Geetika Gupta
![]() The acute phenomenon of renal stones migrating down the ureter is referred to as renal colic.
The acute phenomenon of renal stones migrating down the ureter is referred to as renal colic.
EPIDEMIOLOGY
![]() Urinary stones are three times more common in males and usually occur in the third to fifth decades.
Urinary stones are three times more common in males and usually occur in the third to fifth decades.
![]() Overall incidence is around 12%.
Overall incidence is around 12%.
![]() There is an increased incidence from genetic predisposition and hereditary diseases (eg, renal tubular acidosis, hyperparathyroidism, cystinuria).
There is an increased incidence from genetic predisposition and hereditary diseases (eg, renal tubular acidosis, hyperparathyroidism, cystinuria).
![]() Lifestyle factors augment stone growth. Increasing water intake results in a decreased incidence of calculi. Patients in mountainous, desert, or tropical regions, and those in sedentary jobs suffer a higher frequency of stone disease.
Lifestyle factors augment stone growth. Increasing water intake results in a decreased incidence of calculi. Patients in mountainous, desert, or tropical regions, and those in sedentary jobs suffer a higher frequency of stone disease.
![]() Medications such as protease inhibitors to treat HIV (indinavir sulfate), laxatives, and diuretics have also shown an increase in prevalence.
Medications such as protease inhibitors to treat HIV (indinavir sulfate), laxatives, and diuretics have also shown an increase in prevalence.
![]() Approximately one-third of the patients suffer recurrences within 1 year and 50% in 5 years.
Approximately one-third of the patients suffer recurrences within 1 year and 50% in 5 years.
![]() Children less than 16 years of age constitute approximately 7% of all cases of renal stones with a 1:1 sex distribution.
Children less than 16 years of age constitute approximately 7% of all cases of renal stones with a 1:1 sex distribution.
![]() Common etiologies in pediatrics are metabolic abnormality (50%), urologic anomalies (20%), infection (15%), and immobilization syndrome (5%).
Common etiologies in pediatrics are metabolic abnormality (50%), urologic anomalies (20%), infection (15%), and immobilization syndrome (5%).
PATHOPHYSIOLOGY
![]() The precise cause of urinary stone formation is unknown. What is known is that it requires three elements: supersaturation, lack of inhibitors, and stasis.
The precise cause of urinary stone formation is unknown. What is known is that it requires three elements: supersaturation, lack of inhibitors, and stasis.
![]() Approximately 75% of calculi are composed of calcium, occurring in conjunction with oxalate, phosphate, or a combination of both. Calcium excretion is elevated in conditions such as high dietary calcium intake, immobilization syndrome, or hyperparathyroidism. Oxalate excretion is enhanced in patients with inflammatory bowel disease and as a result of small bowel bypass surgery.
Approximately 75% of calculi are composed of calcium, occurring in conjunction with oxalate, phosphate, or a combination of both. Calcium excretion is elevated in conditions such as high dietary calcium intake, immobilization syndrome, or hyperparathyroidism. Oxalate excretion is enhanced in patients with inflammatory bowel disease and as a result of small bowel bypass surgery.
![]() Ten percent to 15% of stones are magnesium-ammonium-phosphate (struvite). These are associated with infection by urea-splitting bacteria and are the most common cause of staghorn calculi. Urea-splitting organisms include Proteus, Klebsiella, Staphylococcus species, Providencia, and Corynebacterium. Antibiotic penetration into these calculi is low and makes patients with stones prone to urosepsis, thus surgical removal of staghorn calculi is recommended.
Ten percent to 15% of stones are magnesium-ammonium-phosphate (struvite). These are associated with infection by urea-splitting bacteria and are the most common cause of staghorn calculi. Urea-splitting organisms include Proteus, Klebsiella, Staphylococcus species, Providencia, and Corynebacterium. Antibiotic penetration into these calculi is low and makes patients with stones prone to urosepsis, thus surgical removal of staghorn calculi is recommended.
![]() Uric acid causes 10% of uroliths, with cystine and other uncommon stones making up the remainder. Twenty-five percent of patients with gout will have a kidney stone.
Uric acid causes 10% of uroliths, with cystine and other uncommon stones making up the remainder. Twenty-five percent of patients with gout will have a kidney stone.
![]() The majority (90%) of urinary calculi are radiopaque. Calcium phosphate and calcium oxalate stones have a density similar to bone.
The majority (90%) of urinary calculi are radiopaque. Calcium phosphate and calcium oxalate stones have a density similar to bone.
![]() Common areas of impaction include the ureteropel-vic junctions (UPJs), pelvic brim, and ureterovesical junction (UVJ). The UVJ has the smallest diameter of the urinary tract and is the most common location for impacted stones.
Common areas of impaction include the ureteropel-vic junctions (UPJs), pelvic brim, and ureterovesical junction (UVJ). The UVJ has the smallest diameter of the urinary tract and is the most common location for impacted stones.
CLINICAL FEATURES
![]() Patients are usually asymptomatic until there is at least a partial obstruction.
Patients are usually asymptomatic until there is at least a partial obstruction.
![]() Patients complain of the acute onset of severe pain, which can be associated with diaphoresis, nausea, and emesis. During extreme presentations, the patient is anxious, pacing or writhing, and may be unable to hold still or converse.
Patients complain of the acute onset of severe pain, which can be associated with diaphoresis, nausea, and emesis. During extreme presentations, the patient is anxious, pacing or writhing, and may be unable to hold still or converse.
![]() Hematuria is present in 85% of patients.
Hematuria is present in 85% of patients.
![]() Typically pain originates in flank, radiating ipsilater-ally and anteroinferiorly around the abdomen and toward the ipsilateral groin. The radiating pattern is the result of autonomic nerve fibers serving both the kidney and respective gonad. Anterior abdominal pain may radiate back toward the flank and is associated with midureteral stones. Stones near the bladder may cause urinary frequency and urgency.
Typically pain originates in flank, radiating ipsilater-ally and anteroinferiorly around the abdomen and toward the ipsilateral groin. The radiating pattern is the result of autonomic nerve fibers serving both the kidney and respective gonad. Anterior abdominal pain may radiate back toward the flank and is associated with midureteral stones. Stones near the bladder may cause urinary frequency and urgency.
![]() Young pediatric patients present as nonspecific abdominal pain. Twenty percent to 30% of children diagnosed with ureteral stones may present with painless hematuria.
Young pediatric patients present as nonspecific abdominal pain. Twenty percent to 30% of children diagnosed with ureteral stones may present with painless hematuria.
![]() During acute obstruction the serum creatinine is unchanged due to the unaffected kidney functions up to 185% of its baseline capacity.
During acute obstruction the serum creatinine is unchanged due to the unaffected kidney functions up to 185% of its baseline capacity.
![]() Stone size determines the likelihood of spontaneous passage. Seventy-five percent of stones <5 mm will pass spontaneously within 4 weeks, 60% of stones 5 to 7 mm, and only 39% of stones >7 mm will pass spontaneously within 4 weeks.
Stone size determines the likelihood of spontaneous passage. Seventy-five percent of stones <5 mm will pass spontaneously within 4 weeks, 60% of stones 5 to 7 mm, and only 39% of stones >7 mm will pass spontaneously within 4 weeks.
![]() Irregularly shaped stones with spicules and sharp edges will have a lower passage rate. Rates of passage for stones found in the proximal, middle, and distal ureter are approximately 20%, 50%, and 70%, respectively, regardless of stone size.
Irregularly shaped stones with spicules and sharp edges will have a lower passage rate. Rates of passage for stones found in the proximal, middle, and distal ureter are approximately 20%, 50%, and 70%, respectively, regardless of stone size.
![]() Extracorporeal shock wave lithotripsy (ESWL) is used as an aid to fracture stones into small particles using focused sound waves. The resulting sludge is passed in the urine. When there are large fragments left, an acute episode of renal colic re-occurs. The presentation is identical to the de novo episodes of renal colic.
Extracorporeal shock wave lithotripsy (ESWL) is used as an aid to fracture stones into small particles using focused sound waves. The resulting sludge is passed in the urine. When there are large fragments left, an acute episode of renal colic re-occurs. The presentation is identical to the de novo episodes of renal colic.
![]() Stones with obstruction for >3 weeks will lead to irreversible renal parenchyma damage.
Stones with obstruction for >3 weeks will lead to irreversible renal parenchyma damage.
DIAGNOSIS AND DIFFERENTIAL
![]() All patients with suspected renal colic need a urinaly-sis to exclude infection. In 11% to 15% of the cases, there is no blood found in the urine. If there is evidence of pyuria, cultures and sensitivities are recommended due to the likelihood of needing prolonged antibiotic therapy. Blood urea nitrogen and creatinine levels should be considered as many patients with stones as they may have a reduced creatinine clearance. More importantly, 25% of patients with flank pain and hematuria do not have radiographic evidence of nephrolithiasis. As a consequence, other diagnoses must be considered.
All patients with suspected renal colic need a urinaly-sis to exclude infection. In 11% to 15% of the cases, there is no blood found in the urine. If there is evidence of pyuria, cultures and sensitivities are recommended due to the likelihood of needing prolonged antibiotic therapy. Blood urea nitrogen and creatinine levels should be considered as many patients with stones as they may have a reduced creatinine clearance. More importantly, 25% of patients with flank pain and hematuria do not have radiographic evidence of nephrolithiasis. As a consequence, other diagnoses must be considered.
![]() The differential diagnosis in these patients includes a symptomatic abdominal aortic aneurysm, aortic dissection, incarcerated hernia, epididymitis, testicular torsion, ectopic pregnancy, salpingitis, pyelonephritis, papillary necrosis (due to sickle cell disease, diabetes, nonsteroidal analgesic abuse, or infection), renal infarction, appendicitis, diverticulitis, mesenteric ischemia, herpes zoster, drug-seeking behavior, and musculoskeletal strain. A right ureteral stone can also resemble cholecystitis. This list is not exhaustive.
The differential diagnosis in these patients includes a symptomatic abdominal aortic aneurysm, aortic dissection, incarcerated hernia, epididymitis, testicular torsion, ectopic pregnancy, salpingitis, pyelonephritis, papillary necrosis (due to sickle cell disease, diabetes, nonsteroidal analgesic abuse, or infection), renal infarction, appendicitis, diverticulitis, mesenteric ischemia, herpes zoster, drug-seeking behavior, and musculoskeletal strain. A right ureteral stone can also resemble cholecystitis. This list is not exhaustive.
![]() All female patients of childbearing age should have a pregnancy test.
All female patients of childbearing age should have a pregnancy test.
![]() Intravenous pyelogram (IVP) yields information regarding renal function as well as anatomy. The first and most reliable indication of the presence of obstruction is a delay in the appearance of the nephrogram. Adjuncts to diagnosis include distension of the renal pelvis, calyceal distortion, dye extravasation, hydronephrosis, and visualization of the entire ureter.
Intravenous pyelogram (IVP) yields information regarding renal function as well as anatomy. The first and most reliable indication of the presence of obstruction is a delay in the appearance of the nephrogram. Adjuncts to diagnosis include distension of the renal pelvis, calyceal distortion, dye extravasation, hydronephrosis, and visualization of the entire ureter.
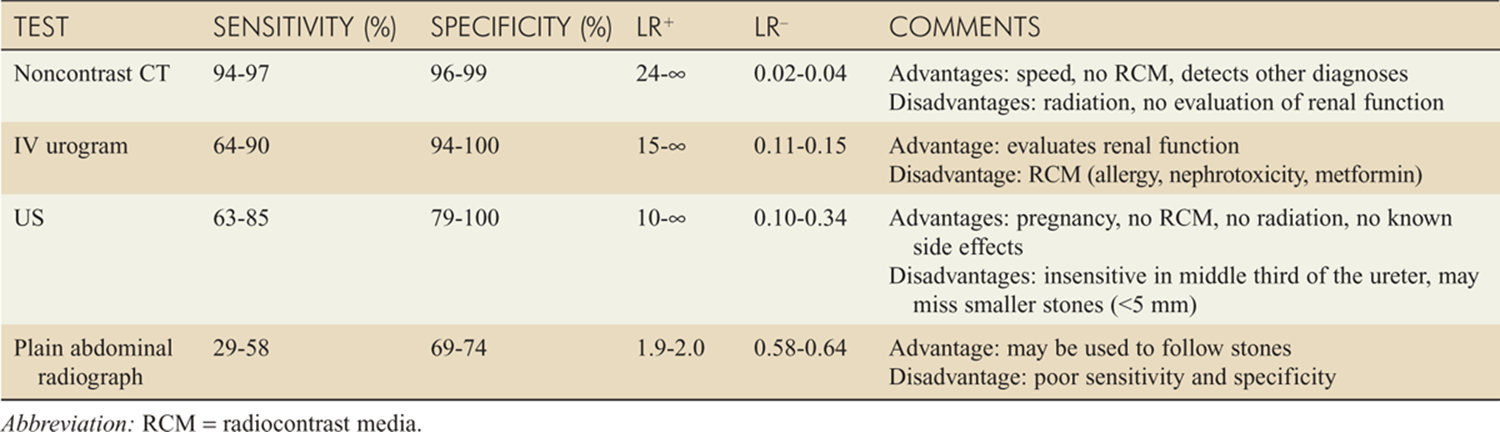
![]() The sensitivity of an IVP is 64% to 90% and the specificity is 94% to 100%. A falsely negative IVP infrequently occurs when there is a radiolucent, partially obstructing stone.
The sensitivity of an IVP is 64% to 90% and the specificity is 94% to 100%. A falsely negative IVP infrequently occurs when there is a radiolucent, partially obstructing stone.
![]() Advantages of the IVP are that it provides information on renal function and the degree of obstruction. The major disadvantages are time to perform the examination, contrast allergy, and the risk of nephrotoxicity.
Advantages of the IVP are that it provides information on renal function and the degree of obstruction. The major disadvantages are time to perform the examination, contrast allergy, and the risk of nephrotoxicity.
![]() Noncontrast helical computed tomography (CT) is the diagnostic procedure of choice in the emergency department (ED). This modality should be strongly considered in first time stone presentation. The sensitivity is 95% to 97% and the specificity is 96% to 98%. Advantages of CT include its speed and that it avoids the risk of contrast allergy and can identify other pathologies. The disadvantage is that it doesn’t evaluate for renal function and the sensitivity and specificity for other diagnoses is low.
Noncontrast helical computed tomography (CT) is the diagnostic procedure of choice in the emergency department (ED). This modality should be strongly considered in first time stone presentation. The sensitivity is 95% to 97% and the specificity is 96% to 98%. Advantages of CT include its speed and that it avoids the risk of contrast allergy and can identify other pathologies. The disadvantage is that it doesn’t evaluate for renal function and the sensitivity and specificity for other diagnoses is low.
![]() Positive findings on CT for obstructive stone include ureteral caliber changes, suspicious calcifications, stranding of perinephric fat, increase in renal size, and dilation of the collecting system (see Fig. 58-1).
Positive findings on CT for obstructive stone include ureteral caliber changes, suspicious calcifications, stranding of perinephric fat, increase in renal size, and dilation of the collecting system (see Fig. 58-1).
![]() Ultrasound (US) is reserved for patients unable to undergo an IVP or CT. US is not a functional test and provides anatomic information only. It is useful in the detection of hydronephrosis and larger stones (>5 mm) in the proximal and distal ureter (see Fig. 58-2).
Ultrasound (US) is reserved for patients unable to undergo an IVP or CT. US is not a functional test and provides anatomic information only. It is useful in the detection of hydronephrosis and larger stones (>5 mm) in the proximal and distal ureter (see Fig. 58-2).
![]() The kidney-ureter-bladder (KUB) radiograph’s greatest utility is in following the migration of a known stone. Ninety percent ureteral stones are composed of calcium phosphate and calcium oxalate and are radiopaque. Radiopaque stones appear 20% greater than their original size.
The kidney-ureter-bladder (KUB) radiograph’s greatest utility is in following the migration of a known stone. Ninety percent ureteral stones are composed of calcium phosphate and calcium oxalate and are radiopaque. Radiopaque stones appear 20% greater than their original size.
![]() Summary of radiographic imaging is in Table 58-1.
Summary of radiographic imaging is in Table 58-1.

FIG. 58-1. A. Red arrow shows 6-mm stone within the proximal third of the left ureter on noncontrast CT reformatted image of upright abdomen. B. From same patient as in A, note 6-mm stone (arrow) within the proximal third of the left ureter on noncontrast CT.

FIG. 58-2. US of renal pelvis showing stones (marked with 1+ and 2+) with shadowing effects (arrows).
TABLE 58-1 Ancillary Tests in Urologic Stone Disease
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Patients are treated symptomatically. Pain medication including narcotics and nonsteroidal anti-inflammatory drugs should not be delayed pending test results. Intravenous antiemetic should be used. Intravenous fluids have not been shown to promote expulsion of the stone.
Patients are treated symptomatically. Pain medication including narcotics and nonsteroidal anti-inflammatory drugs should not be delayed pending test results. Intravenous antiemetic should be used. Intravenous fluids have not been shown to promote expulsion of the stone.
![]() In cases complicated by urinary tract infection (UTI), routine cultures of urine and blood are indicated and renal obstruction must be excluded. Antibiotics should be started promptly while the patient is in the emergency department. Considerations for intravenous (IV) antibiotics include gentamicin or tobramy-cin, 3.0 milligrams/kg/d divided every 8 hours, plus ampicillin, 1 to 2 grams every 4 hours. One can also consider cefipime, 2 grams IV every 8 hours; ticarcillin-clavulanic acid, 3.1 grams every 6 hours; ciprofloxacin, 400 milligrams every 12 hours; or piperacillin-tazobactam, 3.375 grams IV every 6 hours. Local sensitivites should help guide therapy.
In cases complicated by urinary tract infection (UTI), routine cultures of urine and blood are indicated and renal obstruction must be excluded. Antibiotics should be started promptly while the patient is in the emergency department. Considerations for intravenous (IV) antibiotics include gentamicin or tobramy-cin, 3.0 milligrams/kg/d divided every 8 hours, plus ampicillin, 1 to 2 grams every 4 hours. One can also consider cefipime, 2 grams IV every 8 hours; ticarcillin-clavulanic acid, 3.1 grams every 6 hours; ciprofloxacin, 400 milligrams every 12 hours; or piperacillin-tazobactam, 3.375 grams IV every 6 hours. Local sensitivites should help guide therapy.
![]() Hospitalization is required if the patient has an infection with concurrent obstruction, solitary kidney and complete obstruction, hypercalcemic crisis, uncontrolled pain, urosepsis, acute renal failure, or intractable emesis.
Hospitalization is required if the patient has an infection with concurrent obstruction, solitary kidney and complete obstruction, hypercalcemic crisis, uncontrolled pain, urosepsis, acute renal failure, or intractable emesis.
![]() Disposition should be discussed with a urologist in patients with a stone >6 mm, renal insufficiency, severe underlying disease, IVP with extravasation or complete obstruction, or failed outpatient management.
Disposition should be discussed with a urologist in patients with a stone >6 mm, renal insufficiency, severe underlying disease, IVP with extravasation or complete obstruction, or failed outpatient management.
![]() Discharge is appropriate in patients with rounded stones <4–5 mm, with no significant obstruction, and for whom pain is controlled by oral analgesics. Those patients with infection and no systemic signs of illness may be discharged on ciprofloxacin, 500 milligrams PO bid for 10 to 14 days; levofloxacin, 500 milligrams PO daily for 10 to 14 days; or cefpo-doxime, 200 milligrams PO bid 10 to 14 days. The individual should have follow-up with urology in 48 to 72 hours with explicit instructions to return for fever, nausea, or systemic illness.
Discharge is appropriate in patients with rounded stones <4–5 mm, with no significant obstruction, and for whom pain is controlled by oral analgesics. Those patients with infection and no systemic signs of illness may be discharged on ciprofloxacin, 500 milligrams PO bid for 10 to 14 days; levofloxacin, 500 milligrams PO daily for 10 to 14 days; or cefpo-doxime, 200 milligrams PO bid 10 to 14 days. The individual should have follow-up with urology in 48 to 72 hours with explicit instructions to return for fever, nausea, or systemic illness.
![]() Alpha-blockers are associated with increased rate of expulsion, decreased time to expulsion, and decreased pain with a number needed to treat of 3.3 and a 2- to 6-day improvement in time to expulsion. This should be considered in stones in the distal third of the ureter due to theorized increased alpha-receptors in this region. Tamsulosin (0.4 milligram daily), terazosin (5–10 milligrams daily), or doxazosin (4 milligrams daily) can be given daily for up to 4 weeks.
Alpha-blockers are associated with increased rate of expulsion, decreased time to expulsion, and decreased pain with a number needed to treat of 3.3 and a 2- to 6-day improvement in time to expulsion. This should be considered in stones in the distal third of the ureter due to theorized increased alpha-receptors in this region. Tamsulosin (0.4 milligram daily), terazosin (5–10 milligrams daily), or doxazosin (4 milligrams daily) can be given daily for up to 4 weeks.
![]() Calcium channel blockers have been used to promote stone expulsion but have increased adverse effects of hypotension. Nifedipine-XL, 30 milligrams daily up to 8 weeks, has been used. The number needed to treat is 3.9 and time to stone expulsion is reported as <28 days. Steroids are being considered as an adjunct to medical propulsion therapy to improve rates of expulsion.
Calcium channel blockers have been used to promote stone expulsion but have increased adverse effects of hypotension. Nifedipine-XL, 30 milligrams daily up to 8 weeks, has been used. The number needed to treat is 3.9 and time to stone expulsion is reported as <28 days. Steroids are being considered as an adjunct to medical propulsion therapy to improve rates of expulsion.
![]() Follow-up with a urologist is recommended for those patients with hematuria and no definitive diagnosis.
Follow-up with a urologist is recommended for those patients with hematuria and no definitive diagnosis.
![]() Patients whose stones pass in the emergency department require no further treatment.
Patients whose stones pass in the emergency department require no further treatment.
For further reading in Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 97, “Urologic Stone Disease,” by David E. Manthey and Bret A. Nicks.