PULMONARYQ
ASTHMA
Definition and epidemiology
• Chronic inflam. disorder w/ airway hyperresponsiveness + variable airflow obstruction
• Affects ~5% population; ~85% of cases by age 40 y
Clinical manifestations (NEJM 2001;344:350)
• Classic triad = wheezing, cough and dyspnea; others include chest tightness, sputum; symptoms typically chronic with episodic exacerbation
• Precipitants (triggers)
respiratory irritants (smoke, perfume, etc.) & allergens (pets, dust mites, pollen, etc.)
infections (URI, bronchitis, sinusitis)
drugs (eg, ASA & NSAIDs via leukotrienes, bB via bronchospasm, MSO4 via histamine) emotional stress, cold air, exercise (increase in ventilation dries out airways)
Physical examination
• Wheezing and prolonged expiratory phase
• Presence of nasal polyps, rhinitis, rash → allergic component
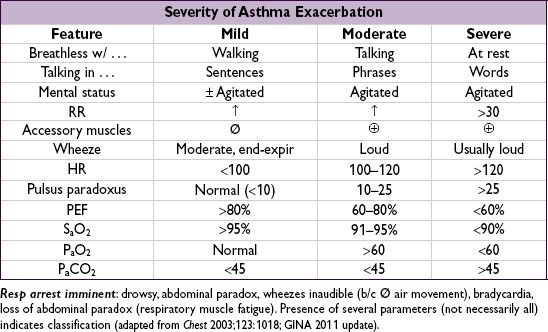
• Exacerbation → ↑ RR, ↑ HR, accessory muscle use, diaphoresis, pulsus paradoxus
Diagnostic studies
• Peak exp flow (PEF): ≥60 L/min ↑ after bronchodil or ≥20% diurnal variation c/w asthma. <80% personal best c/w poor control, <50% c/w severe exacerbation.
• Spirometry: ↓ FEV1, ↓ FEV1/FVC, coved flow-volume loop; lung volumes: ± ↑ RV & TLC
![]() bronchodilator response (↑ FEV1 ≥12% & ≥200 mL) strongly suggestive of asthma methacholine challenge (↓ FEV1 ≥20%) if PFTs nl: Se >90% (AJRCCM 2000;161:309)
bronchodilator response (↑ FEV1 ≥12% & ≥200 mL) strongly suggestive of asthma methacholine challenge (↓ FEV1 ≥20%) if PFTs nl: Se >90% (AJRCCM 2000;161:309)
• Sputum: eos >3% has 86% Se, 88% Sp; can also see Curschmann’s spirals (mucus casts of distal airways) and Charcot-Leyden crystals (eosinophil lysophospholipase)
• Allergy suspected → consider ✓ serum IgE, eos, skin testing/RAST
Ddx (“all that wheezes is not asthma … ”)
• Hyperventilation & panic attacks
• Upper airway obstruction or inh foreign body; laryngeal/vocal cord dysfxn (eg, 2° to GERD)
• CHF (“cardiac asthma”); COPD, bronchiectasis; ILD (including sarcoidosis); vasculitis; PE
“Asthma plus” syndromes (Lancet 2002;360:1313)
• Atopy = asthma + allergic rhinitis + atopic dermatitis
• ASA-sensitive asthma (Samter’s syndrome) = asthma + ASA sensitivity + nasal polyps
• ABPA = asthma + pulmonary infiltrates + allergic rxn to Aspergillus
• Churg-Strauss = asthma + eosinophilia + granulomatous vasculitis
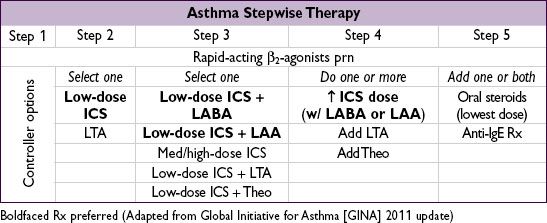
“Reliever” medications (used prn to quickly relieve sx)
• Short-acting inh β2-agonists (SABA): albuterol Rx of choice
• Short-acting inh anticholinergics (ipratropium) ↑ β2-agonist delivery → ↑ bronchodilation
“Controller” meds (taken daily to keep control) (NEJM 2009;360:1002)
• Inh corticosteroids (ICS): Rx of choice ( JAMA 2001;285:2583). PRN ? as good as daily for mild asthma (NEJM 2005;352:1519 & 2007;356:2040). PO steroids may be needed for severely uncontrolled asthma, but avoid if possible b/c systemic side effects.
• Long-acting inh β2-agonists (LABA; eg, salmeterol): ↑ PEF when added to ICS (Lancet 2009;374:1754). Except for exercise-induced asthma, should not be used w/o ICS (may ↑ mortality, esp. in African Americans) (Chest 2006;129:15; Annals 2006;144:904). Clinical relevance of β2-receptor pharmacogenetic interaction not validated (Lancet 2009;374:1754).
• Long-act inh anticholinergics (LAA; eg, tiotropium): add-on if sx despite ICS (superior to ↑ ICS, ![]() to adding LABA; NEJM 2010;363:1715) or if sx despite ICS+LABA (NEJM 2012;367:1198)
to adding LABA; NEJM 2010;363:1715) or if sx despite ICS+LABA (NEJM 2012;367:1198)
• Nedocromil/cromolyn: limited use in adults. Useful in young Pts, exercise-induced bronchospasm; ineffective unless used before trigger or exercise exposure.
• Theophylline: useful if hard to control sx; PO convenient, but high side-effect profile
• Leukotriene antagonists (LTA): some Pts very responsive, esp. ASA-sens (AJRCCM 2002;165:9) and exercise-induced (Annals 2000;132:97). May be noninf to ICS initial Rx and LABA add-on Rx (NEJM 2011;364:1695).
• Anti-IgE: for uncontrolled mod-to-severe allergic asthma (↑ IgE) on ICS ± LABA (NEJM 2006;354:2689; Annals 2011;154:573); not cost-effective for most Pts ( JACI 2007;120:1146)
Other
• Behavior modification: identify and avoid triggers; PPI w/o benefit (NEJM 2009;360:1487)
• Immunotherapy (eg, desensitization): may be useful if significant allergic component
• TNF antagonists may be helpful in Pts w/ refractory asthma (NEJM 2006;354:697)
• Anti-IL5 (mepolizumab) ↓ exac. w/ sev asthma (Lancet 2012;380:651), not yet FDA approved
• Anti-IL13 (lebrikizumab) ↑ FEV1 (NEJM 2011;365:1088), not yet FDA approved
• Bronchial thermoplasty (exp’tal): radiofrequency destruction of airway smooth muscle no Δ in FEV1, but ↓ in sx and # of exacerbations (NEJM 2007;356:1327)
Principles of treatment
• Education and avoidance of environmental triggers for all Pts; yearly flu shot
• Use quick-relief rescue medication as needed for all Pts
• Goal to achieve complete control = daily sx ≤2/wk, Ø nocturnal sx or limitation of activity, reliever med ≤2/wk, nl PEF or FEV1; partly controlled = 1–2 of the above present in a wk; uncontrolled = ≥3 of the above present in a wk
• Step up treatment as needed to gain control, step down as tolerated
• If PEF ↓ 15% × 2 d or ↓ 30%, 4× ICS dose ↓ need for PO steroids (AJRCCM 2009;180:598)
• Variants in glucocorticoid-induced transcript 1 gene a/w resp to ICS (NEJM 2011;365:1173)
EXACERBATION
Evaluation
• History: baseline PEF, steroid requirement, ED visits, hospital admissions, prior intubation Current exacerbation: duration, severity, potential precipitants, meds used
Risk factors for life-threatening: prior intubation, h/o near-fatal asthma, ED visit/hosp for asthma w/in 1 y, current/recent PO steroids, not using ICS, overdependent on SABA, Ψ, h/o noncompl
• Physical exam: VS, pulm, accessory muscle use, pulsus paradoxus, abdominal paradox
Assess for barotrauma: asymmetric breath sounds, tracheal deviation, subcutaneous air → pneumothorax, precordial (Hamman’s) crunch → pneumomediastinum
• Diagnostic studies: PEF (used to follow clinical course); SaO2; CXR to r/o PNA or PTX ABG if severe: low PaCO2 initially; nl or high PaCO2 may signify tiring
Initial treatment (NEJM 2010;363;755)
• Oxygen to keep SaO2 ≥90%
• Inhaled SABA (eg, albuterol) by MDI (4–8 puffs) or nebulizer (2.5–5 mg) q20min
• Corticosteroids: prednisone 0.5–1 mg/kg PO; IV if impending resp arrest
• Ipratropium MDI (4–6 puffs) or nebulizer (0.5 mg) q20min if severe (Chest 2002;121:1977)
• Epinephrine (0.3–0.5 mL SC of 1:1000 dilution) no advantage over inh SABA
• Montelukast IV ↑ FEV1 but did not Δ rate of hosp ( J Allergy Clin Immunol 2010;125:374)
• Reassess after 60–90 min of Rx
Mild-mod exacerbation: cont SABA q1h
Severe exacerbation: SABA & ipratropium q1h or continuously; ± Mg 2 g IV over 20 min (Lancet 2003;361:2114); ± heliox (60–80%)
• Decide disposition within 4 h of presentation and after 1–3 h of Rx
Figure 2-2 Disposition of patients after initial treatment of asthma exacerbation
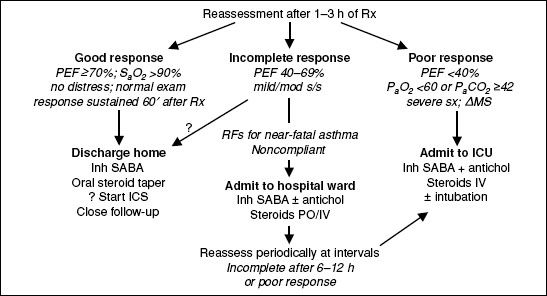
ICU-level care
• High-dose steroids: methylprednisolone 125 mg IV q6h (Archives 1983;143:1324)
• Invasive ventilation:
large ET tube, Pplat <30 cm H2O (predicts barotrauma better than PIP), max exp time
PEEP individualized to Pt physiology
paralysis, inhalational anesthetics, bronchoalveolar lavage w/ mucolytic, heliox (60–80% helium) and ECMO have been used with success
• NPPV likely improves obstruction (Chest 2003;123:1018), but controversial and rarely used