Hypothyroidism/Myxedema Coma
Definition
• Hypothyroidism is characterized by insufficient production of thyroid hormone by the thyroid gland. Cretinism is a form of hypothyroidism found in infants.
• Hypothyroidism can be classified on the basis of its time of onset (congenital or acquired), the level of endocrine Dysfxn (1° [thyroid] or 2° [pituitary or hypothalamic]), & its severity (subclinical, clinical, severe [myxedema coma])
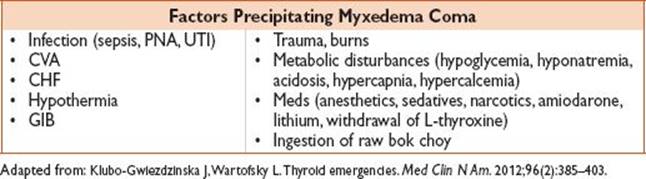
• Myxedema coma is a rare, extreme expression of severe hypothyroidism. Myxedema coma typically occurs in pts who develop systemic illness superimposed on previously undiagnosed hypothyroidism.
History
• Hypothyroidism: Weakness, fatigue, myalgias, HA, depression, cold intolerance, weight gain, constipation, menorrhagia, dry skin, brittle hair, hoarseness
• Myxedema coma: Severely altered mental status/coma
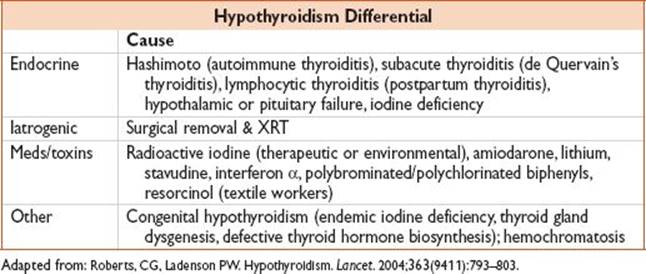
• Meds (see Differential table)
• RFs: Postpartum women, family hx of autoimmune thyroid disorders, prior H&N surgery or irradiation, other autoimmune disorders (ie, Type 1 DM, adrenal insufficiency, autoimmune polyendocrine syndrome types 1 & 2 etc.), Down’s syndrome, Turner’s syndrome
Physical Exam
• Hypothyroidism: Obese, delayed DTRs, diastolic HTN, dry, thick skin SQ tissue (myxedema), bradycardia, pl/pericardial/peritoneal effusion, hypothermia, hypotension, hypoventilation, altered sensorium
• Myxedema coma: Hypothermia & severely altered mental status/coma are hallmark
• Vitals/Pulm/CV: Hypothermia, hypoventilation, hypoxia, hypotension, or bradycardia
• HEENT: Facial swelling, periorbital edema, macroglossia
• Neuro: Lethargy → comatose, cerebellar signs, poor memory & cognition, delayed reflexes
• Psych: “Myxedema madness” disorientation, paranoia, depression, hallucinations, etc.
Evaluation
• Labs: TFTs (TSH elevated); Chem 7 (hyponatremia, hypoglycemia), CBC (anemia); consider T4, free T4, T3, antimicrosomal Ab, antithyroid peroxidase Ab, antithyroglobulin Ab
• ↑ TSH, ↓ free T4 confirms primary hypothyroidism of any cause
• ↑ TSH, ↓ free T4, +antithyroid abs confirms Hashimoto thyroiditis
• variable TSH, ↓ free T4 consistent w/ secondary hypothyroidsm disorders
• mild ↑ TSH, nl free T4, & subtle sxs consistent w/ subclinical hypothyroid
• ECG: Myxedema- bradycardia, AV block, low voltage, flattened/inverted T-waves, prolonged QTc, atrial/ventricular dysrhythmias.
• Bedside cardiac U/S: Pericardial effusion/tamponade may be seen in myxedema
Treatment (Only Start Empiric Treatment if Severely Symptomatic/Coma)
• Thyroid replacement: (Start in ED if severely symptomatic/coma)
• Levothyroxine: 5–8 mcg/kg IV × 1, then 50–100 mcg QD; consider synthetic T3 5–10 mcg IV q8h (b/c peripheral conversion impaired, but is more arrhythmogenic)
• Adrenal replacement: Hydrocortisone 100 mg IV × q8h (decreased reserve in coma)
Disposition
• Home: Discuss w/ PCP prior to starting any thyroid medications; usual starting dose of Levothyroxine 1.8 μg/kg PO QD (required repeat TFTs at 4–6 wk)
• Admit: All pts w/ severe hypothyroidism/myxedema; may require ICU admission
Thyrotoxicosis/Hyperthyroidism/Thyroid Storm
Definition
• Thyrotoxicosis is a disorder of excess thyroid hormone
• Hyperthyroidism specifically describes overproduction & secretion of excess of free thyroid hormones: Thyroxine (T4), triiodothyronine (T3), or both
• Thyroid storm/crisis is a rare, extreme expression of severe thyrotoxicosis
• Precise criteria for thyroid storm have been defined (Burch HB, Wartofsky L. Life-threatening thyrotoxicosis. Thyroid storm. Endocrinol Metab Clin North Am. 1993;22:263–277.)
History
• Neck fullness, double vision, restlessness, anxiety, palpitations, sweating, heat intolerance, tremor, weight loss, diarrhea, irregular menses, periodic paralysis, lethargy, hair thinning/loss
• Thyroid storm: AMS (delirium, agitation, coma), sz, fever, tachycardia, N/V, diarrhea
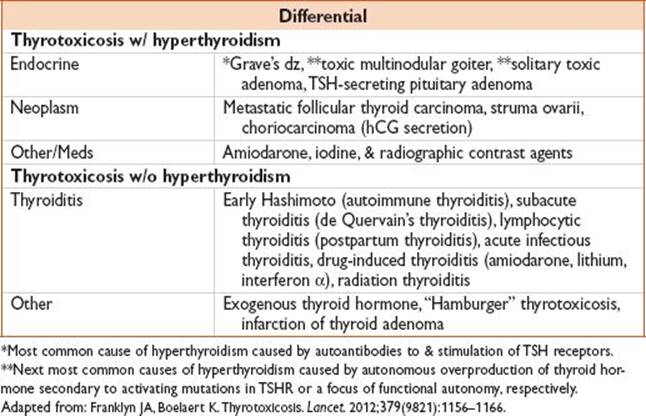
• Meds (see Differential table; assess h/o hyperthyroidism)
Physical Exam
• Thyrotoxicosis: Cachexia, diaphoretic, agitation, tremor, tachycardic, AF, systolic HTN, widened pulse pressure
• Thyroid storm: Hyperthermia & severely AMS are hallmark
• Vitals/Pulm/CV: Hyperthermia, hyperventilation, tachycardia
• GI: Nausea, vomiting, diarrhea, diffuse abdominal pain (may mimic acute abdomen)
• Neuro: AMS (delirium, agitation, coma), sz
• Psych: Disorientation, paranoia, psychosis, etc.
Evaluation
• Labs: TSH (low) w/ elevated free T4 (if TSH low & free T4 nl, free or total T3 concentration should also be measured to identify potential T3 toxicosis; consider thyroxine-binding globulin in pregnancy); Chem 7/Ca/Mg/Phosphorus, LFTs, UA, urine hCG; consider TRH or thyroid peroxidase
• ECG: Tachycardia, supraventricular ectopy, AF
Treatment (Only Start ED Treatment if Severely Symptomatic/Thyroid Storm)
• Thyrotoxicosis: Therapies include antithyroid meds (methimazole/PTU), radioiodine, surgery
• Thyroid storm: βB → PTU or methimazole → iodine or lithium → steroids w/ supportive care
• βB: Propranolol or esmolol (improve α-adrenergic activity & tachycardia)
• Propranolol 1 mg IV over 10 min, then 1–3 mg boluses q3h
• Propanolol 60–80 mg q4h if taking PO
• Esmolol 250–500 mcg/kg loading dose, then 50–100 mcg/kg/min
• PTU: Blocks hormone synthesis, inhibits peripheral conversion of T4 to T3
• Loading dose of 500–1000 mg, then 250 mg q4h
• Preferred to methimazole
• Methimazole: Blocks hormone synthesis
• Dose 20 mg q4h (60–80 mg/d)
• Pts should receive baseline CBC & LFTs prior to tx
• Iodine: Blocks thyroid hormone release but give >1 g after PTU (can potentiate thyroid storm if given before)
• Potassium iodide 5 drops (0.25 mL or 250 mg) PO q6h
• For iodine allergic pts, can use lithium carbonate 300 mg 6 h
• Steroids: Hydrocortisone 100–300 mg IV bolus, then 100 mg IV × q8h (can decrease conversion of T4–T3)
• Consider plasmaphoresis & therapeutic plasma exchange (Grave’s dz)
• Supportive care: Hyperpyrexia – Tylenol as needed; avoid aspirin (can increase T3 conversion)
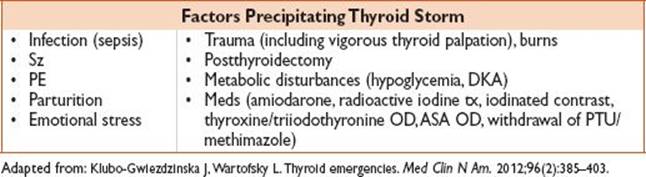
• Treat underlying precipitant (often infection)
Disposition
• Home: TSH low but no severe sxs. F/u w/ PCP or Endocrinologist regarding outpt medication & surgery.
• Admit: All pts w/ severe hyperthyroidism. Pts w/ thyroid storm require ICU admission.
Guideline: Bahn Chai RS, Burch HB, Cooper DS, et. al. Hyperthyroidism and other causes of thyrotoxicosis: Management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011;21(6):593–646.