Daniel A. Handel
ERYTHEMA MULTIFORME
EPIDEMIOLOGY
![]() The highest incidence is in young adults (20-40 years of age), with males affected twice as often as females.
The highest incidence is in young adults (20-40 years of age), with males affected twice as often as females.
PATHOPHYSIOLOGY
![]() Erythema multiforme (EM) is an acute inflammatory skin disease that ranges from a mild papular eruption (EM minor) to a severe vesiculobullous form with mucous membrane involvement and systemic toxicity (Stevens–Johnson syndrome).
Erythema multiforme (EM) is an acute inflammatory skin disease that ranges from a mild papular eruption (EM minor) to a severe vesiculobullous form with mucous membrane involvement and systemic toxicity (Stevens–Johnson syndrome).
![]() EM is usually due to infection, drugs (antibiotics and anticonvulsants), malignancy, rheumatologic disorders, or pregnancy.
EM is usually due to infection, drugs (antibiotics and anticonvulsants), malignancy, rheumatologic disorders, or pregnancy.
![]() No cause is found in 50% of cases.
No cause is found in 50% of cases.
CLINICAL FEATURES
![]() Symptoms include malaise, arthralgias, myalgias, fever, diffuse pruritus, and a generalized burning sensation that may be noted days prior to skin abnormalities.
Symptoms include malaise, arthralgias, myalgias, fever, diffuse pruritus, and a generalized burning sensation that may be noted days prior to skin abnormalities.
![]() Signs noted on examination primarily involve the skin and mucosal surfaces, including erythematous papules (which appear first) and maculopapules, target lesion (evolves in 24-48 hours), urticarial plaques, vesicles, bullae, vesiculobullous lesions, and mucosal (oral, conjunctival, respiratory, and genitourinary) erosions.
Signs noted on examination primarily involve the skin and mucosal surfaces, including erythematous papules (which appear first) and maculopapules, target lesion (evolves in 24-48 hours), urticarial plaques, vesicles, bullae, vesiculobullous lesions, and mucosal (oral, conjunctival, respiratory, and genitourinary) erosions.
![]() The target lesion is highly characteristic of EM. The erythematous papules appear symmetrically on the dorsum of the hands and feet, and the extensor surfaces of the extremities.
The target lesion is highly characteristic of EM. The erythematous papules appear symmetrically on the dorsum of the hands and feet, and the extensor surfaces of the extremities.
![]() Ocular involvement occurs in approximately 9% of patients with EM minor and in almost 70% of patients with Stevens–Johnson syndrome.
Ocular involvement occurs in approximately 9% of patients with EM minor and in almost 70% of patients with Stevens–Johnson syndrome.
![]() Patients are at risk for significant fluid and electrolyte deficiencies as well as secondary infection.
Patients are at risk for significant fluid and electrolyte deficiencies as well as secondary infection.
![]() Recurrence is noted, especially involving cases in which infection or medication is involved.
Recurrence is noted, especially involving cases in which infection or medication is involved.
DIAGNOSIS AND DIFFERENTIAL
![]() The diagnosis of EM is based on the simultaneous presence of lesions with multiple morphologies at times with mucous membrane involvement.
The diagnosis of EM is based on the simultaneous presence of lesions with multiple morphologies at times with mucous membrane involvement.
![]() The differential diagnosis includes herpetic infections, vasculitis, toxic epidermal necrolysis (TEN), primary blistering disorders, Kawasaki’s disease, and toxic-infectious erythemas.
The differential diagnosis includes herpetic infections, vasculitis, toxic epidermal necrolysis (TEN), primary blistering disorders, Kawasaki’s disease, and toxic-infectious erythemas.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Patients with localized papular disease without systemic manifestations and mucous membrane involvement may be managed on an outpatient basis with dermatologic consultation. Systemic steroid bursts as well as oral antihistamines can be used but are unproven to change outcomes and duration of symptoms.
Patients with localized papular disease without systemic manifestations and mucous membrane involvement may be managed on an outpatient basis with dermatologic consultation. Systemic steroid bursts as well as oral antihistamines can be used but are unproven to change outcomes and duration of symptoms.
![]() Diphenhydramine and lidocaine rinses are useful for stomatitis; cool Burrow’s solution compresses are applied to blistered regions.
Diphenhydramine and lidocaine rinses are useful for stomatitis; cool Burrow’s solution compresses are applied to blistered regions.
![]() Inpatient therapy in a critical care setting with immediate dermatologic consultation is advised for patients with extensive disease or systemic toxicity.
Inpatient therapy in a critical care setting with immediate dermatologic consultation is advised for patients with extensive disease or systemic toxicity.
![]() Intensive management of potential fluid, electrolyte, infectious, nutritional, and thermoregulatory issues, as well as parenteral analgesics and antihistamines are required for patients with severe cases.
Intensive management of potential fluid, electrolyte, infectious, nutritional, and thermoregulatory issues, as well as parenteral analgesics and antihistamines are required for patients with severe cases.
TOXIC EPIDERMAL NECROLYSIS
PATHOPHYSIOLOGY
![]() TEN is an explosive dermatosis characterized by tender erythema, bullae formation, and subsequent exfoliation.
TEN is an explosive dermatosis characterized by tender erythema, bullae formation, and subsequent exfoliation.
![]() The most common cause of TEN is medications; other etiologies include chemicals, infections (eg, HIV), malignancy, or immunologic factors.
The most common cause of TEN is medications; other etiologies include chemicals, infections (eg, HIV), malignancy, or immunologic factors.
![]() Sulfa-based drugs, penicillin, anticonvulsants, and nonsteroidal anti-inflammatory drugs (NSAIDs) are the most frequent medication triggers for TEN.
Sulfa-based drugs, penicillin, anticonvulsants, and nonsteroidal anti-inflammatory drugs (NSAIDs) are the most frequent medication triggers for TEN.
CLINICAL FEATURES
![]() Patients may complain of malaise, anorexia, myalgias, arthralgias, fever, painful skin, and symptoms of upper respiratory infection. These symptoms may be present for 1 to 2 weeks prior to the development of skin abnormalities.
Patients may complain of malaise, anorexia, myalgias, arthralgias, fever, painful skin, and symptoms of upper respiratory infection. These symptoms may be present for 1 to 2 weeks prior to the development of skin abnormalities.
![]() Physical examination findings include a warm and tender erythema, flaccid bullae, positive Nikolsky’s sign, erosions with exfoliation, mucous membrane (oral, conjunctival, respiratory, and genitourinary) lesions, and systemic toxicity.
Physical examination findings include a warm and tender erythema, flaccid bullae, positive Nikolsky’s sign, erosions with exfoliation, mucous membrane (oral, conjunctival, respiratory, and genitourinary) lesions, and systemic toxicity.
![]() Nikolsky’s sign is positive when the superficial layers of skin slip free from the lower layers with a slight rubbing pressure; large areas of the skin will blister and peel away, leaving wet, red, painful areas.
Nikolsky’s sign is positive when the superficial layers of skin slip free from the lower layers with a slight rubbing pressure; large areas of the skin will blister and peel away, leaving wet, red, painful areas.
![]() Infection, hypovolemia, and electrolyte disorders are typical causes of death, an end result in as many as 25% to 35% of cases.
Infection, hypovolemia, and electrolyte disorders are typical causes of death, an end result in as many as 25% to 35% of cases.
![]() Predictors of poor prognosis include advanced age, extensive disease, leukopenia, azotemia, and thrombocytopenia.
Predictors of poor prognosis include advanced age, extensive disease, leukopenia, azotemia, and thrombocytopenia.
DIAGNOSIS AND DIFFERENTIAL
![]() Diagnosis of TEN is confirmed by skin biopsy.
Diagnosis of TEN is confirmed by skin biopsy.
![]() The differential diagnosis includes toxic-infectious erythemas, exfoliative drug eruptions, primary blistering disorders, Kawasaki’s disease, and Stevens–Johnson syndrome.
The differential diagnosis includes toxic-infectious erythemas, exfoliative drug eruptions, primary blistering disorders, Kawasaki’s disease, and Stevens–Johnson syndrome.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Patients with TEN are best cared for in a critical care setting such as a burn unit.
Patients with TEN are best cared for in a critical care setting such as a burn unit.
![]() Attention to adequate cardiorespiratory function is essential; correction of fluid, electrolyte, and infectious complications are early treatment considerations.
Attention to adequate cardiorespiratory function is essential; correction of fluid, electrolyte, and infectious complications are early treatment considerations.
![]() Immediate dermatologic consultation is required.
Immediate dermatologic consultation is required.
EXFOLIATIVE DERMATITIS
EPIDEMIOLOGY
![]() Males are affected twice as often as females, and most patients are over the age of 40 years.
Males are affected twice as often as females, and most patients are over the age of 40 years.
PATHOPHYSIOLOGY
![]() Exfoliative dermatitis, a cutaneous reaction to a drug, chemical, or underlying systemic disease state, occurs when most or all of the skin is involved with a scaling erythema, leading subsequently to exfoliation.
Exfoliative dermatitis, a cutaneous reaction to a drug, chemical, or underlying systemic disease state, occurs when most or all of the skin is involved with a scaling erythema, leading subsequently to exfoliation.
![]() The underlying mechanism is largely unknown.
The underlying mechanism is largely unknown.
![]() Etiologies responsible for exfoliative dermatitis include (in decreasing order of incidence) generalized flares of preexisting skin disease (eg, psoriasis, atopic and seborrheic dermatitides, lichen planus, and pemphigus foliaceus), contact dermatitis, malignancy, and medications or chemicals.
Etiologies responsible for exfoliative dermatitis include (in decreasing order of incidence) generalized flares of preexisting skin disease (eg, psoriasis, atopic and seborrheic dermatitides, lichen planus, and pemphigus foliaceus), contact dermatitis, malignancy, and medications or chemicals.
CLINICAL FEATURES
![]() Patients may present with acute, acute-on-chronic, or chronic disease.
Patients may present with acute, acute-on-chronic, or chronic disease.
![]() The acute-onset form is encountered most often in cases involving medications, contact allergens, or malignancy, while the chronic variety usually is related to an underlying cutaneous disease.
The acute-onset form is encountered most often in cases involving medications, contact allergens, or malignancy, while the chronic variety usually is related to an underlying cutaneous disease.
![]() Patients may complain of pain, pruritus, tightening of the skin, a chilling sensation of the skin, fever, nausea, vomiting, weight loss, and fatigue.
Patients may complain of pain, pruritus, tightening of the skin, a chilling sensation of the skin, fever, nausea, vomiting, weight loss, and fatigue.
![]() The physical examination may show generalized warmth and erythroderma, scaling with desiccation, and exfoliation of the skin, as well as fever and other signs of systemic toxicity.
The physical examination may show generalized warmth and erythroderma, scaling with desiccation, and exfoliation of the skin, as well as fever and other signs of systemic toxicity.
![]() The process usually begins on the face and upper trunk with progression to other skin surfaces.
The process usually begins on the face and upper trunk with progression to other skin surfaces.
![]() Chronic findings include dystrophic nails, thinning of body hair, alopecia, and hypo- or hyperpigmentation.
Chronic findings include dystrophic nails, thinning of body hair, alopecia, and hypo- or hyperpigmentation.
![]() Acute complicating factors include fluid and electrolyte losses, secondary infection, and excessive heat loss with hypothermia.
Acute complicating factors include fluid and electrolyte losses, secondary infection, and excessive heat loss with hypothermia.
![]() High-output congestive heart failure (CHF) may be noted due to extensive cutaneous vasodilation in poorly compensated individuals.
High-output congestive heart failure (CHF) may be noted due to extensive cutaneous vasodilation in poorly compensated individuals.
DIAGNOSIS AND DIFFERENTIAL
![]() Diffuse erythema with desiccation or exfoliation must be considered exfoliative dermatitis until proven otherwise.
Diffuse erythema with desiccation or exfoliation must be considered exfoliative dermatitis until proven otherwise.
![]() Diagnosis of exfoliative dermatitis is confirmed by skin biopsy.
Diagnosis of exfoliative dermatitis is confirmed by skin biopsy.
![]() The differential diagnosis includes acute generalized exanthematous pustulosis, TEN, primary blistering disorders, Kawasaki’s disease, and the toxic-infectious erythemas.
The differential diagnosis includes acute generalized exanthematous pustulosis, TEN, primary blistering disorders, Kawasaki’s disease, and the toxic-infectious erythemas.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Correct hypothermia and hypovolemia with appropriate correction of any life-threatening abnormality.
Correct hypothermia and hypovolemia with appropriate correction of any life-threatening abnormality.
![]() After resuscitation has been completed, treatment of secondary infection, correction of electrolyte disorders, and management of CHF are clinical issues to address.
After resuscitation has been completed, treatment of secondary infection, correction of electrolyte disorders, and management of CHF are clinical issues to address.
![]() For patients with a new presentation or a significant recurrence of exfoliative dermatitis, admission with dermatologic consultation is advised. Systemic steroids are commonly given after consultation.
For patients with a new presentation or a significant recurrence of exfoliative dermatitis, admission with dermatologic consultation is advised. Systemic steroids are commonly given after consultation.
![]() For patients with chronic disease with mild recurrence who are not systemically ill, outpatient treatment with prompt dermatologic follow-up is reasonable.
For patients with chronic disease with mild recurrence who are not systemically ill, outpatient treatment with prompt dermatologic follow-up is reasonable.
TOXIC-INFECTIOUS ERYTHEMAS
PATHOPHYSIOLOGY
![]() Toxic-infectious erythemas include toxic shock syndrome (TSS), streptococcal toxic shock syndrome (STSS), and staphylococcal scalded-skin syndrome (SSSS).
Toxic-infectious erythemas include toxic shock syndrome (TSS), streptococcal toxic shock syndrome (STSS), and staphylococcal scalded-skin syndrome (SSSS).
![]() TSS is a multisystem illness presenting with fever, shock, and erythroderma followed by desquamation associated with toxigenic Staphylococcus aureus.
TSS is a multisystem illness presenting with fever, shock, and erythroderma followed by desquamation associated with toxigenic Staphylococcus aureus.
![]() The causative agent of STSS is Streptococcus pyogenes (group A strep).
The causative agent of STSS is Streptococcus pyogenes (group A strep).
![]() SSSS is divided into three stages: (1) initial (erythroderma), (2) exfoliative, and (3) desquamation (recovery).
SSSS is divided into three stages: (1) initial (erythroderma), (2) exfoliative, and (3) desquamation (recovery).
![]() In SSSS, exotoxins released by bacteria cause acantholysis and intraepidermal cleavage of the skin.
In SSSS, exotoxins released by bacteria cause acantholysis and intraepidermal cleavage of the skin.
![]() SSSS occurs primarily in infants, young children, and the immunocompromised.
SSSS occurs primarily in infants, young children, and the immunocompromised.
CLINICAL FEATURES
![]() The manifestations of TSS range from a mild, trivial disease to a rapidly progressive, potentially fatal, multisystem illness.
The manifestations of TSS range from a mild, trivial disease to a rapidly progressive, potentially fatal, multisystem illness.
![]() The dermatologic hallmark of TSS is a nonpruritic, blanching macular erythroderma.
The dermatologic hallmark of TSS is a nonpruritic, blanching macular erythroderma.
![]() The clinical presentation of STSS is similar to that of TSS; in fact, similar criteria may be used for the diagnosis.
The clinical presentation of STSS is similar to that of TSS; in fact, similar criteria may be used for the diagnosis.
![]() STSS presents with fever, hypotension, and skin infections.
STSS presents with fever, hypotension, and skin infections.
![]() The majority of cases of STSS are associated with soft tissue infections; cellulitis, myositis, and fasciitis were the most common presenting diagnoses.
The majority of cases of STSS are associated with soft tissue infections; cellulitis, myositis, and fasciitis were the most common presenting diagnoses.
![]() In SSSS, there is a sudden appearance of a tender, diffuse erythroderma. The involved skin may have a sandpaper texture similar to the rash of scarlet fever.
In SSSS, there is a sudden appearance of a tender, diffuse erythroderma. The involved skin may have a sandpaper texture similar to the rash of scarlet fever.
![]() The exfoliative stage of SSSS begins on the second day of the illness with a wrinkling and peeling of the previously erythematous skin; Nikolsky’s sign is found. Large, flaccid, fluid-filled bullae and vesicles then appear. These lesions easily rupture and are shed in large sheets; the underlying tissue resembles scalded skin and rapidly desiccates.
The exfoliative stage of SSSS begins on the second day of the illness with a wrinkling and peeling of the previously erythematous skin; Nikolsky’s sign is found. Large, flaccid, fluid-filled bullae and vesicles then appear. These lesions easily rupture and are shed in large sheets; the underlying tissue resembles scalded skin and rapidly desiccates.
![]() During the exfoliative phase of SSSS, the patient is often febrile and irritable. After 3 to 5 days of illness, the involved skin desquamates, leaving normal skin in 7 to 10 days.
During the exfoliative phase of SSSS, the patient is often febrile and irritable. After 3 to 5 days of illness, the involved skin desquamates, leaving normal skin in 7 to 10 days.
DIAGNOSIS AND DIFFERENTIAL
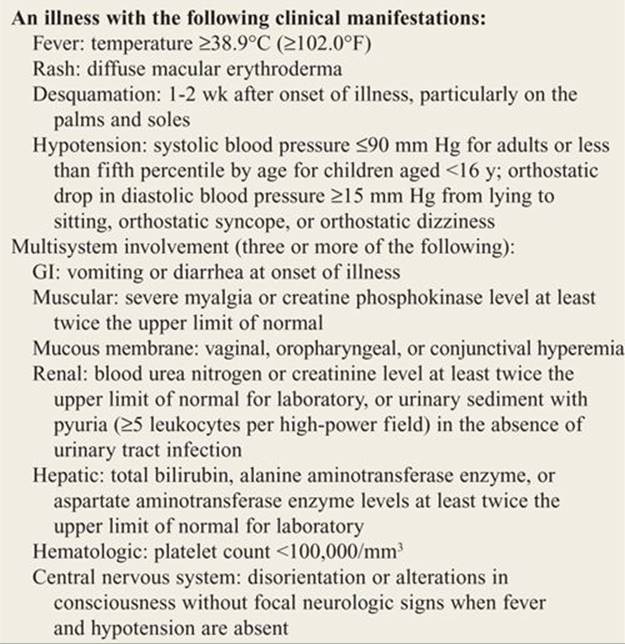
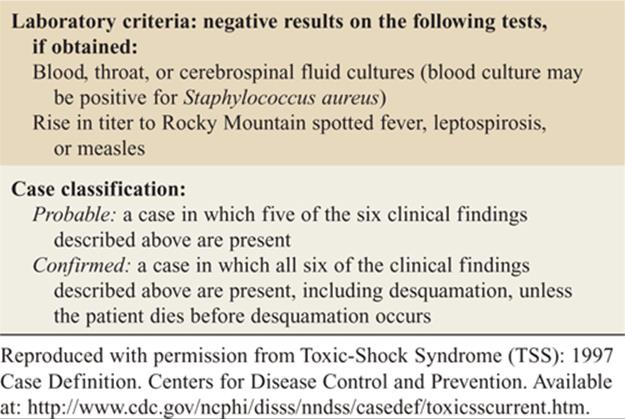
![]() The diagnosis of TSS requires fever, hypotension, rash, desquamation, and the involvement of three or more systems (Table 156-1).
The diagnosis of TSS requires fever, hypotension, rash, desquamation, and the involvement of three or more systems (Table 156-1).
![]() For TSS and STSS, fever and hypotension with associated erythroderma should suggest the diagnosis.
For TSS and STSS, fever and hypotension with associated erythroderma should suggest the diagnosis.
![]() Infants and toddlers with fever and diffuse erythroderma suggest SSSS.
Infants and toddlers with fever and diffuse erythroderma suggest SSSS.
TABLE 156-1 case Definition of Toxic Shock Syndrome
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Management of patients withTSS and STSS is dictated by the severity of their illness. If the patient presents in extremis, airway control, ventilatory status, and hemodynamic status should be addressed emergently.
Management of patients withTSS and STSS is dictated by the severity of their illness. If the patient presents in extremis, airway control, ventilatory status, and hemodynamic status should be addressed emergently.
![]() Patients must be checked for evidence of organ system dysfunction. The vast majority of patients with TSS require hospital admission; the patient who is critically ill is best managed in the intensive care setting.
Patients must be checked for evidence of organ system dysfunction. The vast majority of patients with TSS require hospital admission; the patient who is critically ill is best managed in the intensive care setting.
![]() Management of the patient with SSSS includes fluid resuscitation and correction of electrolyte abnormalities, as well as identification and treatment of the source of the toxigenic Staphylococcus with the appropriate antistaphylococcal antibiotic, including nafcillin, oxacillin, and clindamycin.
Management of the patient with SSSS includes fluid resuscitation and correction of electrolyte abnormalities, as well as identification and treatment of the source of the toxigenic Staphylococcus with the appropriate antistaphylococcal antibiotic, including nafcillin, oxacillin, and clindamycin.
![]() The newborn may be treated with topical sulfadiazine or its equivalent.
The newborn may be treated with topical sulfadiazine or its equivalent.
![]() Corticosteroids are not recommended.
Corticosteroids are not recommended.
DISSEMINATED GONOCOCCAL INFECTION
PATHOPHYSIOLOGY
![]() Generally 0.5% to 3.0% of patients with mucosal lesions develop disseminated disease.
Generally 0.5% to 3.0% of patients with mucosal lesions develop disseminated disease.
![]() The incidence is higher for those in late pregnancy, immediate postpartum period, or within 1 week of onset of menses.
The incidence is higher for those in late pregnancy, immediate postpartum period, or within 1 week of onset of menses.
CLINICAL FEATURES
![]() Fever, arthralgias, and multiple papular, vesicular, or pustular skin lesions are noted.
Fever, arthralgias, and multiple papular, vesicular, or pustular skin lesions are noted.
![]() Rash develops on dorsal aspects of ankles and feet.
Rash develops on dorsal aspects of ankles and feet.
![]() Lesions are initially small red papules or maculopapules; they either resolve or evolve into vesicles with purulent fluid and central necrosis.
Lesions are initially small red papules or maculopapules; they either resolve or evolve into vesicles with purulent fluid and central necrosis.
DIAGNOSIS AND DIFFERENTIAL
![]() Diagnosis is made in sexually active persons with tenosynovitis, arthralgias, and appropriate dermatologic symptoms.
Diagnosis is made in sexually active persons with tenosynovitis, arthralgias, and appropriate dermatologic symptoms.
![]() Gram’s stain of lesion fluid may show Neisseria gonorrhoeae. Blood cultures may be positive.
Gram’s stain of lesion fluid may show Neisseria gonorrhoeae. Blood cultures may be positive.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Parenteral ceftriaxone, cefotaxime, ceftizoxime, or spectinomycin should be administered for 7 days.
Parenteral ceftriaxone, cefotaxime, ceftizoxime, or spectinomycin should be administered for 7 days.
![]() Fluoroqinolones are no longer recommended.
Fluoroqinolones are no longer recommended.
MENINGOCOCCEMIA
PATHOPHYSIOLOGY
![]() Meningococcemia is a potentially fatal infectious illness caused by Neisseria meningitidis.
Meningococcemia is a potentially fatal infectious illness caused by Neisseria meningitidis.
![]() It has a wide clinical spectrum, including pharyngitis, meningitis, and bacteremia.
It has a wide clinical spectrum, including pharyngitis, meningitis, and bacteremia.
![]() Illness typically affects patients under 20 years of age. Epidemics are seen with very virulent strains.
Illness typically affects patients under 20 years of age. Epidemics are seen with very virulent strains.
CLINICAL FEATURES
![]() Infection develops usually within 3 to 4 days (range 2-10 days) after exposure and presents with severe headache, fever, altered mental status, nausea, vomiting, myalgias, arthralgia, and neck stiffness.
Infection develops usually within 3 to 4 days (range 2-10 days) after exposure and presents with severe headache, fever, altered mental status, nausea, vomiting, myalgias, arthralgia, and neck stiffness.
![]() Dermatologic manifestations include petechiae, urticaria, hemorrhagic vesicles, and macules.
Dermatologic manifestations include petechiae, urticaria, hemorrhagic vesicles, and macules.
DIAGNOSIS AND DIFFERENTIAL
![]() Diagnosis relies on clinical suspicion based on presentation of an ill-appearing patient with petechial rash and associated symptoms.
Diagnosis relies on clinical suspicion based on presentation of an ill-appearing patient with petechial rash and associated symptoms.
![]() Cerebrospinal fluid cultures may be positive.
Cerebrospinal fluid cultures may be positive.
![]() The differential diagnosis includes Rocky Mountain spotted fever, TSS, gonococcemia, bacterial endocarditis, vasculitis, viral and bacterial infection, and disseminated intravascular coagulation.
The differential diagnosis includes Rocky Mountain spotted fever, TSS, gonococcemia, bacterial endocarditis, vasculitis, viral and bacterial infection, and disseminated intravascular coagulation.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Ceftriaxone 2 grams IV and vancomycin 1 gram IV should be administered empirically as soon as the disease is suspected.
Ceftriaxone 2 grams IV and vancomycin 1 gram IV should be administered empirically as soon as the disease is suspected.
![]() Hospital admission is necessary.
Hospital admission is necessary.
PEMPHIGUS VULGARIS
PATHOPHYSIOLOGY
![]() Pemphigus vulgaris (PV) is a generalized mucocutaneous autoimmune blistering eruption characterized by intraepidermal acantholytic blistering.
Pemphigus vulgaris (PV) is a generalized mucocutaneous autoimmune blistering eruption characterized by intraepidermal acantholytic blistering.
CLINICAL FEATURES
![]() The primary lesions of PV are vesicles or bullae that vary in diameter from less than 1 cm to several centimeters, commonly first affecting the head, trunk, and mucous membranes.
The primary lesions of PV are vesicles or bullae that vary in diameter from less than 1 cm to several centimeters, commonly first affecting the head, trunk, and mucous membranes.
![]() The blisters are usually clear and tense, originating from normal skin or atop an erythematous or urticarial plaque. Within 2 to 3 days, the bullae become turbid and flaccid with rupture soon following, producing painful, denuded areas. These erosions are slow to heal and prone to secondary infection.
The blisters are usually clear and tense, originating from normal skin or atop an erythematous or urticarial plaque. Within 2 to 3 days, the bullae become turbid and flaccid with rupture soon following, producing painful, denuded areas. These erosions are slow to heal and prone to secondary infection.
![]() Nikolsky’s sign is positive in PV and absent in other autoimmune blistering diseases. Mucous membranes are affected in most patients.
Nikolsky’s sign is positive in PV and absent in other autoimmune blistering diseases. Mucous membranes are affected in most patients.
DIAGNOSIS AND DIFFERENTIAL
![]() Diagnosis is suspected with the appearance of the blistering lesions and confirmed by skin biopsy and immunofluorescence testing.
Diagnosis is suspected with the appearance of the blistering lesions and confirmed by skin biopsy and immunofluorescence testing.
![]() The differential diagnosis of PV includes all of those diseases that can present with primary skin blistering, including TEN, EM, other autoimmune blistering diseases, burns, severe contact dermatitis, bullous diabeticorum, and friction blisters.
The differential diagnosis of PV includes all of those diseases that can present with primary skin blistering, including TEN, EM, other autoimmune blistering diseases, burns, severe contact dermatitis, bullous diabeticorum, and friction blisters.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Patients with PV should be hospitalized with early dermatologic consultant; begin high-dose parenteral steroids and other immunosuppressive drugs to prevent mortality.
Patients with PV should be hospitalized with early dermatologic consultant; begin high-dose parenteral steroids and other immunosuppressive drugs to prevent mortality.
![]() Close observation and rapid treatment with appropriate antibiotics for secondary infection of erosions is imperative.
Close observation and rapid treatment with appropriate antibiotics for secondary infection of erosions is imperative.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 245, “Serious Generalized Skin Disorders,” by J. Jeremy Thomas, Andrew D. Perron, and William J. Brady.