Michael P. Kefer
INTRODUCTION
![]() Rest and elevation are the mainstays of treatment for many inflammatory conditions of the hand. This helps to decrease inflammation, avoid secondary injury, and prevent spread of any existing infection.
Rest and elevation are the mainstays of treatment for many inflammatory conditions of the hand. This helps to decrease inflammation, avoid secondary injury, and prevent spread of any existing infection.
![]() The optimal position for splinting the hand is the position of function: wrist in 15-degree extension, metacarpophalangeal (MCP) joint in 50- to 90-degree flexion, proximal interphalangeal (PIP) joint in 10- to 15-degree flexion, and distal interphalangeal (DIP) joint in 10- to 15-degree flexion.
The optimal position for splinting the hand is the position of function: wrist in 15-degree extension, metacarpophalangeal (MCP) joint in 50- to 90-degree flexion, proximal interphalangeal (PIP) joint in 10- to 15-degree flexion, and distal interphalangeal (DIP) joint in 10- to 15-degree flexion.
HAND INFECTIONS
![]() Hand infections most commonly occur from injury to the dermis. Skin organisms, Staphylococcus and Streptococcus species, are the most common pathogens.
Hand infections most commonly occur from injury to the dermis. Skin organisms, Staphylococcus and Streptococcus species, are the most common pathogens.
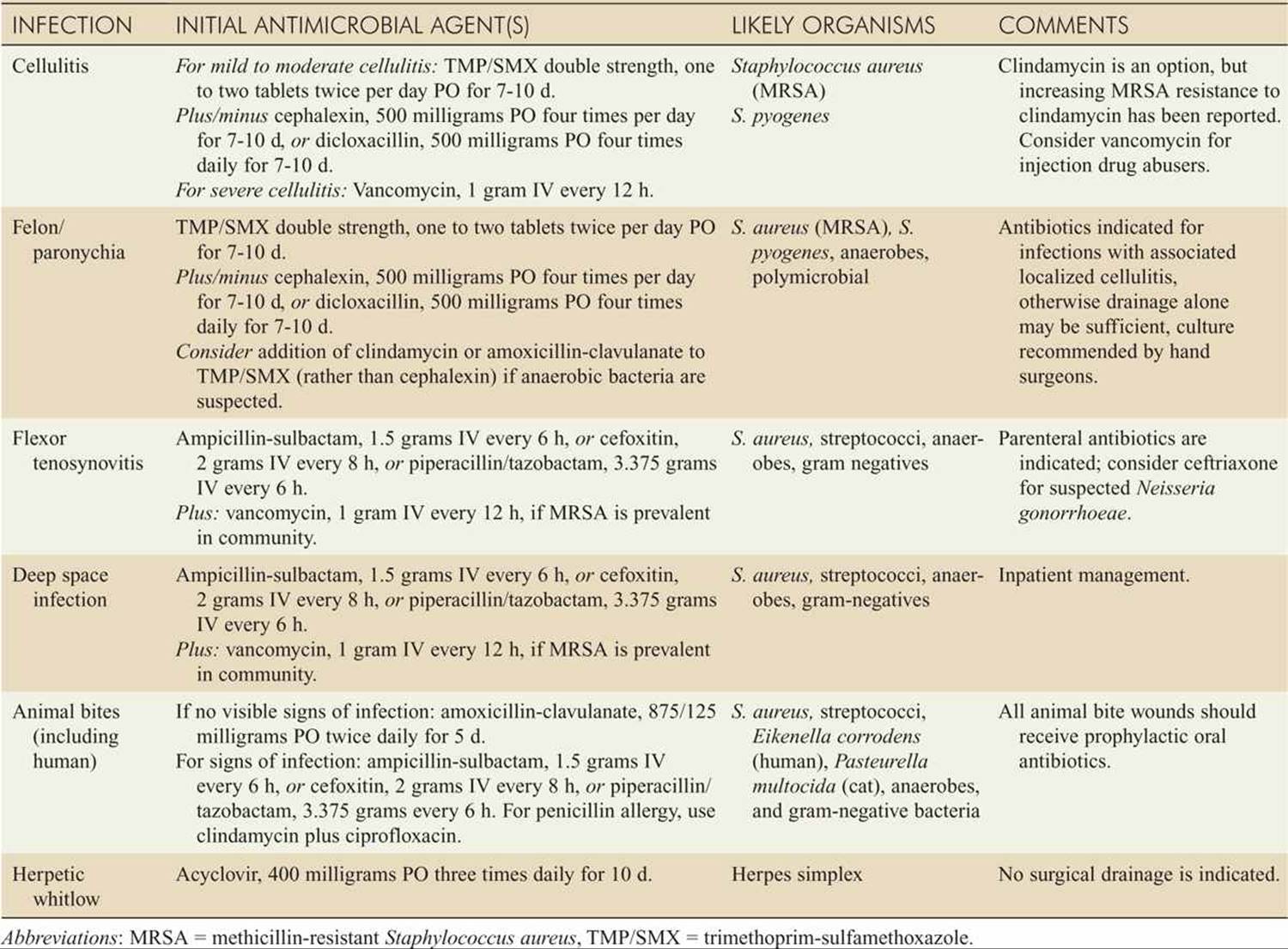
![]() Refer to Table 184-1 for recommended antibiotic therapy for the common hand infections described below.
Refer to Table 184-1 for recommended antibiotic therapy for the common hand infections described below.
CELLULITIS
![]() Presents with localized warmth, erythema, and edema.
Presents with localized warmth, erythema, and edema.
![]() Exclude involvement of deeper structures of the hand by demonstrating absence of tenderness on deep palpation and range of motion.
Exclude involvement of deeper structures of the hand by demonstrating absence of tenderness on deep palpation and range of motion.
![]() Treat with antibiotics, splinting in the position of function, elevation, and close follow-up.
Treat with antibiotics, splinting in the position of function, elevation, and close follow-up.
FLEXOR TENOSYNOVITIS
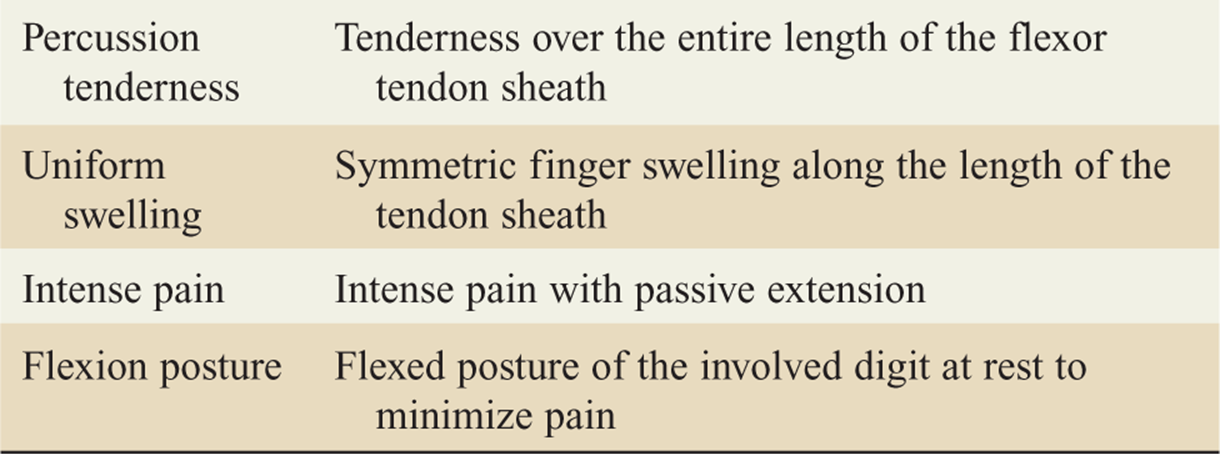
![]() This is a surgical emergency and is diagnosed on examination (Table 184-2).
This is a surgical emergency and is diagnosed on examination (Table 184-2).
![]() Treat with splinting, elevation, IV antibiotics, and hand surgery consult for drainage.
Treat with splinting, elevation, IV antibiotics, and hand surgery consult for drainage.
DEEP SPACE INFECTION
![]() Involves the web or midpalmar space.
Involves the web or midpalmar space.
![]() Web space infection presents as dorsal and volar swelling of the web space causing separation of the affected digits.
Web space infection presents as dorsal and volar swelling of the web space causing separation of the affected digits.
![]() Midpalmar space infection occurs from spread of a flexor tenosynovitis or penetrating wound to the palm, causing infection of the radial or ulnar bursa of the hand.
Midpalmar space infection occurs from spread of a flexor tenosynovitis or penetrating wound to the palm, causing infection of the radial or ulnar bursa of the hand.
![]() Treat with splinting, elevation, IV antibiotics, and hand surgery consult for drainage.
Treat with splinting, elevation, IV antibiotics, and hand surgery consult for drainage.
CLOSED FIST INJURY
![]() Essentially a human bite wound to the MCP joint, this results from a punch to the teeth.
Essentially a human bite wound to the MCP joint, this results from a punch to the teeth.
![]() There is high risk of infection spreading along the extensor tendons.
There is high risk of infection spreading along the extensor tendons.
![]() Wounds penetrating the skin should be explored, irrigated, and allowed to heal by secondary intention.
Wounds penetrating the skin should be explored, irrigated, and allowed to heal by secondary intention.
![]() When inspecting for extensor tendon injury, it is essential to consider the position of the hand at the time of injury.
When inspecting for extensor tendon injury, it is essential to consider the position of the hand at the time of injury.
![]() Treat with splinting, elevation, IV antibiotics, and hand surgery consult.
Treat with splinting, elevation, IV antibiotics, and hand surgery consult.
![]() Extensor tendon repair is delayed until the risk of infection has passed.
Extensor tendon repair is delayed until the risk of infection has passed.
PARONYCHIA
![]() Paronychia is an infection of the lateral nail fold.
Paronychia is an infection of the lateral nail fold.
![]() If there is no pus, treat with warm soaks, elevation, and antibiotics if warranted.
If there is no pus, treat with warm soaks, elevation, and antibiotics if warranted.
![]() Drainage of a small paronychia is by lifting the nail fold with a needle or number 11 blade (see Fig. 184-1).
Drainage of a small paronychia is by lifting the nail fold with a needle or number 11 blade (see Fig. 184-1).
TABLE 184-1 Initial Antibiotic Coverage for Common Hand Infections
![]() If pus is seen beneath the nail, a portion of the nail may have to be removed and packing placed for adequate drainage. Avoid injury to the nail bed.
If pus is seen beneath the nail, a portion of the nail may have to be removed and packing placed for adequate drainage. Avoid injury to the nail bed.
![]() Recheck the wound in 24 to 48 hours, pull the packing, and begin warm soaks.
Recheck the wound in 24 to 48 hours, pull the packing, and begin warm soaks.
FELON
![]() Felon is an infection of the pulp space of the fingertip.
Felon is an infection of the pulp space of the fingertip.
![]() Drainage is by the lateral approach to protect the neurovascular bundle. The incision should remain within the borders of the DIP joint crease proximally and the base of the phalangeal tuft distally. Incise deep enough across the finger pad to divide the septae at the bony insertions.
Drainage is by the lateral approach to protect the neurovascular bundle. The incision should remain within the borders of the DIP joint crease proximally and the base of the phalangeal tuft distally. Incise deep enough across the finger pad to divide the septae at the bony insertions.
TABLE 184-2 Kanavel Four Cardinal Signs of Flexor Tenosynovitis
![]() Unless there is a pointing abscess, the radial aspect of the index and middle fingers and the ulnar aspect of the thumb and small finger should be avoided.
Unless there is a pointing abscess, the radial aspect of the index and middle fingers and the ulnar aspect of the thumb and small finger should be avoided.
![]() Pack the wound. Splint the hand in the position of function.
Pack the wound. Splint the hand in the position of function.
![]() Recheck the wound in 24 to 48 hours, pull the packing, and begin warm soaks.
Recheck the wound in 24 to 48 hours, pull the packing, and begin warm soaks.
HERPETIC WHITLOW
![]() Herpetic whitlow is a viral infection of the fingertip with intracutaneous vesicles.
Herpetic whitlow is a viral infection of the fingertip with intracutaneous vesicles.
![]() Clinically, this may present similar to a felon, but vesicles are present.
Clinically, this may present similar to a felon, but vesicles are present.
![]() Treat with immobilization, elevation, and protection with a dry dressing to prevent autoinoculation and transmission. Antiviral agents may shorten the duration.
Treat with immobilization, elevation, and protection with a dry dressing to prevent autoinoculation and transmission. Antiviral agents may shorten the duration.
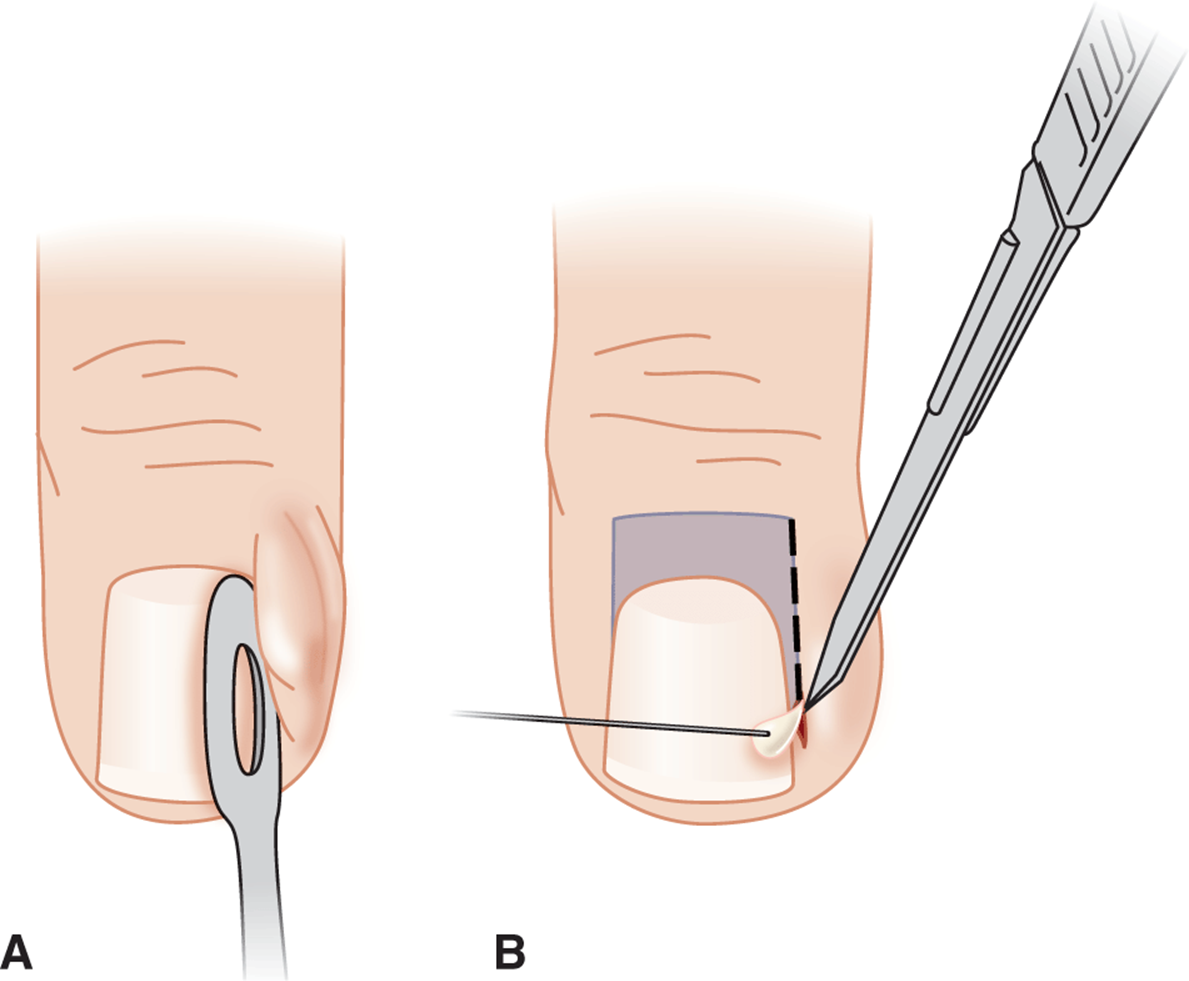
FIG. 184-1. Paronychia. A. The eponychial fold is elevated using a flat probe or a number 11 blade to allow the wound to drain. B. Alternatively, for more extensive infections, a number 11 blade may be used to incise the area of greatest fluctuance directly into the eponychium. The wound may then be gently probed with a small clamp to ensure drainage.
NONINFECTIOUS DISORDERS
TENDINITIS
![]() Tendinitis is usually due to overuse.
Tendinitis is usually due to overuse.
![]() Examination reveals tenderness over the involved tendon.
Examination reveals tenderness over the involved tendon.
![]() Treat with immobilization and nonsteroidal anti-inflammatory drugs (NSAIDs).
Treat with immobilization and nonsteroidal anti-inflammatory drugs (NSAIDs).
TRIGGER FINGER
![]() Results from a tenosynovitis of the flexor sheath of the digit where inflammation or scarring causes stenosis of the sheath.
Results from a tenosynovitis of the flexor sheath of the digit where inflammation or scarring causes stenosis of the sheath.
![]() Impingement and snap release of the tendon occur as the finger is extended from a flexed position.
Impingement and snap release of the tendon occur as the finger is extended from a flexed position.
![]() Steroid injection may be effective in early stages. Definitive treatment is surgery.
Steroid injection may be effective in early stages. Definitive treatment is surgery.
DEQUERVAIN’S TENOSYNOVITIS
![]() Involves the extensor pollicis brevis and abductor pollicis tendons.
Involves the extensor pollicis brevis and abductor pollicis tendons.
![]() Pain occurs at the radial aspect of the wrist and radiates into the forearm.
Pain occurs at the radial aspect of the wrist and radiates into the forearm.
![]() The Finkelstein test is diagnostic: the patient grasps the thumb in the fist and deviates the hand ulnarly, reproducing the pain.
The Finkelstein test is diagnostic: the patient grasps the thumb in the fist and deviates the hand ulnarly, reproducing the pain.
![]() Treat with a thumb spica splint, NSAIDs, and referral.
Treat with a thumb spica splint, NSAIDs, and referral.
CARPAL TUNNEL SYNDROME
![]() Results from compression of the median nerve by the transverse carpal ligament.
Results from compression of the median nerve by the transverse carpal ligament.
![]() The cause is usually edema from overuse, pregnancy, or congestive heart failure.
The cause is usually edema from overuse, pregnancy, or congestive heart failure.
![]() Pain in the median nerve distribution of the hand tends to be worse at night.
Pain in the median nerve distribution of the hand tends to be worse at night.
![]() On examination, pain may be reproduced by tapping over the nerve at the wrist (Tinel’s sign) or by holding the wrist flexed maximally for about 1 minute (Phalen’s sign).
On examination, pain may be reproduced by tapping over the nerve at the wrist (Tinel’s sign) or by holding the wrist flexed maximally for about 1 minute (Phalen’s sign).
![]() Treat with a wrist splint and NSAIDs. Advanced cases require surgical decompression.
Treat with a wrist splint and NSAIDs. Advanced cases require surgical decompression.
DUPUYTREN’S CONTRACTURE
![]() Results from fibrous changes in the subcutaneous tissues of the palm, which may lead to tethering and joint contractures.
Results from fibrous changes in the subcutaneous tissues of the palm, which may lead to tethering and joint contractures.
![]() Refer to hand surgery.
Refer to hand surgery.
GANGLION CYST
![]() Ganglion cyst is a cystic collection of synovial fluid within a joint or tendon sheath.
Ganglion cyst is a cystic collection of synovial fluid within a joint or tendon sheath.
![]() Treat with NSAIDs and referral.
Treat with NSAIDs and referral.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 280, “Nontraumatic Disorders of the Hand,” by Carl A. Germann and Mark W. Foure.