Amy J. Behrman
EPIDEMIOLOGY
![]() Tuberculosis (TB) remains a major global problem. More than 30% of the world’s population is infected with latent or active TB, which causes 2 million deaths yearly.
Tuberculosis (TB) remains a major global problem. More than 30% of the world’s population is infected with latent or active TB, which causes 2 million deaths yearly.
![]() The incidence of TB in the United States rose sharply between 1984 and 1992. The rise was driven by increases in rates of risk factors such as incarceration, human immunodeficiency virus (HIV) infection, drug-resistant TB, and immigration from areas with endemic TB. TB control programs targeting high-risk groups have reversed this trend progressively since 1993.
The incidence of TB in the United States rose sharply between 1984 and 1992. The rise was driven by increases in rates of risk factors such as incarceration, human immunodeficiency virus (HIV) infection, drug-resistant TB, and immigration from areas with endemic TB. TB control programs targeting high-risk groups have reversed this trend progressively since 1993.
![]() TB case rates remain highest among U.S. residents born in high-prevalence foreign countries, who also account for the majority of multidrug-resistant TB (MDR-TB) cases. Other populations with increased prevalence include immune-compromised patients (particularly those with HIV infection), the elderly, and nursing home residents, alcoholics and illicit drug users, and residents and staff of prisons and homeless shelters.
TB case rates remain highest among U.S. residents born in high-prevalence foreign countries, who also account for the majority of multidrug-resistant TB (MDR-TB) cases. Other populations with increased prevalence include immune-compromised patients (particularly those with HIV infection), the elderly, and nursing home residents, alcoholics and illicit drug users, and residents and staff of prisons and homeless shelters.
![]() Patients with unrecognized TB frequently present to EDs for evaluation and care, presenting challenges for diagnosis, treatment, and infection control.
Patients with unrecognized TB frequently present to EDs for evaluation and care, presenting challenges for diagnosis, treatment, and infection control.
PATHOPHYSIOLOGY
![]() Mycobacterium tuberculosis is a slow-growing obligate anaerobic rod with a complex multi-lipid cell wall (responsible for its characteristic acid-fast staining property).
Mycobacterium tuberculosis is a slow-growing obligate anaerobic rod with a complex multi-lipid cell wall (responsible for its characteristic acid-fast staining property).
![]() Transmission occurs through inhalation of droplet nuclei, although only 30% of patients become infected after exposure. Patients with stainable mycobacteria in saliva or sputum are the most infectious.
Transmission occurs through inhalation of droplet nuclei, although only 30% of patients become infected after exposure. Patients with stainable mycobacteria in saliva or sputum are the most infectious.
![]() The organism survives best in areas with high oxygen content and blood flow, including (in the lung) the apical and posterior segments of the upper lobe and the superior segment of the lower lobe. TB organisms also survive well in the renal cortex, the meninges, the epiphyses of long bones, and the vertebrae.
The organism survives best in areas with high oxygen content and blood flow, including (in the lung) the apical and posterior segments of the upper lobe and the superior segment of the lower lobe. TB organisms also survive well in the renal cortex, the meninges, the epiphyses of long bones, and the vertebrae.
![]() After inhalation of infectious particles, organisms that survive initial host defenses may cause granuloma formation in regional lymph nodes. The granulomas may progress to central caseating necrosis and calcification, identifiable on chest radiograph (CXR) as characteristic Ghon complexes.
After inhalation of infectious particles, organisms that survive initial host defenses may cause granuloma formation in regional lymph nodes. The granulomas may progress to central caseating necrosis and calcification, identifiable on chest radiograph (CXR) as characteristic Ghon complexes.
![]() If the granuloma does not contain the primary infection, TB can spread by hematogenous, lymphatic, or direct routes.
If the granuloma does not contain the primary infection, TB can spread by hematogenous, lymphatic, or direct routes.
![]() Progression of early active infection is most likely in immune-compromised patients.
Progression of early active infection is most likely in immune-compromised patients.
In immune-competent hosts, initial TB infection often becomes latent and asymptomatic.
![]() Latent TB infection (LTBI) is manifested by positive tuberculin skin tests (TSTs, also known as purified protein derivative [PPD] testing), or interferon gamma release assays (IGRAs), in the absence of active radiologic or clinical disease.
Latent TB infection (LTBI) is manifested by positive tuberculin skin tests (TSTs, also known as purified protein derivative [PPD] testing), or interferon gamma release assays (IGRAs), in the absence of active radiologic or clinical disease.
![]() Untreated LTBI will progress to active disease in 5% of cases within 2 years of primary infection; an additional 5% will reactivate over their host-patient lifetimes. Reactivation rates are higher in the young, the elderly, persons with recent primary infection, those with immune deficiency (particularly HIV), and those with chronic diseases such as diabetes, silicosis, and renal failure.
Untreated LTBI will progress to active disease in 5% of cases within 2 years of primary infection; an additional 5% will reactivate over their host-patient lifetimes. Reactivation rates are higher in the young, the elderly, persons with recent primary infection, those with immune deficiency (particularly HIV), and those with chronic diseases such as diabetes, silicosis, and renal failure.
CLINICAL FEATURES
![]() Primary TB infection is usually asymptomatic, presenting most frequently with only a new positive TST. Presenting symptoms of active primary TB infection often include fever, malaise, weight loss, and chest pain.
Primary TB infection is usually asymptomatic, presenting most frequently with only a new positive TST. Presenting symptoms of active primary TB infection often include fever, malaise, weight loss, and chest pain.
![]() Most active TB cases manifest as reactivation of LTBI. Patients usually present subacutely with systemic or pulmonary symptoms of fever, night sweats, malaise, weight loss, and fatigue. As lung infection progresses, patients may develop productive cough, hemoptysis, dyspnea, and/or chest pain.
Most active TB cases manifest as reactivation of LTBI. Patients usually present subacutely with systemic or pulmonary symptoms of fever, night sweats, malaise, weight loss, and fatigue. As lung infection progresses, patients may develop productive cough, hemoptysis, dyspnea, and/or chest pain.
![]() Rales and rhonchi may be found, but the pulmonary examination is usually nondiagnostic.
Rales and rhonchi may be found, but the pulmonary examination is usually nondiagnostic.
![]() Extrapulmonary TB develops in up to 20% of cases, most often presenting as painless lymphadenitis, with possible draining sinuses.
Extrapulmonary TB develops in up to 20% of cases, most often presenting as painless lymphadenitis, with possible draining sinuses.
![]() Pleural effusion may occur when a peripheral paren-chymal focus or local lymph node ruptures.
Pleural effusion may occur when a peripheral paren-chymal focus or local lymph node ruptures.
![]() TB peritonitis and pericarditis often require biopsy to diagnose as the exudates are often stain-negative.
TB peritonitis and pericarditis often require biopsy to diagnose as the exudates are often stain-negative.
![]() CNS infection may lead to TB meningitis, generally presenting with fever, headache, meningeal signs, mental status changes, and/or cranial nerve deficits. Presentation is usually acute in children and subacute in adults.
CNS infection may lead to TB meningitis, generally presenting with fever, headache, meningeal signs, mental status changes, and/or cranial nerve deficits. Presentation is usually acute in children and subacute in adults.
![]() Miliary TB is a multisystem disease caused by massive hematogenous dissemination during primary infection or secondary seeding in immune-compromised and pediatric patients. Miliary TB from primary infection often presents as acute severe illness, which may include shock, adult respiratory distress syndrome (ARDS), and multiorgan failure. Reactivation miliary TB may present with chronic and nonspecific constitutional symptoms and signs of multisystem illness such as fever, cough, sweats, weight loss, adenopathy, hepatosplenomegaly, and cytopenias.
Miliary TB is a multisystem disease caused by massive hematogenous dissemination during primary infection or secondary seeding in immune-compromised and pediatric patients. Miliary TB from primary infection often presents as acute severe illness, which may include shock, adult respiratory distress syndrome (ARDS), and multiorgan failure. Reactivation miliary TB may present with chronic and nonspecific constitutional symptoms and signs of multisystem illness such as fever, cough, sweats, weight loss, adenopathy, hepatosplenomegaly, and cytopenias.
![]() Extrapulmonary TB may also involve bone, joints, skin, kidneys, adrenals, and eyes.
Extrapulmonary TB may also involve bone, joints, skin, kidneys, adrenals, and eyes.
![]() Immunocompromised patients (HIV patients in particular) are extremely susceptible to TB and far more likely to develop active infections with atypical presentations. Disseminated extrapulmonary TB is also more common in HIV patients and should be considered in the evaluation of nonpulmonary complaints. Patients with suspected TB should be offered HIV testing.
Immunocompromised patients (HIV patients in particular) are extremely susceptible to TB and far more likely to develop active infections with atypical presentations. Disseminated extrapulmonary TB is also more common in HIV patients and should be considered in the evaluation of nonpulmonary complaints. Patients with suspected TB should be offered HIV testing.
![]() Prior partially treated TB is a risk factor for drug-resistant TB. It should be considered when TB is diagnosed, especially among those with suboptimal prior care (eg, immigrants from endemic areas, prisoners, homeless persons, drug users).
Prior partially treated TB is a risk factor for drug-resistant TB. It should be considered when TB is diagnosed, especially among those with suboptimal prior care (eg, immigrants from endemic areas, prisoners, homeless persons, drug users).
![]() As compared to the general population, HIV patients more commonly have MDR-TB, and the disease is more likely fatal in this group.
As compared to the general population, HIV patients more commonly have MDR-TB, and the disease is more likely fatal in this group.
DIAGNOSIS AND DIFFERENTIAL
![]() TB infection is difficult to diagnose because of its variable presentations. Early consideration of TB in any patient with respiratory or systemic complaints facilitates early diagnosis, appropriate disposition, and protection of staff.
TB infection is difficult to diagnose because of its variable presentations. Early consideration of TB in any patient with respiratory or systemic complaints facilitates early diagnosis, appropriate disposition, and protection of staff.
![]() CXRs remain the most useful diagnostic tool for active TB in the ED. Although atypical (or even normal) CXRs are common in immune-compromised hosts, the clinician should be familiar with common findings. Active primary TB usually presents with parenchymal infiltrates in any lung area. Hilar and/or mediastinal adenopathy may occur with or without infiltrates. Lesions may calcify.
CXRs remain the most useful diagnostic tool for active TB in the ED. Although atypical (or even normal) CXRs are common in immune-compromised hosts, the clinician should be familiar with common findings. Active primary TB usually presents with parenchymal infiltrates in any lung area. Hilar and/or mediastinal adenopathy may occur with or without infiltrates. Lesions may calcify.
![]() Reactivation TB typically presents with lesions in the upper lobes or superior segments of the lower lobes. Cavitation, calcification, scarring, atelectasis, and effusions may be seen (Fig. 33-1). Cavitation is associated with increased infectivity.
Reactivation TB typically presents with lesions in the upper lobes or superior segments of the lower lobes. Cavitation, calcification, scarring, atelectasis, and effusions may be seen (Fig. 33-1). Cavitation is associated with increased infectivity.
![]() Miliary TB may cause diffuse small (1- to 3-mm) nodular infiltrates.
Miliary TB may cause diffuse small (1- to 3-mm) nodular infiltrates.
![]() Acid-fast staining of sputum can detect mycobacteria in 60% of patients with pulmonary TB, although the yield is lower in HIV patients. Atypical mycobacteria can cause false-positive stains. Many patients will have false-negatives on a single sputum sample. Microscopy of non-sputum samples (eg, pleural fluid, cerebrospinal fluid [CSF]) is even less sensitive.
Acid-fast staining of sputum can detect mycobacteria in 60% of patients with pulmonary TB, although the yield is lower in HIV patients. Atypical mycobacteria can cause false-positive stains. Many patients will have false-negatives on a single sputum sample. Microscopy of non-sputum samples (eg, pleural fluid, cerebrospinal fluid [CSF]) is even less sensitive.
![]() Definitive cultures generally take weeks, but new genetic tests employing DNA probes or polymerase chain reaction technology can confirm the diagnosis sooner.
Definitive cultures generally take weeks, but new genetic tests employing DNA probes or polymerase chain reaction technology can confirm the diagnosis sooner.
![]() TST using the Mantoux method (intradermal tuberculin skin testing with PPD) identifies most patients with latent, prior, or active TB infection. Results are read 48 to 72 hours after placement, limiting the usefulness of this test for ED patients. Persons with positive PPDs and no active TB disease should be evaluated for prophylactic treatment with isoniazid (INH) to prevent reactivation TB (see Fig. 33-2).
TST using the Mantoux method (intradermal tuberculin skin testing with PPD) identifies most patients with latent, prior, or active TB infection. Results are read 48 to 72 hours after placement, limiting the usefulness of this test for ED patients. Persons with positive PPDs and no active TB disease should be evaluated for prophylactic treatment with isoniazid (INH) to prevent reactivation TB (see Fig. 33-2).
![]() Patients with HIV or other immunosuppressive conditions and patients with disseminated TB may have false-negative skin tests even if these individuals are not fully anergic.
Patients with HIV or other immunosuppressive conditions and patients with disseminated TB may have false-negative skin tests even if these individuals are not fully anergic.
![]() IGRAs may be helpful in diagnosing latent, and potentially active, TB infection, but results are also unlikely to be available in time for ED management needs.
IGRAs may be helpful in diagnosing latent, and potentially active, TB infection, but results are also unlikely to be available in time for ED management needs.

FIG. 33-1. Cavitary tuberculosis of the right upper lobe.

FIG. 33-2. Reactivation tuberculosis. Multiple fine nodular densities are seen throughout the central and peripheral lungs bilaterally, overlying residual scaring from prior active infection.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() To prevent drug resistance, TB infection is treated with combination antimicrobials. Initial therapy should include at least four drugs until susceptibility profiles are available for the patient.
To prevent drug resistance, TB infection is treated with combination antimicrobials. Initial therapy should include at least four drugs until susceptibility profiles are available for the patient.
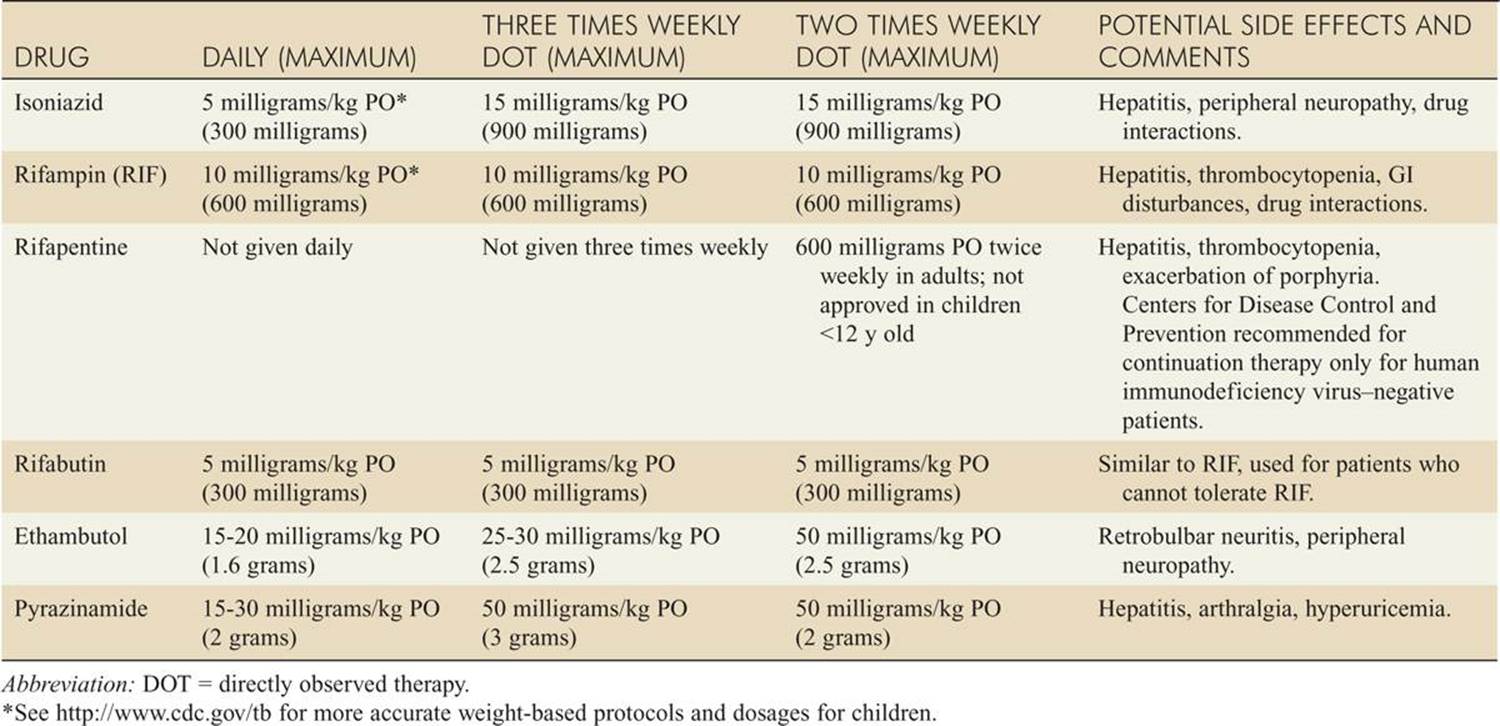
![]() Initial therapy usually includes INH, rifampin, pyrazi-namide, and ethambutol for 2 to 8 weeks; this should be followed by administration of at least two drugs (usually INH and rifampin) for at least 18 weeks (see Table 33-1).
Initial therapy usually includes INH, rifampin, pyrazi-namide, and ethambutol for 2 to 8 weeks; this should be followed by administration of at least two drugs (usually INH and rifampin) for at least 18 weeks (see Table 33-1).
![]() Patients with immune compromise, extrapulmonary TB, or MDR-TB may require more drugs or longer treatment periods.
Patients with immune compromise, extrapulmonary TB, or MDR-TB may require more drugs or longer treatment periods.
![]() Table 33-1 summarizes usual initial daily drug doses and side effects.
Table 33-1 summarizes usual initial daily drug doses and side effects.
![]() Most TB infection is treated in an outpatient setting. Ambulatory treatment for TB should not be initiated in the ED unless coordinated with or directed by the providers who will manage ongoing care.
Most TB infection is treated in an outpatient setting. Ambulatory treatment for TB should not be initiated in the ED unless coordinated with or directed by the providers who will manage ongoing care.
![]() Patients with active TB who are discharged from the ED must have documented immediate referral to a public health department or qualified physician for long-term treatment and monitoring of drug toxicity. Patients should be educated about home isolation, follow-up, and screening of household contacts.
Patients with active TB who are discharged from the ED must have documented immediate referral to a public health department or qualified physician for long-term treatment and monitoring of drug toxicity. Patients should be educated about home isolation, follow-up, and screening of household contacts.
![]() Directly observed treatment (DOT) improves treatment outcomes for patients at high risk for noncom-pliance and the development of MDR-TB.
Directly observed treatment (DOT) improves treatment outcomes for patients at high risk for noncom-pliance and the development of MDR-TB.
![]() Admission is indicated for clinical instability, diagnostic uncertainty, unreliable outpatient follow-up or compliance, and active known MDR-TB. Physicians should know local laws regarding involuntary hospi-talization and treatment.
Admission is indicated for clinical instability, diagnostic uncertainty, unreliable outpatient follow-up or compliance, and active known MDR-TB. Physicians should know local laws regarding involuntary hospi-talization and treatment.
![]() Admission to airborne isolation is mandatory for all cases of suspected TB to protect staff and other patients.
Admission to airborne isolation is mandatory for all cases of suspected TB to protect staff and other patients.
![]() Prehospital and ED staff should be trained to identify patients at risk for active TB as early as possible in their presentation. Patients with suspected TB should be masked or placed in respiratory isolation. TB should be considered in all immune-compromised or high-risk patients with respiratory symptoms.
Prehospital and ED staff should be trained to identify patients at risk for active TB as early as possible in their presentation. Patients with suspected TB should be masked or placed in respiratory isolation. TB should be considered in all immune-compromised or high-risk patients with respiratory symptoms.
![]() Staff caring directly for patients with suspected TB should wear National Institute of Occupational Safety and Health (NIOSH)-approved respiratory protection such as N95 or powered air-purifying respirators.
Staff caring directly for patients with suspected TB should wear National Institute of Occupational Safety and Health (NIOSH)-approved respiratory protection such as N95 or powered air-purifying respirators.
![]() ED staff should receive regular TST or IGRA testing to detect new primary infections, rule out active disease, and guide decisions for INH prophylaxis.
ED staff should receive regular TST or IGRA testing to detect new primary infections, rule out active disease, and guide decisions for INH prophylaxis.
TABLE 33-1 Dosages and Common Side Effects of Some Drugs Used in Tuberculosis (Adults)*
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide 7th ed, see Chapter 70, “Tuberculosis” by Vu D. Phan and Janet M. Poponick.