solid. (B) Bullous type of Sweet syndrome. These are true bullae and pustules. The patient had myelomonocytic leukemia.
General Examination
Patient may appear ill. There may be involvement of cardiovascular, central nervous system, gastrointestinal, hepatic, musculoskeletal, ocular, pulmonary, renal, and splenic organs.
Laboratory Examinations
Complete Blood Count. Leukocytosis with neutrophilia (not always present).
ESR. Elevated.
Dermatopathology. Diagnostic. Epidermis usually normal, sometimes subcorneal pustulation. Massive edema of papillary body, dense leukocytic infiltrate with starburst pattern in mid-dermis, consisting of neutrophils with occasional eosinophils/lymphoid cells. Leukocytoclasia, nuclear dust, but no vasculitis. ± Neutrophilic infiltrates in subcutaneous tissue.
Diagnosis and Differential Diagnosis
Clinical impression and by histopathology.
Differential Diagnosis. Erythema multiforme, erythema nodosum, prevesicular herpes simplex infection, preulcerative PG.
Course and Prognosis
Untreated, lesions enlarge over a period of days or weeks and eventually resolve without scarring. Recurrences occur in 50% of patients, often in previously involved sites. Some cases follow Yersiniainfection or are associated with acute myelocytic leukemia, transient myeloid proliferation, various malignant tumors, ulcerative colitis, benign monoclonal gammopathy; some follow drug administration, most commonly by GSF.
Management
Rule out sepsis.
Prednisone: 30–50 mg/d, tapering in 2–3 weeks lesions resolve within a few days; some, but not all, patients respond to dapsone, 100 mg/d, or to potassium iodide. Some to colchicine.
Antibiotic Therapy. Clears eruption in Yersinia-associated cases; in all other cases, antibiotics are ineffective.
Granuloma Faciale (GF) ICD-9: 686.1 ![]() ICD-10: L92.2
ICD-10: L92.2![]()
![]() A rare, localized inflammatory disease of unknown etiology, clinically characterized by reddish-brown papules or small plaques primarily in the face.
A rare, localized inflammatory disease of unknown etiology, clinically characterized by reddish-brown papules or small plaques primarily in the face.
![]() Single or multiple lesions with characteristic orange peel-like surface (Fig. 7-8).
Single or multiple lesions with characteristic orange peel-like surface (Fig. 7-8).
![]() Histologically, chronic leukocytoclastic vasculitis with eosinophils, fibrin deposition, and fibrosis.
Histologically, chronic leukocytoclastic vasculitis with eosinophils, fibrin deposition, and fibrosis.
![]() Therapy: topical glucocorticoids; dapsone.
Therapy: topical glucocorticoids; dapsone.

Figure 7-8. Granuloma faciale: classic presentation A single, sharply defined, brown plaque with a characteristic orange peel-like surface.
Erythema Nodosum (EN) Syndrome ICD-9: 695.2 ![]() ICD-10: L52
ICD-10: L52 ![]()
![]() EN is an important and common acute inflammatory/immunologic reaction pattern of the subcutaneous fat.
EN is an important and common acute inflammatory/immunologic reaction pattern of the subcutaneous fat.
![]() Characterized by the appearance of painful nodules on the lower legs.
Characterized by the appearance of painful nodules on the lower legs.
![]() Lesions are bright red and flat but nodular upon palpation.
Lesions are bright red and flat but nodular upon palpation.
![]() Often fever and arthritis.
Often fever and arthritis.
![]() Multiple and diverse etiologies.
Multiple and diverse etiologies.
The most common type of panniculitis, with a peak incidence at 20–30 years, but any age may be affected. Three to six times more common in females than in males.
Etiology. EN is cutaneous reaction pattern to various etiologic agents. These include infections, drugs, and other inflammatory/granulomatous diseases, notably sarcoidosis (Table 7-1).
TABLE 7-1 CAUSES OF ERYTHEMA NODOSUMa
Clinical Manifestation
Painful, tender lesions, usually of a few days’ duration, accompanied by fever, malaise, and arthralgia (50%), most frequently of ankle joints. Other symptoms depending on etiology.
Skin Lesions. Indurated, very tender nodules (3–20 cm), not sharply marginated (Fig. 7-9), deep seated in the subcutaneous fat, mostly on the anterior lower legs, bilateral but not symmetric. Nodules are bright to deep red and are appreciated as such only upon palpation. The term erythema nodosum best describes the skin lesions: they look like erythema but feel like nodules (Fig. 7-9). Lesions are oval, round, arciform; as they age, they become violaceous, brownish, yellowish, green, like resolving hematomas. Lesions may also occur on knees and arms but only rarely on the face and on the neck.

Figure 7-9. Erythema nodosum Indurated, very tender, inflammatory nodules mostly in the pretibial region. Lesions are seen as red, ill-defined erythemas but palpated as deep-seated nodules, hence the designation. In this 49-year-old female, there was also fever and arthritis of the ankle joints following an upper respiratory tract infection. The throat cultures yielded β-hemolytic streptococci.
Laboratory Examinations
Hematology. Elevated ESR and C-reactive protein; leukocytosis.
Bacterial Culture. Culture throat for group A β-hemolytic streptococcus, stool for Yersinia.
Imaging. Radiologic examination of the chest and gallium scan are important to rule out or prove sarcoidosis.
Dermatopathology. Acute (polymorphonuclear) and chronic (granulomatous) inflammation in the subcutis, around blood vessels in the septum and adjacent fat. EN is a septal panniculitis.
Course
Spontaneous resolution occurs in 6 weeks, with new lesions erupting during that time. Course depends on the etiology. Lesions never break down or ulcerate and heal without scarring.
Diagnosis and Differential Diagnosis
Diagnosis rests on clinical criteria, and histopathology if needed. Differential diagnosis includes all other forms of panniculitis, panarteritis nodosa, nodular vasculitis, pretibial myxedema, nonulcerated gumma, and lymphoma.
Management
Symptomatic. Bed rest or compressive bandages (lower legs), wet dressings.
Anti-inflammatory Treatment. Salicylates, nonsteroidal anti-inflammatory drugs. Systemic glucocorticoids—response is rapid, but their use is indicated only when the etiology is known and infectious agents are excluded.
Other Panniculitides ICD-9: 729.3 ![]() ICD-10: M79.3
ICD-10: M79.3 ![]()
![]() Panniculitis is the term used to describe diseases where the major focus of inflammation is in the subcutaneous tissue. In general, panniculitis presents as an erythematous or violaceous nodule in the subcutaneous fat that may be tender or not, that may ulcerate or heal without scarring, and that may be soft or hard on palpation. Thus, the term panniculitis describes a wide spectrum of disease manifestations.
Panniculitis is the term used to describe diseases where the major focus of inflammation is in the subcutaneous tissue. In general, panniculitis presents as an erythematous or violaceous nodule in the subcutaneous fat that may be tender or not, that may ulcerate or heal without scarring, and that may be soft or hard on palpation. Thus, the term panniculitis describes a wide spectrum of disease manifestations.
![]() An accurate diagnosis requires an ample deep skin biopsy that should reach down to or even beyond the fascia. The panniculitides are classified histologically as lobular or septal but a clear separation is often not possible. A simplified classification of panniculitis is given in Table 7-2.
An accurate diagnosis requires an ample deep skin biopsy that should reach down to or even beyond the fascia. The panniculitides are classified histologically as lobular or septal but a clear separation is often not possible. A simplified classification of panniculitis is given in Table 7-2.
![]() Only two forms of panniculitis are briefly discussed here.* Other diseases in which panniculitis occurs are referred to in Table 7-2.
Only two forms of panniculitis are briefly discussed here.* Other diseases in which panniculitis occurs are referred to in Table 7-2.
![]() Pancreatic panniculitis also manifests as painful erythematous nodules and plaques that may fluctuate and occur at any site, with a predilection for abdomen, buttocks, legs (Fig. 7-10). Frequently accompanied by arthritis and polyserositis. Associated with pancreatitis or pancreatic carcinoma. In middle-aged to elderly individuals, males > females. History: alcoholism, abdominal pain, weight loss, or recent-onset diabetes mellitus. Skin biopsy reveals lobular panniculitis; liquefied fat may drain from the biopsy site. General examination may reveal pleural effusion, ascites, and arthritis, particularly of the ankles. Laboratory: eosinophilia, hyperlipasemia, hyperamylasemia, and increased excretion of amylase and/or lipase in the urine. The pathophysiology is probably a breakdown of subcutaneous fat caused by pancreatic enzymes released into the circulation. Course and prognosis depend on the type of pancreatic disease. Treatment is directed at the underlying pancreatic disorder.
Pancreatic panniculitis also manifests as painful erythematous nodules and plaques that may fluctuate and occur at any site, with a predilection for abdomen, buttocks, legs (Fig. 7-10). Frequently accompanied by arthritis and polyserositis. Associated with pancreatitis or pancreatic carcinoma. In middle-aged to elderly individuals, males > females. History: alcoholism, abdominal pain, weight loss, or recent-onset diabetes mellitus. Skin biopsy reveals lobular panniculitis; liquefied fat may drain from the biopsy site. General examination may reveal pleural effusion, ascites, and arthritis, particularly of the ankles. Laboratory: eosinophilia, hyperlipasemia, hyperamylasemia, and increased excretion of amylase and/or lipase in the urine. The pathophysiology is probably a breakdown of subcutaneous fat caused by pancreatic enzymes released into the circulation. Course and prognosis depend on the type of pancreatic disease. Treatment is directed at the underlying pancreatic disorder.
![]() α1-Antitrypsin-deficiency panniculitis is also characterized by recurrent tender, erythematous, subcutaneous nodules ranging from 1 to 5 cm and located predominantly on the trunk and the proximal extremities. Nodules break down and discharge a clear serous or oily fluid. Diagnosis is substantiated by a decrease of serum α1- antitrypsin, and treatment consists of oral dapsone in doses up to 200 mg/d. The intravenous infusion of human α1-proteinase inhibitor concentrate has been shown to be very effective.
α1-Antitrypsin-deficiency panniculitis is also characterized by recurrent tender, erythematous, subcutaneous nodules ranging from 1 to 5 cm and located predominantly on the trunk and the proximal extremities. Nodules break down and discharge a clear serous or oily fluid. Diagnosis is substantiated by a decrease of serum α1- antitrypsin, and treatment consists of oral dapsone in doses up to 200 mg/d. The intravenous infusion of human α1-proteinase inhibitor concentrate has been shown to be very effective.
*The reader is also referred to Aronson IK et al., in Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, and Wolff K (eds.): Fitzpatrick’s Dermatology in General Medicine 8th edition. New York, McGraw-Hill, 2012.
TABLE 7-2 SIMPLIFIED CLASSIFICATION OF PANNICULITIS
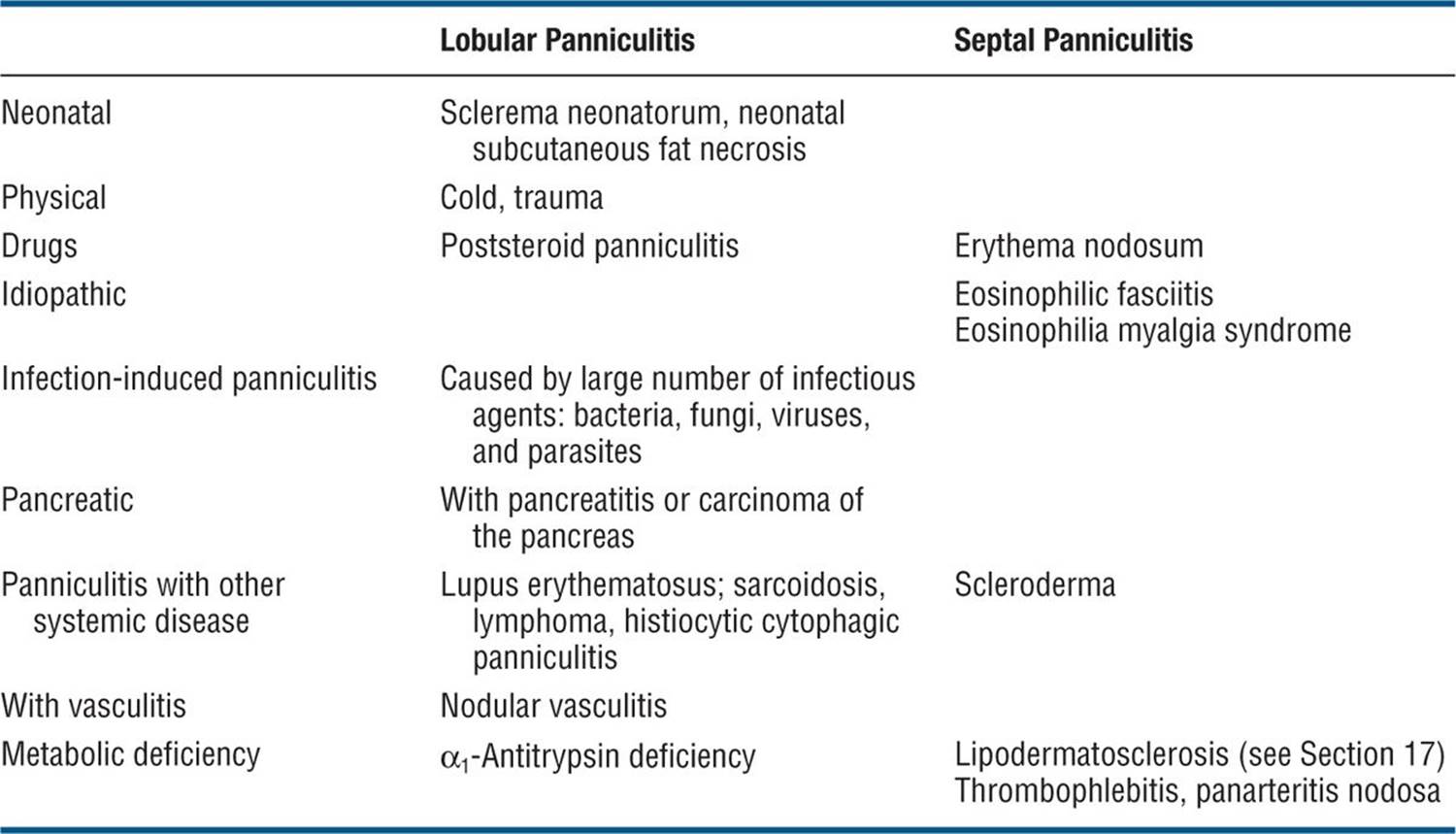

Figure 7-10. Pancreatic panniculitis There are multiple, painful, erythematous nodules and plaques that fluctuate on the lower extremities, but similar lesions were also found on the trunk and on the buttocks.