Sandra L. Najarian
STERNOCLAVICULAR JOINT SPRAINS AND DISLOCATION
PATHOPHYSIOLOGY
![]() The sternoclavicular joint is the most frequently moved, nonaxial joint of the body. Sprains are more common than dislocations or fractures.
The sternoclavicular joint is the most frequently moved, nonaxial joint of the body. Sprains are more common than dislocations or fractures.
![]() Injuries result from direct trauma or forceful rolling of the shoulder forward or backward.
Injuries result from direct trauma or forceful rolling of the shoulder forward or backward.
![]() Anterior dislocations are more common than posterior dislocations.
Anterior dislocations are more common than posterior dislocations.
![]() Posterior dislocations can be associated with life-threatening injuries to mediastinal contents.
Posterior dislocations can be associated with life-threatening injuries to mediastinal contents.
CLINICAL FEATURES
![]() Patients with simple sprains have pain and tenderness localized to the joint, whereas patients with dislocations have severe pain that is exacerbated by arm motion and lying supine.
Patients with simple sprains have pain and tenderness localized to the joint, whereas patients with dislocations have severe pain that is exacerbated by arm motion and lying supine.
![]() The medial clavicle is visibly prominent and palpable anterior to the sternum in anterior dislocations.
The medial clavicle is visibly prominent and palpable anterior to the sternum in anterior dislocations.
![]() The medial clavicle is less visible and often not palpable in posterior dislocations.
The medial clavicle is less visible and often not palpable in posterior dislocations.
![]() Symptoms of hoarseness, dysphagia, dyspnea, upper extremity paresthesias, or weakness may indicate life-threatening injuries to mediastinal contents, such as pneumothorax or compression or laceration of surrounding great vessels, trachea, and esophagus.
Symptoms of hoarseness, dysphagia, dyspnea, upper extremity paresthesias, or weakness may indicate life-threatening injuries to mediastinal contents, such as pneumothorax or compression or laceration of surrounding great vessels, trachea, and esophagus.
DIAGNOSIS AND DIFFERENTIAL
![]() CT is the imaging test of choice, and IV contrast may be needed to detect injury to adjacent mediastinal structures.
CT is the imaging test of choice, and IV contrast may be needed to detect injury to adjacent mediastinal structures.
![]() Consider septic arthritis in the nontraumatic patient, especially in injection drug users.
Consider septic arthritis in the nontraumatic patient, especially in injection drug users.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment for sprains and uncomplicated anterior dislocations includes arm sling, ice, analgesics, and orthopedic referral. Attempted closed reduction is not necessary.
Treatment for sprains and uncomplicated anterior dislocations includes arm sling, ice, analgesics, and orthopedic referral. Attempted closed reduction is not necessary.
![]() All posterior dislocations require urgent orthopedic consultation for operative reduction.
All posterior dislocations require urgent orthopedic consultation for operative reduction.
CLAVICLE AND SCAPULA FRACTURES
PATHOPHYSIOLOGY
![]() A direct blow to the shoulder or fall on an outstretched hand is the most common mechanism for fracture.
A direct blow to the shoulder or fall on an outstretched hand is the most common mechanism for fracture.
![]() The middle third of the clavicle is involved in 80% of clavicle fractures.
The middle third of the clavicle is involved in 80% of clavicle fractures.
![]() Associated injuries to the adjacent lung and neurovascular structures rarely occur with clavicle fractures.
Associated injuries to the adjacent lung and neurovascular structures rarely occur with clavicle fractures.
![]() Scapula fractures have a high incidence (>75%) of associated injuries to the thoracic cage, ipsilateral lung, and shoulder girdle. The scapula is well protected and requires a significant force to break.
Scapula fractures have a high incidence (>75%) of associated injuries to the thoracic cage, ipsilateral lung, and shoulder girdle. The scapula is well protected and requires a significant force to break.
![]() Rib fractures are the most common injury associated with scapula fracture.
Rib fractures are the most common injury associated with scapula fracture.
CLINICAL FEATURES
![]() Patients with clavicle fracture have localized tenderness, swelling, and deformity overlying the clavicle.
Patients with clavicle fracture have localized tenderness, swelling, and deformity overlying the clavicle.
![]() Patients with scapula fractures have localized tenderness over the scapula, hold the ipsilateral arm in adduction, and resist any arm movement.
Patients with scapula fractures have localized tenderness over the scapula, hold the ipsilateral arm in adduction, and resist any arm movement.
DIAGNOSIS AND DIFFERENTIAL
![]() Routine radiographs can miss clavicle and scapula fractures.
Routine radiographs can miss clavicle and scapula fractures.
![]() CT can confirm the diagnosis of scapula fracture as well as identify any associated pathology.
CT can confirm the diagnosis of scapula fracture as well as identify any associated pathology.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment includes sling immobilization, ice, analgesics, and early range of motion exercises.
Treatment includes sling immobilization, ice, analgesics, and early range of motion exercises.
![]() Orthopedic consultation is warranted for clavicle fractures that are open, have neurovascular compromise, or have persistent skin tenting or interposition of soft tissue.
Orthopedic consultation is warranted for clavicle fractures that are open, have neurovascular compromise, or have persistent skin tenting or interposition of soft tissue.
![]() The presence of scapular fracture mandates an investigation for associated intrathoracic injuries.
The presence of scapular fracture mandates an investigation for associated intrathoracic injuries.
![]() Displaced glenoid articular fractures, angulated gle-noid neck fractures, and certain acromial and cora-coid fractures may require surgical intervention.
Displaced glenoid articular fractures, angulated gle-noid neck fractures, and certain acromial and cora-coid fractures may require surgical intervention.
ACROMIOCLAVICULAR JOINT INJURIES
CLINICAL FEATURES
![]() Injuries range from mild sprain to complete disruption of all ligaments that attach the scapula and clavicle.
Injuries range from mild sprain to complete disruption of all ligaments that attach the scapula and clavicle.
![]() The mechanism of injury is usually from direct trauma to the shoulder with arm adducted, such as a sports-related injury.
The mechanism of injury is usually from direct trauma to the shoulder with arm adducted, such as a sports-related injury.
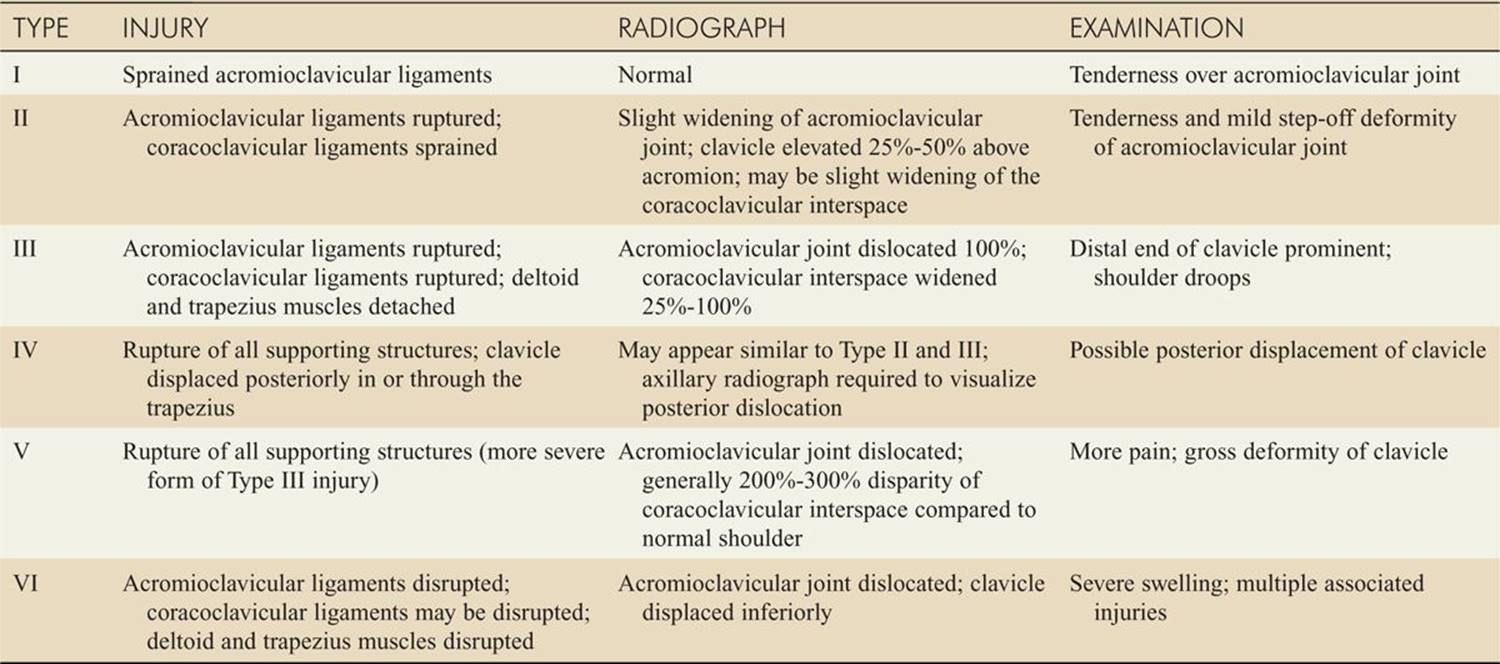
![]() Patients typically present with tenderness and deformity at the acromioclavicular joint. The classification of injuries and their physical findings are outlined in Table 174-1.
Patients typically present with tenderness and deformity at the acromioclavicular joint. The classification of injuries and their physical findings are outlined in Table 174-1.
TABLE 174-1 Classification and Physical Findings in Acromioclavicular Joint Injuries
DIAGNOSIS AND DIFFERENTIAL
![]() Diagnosis is often clinical.
Diagnosis is often clinical.
![]() Stress radiographs are low yield and not recommended.
Stress radiographs are low yield and not recommended.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment for Type I and II injuries includes sling immobilization, ice, analgesics, and early range of motion exercises at 7 to 14 days.
Treatment for Type I and II injuries includes sling immobilization, ice, analgesics, and early range of motion exercises at 7 to 14 days.
![]() Treatment for Type III injuries is controversial, but the trend favors conservative management with sling immobilization.
Treatment for Type III injuries is controversial, but the trend favors conservative management with sling immobilization.
![]() Type IV, V, and VI injuries are severe and require urgent orthopedic consultation for surgical repair.
Type IV, V, and VI injuries are severe and require urgent orthopedic consultation for surgical repair.
GLENOHUMERAL JOINT DISLOCATION
CLINICAL FEATURES
![]() The most common major joint dislocation is the glenohumeral joint dislocation.
The most common major joint dislocation is the glenohumeral joint dislocation.
![]() The majority of glenohumeral joint dislocations are anterior.
The majority of glenohumeral joint dislocations are anterior.
![]() The axillary nerve is the most common neurovascular structure injured in anterior dislocations and is tested by pinprick sensation over the skin of the lateral deltoid muscle.
The axillary nerve is the most common neurovascular structure injured in anterior dislocations and is tested by pinprick sensation over the skin of the lateral deltoid muscle.
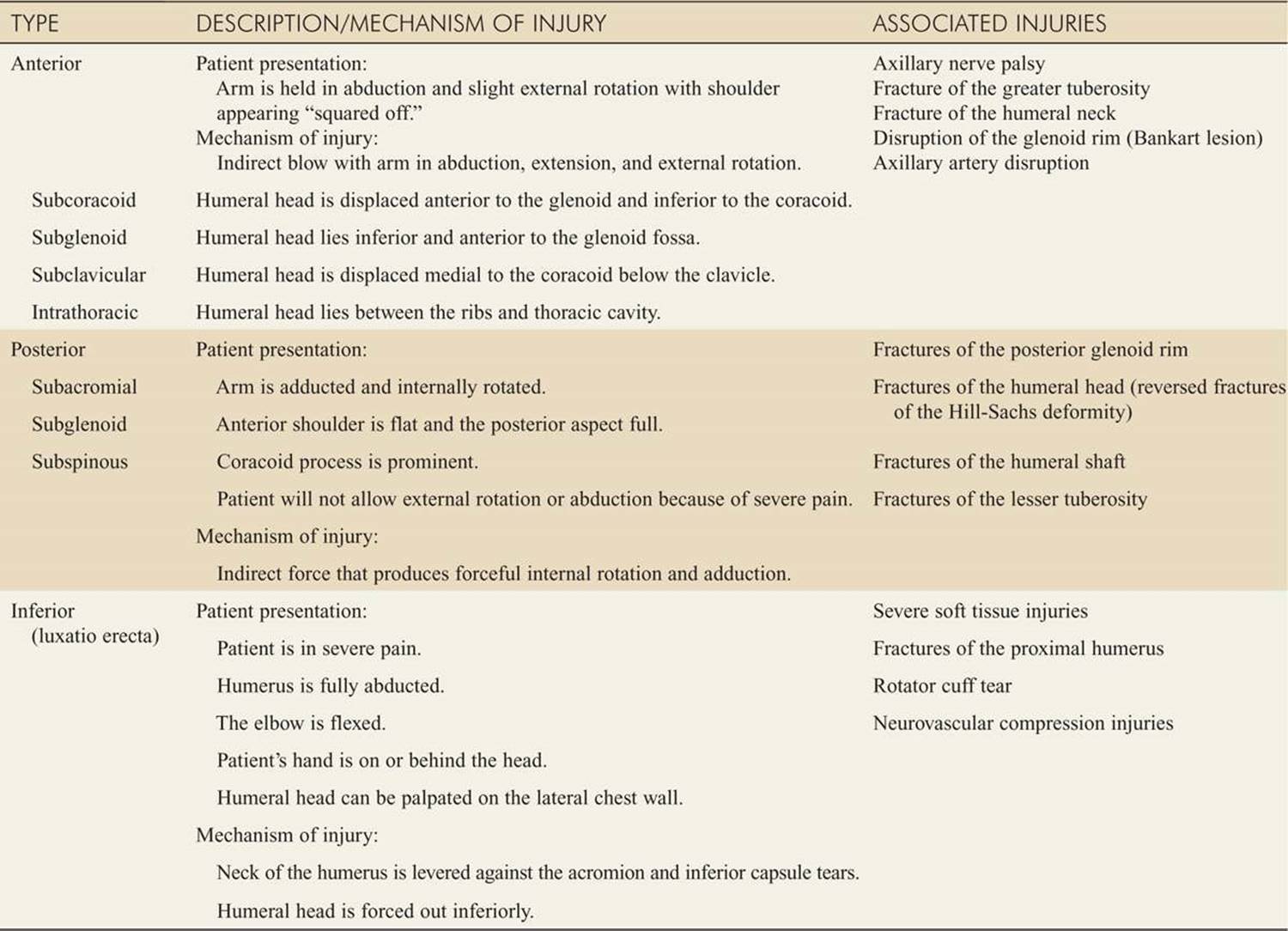
![]() Table 174-2 describes the various mechanisms of injury, physical findings, and associated injuries with each type of glenohumeral joint dislocation.
Table 174-2 describes the various mechanisms of injury, physical findings, and associated injuries with each type of glenohumeral joint dislocation.
TABLE 174-2 Classification and Physical Findings in Dislocations of the Glenohumeral Joint
DIAGNOSIS AND DIFFERENTIAL
![]() AP and scapular “Y” view radiographs confirm the type of dislocation and identify any associated fractures.
AP and scapular “Y” view radiographs confirm the type of dislocation and identify any associated fractures.
![]() The presence of minor fractures, such as a Hill–Sachs lesion or Bankart fracture, does not change ED management.
The presence of minor fractures, such as a Hill–Sachs lesion or Bankart fracture, does not change ED management.
![]() Consider omitting pre-reduction radiographs in patients with a history of recurrent shoulder dislocation who present with signs and symptoms of a recurrence in the absence of trauma.
Consider omitting pre-reduction radiographs in patients with a history of recurrent shoulder dislocation who present with signs and symptoms of a recurrence in the absence of trauma.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Main reduction techniques include traction, leverage, and scapular manipulation.
Main reduction techniques include traction, leverage, and scapular manipulation.
![]() Procedural sedation is recommended; however, an intra-articular injection of 10 to 20 mL of 1% lido-caine can facilitate reduction and may obviate the need for sedation.
Procedural sedation is recommended; however, an intra-articular injection of 10 to 20 mL of 1% lido-caine can facilitate reduction and may obviate the need for sedation.
![]() Assess neurovascular status and provide sling immobilization after reduction.
Assess neurovascular status and provide sling immobilization after reduction.
![]() Post-reduction radiographs are useful for confirmation and documentation of successful reduction.
Post-reduction radiographs are useful for confirmation and documentation of successful reduction.
![]() Urgent orthopedic follow-up is necessary. Shoulder dislocations associated with proximal humerus fractures often mandate orthopedic consultation for surgical repair.
Urgent orthopedic follow-up is necessary. Shoulder dislocations associated with proximal humerus fractures often mandate orthopedic consultation for surgical repair.
HUMERUS FRACTURES
CLINICAL FEATURES
![]() Proximal humerus fractures typically occur in elderly patients with osteoporosis after a fall on an outstretched hand.
Proximal humerus fractures typically occur in elderly patients with osteoporosis after a fall on an outstretched hand.
![]() Humeral shaft fractures typically occur in active young men and elderly women after direct or indirect trauma to the humeral shaft.
Humeral shaft fractures typically occur in active young men and elderly women after direct or indirect trauma to the humeral shaft.
![]() Patients with proximal humerus fractures present with pain, swelling, ecchymosis, and tenderness over the shoulder with the arm held in adduction.
Patients with proximal humerus fractures present with pain, swelling, ecchymosis, and tenderness over the shoulder with the arm held in adduction.
![]() Patients with humeral shaft fractures present with localized pain, swelling, tenderness, and abnormal mobility. Shortening of the upper extremity is present in displaced shaft fractures.
Patients with humeral shaft fractures present with localized pain, swelling, tenderness, and abnormal mobility. Shortening of the upper extremity is present in displaced shaft fractures.
![]() The axillary nerve and the radial nerve are the most commonly injured nerves in proximal humerus and humeral shaft fractures, respectively.
The axillary nerve and the radial nerve are the most commonly injured nerves in proximal humerus and humeral shaft fractures, respectively.
DIAGNOSIS AND DIFFERENTIAL
![]() Radiographs are confirmatory.
Radiographs are confirmatory.
![]() The Neer classification system divides the proximal humerus into four “parts” (the articular surface of the humeral head, the greater tubercle, the lesser tubercle, and the diaphysis of the humerus) and is used to guide treatment.
The Neer classification system divides the proximal humerus into four “parts” (the articular surface of the humeral head, the greater tubercle, the lesser tubercle, and the diaphysis of the humerus) and is used to guide treatment.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Proximal humerus fractures that are nondisplaced or one-part fractures (displaced less than 1 cm or angu-lated less than 45 degrees) require sling immobilization, ice, analgesics, and orthopedic referral.
Proximal humerus fractures that are nondisplaced or one-part fractures (displaced less than 1 cm or angu-lated less than 45 degrees) require sling immobilization, ice, analgesics, and orthopedic referral.
![]() Humeral shaft fractures that are nondisplaced require a coaptation splint (sugar tong), hanging cast, or functional bracing.
Humeral shaft fractures that are nondisplaced require a coaptation splint (sugar tong), hanging cast, or functional bracing.
![]() Multipart proximal humerus fractures, significantly displaced or angulated shaft fractures, open fractures, or any fracture with neurovascular injuries require immediate orthopedic consultation.
Multipart proximal humerus fractures, significantly displaced or angulated shaft fractures, open fractures, or any fracture with neurovascular injuries require immediate orthopedic consultation.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 268, “Shoulder and Humerus Injuries,” by John R Rudzinski, Laura M. Pittman, Dennis T. Uehara.