DEFINITIONS AND EPIDEMIOLOGY
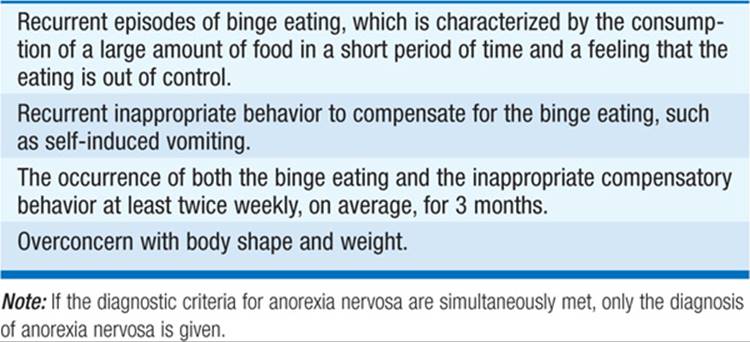
Anorexia nervosa is characterized by refusal to maintain normal body weight, resulting in a body weight <85% of the expected weight for age and height. Bulimia nervosa is characterized by recurrent episodes of binge eating followed by abnormal compensatory behaviors, such as self-induced vomiting, laxative abuse, or excessive exercise. Weight is in the normal range or above. Binge eating disorder is similar to bulimia nervosa but lacks the compensatory behavior element. As a result, binge eating disorder is typically associated with obesity.
Both anorexia nervosa and bulimia nervosa occur primarily among previously healthy young women who become overly concerned with body shape and weight. Binge eating and purging behavior may be present in both conditions, with the critical distinction between the two resting on the weight of the individual. The lifetime prevalence of anorexia nervosa is 1%, that of bulimia nervosa 1–3%, but mild forms of occasional bulimia may occur in up to 5–10% of women. Binge eating disorder has a 4% prevalence. There is a 10:1 female to male ratio for both conditions; binge eating disorder is more evenly divided between women and men (2:1). The typical time of onset of anorexia is mid-adolescence, that of bulimia in early adulthood. Both can occur later, but onset is uncommon after age 40.
Anorexia and bulimia nervosa are disorders of the affluent, well-educated societies in Western cultures. Affected pts frequently exhibit perfectionist and obsessional tendencies. Pursuit of activities that emphasize thinness (ballet, modeling, distance running) are prevalent, as is a drive for high scholastic achievement. Risk factors are a family history of mood disturbance, childhood obesity, and psychological or physical abuse during childhood.
The diagnostic features of anorexia and bulimia nervosa are shown in Tables 210-1 and 210-2.
TABLE 210-1 DIAGNOSTIC FEATURES OF ANOREXIA NERVOSA
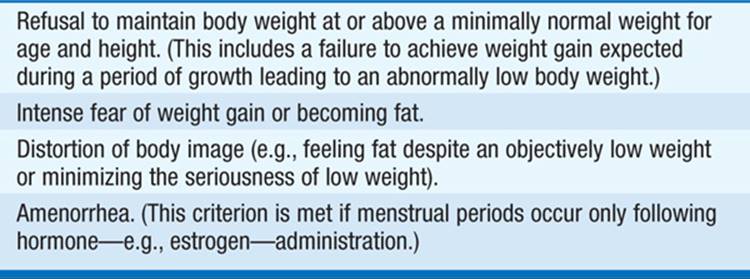
TABLE 210-2 DIAGNOSTIC FEATURES OF BULIMIA NERVOSA
CLINICAL FEATURES
Anorexia Nervosa
• General: feeling cold
• Skin, hair, nails: alopecia, lanugo hair, acrocyanosis, edema
• Cardiovascular: bradycardia, hypotension
• Gastrointestinal: salivary gland enlargement, slow gastric emptying, constipation, elevated liver enzymes
• Hematopoietic: normochromic, normocytic anemia; leukopenia
• Fluid/electrolyte: increased blood urea nitrogen, increased creatinine, hyponatremia, hypokalemia. Hypokalemia can become life-threatening.
• Endocrine: low luteinizing hormone and follicle-stimulating hormone with secondary amenorrhea, hypoglycemia, normal thyroid-stimulating hormone with low normal thyroxine, increased plasma cortisol, osteopenia
Bulimia Nervosa
• Gastrointestinal: salivary gland enlargement, dental erosion from gastric acid exposure
• Fluid/electrolyte: hypokalemia, hypochloremia, alkalosis (from vomiting) or acidosis (from laxative abuse)
• Other: callus or scar on dorsum of hand (from repeated scraping against teeth during induced vomiting)
TREATMENT Eating Disorders
ANOREXIA NERVOSA Weight restoration to 90% of predicted weight (BMI >18.5 kg/m2) is the primary goal in the treatment of anorexia nervosa. The intensity of the initial treatment, including the need for hospitalization, is determined by the pt’s current weight, the rapidity of recent weight loss, and the severity of medical and psychological complications (Fig. 210-1). Severe electrolyte imbalances should be identified and corrected. Nutritional restoration can almost always be successfully accomplished by oral feeding. For severely underweight pts, sufficient calories should be provided initially in divided meals as food or liquid supplements to maintain weight and to permit stabilization of fluid and electrolyte balance (1200–1800 kcal/d intake). Calories can be gradually increased to achieve a weight gain of 1–2 kg per week (3000–4000 kcal/d intake). Meals must be supervised. Intake of vitamin D (400 IU/d) and calcium (1500 mg/d) should be sufficient to minimize bone loss. The assistance of psychiatrists or psychologists experienced in the treatment of anorexia nervosa is usually necessary. No psychotropic medications are of established value in the treatment of anorexia nervosa. Medical complications occasionally occur during refeeding; most pts transiently retain excess fluid, occasionally resulting in peripheral edema. Congestive heart failure and acute gastric dilatation have been described when refeeding is rapid. Transient modest elevations in serum levels of liver enzymes occasionally occur. Low levels of magnesium and phosphate should be replaced. Mortality is 5% per decade, from either chronic starvation or suicide.
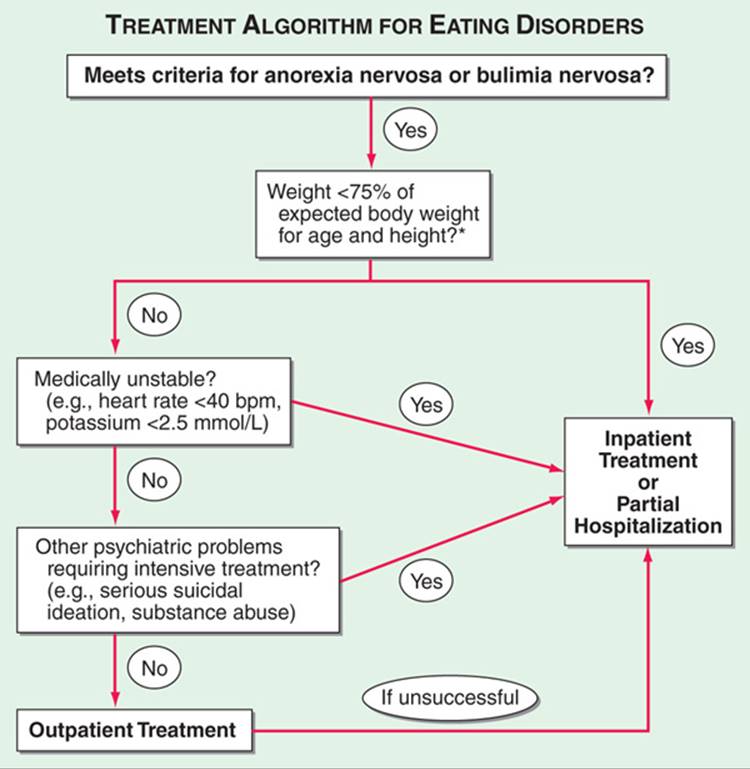
FIGURE 210-1 An algorithm for basic treatment decisions regarding pts with anorexia nervosa or bulimia nervosa. Based on the American Psychiatric Association practice guidelines for the treatment of pts with eating disorders. *Although outpatient management may be considered for pts with anorexia nervosa weighing more than 75% of expected, there should be a low threshold for using more intensive interventions if the weight loss has been rapid or if current weight is <80% of expected.
BULIMIA NERVOSA Bulimia nervosa can usually be treated on an out-patient basis (Fig. 210-1). Cognitive behavioral therapy and fluoxetine (Prozac) are first-line therapies. The recommended treatment dose for fluoxetine (60 mg/d) is higher than that typically used to treat depression.
PROGNOSIS
The prognosis of anorexia nervosa is variable. Full recovery is seen in 25–50% of pts, but many have persistent difficulties with weight maintenance, depression, and eating disturbances, including bulimia. Mortality is 5% per decade, from starvation, electrolyte abnormalities, or suicide. Bulimia nervosa has a more benign outcome. Full recovery occurs in ~50% of pts within 10 years; 25% have persistent bulimia, but mortality is low.

For a more detailed discussion, see Walsh TB, Attia E: Eating Disorders, Chap. 79, p. 636, in HPIM-18.