Bret A. Nicks
EPIDEMIOLOGY
![]() Syncope accounts for 1% to 2% of ED visits each year.
Syncope accounts for 1% to 2% of ED visits each year.
![]() The elderly have the highest incidence and risk for morbidity.
The elderly have the highest incidence and risk for morbidity.
![]() Cause remains idiopathic in 40% of patients.
Cause remains idiopathic in 40% of patients.
PATHOPHYSIOLOGY
![]() The final common pathway of syncope is lack of blood flow or vital nutrient delivery to the brain stem reticular activating system, leading to loss of consciousness and postural tone.
The final common pathway of syncope is lack of blood flow or vital nutrient delivery to the brain stem reticular activating system, leading to loss of consciousness and postural tone.
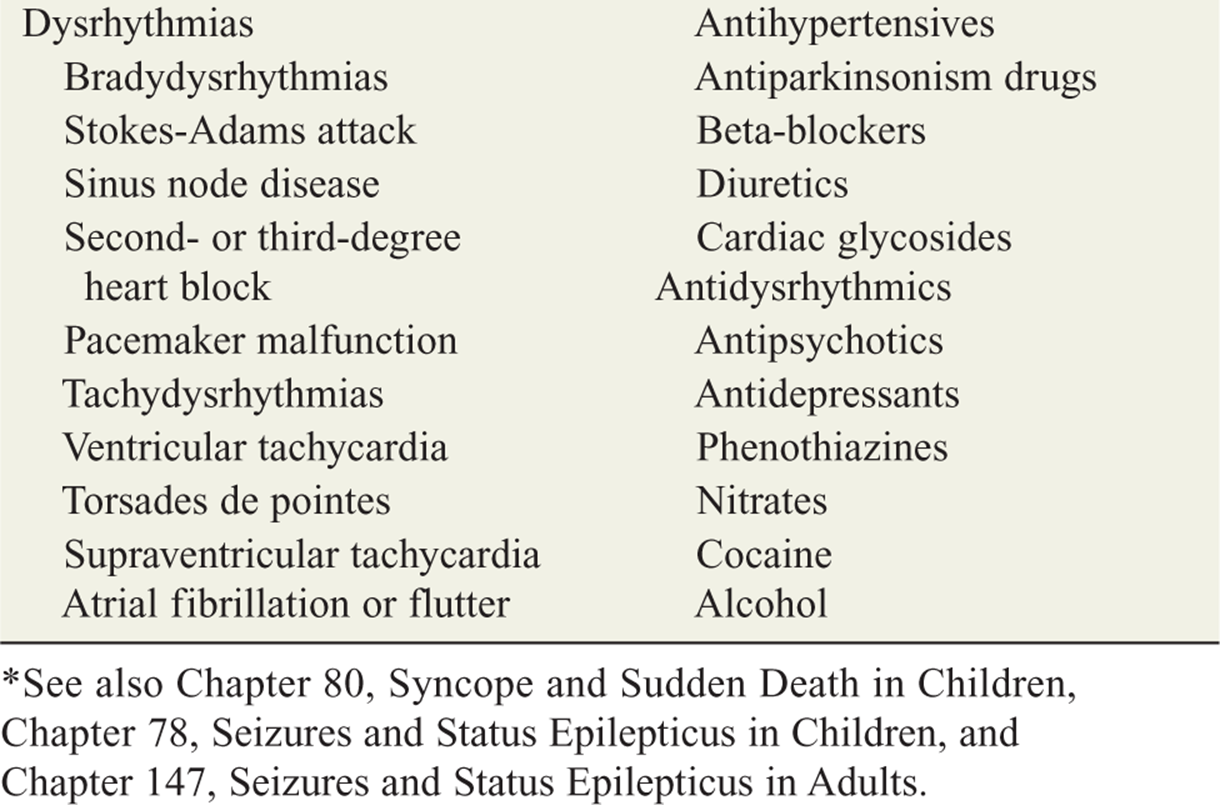
![]() The most common causes of syncope are vasovagal reflex, cardiac-related (structural and dysrhythmias), and orthostatic hypotension (Table 23-1).
The most common causes of syncope are vasovagal reflex, cardiac-related (structural and dysrhythmias), and orthostatic hypotension (Table 23-1).
TABLE 23-1 Causes of Syncope

![]() An inciting event causes a drop in cardiac output, which decreases oxygen and substrate delivery to the brain. The reclined posture and the response of autonomic autoregulation centers re-establish cerebral perfusion, leading to a spontaneous return of consciousness.
An inciting event causes a drop in cardiac output, which decreases oxygen and substrate delivery to the brain. The reclined posture and the response of autonomic autoregulation centers re-establish cerebral perfusion, leading to a spontaneous return of consciousness.
![]() In patients with reflex-mediated (vasovagal) syncope, a stimulus produces an abnormal autonomic response: vagal tone increases. Vasodilatory hypotension with or without bradycardia ensues. Less commonly, the stimulus leads directly to vagal hyperactivity.
In patients with reflex-mediated (vasovagal) syncope, a stimulus produces an abnormal autonomic response: vagal tone increases. Vasodilatory hypotension with or without bradycardia ensues. Less commonly, the stimulus leads directly to vagal hyperactivity.
CLINICAL FEATURES
![]() The most common cause of syncope is reflex-mediated, which leads to inappropriate vagal tone with hypotension and/or bradycardia.
The most common cause of syncope is reflex-mediated, which leads to inappropriate vagal tone with hypotension and/or bradycardia.
![]() Less common causes of syncope include cerebrov-ascular disorders, subarachnoid hemorrhage, and subclavian steal syndrome. Patients with a loss of consciousness with persistent neurologic deficits or altered mental status do not have true syncope.
Less common causes of syncope include cerebrov-ascular disorders, subarachnoid hemorrhage, and subclavian steal syndrome. Patients with a loss of consciousness with persistent neurologic deficits or altered mental status do not have true syncope.
![]() The hallmark of vasovagal syncope is the slow progressive prodrome of dizziness, nausea, diminished vision, pallor, and diaphoresis.
The hallmark of vasovagal syncope is the slow progressive prodrome of dizziness, nausea, diminished vision, pallor, and diaphoresis.
![]() Carotid sinus hypersensitivity, a form of reflex-mediated syncope, may result in bradycardia, asystole (for over 3 seconds), or hypotension. This diagnosis should be considered in older patients with recurrent syncope and negative cardiac evaluations (only 25% of these patients have spontaneous symptoms due to true carotid sinus syndrome).
Carotid sinus hypersensitivity, a form of reflex-mediated syncope, may result in bradycardia, asystole (for over 3 seconds), or hypotension. This diagnosis should be considered in older patients with recurrent syncope and negative cardiac evaluations (only 25% of these patients have spontaneous symptoms due to true carotid sinus syndrome).
![]() Orthostatic syncope results from a sudden change to an upright posture, combined with inability to mount an adequate increase in heart rate and/or peripheral vascular resistance. Orthostasis can be associated with medications, aging, volume depletion, and autonomic dysfunction.
Orthostatic syncope results from a sudden change to an upright posture, combined with inability to mount an adequate increase in heart rate and/or peripheral vascular resistance. Orthostasis can be associated with medications, aging, volume depletion, and autonomic dysfunction.
![]() Cardiac-related syncope is due to dysrhythmia or structural heart disease and is a harbinger of sudden death. Syncope from dysrhythmia is typically sudden, usually without prodromal symptoms. Structural heart disease is usually unmasked as syncope during exertion or vasodilation. In the elderly this is most commonly due to aortic stenosis. In the young it is most commonly hypertrophic cardiomy-opathy (Table 23-1).
Cardiac-related syncope is due to dysrhythmia or structural heart disease and is a harbinger of sudden death. Syncope from dysrhythmia is typically sudden, usually without prodromal symptoms. Structural heart disease is usually unmasked as syncope during exertion or vasodilation. In the elderly this is most commonly due to aortic stenosis. In the young it is most commonly hypertrophic cardiomy-opathy (Table 23-1).
![]() Ten percent of patients with pulmonary embolism will present with syncope.
Ten percent of patients with pulmonary embolism will present with syncope.
![]() Hyperventilation, classically used as a provocative maneuver in diagnosing panic disorders, can lead to hypocarbia, cerebral vasoconstriction, and subsequent syncope.
Hyperventilation, classically used as a provocative maneuver in diagnosing panic disorders, can lead to hypocarbia, cerebral vasoconstriction, and subsequent syncope.
![]() Patients with syncope associated with a concurrent psychiatric disorder are likely to be young, with repeated episodes of syncope, multiple prodromal symptoms, and a generally positive review of systems.
Patients with syncope associated with a concurrent psychiatric disorder are likely to be young, with repeated episodes of syncope, multiple prodromal symptoms, and a generally positive review of systems.
![]() Multiple medications, such as antidepressants and antihypertensives (eg, β-blockers, calcium channel antagonists, diuretics), are frequent causes of syncope, especially in the elderly.
Multiple medications, such as antidepressants and antihypertensives (eg, β-blockers, calcium channel antagonists, diuretics), are frequent causes of syncope, especially in the elderly.
DIAGNOSIS AND DIFFERENTIAL
![]() The most important tools in the work-up of syncope are the history, physical examination, and ECG.
The most important tools in the work-up of syncope are the history, physical examination, and ECG.
![]() The history is aimed at identifying any high-risk features, including age, history of structural heart disease, and prodromal events.
The history is aimed at identifying any high-risk features, including age, history of structural heart disease, and prodromal events.
![]() Syncope without warning suggests a dysrhythmia; exertional syncope suggests outflow obstruction.
Syncope without warning suggests a dysrhythmia; exertional syncope suggests outflow obstruction.
![]() The cardiac examination may uncover a murmur such as due to aortic stenosis or hypertrophic cardiomyopathy.
The cardiac examination may uncover a murmur such as due to aortic stenosis or hypertrophic cardiomyopathy.
![]() An ECG may identify evidence of previous unknown myocardial infarction, acute ischemia, dysrhythmia, heart block, prolonged QT, or evidence of Wolff-Parkinson-White (WPW) syndrome.
An ECG may identify evidence of previous unknown myocardial infarction, acute ischemia, dysrhythmia, heart block, prolonged QT, or evidence of Wolff-Parkinson-White (WPW) syndrome.
![]() Selective laboratory testing directed by the history may consist of a hematocrit, pregnancy test, or electrolytes and glucose.
Selective laboratory testing directed by the history may consist of a hematocrit, pregnancy test, or electrolytes and glucose.
![]() Seizure, the most common disorder mistaken for syncope, can often be distinguished by the identification of a postictal phase. A tongue laceration is strong evidence for seizure, but occurs in a minority of seizures.
Seizure, the most common disorder mistaken for syncope, can often be distinguished by the identification of a postictal phase. A tongue laceration is strong evidence for seizure, but occurs in a minority of seizures.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() The goal of ED evaluation is to identify those at risk for immediate decompensation and future risk of serious morbidity or sudden death.
The goal of ED evaluation is to identify those at risk for immediate decompensation and future risk of serious morbidity or sudden death.
![]() If the cause of syncope can be determined by the initial history, physical examination, and ECG, the disposition can be made accordingly.
If the cause of syncope can be determined by the initial history, physical examination, and ECG, the disposition can be made accordingly.
![]() The algorithm in Fig. 23-1 provides a framework for the assessment, management, and disposition of syncope patients.
The algorithm in Fig. 23-1 provides a framework for the assessment, management, and disposition of syncope patients.
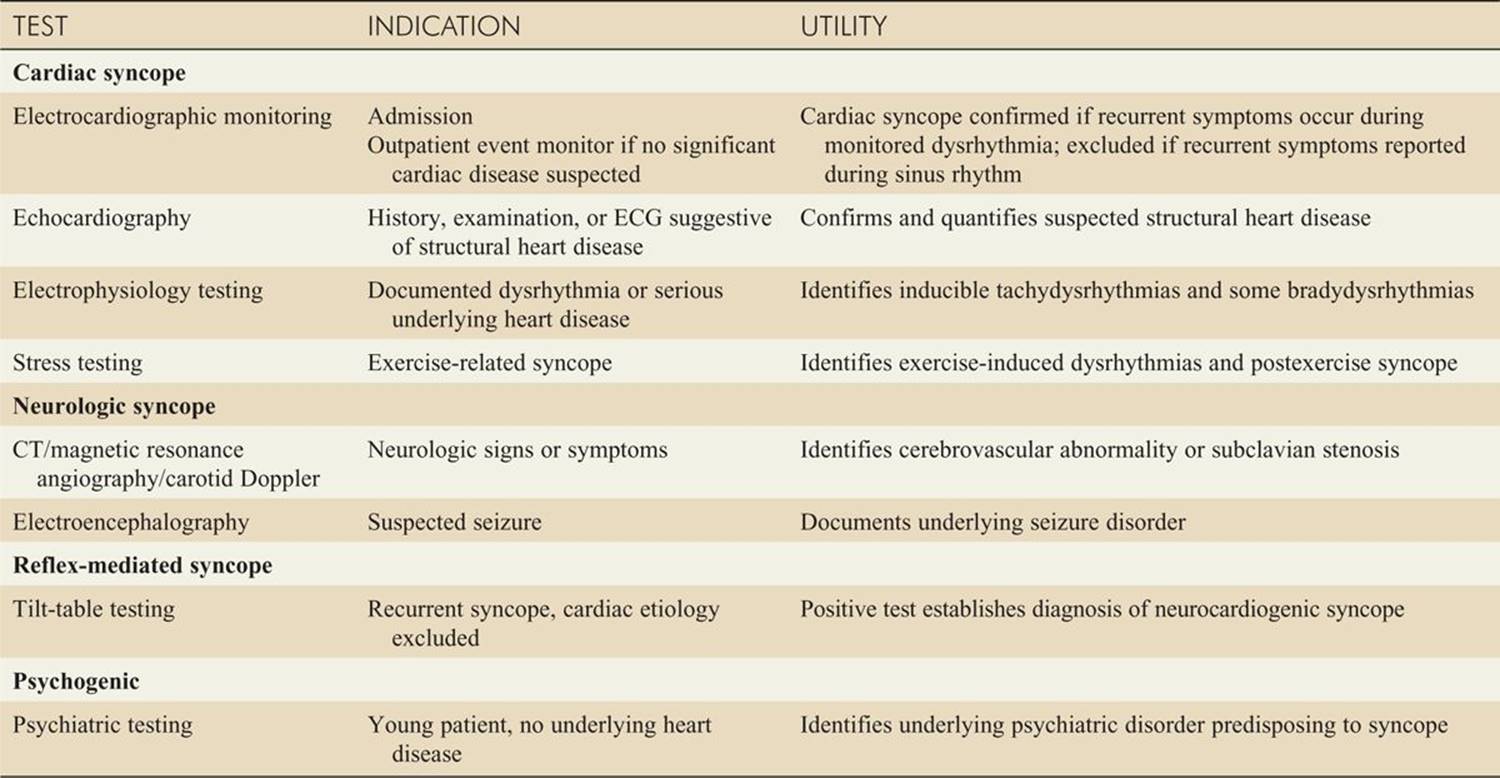
![]() Additional or post-ED testing, inpatient or outpatient, is defined by syncope’s cause or related symptoms (Table 23-2).
Additional or post-ED testing, inpatient or outpatient, is defined by syncope’s cause or related symptoms (Table 23-2).
![]() Patients who are not at high risk, are unlikely to have a cardiac etiology and therefore are appropriate for outpatient follow-up.
Patients who are not at high risk, are unlikely to have a cardiac etiology and therefore are appropriate for outpatient follow-up.
![]() Common outpatient evaluations may include 24-hour ambulatory or event monitoring and tilt testing.
Common outpatient evaluations may include 24-hour ambulatory or event monitoring and tilt testing.
![]() Discharge recommendations may include advising patients not to drive, work at heights, or place themselves in situations that would be dangerous in the event of another syncopal episode.
Discharge recommendations may include advising patients not to drive, work at heights, or place themselves in situations that would be dangerous in the event of another syncopal episode.
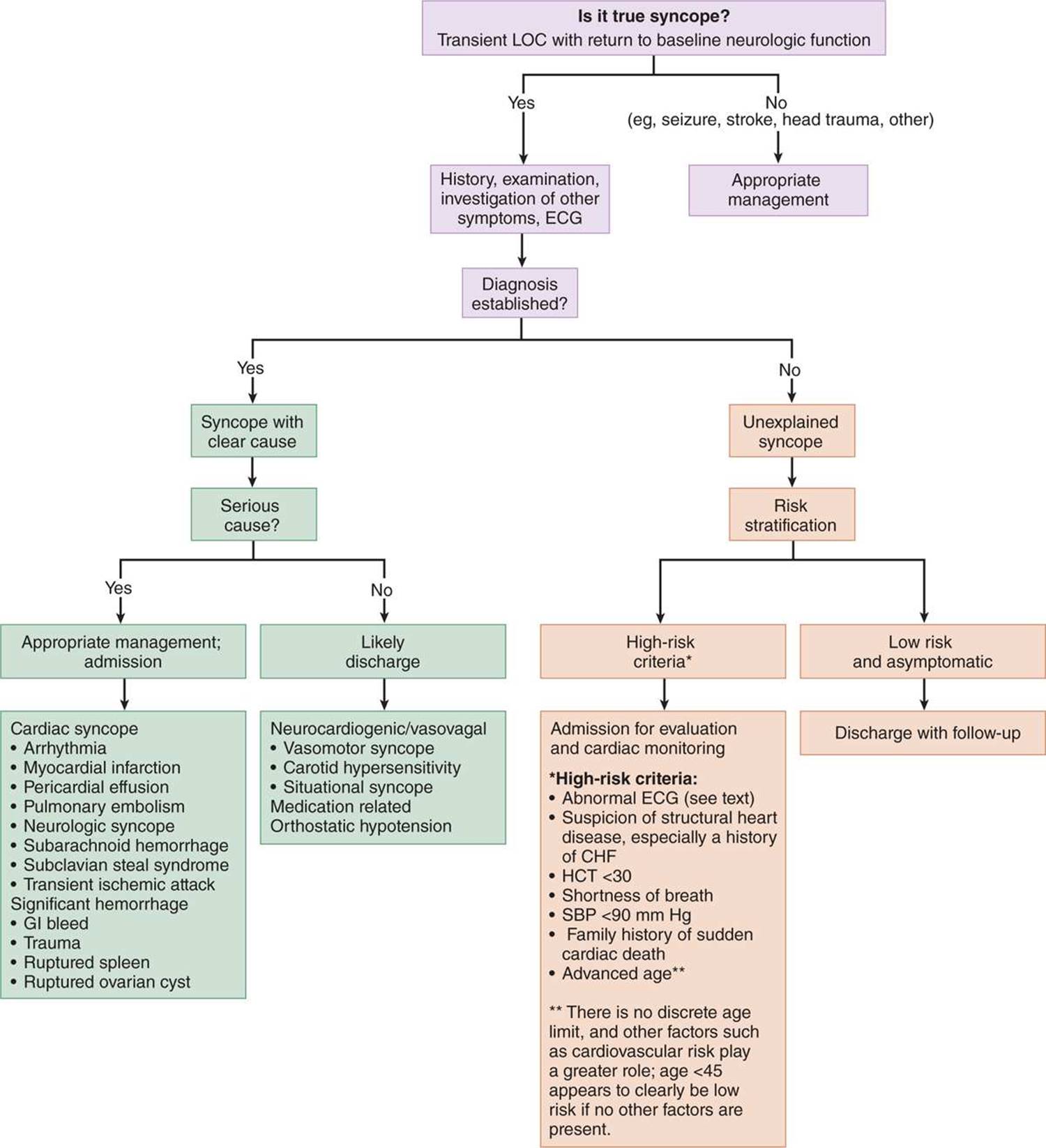
FIG. 23-1. ED evaluation of syncope provides a general management strategy. CHF = congestive heart failure; HCT = hematocrit; LOC = loss of consciousness; SBP = systolic blood pressure.
TABLE 23-2 Posted Testing for Syncope
Further Reading or further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th edition, see Chap. 56, “Syncope,” by James Quinn.