Katrina A. Leone
EPIDEMIOLOGY
![]() Hypothyroidism is a condition of insufficient thyroid hormone production that causes slowed metabolism.
Hypothyroidism is a condition of insufficient thyroid hormone production that causes slowed metabolism.
![]() Hypothyroidism is more common in women than in men.
Hypothyroidism is more common in women than in men.
![]() Myxedema coma is a life-threatening expression of severe hypothyroidism. Vast majority of cases occur during the winter months in elderly women with undi-agnosed or under-treated hypothyroidism.
Myxedema coma is a life-threatening expression of severe hypothyroidism. Vast majority of cases occur during the winter months in elderly women with undi-agnosed or under-treated hypothyroidism.
![]() Mortality for myxedema coma ranges from 30% to 60%, depending on the extent of comorbid diseases.
Mortality for myxedema coma ranges from 30% to 60%, depending on the extent of comorbid diseases.
PATHOPHYSIOLOGY
![]() The most common etiologies of hypothyroidism are primary thyroid failure due to autoimmune disease (Hashimoto’s thyroiditis), idiopathic causes, ablative surgery, or iodine deficiency.
The most common etiologies of hypothyroidism are primary thyroid failure due to autoimmune disease (Hashimoto’s thyroiditis), idiopathic causes, ablative surgery, or iodine deficiency.
![]() Secondary hypothyroidism is due to a deficiency of thyroid stimulating hormone (TSH) from pituitary tumors, infiltrative disease, or hemorrhage, or a deficiency of thyrotropin-releasing hormone from the hypothalamus.
Secondary hypothyroidism is due to a deficiency of thyroid stimulating hormone (TSH) from pituitary tumors, infiltrative disease, or hemorrhage, or a deficiency of thyrotropin-releasing hormone from the hypothalamus.
![]() Medications that cause hypothyroidism include amio-darone and lithium.
Medications that cause hypothyroidism include amio-darone and lithium.
![]() Precipitating events of myxedema coma include infection, congestive heart failure, drugs, trauma, and exposure to a cold environment.
Precipitating events of myxedema coma include infection, congestive heart failure, drugs, trauma, and exposure to a cold environment.
CLINICAL FEATURES
![]() Typical signs and symptoms of hypothyroidism include fatigue, weakness, cold intolerance, constipation, weight gain, and deepening of the voice.
Typical signs and symptoms of hypothyroidism include fatigue, weakness, cold intolerance, constipation, weight gain, and deepening of the voice.
![]() Cutaneous signs include dry skin, non-pitting edema of the face and extremities (myxedema), and thinning eyebrows.
Cutaneous signs include dry skin, non-pitting edema of the face and extremities (myxedema), and thinning eyebrows.
![]() Cardiac findings include bradycardia, cardiomyopa-thy, and a low-voltage electrocardiogram.
Cardiac findings include bradycardia, cardiomyopa-thy, and a low-voltage electrocardiogram.
![]() Paresthesias, ataxia, and prolongation of the deep tendon reflexes are characteristic neurologic findings.
Paresthesias, ataxia, and prolongation of the deep tendon reflexes are characteristic neurologic findings.
![]() A thyroidectomy scar may be present, but a goiter is uncommon.
A thyroidectomy scar may be present, but a goiter is uncommon.
![]() In addition to the above features of hypothyroidism, patients with myxedema coma present with hypothermia, hypotension, altered mental status, hyponatremia, hypoglycemia, and respiratory failure.
In addition to the above features of hypothyroidism, patients with myxedema coma present with hypothermia, hypotension, altered mental status, hyponatremia, hypoglycemia, and respiratory failure.
DIAGNOSIS AND DIFFERENTIAL
![]() Thyroid tests will typically demonstrate low free thy-roxine (FT4) or triiodothyronine (FT3) levels and elevated TSH in primary hypothyroidism. Low TSH with low FT4 and FT3 indicates secondary hypothyroidism.
Thyroid tests will typically demonstrate low free thy-roxine (FT4) or triiodothyronine (FT3) levels and elevated TSH in primary hypothyroidism. Low TSH with low FT4 and FT3 indicates secondary hypothyroidism.
![]() Myxedema coma is a clinical diagnosis that must be suspected based upon the clinical presentation. There is no level of TSH or thyroid hormone that differentiates hypothyroidism from myxedema coma, and treatment should not be delayed to obtain confirmatory laboratory tests.
Myxedema coma is a clinical diagnosis that must be suspected based upon the clinical presentation. There is no level of TSH or thyroid hormone that differentiates hypothyroidism from myxedema coma, and treatment should not be delayed to obtain confirmatory laboratory tests.
![]() The differential diagnosis of myxedema coma includes sepsis, adrenal crisis, hypoglycemia, meningitis, hypercarbia, hyponatremia, environmental hypothermia, congestive heart failure, stroke, and drug overdose.
The differential diagnosis of myxedema coma includes sepsis, adrenal crisis, hypoglycemia, meningitis, hypercarbia, hyponatremia, environmental hypothermia, congestive heart failure, stroke, and drug overdose.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Most patients with uncomplicated symptomatic hypothyroidism may be referred to their primary care physician for further evaluation and initiation of treatment.
Most patients with uncomplicated symptomatic hypothyroidism may be referred to their primary care physician for further evaluation and initiation of treatment.
![]() Supportive care for myxedema coma includes airway stabilization and establishment of adequate oxygenation and ventilation. A difficult airway should be anticipated due to macroglossia and oropharyngeal edema.
Supportive care for myxedema coma includes airway stabilization and establishment of adequate oxygenation and ventilation. A difficult airway should be anticipated due to macroglossia and oropharyngeal edema.
![]() Initiate cardiac monitoring, gradual rewarming for hypothermia, and correction of hypoglycemia. Hyponatremia typically responds to fluid restriction.
Initiate cardiac monitoring, gradual rewarming for hypothermia, and correction of hypoglycemia. Hyponatremia typically responds to fluid restriction.
![]() Vasopressors are often ineffective and should be reserved for severe hypotension. Sedating drugs should be avoided.
Vasopressors are often ineffective and should be reserved for severe hypotension. Sedating drugs should be avoided.
![]() Investigate and treat precipitating causes.
Investigate and treat precipitating causes.
![]() Pharmacologic therapy for myxedema coma includes hydrocortisone 100 milligrams IV (to treat possible concurrent adrenal insufficiency) and levothyroxine (T4) 4 micrograms/kg by slow IV infusion. Add L-triiodothy-ronine (T3) 20 micrograms IV for severe symptoms. L-triiodothyronine dosage should be halved (or avoided completely) in patients with cardiovascular disease due to a risk of arrhythmias and myocardial infarction.
Pharmacologic therapy for myxedema coma includes hydrocortisone 100 milligrams IV (to treat possible concurrent adrenal insufficiency) and levothyroxine (T4) 4 micrograms/kg by slow IV infusion. Add L-triiodothy-ronine (T3) 20 micrograms IV for severe symptoms. L-triiodothyronine dosage should be halved (or avoided completely) in patients with cardiovascular disease due to a risk of arrhythmias and myocardial infarction.
![]() Admit all patients with myxedema coma to an ICU setting.
Admit all patients with myxedema coma to an ICU setting.
THYROTOXICOSIS AND THYROID STORM
EPIDEMIOLOGY
![]() Thyrotoxicosis is a general term for excess circulating thyroid hormone from any cause. Hyperthyroidism is defined as excess circulating thyroid hormone due to thyroid gland hyperactivity
Thyrotoxicosis is a general term for excess circulating thyroid hormone from any cause. Hyperthyroidism is defined as excess circulating thyroid hormone due to thyroid gland hyperactivity
![]() Graves’ disease is the most common cause of hyper-thyroidism (85%) and typically presents in the third and fourth decades of life.
Graves’ disease is the most common cause of hyper-thyroidism (85%) and typically presents in the third and fourth decades of life.
![]() Thyroid storm is an acute, life-threatening manifestation of thyrotoxicosis most often seen in patients with unrecognized or undertreated hyperthyroidism.
Thyroid storm is an acute, life-threatening manifestation of thyrotoxicosis most often seen in patients with unrecognized or undertreated hyperthyroidism.
![]() Thyroid storm mortality is high, even with aggressive treatment.
Thyroid storm mortality is high, even with aggressive treatment.
PATHOPHYSIOLOGY
![]() Primary hyperthyroidism is caused by excess production of thyroid hormones from the thyroid gland. Secondary hyperthyroidism is due to excess production of thyroid-releasing hormone from the hypothalamus or TSH from the pituitary.
Primary hyperthyroidism is caused by excess production of thyroid hormones from the thyroid gland. Secondary hyperthyroidism is due to excess production of thyroid-releasing hormone from the hypothalamus or TSH from the pituitary.
![]() Other causes of hyperthyroidism include iodine or amiodarone use, ingestion of excessive thyroid hormone, and thyroid hormone production at ectopic sites (ovarian teratoma, hydatidiform mole, metastatic thyroid cancer).
Other causes of hyperthyroidism include iodine or amiodarone use, ingestion of excessive thyroid hormone, and thyroid hormone production at ectopic sites (ovarian teratoma, hydatidiform mole, metastatic thyroid cancer).
![]() Precipitants of thyroid storm include infection, trauma, diabetic ketoacidosis (DKA), myocardial infarction, stroke, pulmonary embolism, surgery, withdrawal of thyroid medication, iodine administration, palpation of the thyroid gland, ingestion of thyroid hormone, and idiopathic causes (∼25%).
Precipitants of thyroid storm include infection, trauma, diabetic ketoacidosis (DKA), myocardial infarction, stroke, pulmonary embolism, surgery, withdrawal of thyroid medication, iodine administration, palpation of the thyroid gland, ingestion of thyroid hormone, and idiopathic causes (∼25%).
CLINICAL FEATURES
![]() Symptoms of hyperthyroidism include heat intolerance, palpitations, weight loss, sweating, tremor, nervousness, weakness, fatigue, ophthalmoplegia, exophthal-mos, widened pulse pressure, and a palpable goiter.
Symptoms of hyperthyroidism include heat intolerance, palpitations, weight loss, sweating, tremor, nervousness, weakness, fatigue, ophthalmoplegia, exophthal-mos, widened pulse pressure, and a palpable goiter.
![]() The signs and symptoms associated with thyroid storm are related to enhanced sympathetic nervous system activity and include central nervous system disturbance (confusion, delirium, seizure, coma), cardiovascular abnormalities (sinus tachycardia, atrial fibrillation, premature ventricular contractions, congestive heart failure), and stimulated gastrointestinal motility and diarrhea.
The signs and symptoms associated with thyroid storm are related to enhanced sympathetic nervous system activity and include central nervous system disturbance (confusion, delirium, seizure, coma), cardiovascular abnormalities (sinus tachycardia, atrial fibrillation, premature ventricular contractions, congestive heart failure), and stimulated gastrointestinal motility and diarrhea.
![]() Apathetic thyrotoxicosis is a distinct presentation of thyroid storm in the elderly that includes lethargy, slowed mentation, apathetic facies, goiter, weight loss, and proximal muscle weakness.
Apathetic thyrotoxicosis is a distinct presentation of thyroid storm in the elderly that includes lethargy, slowed mentation, apathetic facies, goiter, weight loss, and proximal muscle weakness.
DIAGNOSIS AND DIFFERENTIAL
![]() A suppressed TSH and elevated free FT4 or FT3 level confirm the diagnosis of primary hyperthyroidism. In cases of secondary hyperthyroidism, TSH, FT4, and FT3 are all elevated.
A suppressed TSH and elevated free FT4 or FT3 level confirm the diagnosis of primary hyperthyroidism. In cases of secondary hyperthyroidism, TSH, FT4, and FT3 are all elevated.
![]() Thyroid hormone levels do not differentiate between symptomatic, uncomplicated thyrotoxicosis and thyroid storm.
Thyroid hormone levels do not differentiate between symptomatic, uncomplicated thyrotoxicosis and thyroid storm.
![]() The differential diagnosis of thyroid storm includes sepsis, other causes of congestive heart failure, stroke, complications of diabetes (eg, DKA or hypoglycemia), heat stroke, delirium tremens, malignant hyperther-mia, neuroleptic malignant syndrome, pheochromocy-toma, medication withdrawal, and sympathomimetic or organophosphate overdose.
The differential diagnosis of thyroid storm includes sepsis, other causes of congestive heart failure, stroke, complications of diabetes (eg, DKA or hypoglycemia), heat stroke, delirium tremens, malignant hyperther-mia, neuroleptic malignant syndrome, pheochromocy-toma, medication withdrawal, and sympathomimetic or organophosphate overdose.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
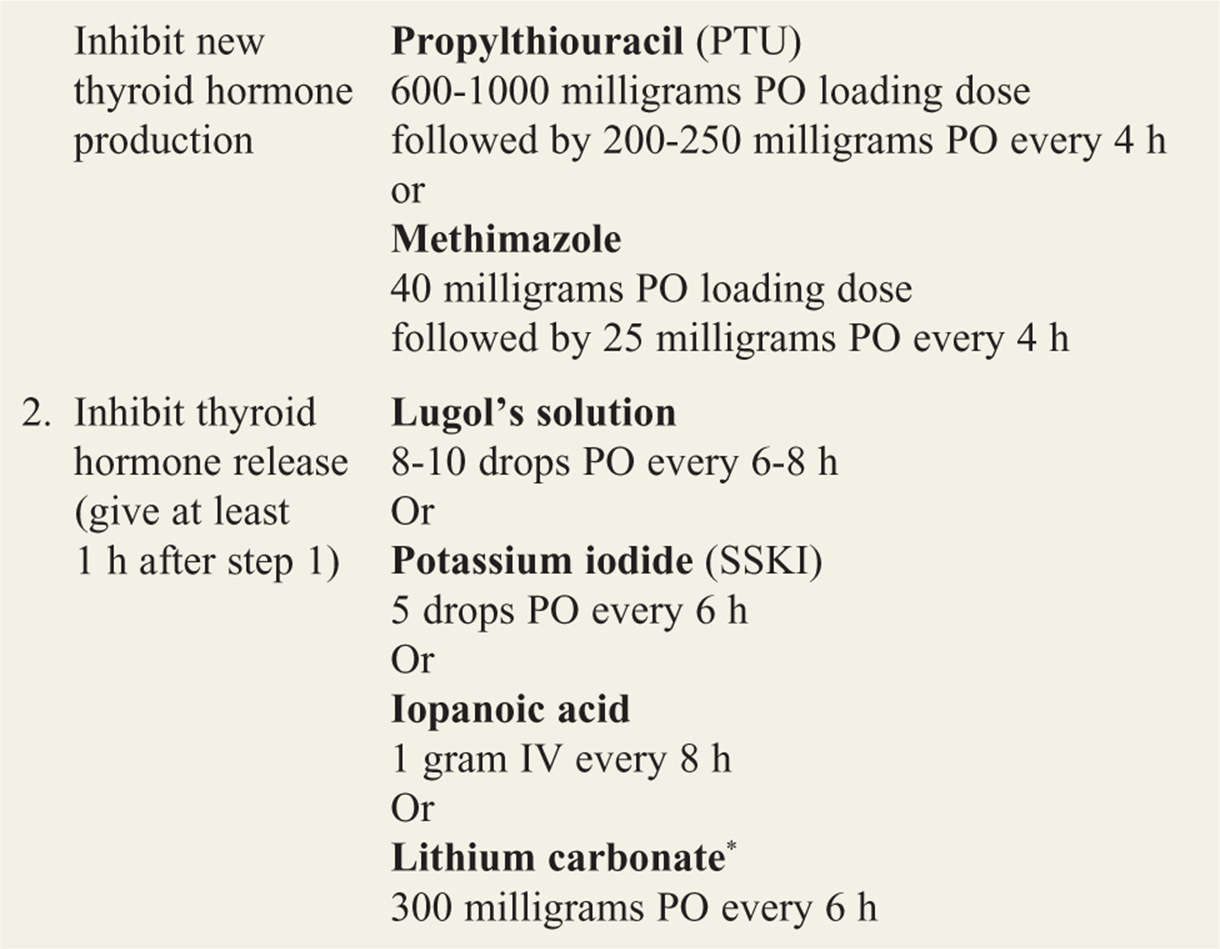
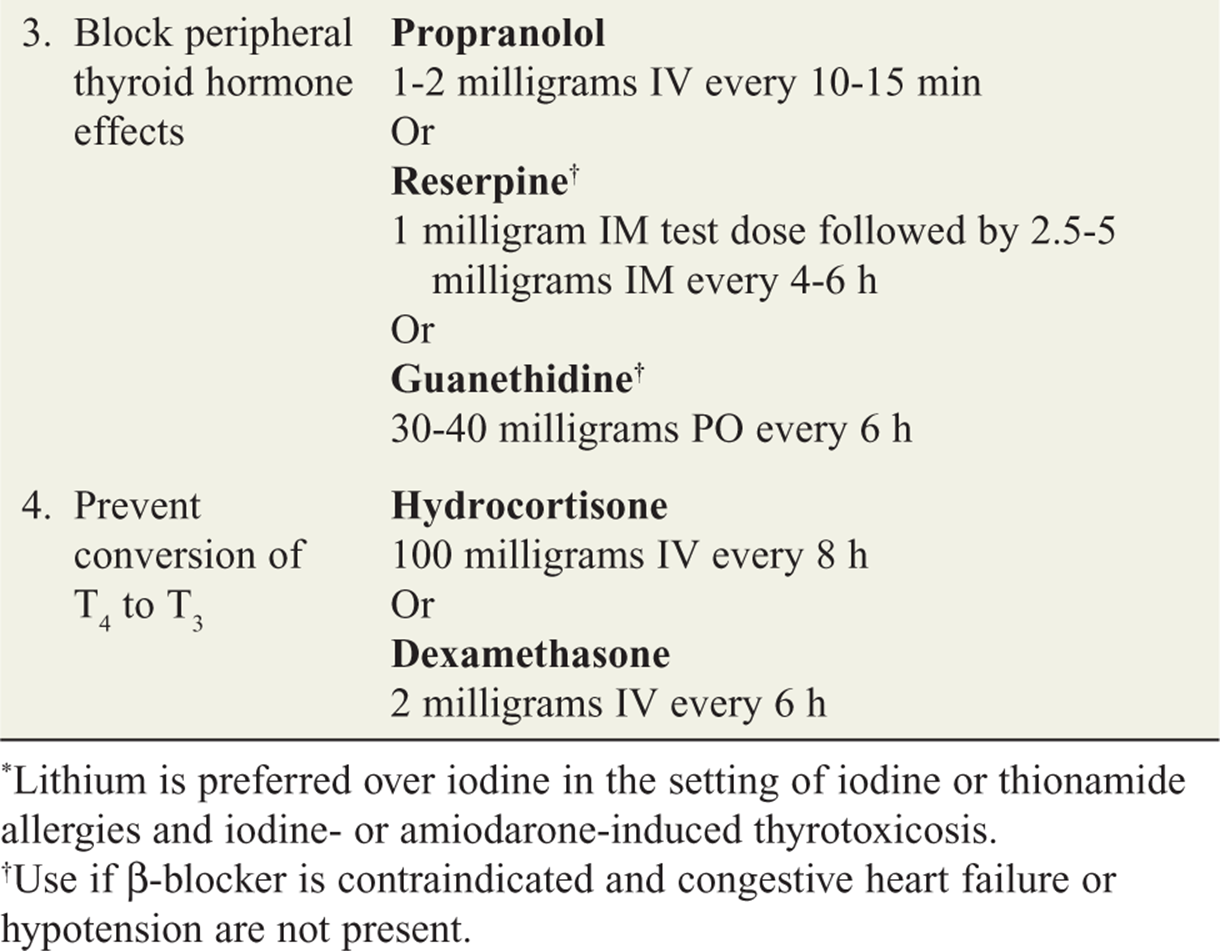
![]() Treatment of thyroid storm can be divided into three areas: (1) general supportive care, including airway assessment, supplemental oxygen, intravenous fluids, and cardiac monitoring; (2) pharmacologic therapy to inhibit thyroid hormone synthesis, prevent thyroid hormone release, block peripheral thyroid hormone effects, and prevent peripheral conversion of FT4 to FT3 (Table 133-1); and (3) identification and treatment of precipitating events.
Treatment of thyroid storm can be divided into three areas: (1) general supportive care, including airway assessment, supplemental oxygen, intravenous fluids, and cardiac monitoring; (2) pharmacologic therapy to inhibit thyroid hormone synthesis, prevent thyroid hormone release, block peripheral thyroid hormone effects, and prevent peripheral conversion of FT4 to FT3 (Table 133-1); and (3) identification and treatment of precipitating events.
![]() All patients with thyroid storm should be admitted to a monitored or intensive care unit setting.
All patients with thyroid storm should be admitted to a monitored or intensive care unit setting.
TABLE 133-1 Drug Treatment of Thyroid Storm
For further reading in Tintinalli’s Emergency Medicine; A Comprehensive Study Guide, 7th ed., see Chapter 223, “Thyroid Disorders: Hypothyroidism and Myxedema Crisis,” by Alzamani Mohammad Idrose, and Chapter 224, “Thyroid Disorders: Hyperthyroidism and Thyroid Storm,” by Alzamani Mohammad Idrose.