Definition
• Valvular heart disease caused by the incomplete opening or narrowing of the aortic valve resulting in impediment of blood flow from the left ventricle to the aorta
Pathogenesis
• Predisposing conditions include superimposed calcification of a congenital bicuspid aortic valve and postinflammatory scarring due to rheumatic heart disease
• Senile calcification of a normal trileaflet aortic valve is most common
• Ochronosis with alkaptonuria is an infrequent contributing factor
• Rarely, caused by severe atherosclerosis occurring most frequently in patients with hypercholesterolemia and children with homozygous type II hyperlipoproteinemia
• Familial clustering and genetic polymorphisms have been linked to calcific aortic stenosis
• Usually leads to left ventricular concentric hypertrophy
Clinical features
Epidemiology
• Usually seen in patients older than 65 years
• Most common valvular disease in the United States and Europe
• Male predominance: 2:1 ratio
Presentation
• Cardinal manifestations include syncope, angina pectoris, and exertional dyspnea (thus the mnemonic SAD)
• Clinical features include a slow upstroke of the arterial pulse, an apical–carotid delay, an ejection systolic murmur increased with squatting and fatigue
• Late findings in patients include atrial fibrillation, pulmonary hypertension, and systemic venous hypertension; gastrointestinal bleeding, infective endocarditis, and von Willebrand disease have been reported in some cases
• Chest x-ray film confirms hypertrophy of the left ventricle, a prominent ascending aorta, and aortic valve calcification
Prognosis and treatment
• Patients with mild stenosis have a slow progression and may remain asymptomatic for 10 to 15 years
• Symptomatic patients are treated with ACE inhibitors
• Patients with severe symptoms require valve replacement
• Untreated severe symptomatic patients have a poor prognosis
Pathology
• Gross appearance of valves is distorted because of permanently deformed leaflets. Commisural fusion of the valve cusps and shortening, thickening, and fusion of the tendinous cords are present
• Rheumatic disease: Aschoff nodules are found on the valves only in acute rheumatic fever and are gradually replaced by diffused fibrotic scars. The edges of cusps eventually adhere together and become stenotic
• Infective endocarditis: characteristic appearance is the presence of firm, irregular, brownish gray, friable vegetations on the valve leaflets. Inflammation, hyalinization, and calcification of the vegetations are found. Microscopically, vegetations consist of platelets, fibrin, leukocytes, and the infecting organism. Invasion of the fibrinous layer by granulation tissue results in fibrosis of the valves
• Congenital anomalies: calcification of single or bicuspid aortic valves occurs with age. Heaped-up subendothelial rigid calcific masses are seen and cause thick and immobile valve cusps
Immunopathology/special stains
• Not contributory
Main differential diagnoses
• Atherosclerosis
• Supravalvular aortic stenosis
• Hypertrophic cardiomyopathy (idiopathic hypertrophic subaortic stenosis)
• Hypertension: concentric left ventricular hypertrophy with a normal valve

Fig 1 Aortic valve stenosis. Gross photograph of a thickened, calcified, stenotic aortic valve viewed from the aorta.
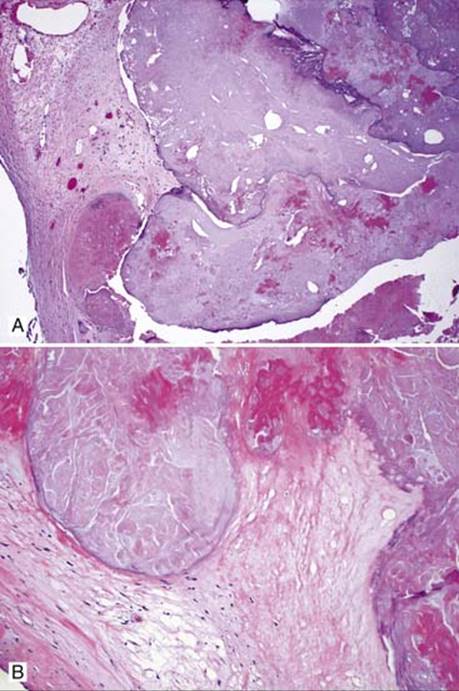
Fig 2 Aortic valve stenosis. Aortic valve with extensive calcification seen at low (A) and medium (B) powers.

Fig 3 Aortic valve stenosis. Neovascularization is present adjacent to calcification. There is mild chronic inflammation (A) and focal foreign body giant cell reaction (B).