Chad E. Branecki
HEMORRHOIDS
EPIDEMIOLOGY
![]() Hemorrhoids are associated with constipation, straining at stool, frequent diarrhea, advanced age, and pregnancy. Chronic liver disease, portal hypertension, obesity, and tumors or the rectum and colon may contribute to the formation of hemorrhoids.
Hemorrhoids are associated with constipation, straining at stool, frequent diarrhea, advanced age, and pregnancy. Chronic liver disease, portal hypertension, obesity, and tumors or the rectum and colon may contribute to the formation of hemorrhoids.
PATHOPHYSIOLOGY
![]() Internal hemorrhoid veins are proximal to the dentate line, and drain into the portal venous system.
Internal hemorrhoid veins are proximal to the dentate line, and drain into the portal venous system.
![]() External hemorrhoid veins are distal to the dentate line, therefore have sensory innervation, and can be viewed on external inspection (Fig. 49-1).
External hemorrhoid veins are distal to the dentate line, therefore have sensory innervation, and can be viewed on external inspection (Fig. 49-1).

FIG. 49-1. Coronal section of the anorectum.
CLINICAL FEATURES
![]() Internal hemorrhoids are best visualized through an anoscope and frequently located at the 2-, 5-, and 9-o’clock positions in a prone patient.
Internal hemorrhoids are best visualized through an anoscope and frequently located at the 2-, 5-, and 9-o’clock positions in a prone patient.
![]() External hemorrhoids cause severe pain, discomfort, and bleeding at the time of defecation.
External hemorrhoids cause severe pain, discomfort, and bleeding at the time of defecation.
![]() Thrombosis of external hemorrhoids may appear as a bluish-purple mass protruding from the rectum and is exquisitely tender to palpation.
Thrombosis of external hemorrhoids may appear as a bluish-purple mass protruding from the rectum and is exquisitely tender to palpation.
![]() Prolapse can occur with large hemorrhoids, requiring manual reduction by the patient or clinician. The hemorrhoid may become incarcerated causing mucous drainage, pruritus ani, heavy bleeding, urinary retention, gangrene, or even sepsis. Surgical intervention may be required.
Prolapse can occur with large hemorrhoids, requiring manual reduction by the patient or clinician. The hemorrhoid may become incarcerated causing mucous drainage, pruritus ani, heavy bleeding, urinary retention, gangrene, or even sepsis. Surgical intervention may be required.
DIAGNOSIS AND DIFFERENTIAL
![]() Other causes of rectal pain and bleeding may include malignancy, abscess, cryptitis, anal fissure, trauma, foreign bodies, rectal prolapse, or venereal proctitis.
Other causes of rectal pain and bleeding may include malignancy, abscess, cryptitis, anal fissure, trauma, foreign bodies, rectal prolapse, or venereal proctitis.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treatment is usually nonsurgical. Most hemorrhoids can be relieved by hot sitz baths, topical steroids, analgesics, and bulk laxatives (psyllium seed compounds, stool softeners) after the acute phase has subsided.
Treatment is usually nonsurgical. Most hemorrhoids can be relieved by hot sitz baths, topical steroids, analgesics, and bulk laxatives (psyllium seed compounds, stool softeners) after the acute phase has subsided.
![]() Acute (<48 hours), non-tolerable painful thrombosed external hemorrhoids can be managed by clot excision. The thrombosed vein should be unroofed by an elliptical incision that allows evacuation of the clot (Fig. 49-2).
Acute (<48 hours), non-tolerable painful thrombosed external hemorrhoids can be managed by clot excision. The thrombosed vein should be unroofed by an elliptical incision that allows evacuation of the clot (Fig. 49-2).
![]() Surgical referral and intervention is indicated for continued bleeding, intractable pain, or incarceration and strangulation.
Surgical referral and intervention is indicated for continued bleeding, intractable pain, or incarceration and strangulation.
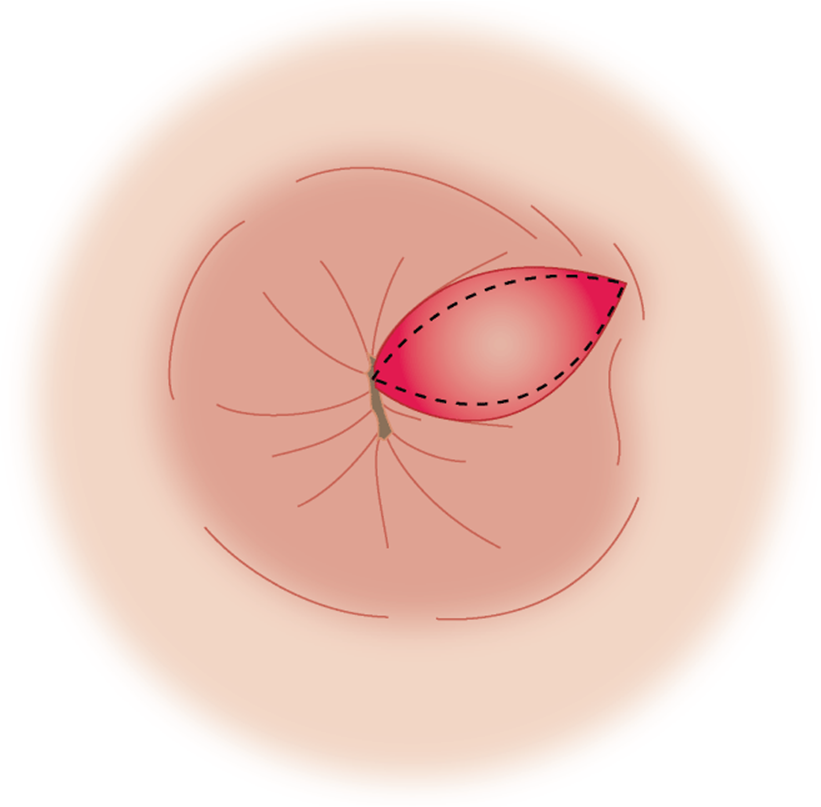
FIG. 49-2. Elliptical incision of thrombosed external hemorrhoid.
CRYPTITIS
EPIDEMIOLOGY
![]() Cryptitis is associated with repetitive sphincter trauma from spasm, recurrent diarrhea, or passage of large, hard stools.
Cryptitis is associated with repetitive sphincter trauma from spasm, recurrent diarrhea, or passage of large, hard stools.
PATHOPHYSIOLOGY
![]() Anal crypts are superficial mucosal pockets that lie between the columns of Morgagni. This tissue becomes hypertrophicd from the repeated puckering action of the sphincter muscles, resulting in local inflammation or infection (cryptitis).
Anal crypts are superficial mucosal pockets that lie between the columns of Morgagni. This tissue becomes hypertrophicd from the repeated puckering action of the sphincter muscles, resulting in local inflammation or infection (cryptitis).
CLINICAL FEATURES
![]() Anal pain, spasm, and itching with or without bleeding are the cardinal signs and symptoms.
Anal pain, spasm, and itching with or without bleeding are the cardinal signs and symptoms.
![]() The Crypts that are most commonly involved are located in the posterior midline portion of the anal ring. The crypts involved may be tender, swollen, and nodular in appearance.
The Crypts that are most commonly involved are located in the posterior midline portion of the anal ring. The crypts involved may be tender, swollen, and nodular in appearance.
DIAGNOSIS AND DIFFERENTIAL
![]() Definitive diagnosis of cryptitis, inflammation, erythema, and pus is made by palpation and visualization by anoscopy.
Definitive diagnosis of cryptitis, inflammation, erythema, and pus is made by palpation and visualization by anoscopy.
![]() Cryptitis may coexist and lead to the development of fissures, fistulae, and abscesses.
Cryptitis may coexist and lead to the development of fissures, fistulae, and abscesses.
EMERGENCY DEPARTMENT CARE AND DISPOSITON
![]() Bulk laxatives, a high-fiber diet, and sitz baths will enhance passage of stool and healing by keeping the anus clean and crypts empty.
Bulk laxatives, a high-fiber diet, and sitz baths will enhance passage of stool and healing by keeping the anus clean and crypts empty.
![]() Refractory cases or deep large crypts may require surgical intervention.
Refractory cases or deep large crypts may require surgical intervention.
ANAL FISSURES
EPIDEMIOLOGY
![]() Anal fissures are the most common cause of painful rectal bleeding.
Anal fissures are the most common cause of painful rectal bleeding.
![]() Anal fissures are common among infants, children, young adults, and postpartum women.
Anal fissures are common among infants, children, young adults, and postpartum women.
PATHOPHYSIOLOGY
![]() Traditional midline anal fissures are caused by the passage of hard, large fecal masses, but can be seen after acute episodes of diarrhea. Anal fissures are a linear tear from the dentate line through the andodermal tissue of the anal canal.
Traditional midline anal fissures are caused by the passage of hard, large fecal masses, but can be seen after acute episodes of diarrhea. Anal fissures are a linear tear from the dentate line through the andodermal tissue of the anal canal.
![]() As the fissure becomes more chronic, it will appear pale and edematous, and often have a sentinel pile.
As the fissure becomes more chronic, it will appear pale and edematous, and often have a sentinel pile.
CLINICAL FEATURES
![]() In 90% of cases, anal fissures occur in the midline posteriorly.
In 90% of cases, anal fissures occur in the midline posteriorly.
![]() Associated with severe, cutting pain during and immediately following defecation, which subsides between bowel movements.
Associated with severe, cutting pain during and immediately following defecation, which subsides between bowel movements.
![]() Digital rectal examination and anoscopy may be limited due to pain with examination.
Digital rectal examination and anoscopy may be limited due to pain with examination.
DIAGNOSIS AND DIFFERENTIAL
![]() A nonhealing fissure or non-midline location should arouse the suspicion for other more serious causes, such as Crohn’s disease, ulcerative colitis, carcinomas, or child abuse.
A nonhealing fissure or non-midline location should arouse the suspicion for other more serious causes, such as Crohn’s disease, ulcerative colitis, carcinomas, or child abuse.
![]() Abscess and stricture formation are complications of prolonged severe anal fissures.
Abscess and stricture formation are complications of prolonged severe anal fissures.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Hot sitz baths, a high-fiber diet, and local analgesic and/or hydrocortisone ointments will provide symptomatic relief. Most uncomplicated fissures will heal in a few weeks.
Hot sitz baths, a high-fiber diet, and local analgesic and/or hydrocortisone ointments will provide symptomatic relief. Most uncomplicated fissures will heal in a few weeks.
FISTULA IN ANO
EPIDEMIOLOGY
![]() A fistula in ano most commonly results as a complication of perianal or ischiorectal abscesses.
A fistula in ano most commonly results as a complication of perianal or ischiorectal abscesses.
![]() Fistulas can also be associated with ulcerative colitis, Crohn’s disease, malignancies, STDs, trauma, or TB.
Fistulas can also be associated with ulcerative colitis, Crohn’s disease, malignancies, STDs, trauma, or TB.
PATHOPHYSIOLOGY
![]() An anal fistula is an abnormal inflammatory tract, connecting the anal canal with external skin.
An anal fistula is an abnormal inflammatory tract, connecting the anal canal with external skin.
![]() Anterior opening fistulas tend to follow a simple direct course to the anal canal (Goodsall rule), whereas posterior opening fistulas tend to follow a more curving path to the posterior midline.
Anterior opening fistulas tend to follow a simple direct course to the anal canal (Goodsall rule), whereas posterior opening fistulas tend to follow a more curving path to the posterior midline.
CLINICAL FEATURES
![]() Malodorous, blood-stained discharge will be present as long as the tract remains open.
Malodorous, blood-stained discharge will be present as long as the tract remains open.
![]() Throbbing constant pain worsened by sitting, moving, and stooling will be present when the tract is blocked and abscess formation occurs.
Throbbing constant pain worsened by sitting, moving, and stooling will be present when the tract is blocked and abscess formation occurs.
DIAGNOSIS AND DIFFERENTIAL
![]() Abscess may be the initial presenting symptom.
Abscess may be the initial presenting symptom.
![]() Ultrasound using 7-MHz endoprobe with hydrogen peroxide may aid in the diagnosis.
Ultrasound using 7-MHz endoprobe with hydrogen peroxide may aid in the diagnosis.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Non-ill-appearing patients can be treated with analgesia, antipyretics, and oral antibiotics (ciprofloxin 750 milligrams BID and metronidazole 500 milligrams QID for 7 days).
Non-ill-appearing patients can be treated with analgesia, antipyretics, and oral antibiotics (ciprofloxin 750 milligrams BID and metronidazole 500 milligrams QID for 7 days).
![]() Surgical excision is the definitive treatment.
Surgical excision is the definitive treatment.
ANORECTAL ABCESSES
EPIDEMIOLOGY
![]() Abscesses originate from infected anal crypts and spread to the perianal and deep rectal spaces.
Abscesses originate from infected anal crypts and spread to the perianal and deep rectal spaces.
![]() Perianal abscess is the most common type and is located close to the anal verge.
Perianal abscess is the most common type and is located close to the anal verge.
![]() Anorectal abscesses are most common among middle-aged men.
Anorectal abscesses are most common among middle-aged men.
PATHOPHYSIOLOGY
![]() The mechanism involves the obstruction of an anal gland, resulting in a polymicrobial abscess formation.
The mechanism involves the obstruction of an anal gland, resulting in a polymicrobial abscess formation.
![]() Infection can progress to any potential spaces that are normally filled with fatty areolar tissue.
Infection can progress to any potential spaces that are normally filled with fatty areolar tissue.
![]() Other diseases that are associated with rectal abscess should be investigated, including Crohn’s disease, ulcerative colitis, carcinomas, TB, venereal disease, and trauma.
Other diseases that are associated with rectal abscess should be investigated, including Crohn’s disease, ulcerative colitis, carcinomas, TB, venereal disease, and trauma.
CLINICAL FEATURES
![]() Persistent dull, aching, throbbing pain that increases prior to defecation is typical.
Persistent dull, aching, throbbing pain that increases prior to defecation is typical.
![]() As the abscess progresses, pain may interfere with walking or sitting.
As the abscess progresses, pain may interfere with walking or sitting.
![]() Fever, leukocytosis, and a painful tender mass on digital rectal examination may be observed.
Fever, leukocytosis, and a painful tender mass on digital rectal examination may be observed.
DIAGNOSIS AND DIFFERENTIAL
![]() Deep space abscesses can be difficult to detect on physical examination alone.
Deep space abscesses can be difficult to detect on physical examination alone.
![]() Endorectal ultrasonography, CT, MRI, or needle localization may be needed to confirm the diagnosis of deep space abscess.
Endorectal ultrasonography, CT, MRI, or needle localization may be needed to confirm the diagnosis of deep space abscess.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Simple perianal abscess without systemic illness is the only abscess that should be drained in the ED. Other deep space abscess should be drained in the operating room.
Simple perianal abscess without systemic illness is the only abscess that should be drained in the ED. Other deep space abscess should be drained in the operating room.
![]() After adequate local anesthesia, a cruciate incision is made over the abscess and the “dog ears” are excised. Packing is usually not necessary.
After adequate local anesthesia, a cruciate incision is made over the abscess and the “dog ears” are excised. Packing is usually not necessary.
![]() Antibiotics usually are not necessary unless systemic infection or toxicity is present.
Antibiotics usually are not necessary unless systemic infection or toxicity is present.
![]() The patient should have follow-up care in 24 hours, and surgical referral.
The patient should have follow-up care in 24 hours, and surgical referral.
PROCTITIS
EPIDEMIOLOGY/PATHOPHYSIOLOGY
![]() Proctitis is inflammation of the rectal mucosa.
Proctitis is inflammation of the rectal mucosa.
![]() Common causes include prior radiation treatments, autoimmune disorders, vasculitis, ischemia, and infections.
Common causes include prior radiation treatments, autoimmune disorders, vasculitis, ischemia, and infections.
![]() STDs of the anorectum can be seen in individuals who engage in anal sex.
STDs of the anorectum can be seen in individuals who engage in anal sex.
CLINICAL FEATURES
![]() Symptoms include anorectal pain, itching, discharge, diarrhea, bleeding, and lower abdominal cramping.
Symptoms include anorectal pain, itching, discharge, diarrhea, bleeding, and lower abdominal cramping.
![]() Mucosal inflammation, erythema, ulcers, or discharge may be noted using anoscopy.
Mucosal inflammation, erythema, ulcers, or discharge may be noted using anoscopy.
DIAGNOSIS AND DIFFERENTIAL
![]() Condylomata acuminata, gonorrhea, syphilis, herpes, and AIDS-related infections should be investigated in patients presenting with proctitis.
Condylomata acuminata, gonorrhea, syphilis, herpes, and AIDS-related infections should be investigated in patients presenting with proctitis.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Obtain cultures if infectious etiology is suspected.
Obtain cultures if infectious etiology is suspected.
![]() Sitz bath, stool softeners, good anal hygiene, and analgesics will provide some relief.
Sitz bath, stool softeners, good anal hygiene, and analgesics will provide some relief.
![]() Empiric therapy aimed at eradicating infection should be started while cultures are pending.
Empiric therapy aimed at eradicating infection should be started while cultures are pending.
![]() Referral for appropriate follow-up and further evaluation should be recommended.
Referral for appropriate follow-up and further evaluation should be recommended.
RECTAL PROLAPSE
EPIDEMIOLOGY
![]() Prolapse of the rectal mucosa only is most commonly seen in children under the age of 2 years. Mucosal prolapse can also occur in adults with third- and fourth-degree hemorrhoids.
Prolapse of the rectal mucosa only is most commonly seen in children under the age of 2 years. Mucosal prolapse can also occur in adults with third- and fourth-degree hemorrhoids.
![]() Complete rectal prolapse occurs with extremes of age, most commonly in elderly women.
Complete rectal prolapse occurs with extremes of age, most commonly in elderly women.
PATHOPHYSIOLOGY
![]() There are three classes of rectal prolapse based on anatomic differences: (1) prolapse of rectal mucosa only; (2) prolapse of all three layers of mucosa; (3) intussusception of the upper rectum through the lower rectum.
There are three classes of rectal prolapse based on anatomic differences: (1) prolapse of rectal mucosa only; (2) prolapse of all three layers of mucosa; (3) intussusception of the upper rectum through the lower rectum.
![]() Occurs due to both laxity in the pelvic floor and weakening of the sphincter muscles.
Occurs due to both laxity in the pelvic floor and weakening of the sphincter muscles.
CLINICAL FEATURES
![]() Most patients detect as mass, accompanied by bloody mucous discharge, and/or fecal incontinence.
Most patients detect as mass, accompanied by bloody mucous discharge, and/or fecal incontinence.
![]() Mucosal prolapse will only extrude few centimeters from the dentate line.
Mucosal prolapse will only extrude few centimeters from the dentate line.
![]() Complete rectal prolapse can extend up to 15 cm outside the anus, and appears as a red, ball-like mass.
Complete rectal prolapse can extend up to 15 cm outside the anus, and appears as a red, ball-like mass.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Manual reduction with gentle steady pressure should be attempted to prevent edema, strangulation, or ischemia.
Manual reduction with gentle steady pressure should be attempted to prevent edema, strangulation, or ischemia.
![]() Analgesia, sedation, and application of generous amounts of granulated sugar to the prolapsed segment may aid in reduction if tissue is edematous.
Analgesia, sedation, and application of generous amounts of granulated sugar to the prolapsed segment may aid in reduction if tissue is edematous.
![]() Surgical correction is often required; however, the patient can be discharged from the ED with stool softeners to prevent constipation.
Surgical correction is often required; however, the patient can be discharged from the ED with stool softeners to prevent constipation.
ANORECTAL TUMORS
EPIDEMIOLOGY
![]() Factors such as smoking, anal intercourse, HIV, and genital warts have been associated with anorectal cancers.
Factors such as smoking, anal intercourse, HIV, and genital warts have been associated with anorectal cancers.
![]() Anal canal neoplasms are more common, and have a poorer prognosis.
Anal canal neoplasms are more common, and have a poorer prognosis.
PATHOPHYSIOLOGY
![]() Classification depends on location in respect to dentate line. Anal canal neoplasms are proximal to the dentate line; whereas anal margin neoplasms are distal to the dentate line.
Classification depends on location in respect to dentate line. Anal canal neoplasms are proximal to the dentate line; whereas anal margin neoplasms are distal to the dentate line.
![]() Anal canal neoplasms include adenocarcinoma, melanoma, and Kaposi’s sarcoma.
Anal canal neoplasms include adenocarcinoma, melanoma, and Kaposi’s sarcoma.
CLINICAL FEATURES
![]() Patients present with nonspecific symptoms including sensation of a mass, pruritus, and bloody stools. As the neoplasm progresses, anorexia, bloating, weight loss, diarrhea, constipation, and narrowing of the stool caliber develop.
Patients present with nonspecific symptoms including sensation of a mass, pruritus, and bloody stools. As the neoplasm progresses, anorexia, bloating, weight loss, diarrhea, constipation, and narrowing of the stool caliber develop.
DIAGNOSIS AND DIFFERENTIAL
![]() All anorectal tumors can be detected by careful visual examination, anoscopy, or sigmoidoscopy.
All anorectal tumors can be detected by careful visual examination, anoscopy, or sigmoidoscopy.
![]() Tumors may be misdiagnosed as hemorrhoids.
Tumors may be misdiagnosed as hemorrhoids.
![]() Complications of anorectal tumors include rectal prolapse, prolonged blood loss, abscess, or fistula formation.
Complications of anorectal tumors include rectal prolapse, prolonged blood loss, abscess, or fistula formation.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Referral for proctoscopic or sigmoidoscopic examination with biopsy is mandatory.
Referral for proctoscopic or sigmoidoscopic examination with biopsy is mandatory.
RECTAL FOREIGN BODIES
EPIDEMIOLOGY
![]() Not all patients may be forthcoming with accurate history of rectal foreign-body insertion.
Not all patients may be forthcoming with accurate history of rectal foreign-body insertion.
PATHOPHYSIOLOGY
![]() Most foreign bodies are in the rectal ampulla.
Most foreign bodies are in the rectal ampulla.
![]() Peritoneal reflection determines where presence of free air on radiography will be found. Below the peritoneal reflection causes air along the psoas muscles, whereas above the peritoneal reflection causes air under the diaphragm.
Peritoneal reflection determines where presence of free air on radiography will be found. Below the peritoneal reflection causes air along the psoas muscles, whereas above the peritoneal reflection causes air under the diaphragm.
CLINICAL FEATURES
![]() Patient may complain of pain, cramping, bleeding, or discharge.
Patient may complain of pain, cramping, bleeding, or discharge.
![]() Perforation of the rectum may cause fever, leukocytosis, peritoneal signs, and bleeding.
Perforation of the rectum may cause fever, leukocytosis, peritoneal signs, and bleeding.
DIAGNOSIS AND DIFFERENTIAL
![]() Radiographs must be obtained to determine the position, shape, and number of foreign bodies and perforation.
Radiographs must be obtained to determine the position, shape, and number of foreign bodies and perforation.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Most of the foreign bodies in the distal rectum can be removed in the ED with adequate sedation.
Most of the foreign bodies in the distal rectum can be removed in the ED with adequate sedation.
![]() Objects that are made of glass, have sharp edges, or cannot be easily removed may require surgery or gas-troenterology consultation.
Objects that are made of glass, have sharp edges, or cannot be easily removed may require surgery or gas-troenterology consultation.
![]() Broad-spectrum antibiotics (piperacillin/tazobactam 3.375 grams every 6 hours) should be administered if perforation is suspected.
Broad-spectrum antibiotics (piperacillin/tazobactam 3.375 grams every 6 hours) should be administered if perforation is suspected.
PRURITUS ANI
EPIDEMIOLOGY
![]() Common causes include diet, infectious agents, and irritants.
Common causes include diet, infectious agents, and irritants.
![]() This disorder is most common in males during the fifth and sixth decades of life.
This disorder is most common in males during the fifth and sixth decades of life.
![]() Pinworms (Enterobius vermicularis) are the most common cause in children.
Pinworms (Enterobius vermicularis) are the most common cause in children.
CLINICAL FEATURES
![]() Rectal itching, with a reddened, excoriated, and moist perianal area.
Rectal itching, with a reddened, excoriated, and moist perianal area.
DIAGNOSIS AND DIFFERNTIAL
![]() Atopic dermatitis, lichen planus, psoriasis, and anal margin neoplasms need to be considered in the differential diagnosis of puritus ani.
Atopic dermatitis, lichen planus, psoriasis, and anal margin neoplasms need to be considered in the differential diagnosis of puritus ani.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Increased fiber, sitz bath, anti-histamines, zinc oxide, and 1% hydrocortisone creams can be used for acute symptoms and enhance healing.
Increased fiber, sitz bath, anti-histamines, zinc oxide, and 1% hydrocortisone creams can be used for acute symptoms and enhance healing.
![]() Consider referral to proctologist or dermatologist for refractory cases.
Consider referral to proctologist or dermatologist for refractory cases.
PILONIDAL SINUS
EPIDEMIOLOGY
![]() Most commonly affects males before the fourth decade of life.
Most commonly affects males before the fourth decade of life.
PATHOPHYSIOLOGY
![]() Pilonidal sinus is an acquired problem, formed by a recurring foreign-body granulomatous reaction to an ingrown hair.
Pilonidal sinus is an acquired problem, formed by a recurring foreign-body granulomatous reaction to an ingrown hair.
CLINICAL FEATURES
![]() A pilonidal cyst can present as a painless, cyst, an acute infected abscess, or chronic drainage in the midline part of the natal cleft, which overlies the lower sacrum and coccyx.
A pilonidal cyst can present as a painless, cyst, an acute infected abscess, or chronic drainage in the midline part of the natal cleft, which overlies the lower sacrum and coccyx.
![]() Ultrasound may be helpful in determining the extent of the abscess.
Ultrasound may be helpful in determining the extent of the abscess.
DIAGNOSIS AND DIFFERENTIAL
![]() Pilonidal disease is often mistakenly diagnosed as perirectal abscesses.
Pilonidal disease is often mistakenly diagnosed as perirectal abscesses.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Acute abscesses should be incised, drained, and packed in the ED.
Acute abscesses should be incised, drained, and packed in the ED.
![]() Antibiotics are not usually necessary unless the patient is immune compromised or surrounding cel-lulitis is present.
Antibiotics are not usually necessary unless the patient is immune compromised or surrounding cel-lulitis is present.
![]() Surgical referral is necessary to prevent recurrence.
Surgical referral is necessary to prevent recurrence.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 88, “Anorectal Disorders,” by Brian E. Burgess.