Joshua Gentges
EPIDEMIOLOGY
![]() Asthma is a common, chronic respiratory complaint. Increased incidence is associated with a Western lifestyle, increased environmental pollutants, and exposure to allergens.
Asthma is a common, chronic respiratory complaint. Increased incidence is associated with a Western lifestyle, increased environmental pollutants, and exposure to allergens.
![]() Chronic obstructive pulmonary disease (COPD) is a worldwide respiratory health problem. It is the only major cause of death that is increasing.
Chronic obstructive pulmonary disease (COPD) is a worldwide respiratory health problem. It is the only major cause of death that is increasing.
![]() COPD is more common and more severe in the elderly. The incidence of and mortality from COPD is rising in women. Worldwide, COPD prevalence is rising and is closely associated with cigarette use.
COPD is more common and more severe in the elderly. The incidence of and mortality from COPD is rising in women. Worldwide, COPD prevalence is rising and is closely associated with cigarette use.
PATHOPHYSIOLOGY
![]() The pathophysiologic hallmark of asthma is the reduction in airway diameter caused by smooth muscle contraction, vascular congestion, bronchial wall edema, and thick secretions. The inflammatory reaction that triggers the decrease in airway diameter results in increasing work of breathing and has a significant effect on pulmonary function.
The pathophysiologic hallmark of asthma is the reduction in airway diameter caused by smooth muscle contraction, vascular congestion, bronchial wall edema, and thick secretions. The inflammatory reaction that triggers the decrease in airway diameter results in increasing work of breathing and has a significant effect on pulmonary function.
![]() Acute airway inflammation is triggered when antigens come into contact with mast cells, resulting in the release of inflammatory mediators and bronchoc-onstriction, vascular congestion, edema formation, increased mucus production, and impaired mucociliary transport.
Acute airway inflammation is triggered when antigens come into contact with mast cells, resulting in the release of inflammatory mediators and bronchoc-onstriction, vascular congestion, edema formation, increased mucus production, and impaired mucociliary transport.
![]() Antigens or precipitants of an acute attack include viral respiratory tract infections, environmental pollutants, medications, occupational exposures to industrial chemicals, exercise, and emotional stress.
Antigens or precipitants of an acute attack include viral respiratory tract infections, environmental pollutants, medications, occupational exposures to industrial chemicals, exercise, and emotional stress.
![]() COPD is characterized by airflow obstruction, especially in expiratory airflow secondary to airway secretions, mucosal edema, bronchospasm, and bron-choconstriction due to impaired lung elasticity.
COPD is characterized by airflow obstruction, especially in expiratory airflow secondary to airway secretions, mucosal edema, bronchospasm, and bron-choconstriction due to impaired lung elasticity.
![]() Physiologic consequences of airflow obstruction are demonstrated in increased airway resistance, decreased maximum expiratory flow rates, air trapping, increased airway pressures (with resultant barotrauma and adverse hemodynamic effects), ventilation-perfusion imbalance (causing hypoxemia/hypercarbia), and increased work of breathing causing respiratory muscle fatigue with ventilatory failure.
Physiologic consequences of airflow obstruction are demonstrated in increased airway resistance, decreased maximum expiratory flow rates, air trapping, increased airway pressures (with resultant barotrauma and adverse hemodynamic effects), ventilation-perfusion imbalance (causing hypoxemia/hypercarbia), and increased work of breathing causing respiratory muscle fatigue with ventilatory failure.
![]() The major risk factor for developing COPD is tobacco smoke. Other risk factors associated with COPD include respiratory infections, occupational exposures, and chemical exposures. The only genetic risk factor is (α1-antitrypsin deficiency.
The major risk factor for developing COPD is tobacco smoke. Other risk factors associated with COPD include respiratory infections, occupational exposures, and chemical exposures. The only genetic risk factor is (α1-antitrypsin deficiency.
CLINICAL FEATURES
![]() Classically, asthma and COPD exacerbations present with dyspnea, chest tightness, wheezing, and cough.
Classically, asthma and COPD exacerbations present with dyspnea, chest tightness, wheezing, and cough.
![]() Physical examination findings of a mild asthma attack include wheezing and a prolonged expiratory phase. Wheezing does not correlate with the degree of airflow obstruction, as a quiet chest may indicate severe airflow obstruction.
Physical examination findings of a mild asthma attack include wheezing and a prolonged expiratory phase. Wheezing does not correlate with the degree of airflow obstruction, as a quiet chest may indicate severe airflow obstruction.
![]() A patient with a severe asthma exacerbation may present in a tripod position gasping for air with audible wheezing, diaphoresis, and accessory muscle use. Other signs of severe exacerbation include tachycardia, tachypnea, hypertension, and hypoxia. Paradoxical respirations, altered mental status, lethargy, and a quiet chest are all indicative of severe airflow obstruction and impending respiratory failure.
A patient with a severe asthma exacerbation may present in a tripod position gasping for air with audible wheezing, diaphoresis, and accessory muscle use. Other signs of severe exacerbation include tachycardia, tachypnea, hypertension, and hypoxia. Paradoxical respirations, altered mental status, lethargy, and a quiet chest are all indicative of severe airflow obstruction and impending respiratory failure.
![]() The two dominant clinical forms of COPD are pulmonary emphysema and chronic bronchitis. Emphysema is characterized by abnormal permanent enlargement and destruction of the air spaces distal to terminal bronchioles. By contrast, excess mucus secretion in the bronchial tree with a chronic productive cough occurring on most days for at least 3 months, in the year for two consecutive years, is characteristic of chronic bronchitis. Elements of both clinical forms are often present, although one may predominate.
The two dominant clinical forms of COPD are pulmonary emphysema and chronic bronchitis. Emphysema is characterized by abnormal permanent enlargement and destruction of the air spaces distal to terminal bronchioles. By contrast, excess mucus secretion in the bronchial tree with a chronic productive cough occurring on most days for at least 3 months, in the year for two consecutive years, is characteristic of chronic bronchitis. Elements of both clinical forms are often present, although one may predominate.
![]() Signs of hypercapnia include confusion, tremor, plethora, stupor, hypopnea, and apnea.
Signs of hypercapnia include confusion, tremor, plethora, stupor, hypopnea, and apnea.
![]() Risk factors for death from asthma include past history of intubation, multiple hospitalizations or recent emergency room visits, heavy use of inhaled β2-agonists, illicit drug use, and chronic psychiatric disease.
Risk factors for death from asthma include past history of intubation, multiple hospitalizations or recent emergency room visits, heavy use of inhaled β2-agonists, illicit drug use, and chronic psychiatric disease.
![]() Respiratory failure from COPD is associated with severe dyspnea refractory to initial treatment, worsening hypoxemia or hypercapnia, or respiratory acidosis.
Respiratory failure from COPD is associated with severe dyspnea refractory to initial treatment, worsening hypoxemia or hypercapnia, or respiratory acidosis.
DIAGNOSIS AND DIFFERENTIAL
![]() Diagnosis of asthma or COPD is based on the history and physical examination. Investigate possible causes of decompensation.
Diagnosis of asthma or COPD is based on the history and physical examination. Investigate possible causes of decompensation.
![]() Spirometry is commonly used to determine the severity of airflow obstruction and the effectiveness of therapy by measuring the peak expiratory flow rate (PEFR). Sequential measurements of PEFR assess the response of treatment and can be used to predict need for hospitalization. PEFR less than 40% of predicted is associated with severe airway obstruction.
Spirometry is commonly used to determine the severity of airflow obstruction and the effectiveness of therapy by measuring the peak expiratory flow rate (PEFR). Sequential measurements of PEFR assess the response of treatment and can be used to predict need for hospitalization. PEFR less than 40% of predicted is associated with severe airway obstruction.
![]() Pulse oximetry is a noninvasive means for assessing and monitoring oxygen saturation during treatment. It does not provide information about acid-base disturbances and hypercapnia.
Pulse oximetry is a noninvasive means for assessing and monitoring oxygen saturation during treatment. It does not provide information about acid-base disturbances and hypercapnia.
![]() Arterial blood gases (ABGs) may be used in asthma and COPD to assess for hypercapnia and respiratory acidosis. These are ominous findings and indicate extreme airway obstruction and fatigue with possible onset of acute respiratory failure.
Arterial blood gases (ABGs) may be used in asthma and COPD to assess for hypercapnia and respiratory acidosis. These are ominous findings and indicate extreme airway obstruction and fatigue with possible onset of acute respiratory failure.
![]() A chest radiograph should be obtained if there is clinical suspicion of pneumothorax, pneumomediasti-num, pneumonia, or other medical concerns such as congestive heart failure (CHF), pleural effusions, or pulmonary neoplasia (see Fig. 36-1).
A chest radiograph should be obtained if there is clinical suspicion of pneumothorax, pneumomediasti-num, pneumonia, or other medical concerns such as congestive heart failure (CHF), pleural effusions, or pulmonary neoplasia (see Fig. 36-1).
![]() Electrocardiograms (ECGs) are helpful in asthma and COPD to assess for cardiac ischemia, myocar-dial infarction, and arrhythmias such as multifocal atrial tachycardia. ECG findings in moderate to severe pulmonary disease may reveal right ventricular strain, abnormal P waves, or nonspecific ST-T wave abnormalities, which may resolve with treatment (see Fig. 36-2).
Electrocardiograms (ECGs) are helpful in asthma and COPD to assess for cardiac ischemia, myocar-dial infarction, and arrhythmias such as multifocal atrial tachycardia. ECG findings in moderate to severe pulmonary disease may reveal right ventricular strain, abnormal P waves, or nonspecific ST-T wave abnormalities, which may resolve with treatment (see Fig. 36-2).
![]() The differential diagnosis of decompensated asthma and COPD includes CHF, upper airway obstruction, aspiration, pulmonary neoplasia, pleural effusions, interstitial lung diseases, pneumonia, pulmonary embolism, and exposure to asphyxiants. COPD is a major risk factor for pneumothorax. CHF, pneumonia, and acute coronary syndrome commonly coexist with decompensated COPD.
The differential diagnosis of decompensated asthma and COPD includes CHF, upper airway obstruction, aspiration, pulmonary neoplasia, pleural effusions, interstitial lung diseases, pneumonia, pulmonary embolism, and exposure to asphyxiants. COPD is a major risk factor for pneumothorax. CHF, pneumonia, and acute coronary syndrome commonly coexist with decompensated COPD.
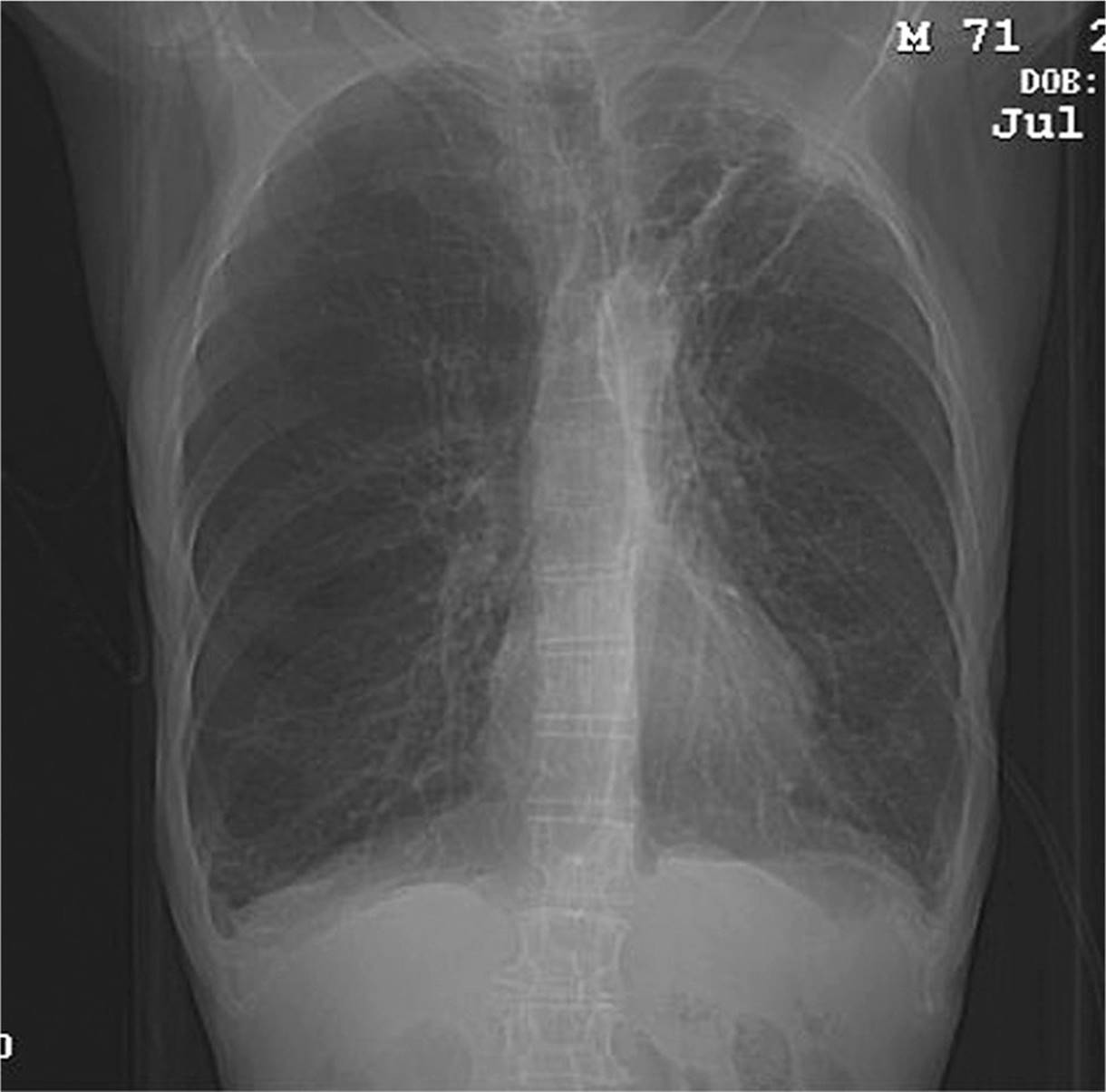
FIG. 36-1. Posterior-anterior chest radiograph in a patient with chronic obstructive pulmonary disease.
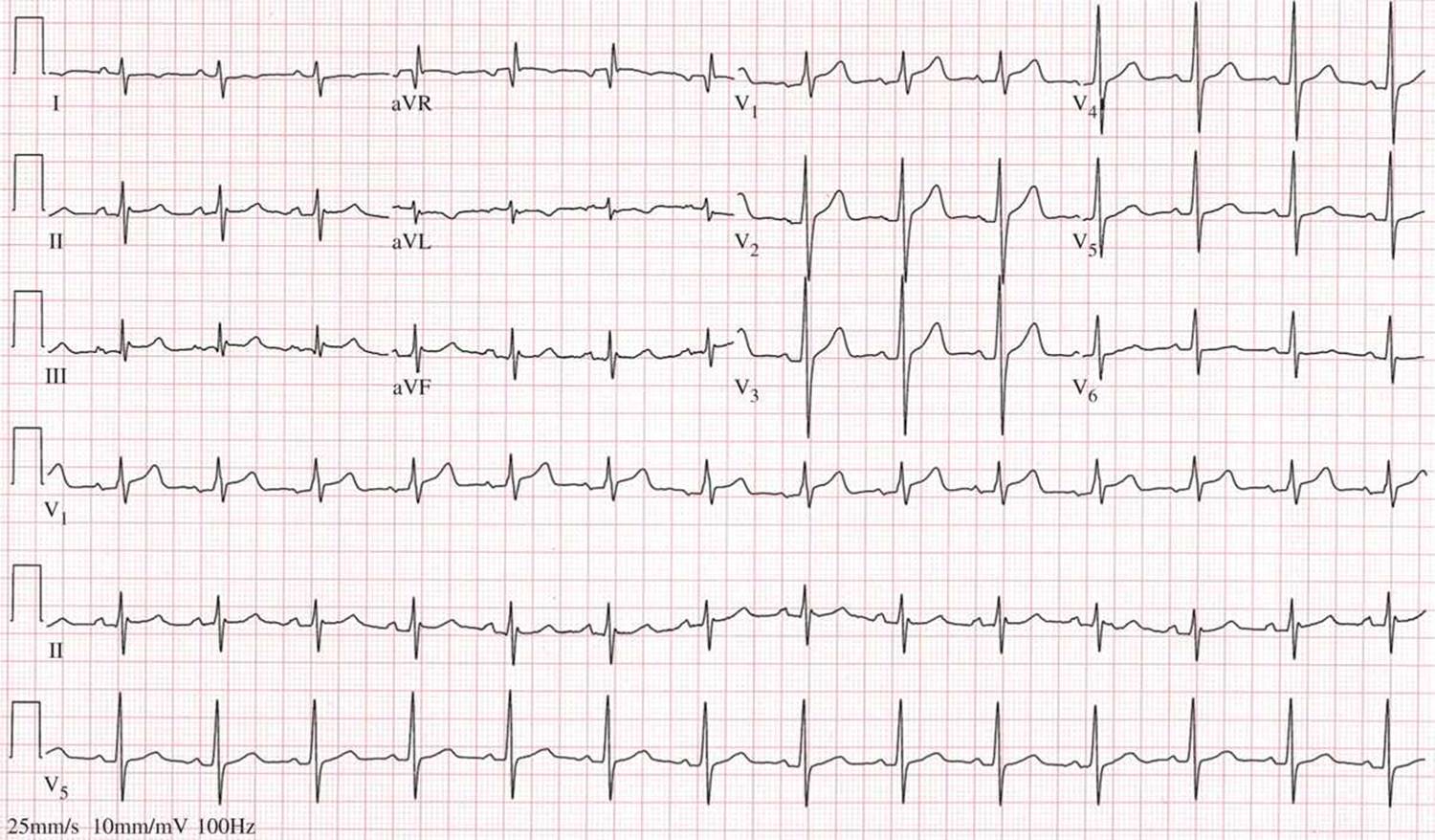
FIG. 36-2. ECG findings of right ventricular hypertrophy in a patient with chronic obstructive pulmonary disease: rightward axis, R wave taller than the S wave in lead V1, and a persistent S wave into the lateral precordial leads. Findings of right ventricular hypertrophy, not demonstrated here, are an incomplete right bundle branch block pattern, and a strain pattern (asymmetric ST-segment depression and T-wave inversion) in right ventricular leads.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() All patients should be placed on a cardiac monitor, pulse oximeter, and noninvasive blood pressure monitor, and patients with moderate to severe attacks should have IV access.
All patients should be placed on a cardiac monitor, pulse oximeter, and noninvasive blood pressure monitor, and patients with moderate to severe attacks should have IV access.
![]() Empiric supplemental oxygen should be administered to correct Sao2 above 90%. Oxygen may exacerbate hypercapnia in the setting of COPD. Perform an ABG measurement if there is concern for symptomatic hypercapnia.
Empiric supplemental oxygen should be administered to correct Sao2 above 90%. Oxygen may exacerbate hypercapnia in the setting of COPD. Perform an ABG measurement if there is concern for symptomatic hypercapnia.
![]() β-Adrenergic agonists are first-line agents used to treat acute bronchospasm in COPD and asthma. Aerosolized forms minimize systemic toxicity and are preferred. Albuterol sulfate 2.5 to 5 milligrams is the most common agent. Deliver doses every 20 minutes or as continuous nebulization (10–15 milligrams/h), continuing treatment based on clinical response and signs of toxicity (tachycardia, hypertension, and palpitations). Levalbuterol can be given at one-half of the dose of albuterol, but has not been studied by continuous nebulization. Terbutaline sulfate (0.25–25.0 mL) or epinephrine 1:1000 (0.1–1.0 mL) SC may be administered to patients not tolerating aerosolized therapy. Epinephrine should be avoided in the first trimester of pregnancy and in patients with underlying cardiovascular disease.
β-Adrenergic agonists are first-line agents used to treat acute bronchospasm in COPD and asthma. Aerosolized forms minimize systemic toxicity and are preferred. Albuterol sulfate 2.5 to 5 milligrams is the most common agent. Deliver doses every 20 minutes or as continuous nebulization (10–15 milligrams/h), continuing treatment based on clinical response and signs of toxicity (tachycardia, hypertension, and palpitations). Levalbuterol can be given at one-half of the dose of albuterol, but has not been studied by continuous nebulization. Terbutaline sulfate (0.25–25.0 mL) or epinephrine 1:1000 (0.1–1.0 mL) SC may be administered to patients not tolerating aerosolized therapy. Epinephrine should be avoided in the first trimester of pregnancy and in patients with underlying cardiovascular disease.
![]() Anticholinergics are useful adjuvants when given with other therapies. Nebulized ipratropium (500 milligrams = 2.5 mL) may be administered alone or mixed with albuterol. The effects of ipratropium peak in 1 to 2 hours and last 3 to 4 hours. Dosages may be repeated every 1 to 4 hours.
Anticholinergics are useful adjuvants when given with other therapies. Nebulized ipratropium (500 milligrams = 2.5 mL) may be administered alone or mixed with albuterol. The effects of ipratropium peak in 1 to 2 hours and last 3 to 4 hours. Dosages may be repeated every 1 to 4 hours.
![]() Steroids should be given immediately to patients with exacerbations of asthma and COPD. The initial dose is the equivalent of 40 to 60 milligrams of oral pred-nisone. If the patient is unable to take oral medication, intravenous methylprednisolone 60 to 125 milligrams may be used. Additional doses may be given every 4 to 6 hours. Inhaled steroids are not indicated for the treatment of acute symptoms. A 5- to 10-day course of oral steroids (prednisone 40–60 milligrams/d) is beneficial for discharged patients with a significant exacerbation of asthma or COPD.
Steroids should be given immediately to patients with exacerbations of asthma and COPD. The initial dose is the equivalent of 40 to 60 milligrams of oral pred-nisone. If the patient is unable to take oral medication, intravenous methylprednisolone 60 to 125 milligrams may be used. Additional doses may be given every 4 to 6 hours. Inhaled steroids are not indicated for the treatment of acute symptoms. A 5- to 10-day course of oral steroids (prednisone 40–60 milligrams/d) is beneficial for discharged patients with a significant exacerbation of asthma or COPD.
![]() COPD exacerbations with change in sputum color or volume should be administered antibiotic therapy directed at respiratory pathogens. No specific agents are shown to be superior. Reserve antibiotic use in asthma for concurrent bacterial infections.
COPD exacerbations with change in sputum color or volume should be administered antibiotic therapy directed at respiratory pathogens. No specific agents are shown to be superior. Reserve antibiotic use in asthma for concurrent bacterial infections.
![]() Magnesium sulfate (1–2 grams IV) may be used in severe asthma attack due to its bronchodilatory properties.
Magnesium sulfate (1–2 grams IV) may be used in severe asthma attack due to its bronchodilatory properties.
![]() Heliox (80% helium and 20% oxygen) can be used in severe asthma exacerbations to lower airway resistance in patients with no supplemental oxygen requirement.
Heliox (80% helium and 20% oxygen) can be used in severe asthma exacerbations to lower airway resistance in patients with no supplemental oxygen requirement.
![]() Patients with respiratory muscle fatigue, respiratory acidosis, altered mental status, or hypoxia refractory to standard therapies need mechanical ventilation. Noninvasive partial pressure ventilation (NPPV) is a useful alternative to intubation and invasive ventilation. It lowers intubation rates, short-term mortality, and length of hospitalization in COPD. NPPV can be given by continuous positive airway pressure (CPAP) or bi-level positive airway pressure (BiPAP). BiPAP has the advantage of reducing the work of breathing. CPAP is titrated up to 15 cm H2O, while BiPAP settings are between 8 and 20 cm H2O for inspiration and 4 and 15 cm H2O for expiration. Evidence for NPPV in severe asthma is promising but less compelling than that for COPD. NPPV should not be used for patients with a suspected pneumothorax.
Patients with respiratory muscle fatigue, respiratory acidosis, altered mental status, or hypoxia refractory to standard therapies need mechanical ventilation. Noninvasive partial pressure ventilation (NPPV) is a useful alternative to intubation and invasive ventilation. It lowers intubation rates, short-term mortality, and length of hospitalization in COPD. NPPV can be given by continuous positive airway pressure (CPAP) or bi-level positive airway pressure (BiPAP). BiPAP has the advantage of reducing the work of breathing. CPAP is titrated up to 15 cm H2O, while BiPAP settings are between 8 and 20 cm H2O for inspiration and 4 and 15 cm H2O for expiration. Evidence for NPPV in severe asthma is promising but less compelling than that for COPD. NPPV should not be used for patients with a suspected pneumothorax.
![]() Patients that are uncooperative or obtunded, cannot clear airway secretions, are hemodynamically unstable, in respiratory arrest, have had recent facial or gastroesophageal surgery, facial burns, extreme obesity, or poor NPPV mask fit are not candidates for NPPV and require invasive ventilation. Oral intubation is the preferred method. Using rapid inspira-tory flow rates at a reduced respiratory frequency (12–14 breaths/min) and allowing for an adequate expiratory phase may help reduce air trapping and subsequent barotrauma. Therapy should be guided by pulse oximetry and ABG results. Sedation and continued therapy for bronchospasm should continue after the patient has been placed on artificial ventilation.
Patients that are uncooperative or obtunded, cannot clear airway secretions, are hemodynamically unstable, in respiratory arrest, have had recent facial or gastroesophageal surgery, facial burns, extreme obesity, or poor NPPV mask fit are not candidates for NPPV and require invasive ventilation. Oral intubation is the preferred method. Using rapid inspira-tory flow rates at a reduced respiratory frequency (12–14 breaths/min) and allowing for an adequate expiratory phase may help reduce air trapping and subsequent barotrauma. Therapy should be guided by pulse oximetry and ABG results. Sedation and continued therapy for bronchospasm should continue after the patient has been placed on artificial ventilation.
![]() In patients being discharged, continued treatment with β2-agonists and oral steroids is important. In addition, patient education and close medical follow-up is essential.
In patients being discharged, continued treatment with β2-agonists and oral steroids is important. In addition, patient education and close medical follow-up is essential.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 72, “Acute Asthma in Adults,” by Rita K. Cydulka, and Chapter 73, “Chronic Obstructive Pulmonary Disease,” by Craig G. Bates and Rita K. Cydulka.