Setting: office
CC: “I want a PSA!”
VS: normal
HPI: The 51-year-old chairman of medicine of your hospital comes to be screened for prostate cancer. He is asymptomatic.
PMHx/Medications: none
PE: normal
What screening test lowers mortality for prostate cancer?
a. None
b. Prostate specific antigen (PSA) above age 40 years
c. PSA above age 50 years
d. Digital rectal examination
Answer a. None
PSA should not be routinely done. It does not lower mortality and does not improve a patient’s quality of life. In fact, it worsens quality of life. The PSA has been changed to a “D” recommendation, which is “Recommend against.” The PSA results in prostatectomy and radiation that damages erectile function and urinary continence without preventing metastases.
You and the patient acknowledge all this (as does the author of this book). They understand the risk of unnecessary procedures and the lack of clear efficacy, yet the patient still wants the PSA test.
Initial Orders:
![]() PSA
PSA
Do not forget the screening colonoscopy at age 50!
Finasteride and dutasteride have been shown to decrease the risk of prostate cancer on biopsy, but still do not lower mortality or prevent metastatic disease. What is the reason?
a. Tachyphylaxis—they wear off over time.
b. They suppress only small stage A1 cancers.
c. They only work on benign prostatic hyperplasia (BPH).
d. They cannot be used as single agents.
e. Adverse effects lead to discontinuation.
Answer b. They suppress only small stage A1 cancers.
Finasteride and dutasteride are medications that do decrease the overall number of prostate cancers. However, they have been shown to have no effect on larger cancers that have the propensity to grow and metastasize. They only suppress small, early stage A1 prostate cancer that would not have metastasized or grown.
Finasteride
• Small cancers are suppressed.
• Larger cancers present later.
The patient wants to know what to do about using finasteride. You tell him that it definitely will not help him. He still wants the finasteride to prevent prostate cancer.
What do you tell him?
a. Give him the finasteride.
b. Refuse to give it to him.
c. Refer this patient to another physician in another department such as urology to give it to him.
Answer b. Refuse to give it to him.
There is a difference between allowing the PSA, which is a subject of controversy that had been recommended before, and allowing finasteride. There is no benefit of using finasteride in preventing prostate cancer and, in fact, because it suppresses the rate of rise of PSA, can mask the diagnosis of larger prostate cancers until they are more widely spread.
Patients do not have a right to therapy you feel is useless.
Finasteride and Dutasteride
• They block 5-alpha-reductase.
• They block production of dihydrotestosterone.
• Dihydrotestosterone stimulates prostate growth.
Finasteride treats benign prostatic hypertrophy not cancer.
The patient returns in a week for results:
![]() Report: PSA 8 ng/mL (normal 0–4 ng/mL)
Report: PSA 8 ng/mL (normal 0–4 ng/mL)
PE: rectal: no masses found
What should be done to guide therapy?
a. Computed tomography (CT) of pelvis
b. US of pelvis
c. Transrectal US
d. Sigmoidoscopy
Answer c. Transrectal US
If you see an elevated PSA, you need to be sure if there is really a prostate cancer there. Do not do a test if you do not want to know the answer. If you feel a mass on rectal examination, then biopsy the mass you feel. If you do not feel a mass, then use the transrectal US to guide a biopsy.
The patient undergoes the transrectal US, which is negative and shows no masses.
![]() Repeat PSA: 8.5 ng/mL
Repeat PSA: 8.5 ng/mL
What should you recommend to exclude prostate cancer?
a. No further action is needed.
b. Do multiple palpation-guided biopsies.
c. Repeat the transrectal US.
Answer b. Do multiple palpation-guided biopsies.
The only way to be truly sure that there is no prostate cancer is to do multiple palpationguided biopsies. This means if the PSA is elevated, it always results in a biopsy.
The patient declines having the multiple palpation-guided biopsies. He leaves with plans to follow up in 6 months.
On CCS, patients can refuse procedures that they do not want or do not feel are indicated.
The patient is lost to follow-up for 2 years. Two years later he comes because of symptoms of dysuria, hesitancy, and dribbling.
PE:
![]() Rectal: enlarged prostate with nodule palpated in one lobe
Rectal: enlarged prostate with nodule palpated in one lobe
Orders:
![]() PSA
PSA
![]() Prostate biopsy
Prostate biopsy
Report:
![]() PSA: 18 ng/mL
PSA: 18 ng/mL
![]() Biopsy: adenocarcinoma of prostate
Biopsy: adenocarcinoma of prostate
Prostate Cancer Treatment
• Local: prostate resection
• Metastases: hormonal manipulation
A staging evaluation with a head CT and bone scan show no metastases. The patient is reluctant to have radical prostatectomy because of the risk of incontinence and erectile dysfunction.
Which of the following indicates the likelihood of metastasis occurring?
a. Number of lobes
b. Gleason scoring on pathology
c. PSA level
d. Age of patient
Answer b. Gleason scoring of the pathology
Gleason scoring is a numerical measurement of the pathogenicity of prostate cancer (Figure 9-2). A low score of 1 is closest to normal tissue. A high score of 10 is the most anaplastic or highest likelihood of metastasizing. When you have patients who are uncertain as to whether to risk prostate surgery, you can use the Gleason scoring as a way of giving them a likelihood of spread. For example, a young man with a high Gleason score should undergo radical prostatectomy with the intention of cure because of the high likelihood he will live a long time with a risk of spread. In an older man with a low Gleason score, it may be safe just to use radiation therapy.
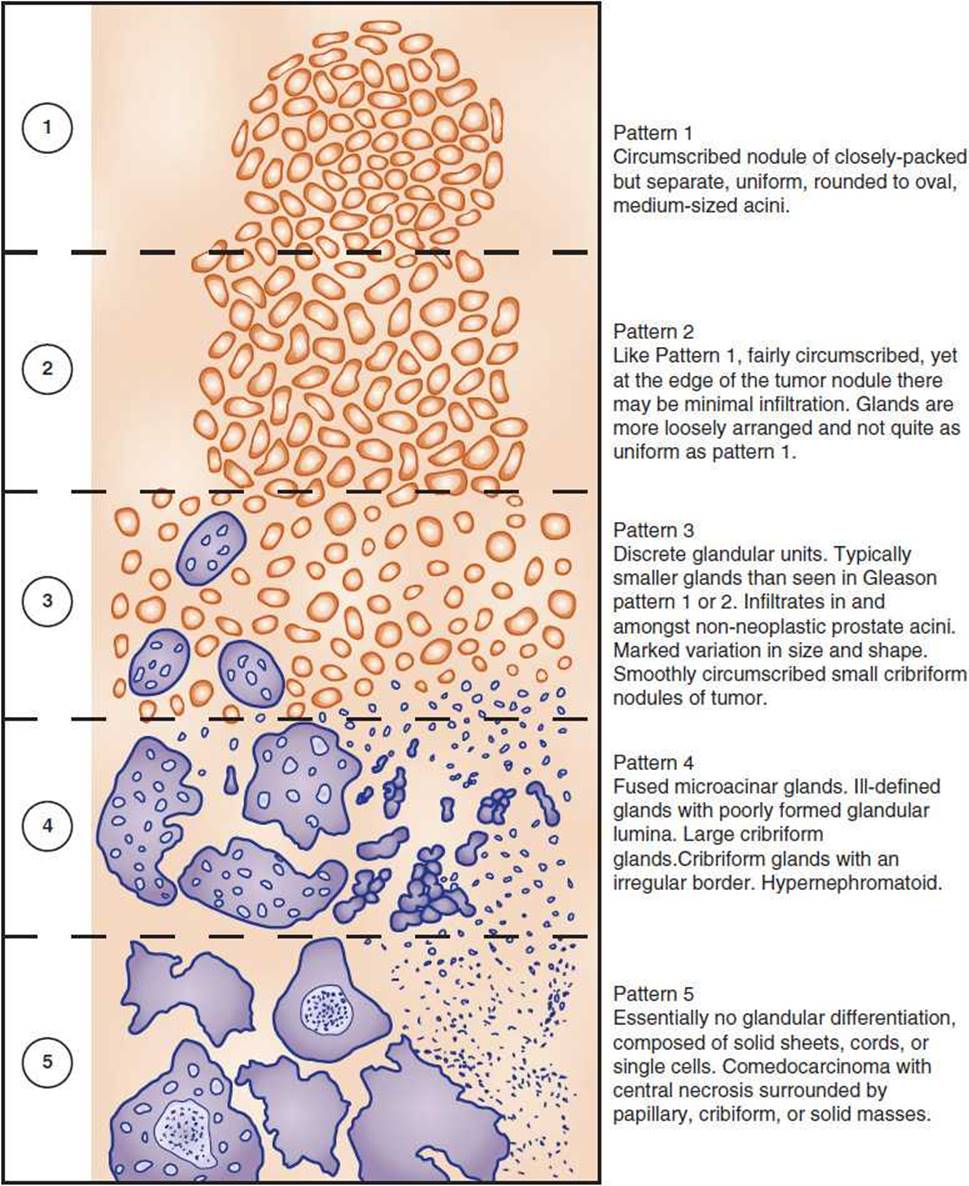
Figure 9-2. Prostate cancer staging. (Adapted with permission from Epstein JI, et al. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am J Surg Pathol. 2005;29(9):1228–1242.)
The patient ultimately refuses surgery and opts for brachytherapy. Radioactive seeds are implanted into the prostate. Over the next few months, the PSA goes down and the symptoms of obstructive uropathy subside.
There is no “adjuvant” chemotherapy for prostate cancer.
There is no “modified radical prostatectomy.”
There is no “lumpectomy” for prostate cancer.
One year later, the patient is brought to the emergency department (ED) with severe back pain and weakness in his legs.
PE:
![]() Musculoskeletal: focal spine tenderness present
Musculoskeletal: focal spine tenderness present
Neurological: extensor plantar reflexes present; hyperreflexic knee jerk reflexes present; sensation in lower extremities normal
What is the next “best step” in the management of this patient?
a. Dexamethasone
b. MRI
c. Radiation
d. Flutamide
e. Goserelin (GnRH agonist)
Answer a. Dexamethasone
Cord compression needs stat intravenous (IV) glucocorticoids. The most important thing is to prevent permanent neurological damage from impingement on the spinal cord. Steroids work faster than radiation. A biopsy is unlikely to be needed in this person who has a clear history of prostate cancer. Hormonal manipulation will help stop the growth of the lesion, but it will not actually shrink the lesion that is already there. Steroids will shrink the lesion. MRI is needed. Steroids are needed more. With back pain and focal neurological deficits and hyperreflexia, this is enough information to warrant steroids. Get the MRI done afterward. If it is a CCS case, you can order all of these things at the same time, because all of them are needed. CCS is a test of understanding timing. When you have cord compression, it is a big deal to give steroids before waiting for an MRI.
Dexamethasone is given and radiation is ordered. The patient is transferred to the hospital ward because you cannot send a person home with progressive neurological damage.
Report:
![]() The MRI shows compression of the spinal cord.
The MRI shows compression of the spinal cord.
After the start of steroids and radiation, which of the following is most urgent?
a. Denosumab
b. Finasteride
c. Flutamide
d. Goserelin (GnRH agonist)
Answer c. Flutamide
Flutamide and bicalutamide are testosterone receptor antagonists. In terms of hormonal therapy, it is critically important to start the target organ receptor blocker first.
GnRH agonists such as goserelin or leuprolide must never be started before flutamide in a person with metastatic prostate cancer, especially when it is on the spinal cord. The GnRH agonists initially give a burst up in LH and FSH levels. This will raise the testosterone levels and briefly increase the growth of the prostate cancer. Denosumab is a treatment for bone destruction from metastases and it is also a treatment for osteoporosis.
1. Block the testosterone target first.
2. Stop the gonadotropins (LH and FSH) after.
Finasteride and Dutasteride
• They are useless in prostate cancer.
• They block 5-alpha-reductase.
• They only decrease dihydrotestosterone.
What is the mechanism whereby goserelin or leuprolide decreases testosterone?
a. They downregulate at the pituitary gland.
b. They block testicular LH and FSH receptors.
c. They block dehydroepiandrosterone (DHEA) production at the adrenal gland.
d. They inhibit 17,20-lyase
e. They decrease the hypothalamic release of GnRH.
Answer a. Downregulation at the pituitary.
Hormones are usually made in pulsatile form. When a target organ is exposed to a constant amount of a hormone, the receptors at the target begin to involute and decrease. This is called either “downregulation” or “target organ resistance.” Because the pituitary gland is the target organ of GnRH, it is the pituitary gland where the receptors downregulate.
Denosumab
• It protects bones.
• It inhibits the receptor activator of nuclear factor kappa B ligand (RANKL).
• RANKL is similar to tumor necrosis factor (TNF).
RANKL = Receptor Activator of Nuclear Factor Kappa B Ligand
The patient undergoes treatment with radiation and has flutamide started, followed by a GnRH agonist shortly after. Symptoms of back pain resolve. Weakness in the legs improves.
Orchiectomy is the fastest way to lower androgen levels.
What other therapy can be done to block androgen production?
a. Abiraterone and degarelix
b. Estrogen and progesterone
c. Tamoxifen and exemestane
d. Nothing
Answer a. Abiraterone and degarelix
Abiraterone is an inhibitor of 17-alpha-hydroxylase in the gonads and adrenal glands. This drug shuts off production of the testosterone precursor DHEA. You cannot make testosterone if you do not make DHEA first. This drug closes the precursor “pipeline” for all sex hormones.
Degarelix is a GnRH receptor antagonist. It directly blocks the effect of GnRH on the pituitary gland.
The other medications manipulate estrogen. Exemestane is an aromatase inhibitor.
Chemotherapy is poor for prostate cancer.
Prostate metastases are controlled with hormone inhibitors.