Mary A. Wittler
FLUIDS
![]() An average normal adult requires approximately 2000–3000 mL of water per day to maintain fluid balance.
An average normal adult requires approximately 2000–3000 mL of water per day to maintain fluid balance.
![]() When altered, fluids and electrolytes should be corrected in the following order: (1) volume; (2) pH; (3) potassium, calcium, magnesium; and (4) sodium and chloride. Reestablishment of tissue perfusion often re-equilibrates the fluid-electrolyte and acid-base balance.
When altered, fluids and electrolytes should be corrected in the following order: (1) volume; (2) pH; (3) potassium, calcium, magnesium; and (4) sodium and chloride. Reestablishment of tissue perfusion often re-equilibrates the fluid-electrolyte and acid-base balance.
![]() Since the osmolarity of normal saline (NS) matches that of the serum, it is an excellent fluid for volume replacement.
Since the osmolarity of normal saline (NS) matches that of the serum, it is an excellent fluid for volume replacement.
![]() Hypotonic fluids such as 5% dextrose in water (D5W) should never be used to replace volume.
Hypotonic fluids such as 5% dextrose in water (D5W) should never be used to replace volume.
![]() Lactated Ringer’s solution is commonly used for surgical patients or trauma patients; however, only NS can be given in the same line with blood components.
Lactated Ringer’s solution is commonly used for surgical patients or trauma patients; however, only NS can be given in the same line with blood components.
![]() The more concentrated dextrose solutions, D10W or D20W, are used for patients with compromised ability to mobilize glucose stores, such as patients with hepatic failure, or as part of total parenteral nutrition (TPN) solutions.
The more concentrated dextrose solutions, D10W or D20W, are used for patients with compromised ability to mobilize glucose stores, such as patients with hepatic failure, or as part of total parenteral nutrition (TPN) solutions.
CLINICAL ASSESSMENT OF VOLUME STATUS
![]() Volume loss and dehydration can be inferred from the patient history. Historical features include vomiting, diarrhea, fever, adverse working conditions, decreased fluid intake, chronic disease, altered level of consciousness, and reduced urine output.
Volume loss and dehydration can be inferred from the patient history. Historical features include vomiting, diarrhea, fever, adverse working conditions, decreased fluid intake, chronic disease, altered level of consciousness, and reduced urine output.
![]() Tachycardia and hypotension are late signs of dehydration.
Tachycardia and hypotension are late signs of dehydration.
![]() Physical exam findings include dry mucosa, shrunken tongue (excellent indicator), and decreased skin turgor. In infants and children, sunken fontanelles, decreased capillary refill, lack of tears, and decreased wet diapers are typical signs and symptoms of dehydration (see Chap. 83).
Physical exam findings include dry mucosa, shrunken tongue (excellent indicator), and decreased skin turgor. In infants and children, sunken fontanelles, decreased capillary refill, lack of tears, and decreased wet diapers are typical signs and symptoms of dehydration (see Chap. 83).
![]() Lethargy and coma are more ominous signs and may indicate a significant comorbid condition.
Lethargy and coma are more ominous signs and may indicate a significant comorbid condition.
![]() Laboratory values are not reliable indicators of fluid status. Plasma and urine osmolarity are perhaps the most reliable measures of dehydration. Blood urea nitrogen (BUN), creatinine, hematocrit, and other chemistries are insensitive.
Laboratory values are not reliable indicators of fluid status. Plasma and urine osmolarity are perhaps the most reliable measures of dehydration. Blood urea nitrogen (BUN), creatinine, hematocrit, and other chemistries are insensitive.
![]() Volume overload is a purely clinical diagnosis and presents with edema (central or peripheral), respiratory distress (pulmonary edema), and jugular venous distention (in congestive heart failure [CHF]).
Volume overload is a purely clinical diagnosis and presents with edema (central or peripheral), respiratory distress (pulmonary edema), and jugular venous distention (in congestive heart failure [CHF]).
![]() The significant risk factors for volume overload are renal, cardiovascular, and liver disease. Blood pressure (BP) does not necessarily correlate with volume status alone; patients with volume overload can present with hypotension or hypertension.
The significant risk factors for volume overload are renal, cardiovascular, and liver disease. Blood pressure (BP) does not necessarily correlate with volume status alone; patients with volume overload can present with hypotension or hypertension.
MAINTENANCE FLUIDS
![]() Adult: D5½NS at 75 to 125 mL/h + 20 mEq/L of potassium chloride for an average adult (approximately 70 kg).
Adult: D5½NS at 75 to 125 mL/h + 20 mEq/L of potassium chloride for an average adult (approximately 70 kg).
![]() Children: D5½NS or D10½NS, 100 mL/kg/d for the first 10 kg (of body weight), 50 mL/kg/d for the second 10 kg, and 20 mL/kg/d for every kilogram thereafter (see Chap. 83 for further discussion of pediatric fluid management).
Children: D5½NS or D10½NS, 100 mL/kg/d for the first 10 kg (of body weight), 50 mL/kg/d for the second 10 kg, and 20 mL/kg/d for every kilogram thereafter (see Chap. 83 for further discussion of pediatric fluid management).
ELECTROLYTE DISORDERS
![]() Correcting a single abnormality may not be the only intervention needed, as most electrolytes exist in equilibrium with others.
Correcting a single abnormality may not be the only intervention needed, as most electrolytes exist in equilibrium with others.
![]() Laboratory errors are common. Results should be double-checked when the clinical picture and the laboratory data conflict.
Laboratory errors are common. Results should be double-checked when the clinical picture and the laboratory data conflict.
![]() Abnormalities should be corrected at the same rate they developed; however, slower correction is usually safe unless the condition warrants rapid and/or early intervention (ie, hypoglycemia, hyperkalemia).
Abnormalities should be corrected at the same rate they developed; however, slower correction is usually safe unless the condition warrants rapid and/or early intervention (ie, hypoglycemia, hyperkalemia).
![]() Evaluation of electrolyte disorders frequently requires a comparison of the measured and calculated osmolarity (number of particles per liter of solution). To calculate osmolarity, measured serum values in mEq/L are used:
Evaluation of electrolyte disorders frequently requires a comparison of the measured and calculated osmolarity (number of particles per liter of solution). To calculate osmolarity, measured serum values in mEq/L are used:
Osmolarity (mOsm/L) = 2 [Na+] + (glucose/18) + (BUN/2.8) + (ETOCH/4.6)
HYPONATREMIA ([Na+] <135 mEq/L)
CLINICAL FINDINGS
![]() The clinical manifestations of hyponatremia are more likely to occur when the [Na+] drops below 120 mEq/L, and include nausea, weakness, headache, agitation, hallucinations, cramps, confusion, lethargy, and seizures.
The clinical manifestations of hyponatremia are more likely to occur when the [Na+] drops below 120 mEq/L, and include nausea, weakness, headache, agitation, hallucinations, cramps, confusion, lethargy, and seizures.
DIAGNOSIS AND DIFFERENTIAL
![]() Evaluate volume status, measured serum, and calculated osmolarities.
Evaluate volume status, measured serum, and calculated osmolarities.
![]() True hyponatremia presents with reduced osmolarity in the face of normal volume status and low urine [Na+]. This state results from primary water gain, [Na+] loss greater than that of water, or alteration in the distribution of water.
True hyponatremia presents with reduced osmolarity in the face of normal volume status and low urine [Na+]. This state results from primary water gain, [Na+] loss greater than that of water, or alteration in the distribution of water.
![]() Factitious hyponatremia (false low measurement of the serum sodium) is due to hyperglycemia, hyper-proteinemia, hyperlipidemia, and other osmotically active solutes and is associated with a normal-to-high osmolarity.
Factitious hyponatremia (false low measurement of the serum sodium) is due to hyperglycemia, hyper-proteinemia, hyperlipidemia, and other osmotically active solutes and is associated with a normal-to-high osmolarity.
![]() The diagnostic criteria for syndrome of inappropriate secretion of antidiuretic hormone (SIADH) are (1) hypotonic hyponatremia, (2) inappropriately elevated urinary osmolality (usually >200 mOsm/kg), (3) elevated urinary [Na+] (typically >20 mEq/L), (4) clinical euvolemia, (5) normal adrenal, renal, cardiac, hepatic, and thyroid functions, and (6) correctable with water restriction.
The diagnostic criteria for syndrome of inappropriate secretion of antidiuretic hormone (SIADH) are (1) hypotonic hyponatremia, (2) inappropriately elevated urinary osmolality (usually >200 mOsm/kg), (3) elevated urinary [Na+] (typically >20 mEq/L), (4) clinical euvolemia, (5) normal adrenal, renal, cardiac, hepatic, and thyroid functions, and (6) correctable with water restriction.
![]() Isotonic hyponatremia (Posm 275–295) may be due to hyperlipidemia, hyperproteinemia, or hyperglycemia.
Isotonic hyponatremia (Posm 275–295) may be due to hyperlipidemia, hyperproteinemia, or hyperglycemia.
![]() Hypertonic hyponatremia (Posm >295) may be due to hyperglycemia, mannitol excess, or glycerol use.
Hypertonic hyponatremia (Posm >295) may be due to hyperglycemia, mannitol excess, or glycerol use.
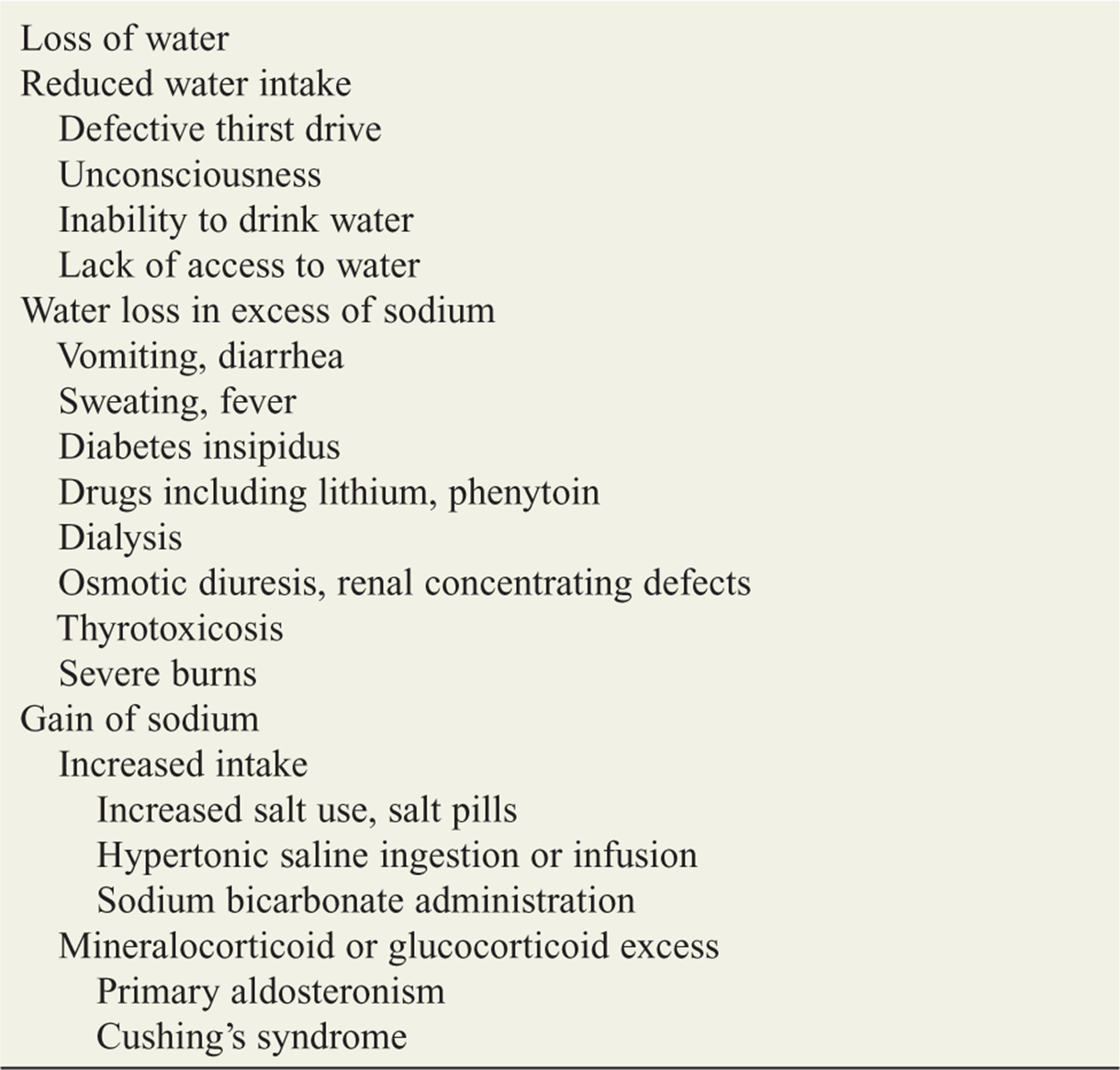
![]() Causes of hyponatremia are listed in Table 6-1.
Causes of hyponatremia are listed in Table 6-1.
TABLE 6-1 Causes of Hyponatremia

EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Correct existing volume or perfusion deficits with NS.
Correct existing volume or perfusion deficits with NS.
![]() In euvolemic or hypervolemic patients, restrict fluids (500–1500 mL of water daily).
In euvolemic or hypervolemic patients, restrict fluids (500–1500 mL of water daily).
![]() Treat severe hyponatremia ([Na+] <120 mEq/L) that has developed rapidly with central nervous system (CNS) changes such as coma or seizures with hypertonic saline, 3% NS (513 mEq/L), at 25–100 mL/h. The [Na+] should not be corrected faster than 0.5 mEq/L/h in chronic hyponatremia or 1.0 mEq/L/h in acute hyponatremia. The [Na+] correction should not exceed 12 mEq/L/d.
Treat severe hyponatremia ([Na+] <120 mEq/L) that has developed rapidly with central nervous system (CNS) changes such as coma or seizures with hypertonic saline, 3% NS (513 mEq/L), at 25–100 mL/h. The [Na+] should not be corrected faster than 0.5 mEq/L/h in chronic hyponatremia or 1.0 mEq/L/h in acute hyponatremia. The [Na+] correction should not exceed 12 mEq/L/d.
![]() The sodium dose can be calculated as follows: weight (kg) × 0.6 × (desired [Na+] – measured [Na+]) = sodium deficit (mEq).
The sodium dose can be calculated as follows: weight (kg) × 0.6 × (desired [Na+] – measured [Na+]) = sodium deficit (mEq).
![]() Complications of rapid correction include CHF and central pontine myelinolysis, which can cause alterations in consciousness, dysphagia, dysarthria, and paresis.
Complications of rapid correction include CHF and central pontine myelinolysis, which can cause alterations in consciousness, dysphagia, dysarthria, and paresis.
HYPERNATREMIA ([Na+] >150 mEq/L)
CLINICAL FEATURES
![]() Symptoms of hypernatremia are usually noticeable at a serum osmolarity >350 mOsm/L or [Na+] >158 mEq/L. Initial symptoms include irritability and ataxia; spasticity, hyperreflexia, lethargy, coma, and seizures occur with osmolarities above 400 mOsm/L.
Symptoms of hypernatremia are usually noticeable at a serum osmolarity >350 mOsm/L or [Na+] >158 mEq/L. Initial symptoms include irritability and ataxia; spasticity, hyperreflexia, lethargy, coma, and seizures occur with osmolarities above 400 mOsm/L.
![]() An osmolarity increase of 2% stimulates thirst to prevent hypernatremia.
An osmolarity increase of 2% stimulates thirst to prevent hypernatremia.
![]() Morbidity and mortality are highest in infants and the elderly, who may be unable to respond to increased thirst.
Morbidity and mortality are highest in infants and the elderly, who may be unable to respond to increased thirst.
DIAGNOSIS AND DIFFERENTIAL
![]() Hypernatremia is most commonly caused by a decrease in total body water due to decreased intake or excessive loss. It is less often due to an increase in total body [Na+].
Hypernatremia is most commonly caused by a decrease in total body water due to decreased intake or excessive loss. It is less often due to an increase in total body [Na+].
![]() Common causes are diarrhea, vomiting, hyperpyrexia, and excessive sweating.
Common causes are diarrhea, vomiting, hyperpyrexia, and excessive sweating.
![]() An important etiology of hypernatremia is diabetes insipidus (DI), which results in the loss of hypo-tonic urine. Central DI (no antidiuretic hormone secreted) results from CNS disease, surgery, or trauma. Nephrogenic DI (unresponsive to antidiuretic hormone) results from congenital disease, drugs, hypercalcemia, hypokalemia, or renal disease.
An important etiology of hypernatremia is diabetes insipidus (DI), which results in the loss of hypo-tonic urine. Central DI (no antidiuretic hormone secreted) results from CNS disease, surgery, or trauma. Nephrogenic DI (unresponsive to antidiuretic hormone) results from congenital disease, drugs, hypercalcemia, hypokalemia, or renal disease.
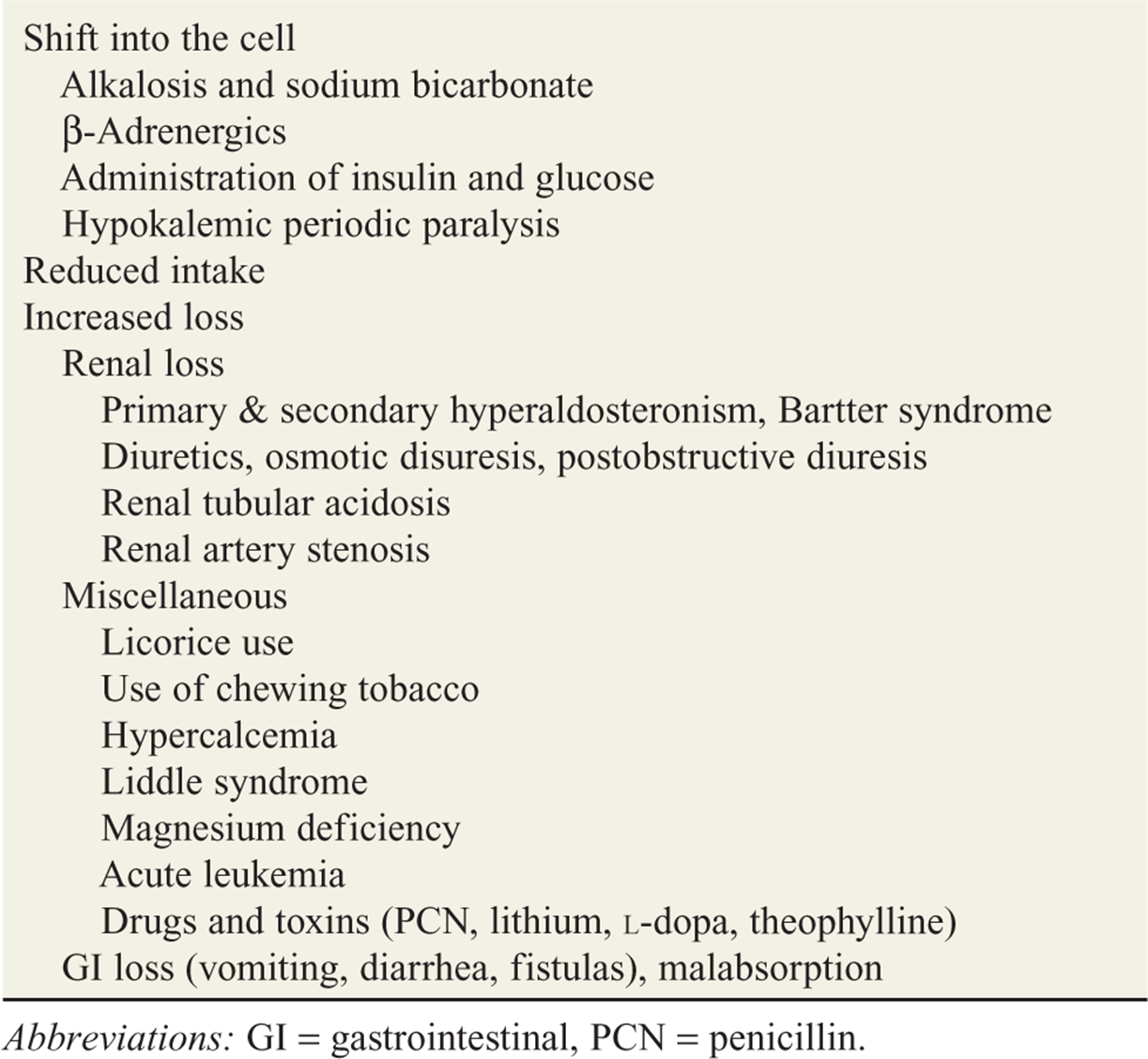
![]() The causes of hypernatremia are listed in Table 6-2.
The causes of hypernatremia are listed in Table 6-2.
TABLE 6-2 Causes of Hypernatremia
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Correct existing volume or perfusion deficits with NS or lactated Ringer’s solution. Free water deficits are corrected with ½NS. Avoid lowering the [Na+] more than 10 mEq/L/d.
Correct existing volume or perfusion deficits with NS or lactated Ringer’s solution. Free water deficits are corrected with ½NS. Avoid lowering the [Na+] more than 10 mEq/L/d.
![]() Each liter of water deficit causes the [Na+] to increase 3 to 5 mEq/L. Use the formula to calculate the free water deficit: water deficit (L) = (measured [Na+]/desired [Na+])– 1.
Each liter of water deficit causes the [Na+] to increase 3 to 5 mEq/L. Use the formula to calculate the free water deficit: water deficit (L) = (measured [Na+]/desired [Na+])– 1.
![]() If no urine output is observed after NS or lactated Ringer’s solution rehydration, rapidly switch to ½NS: unload the body of the extra sodium by using a diuretic (eg, furosemide 20–40 milligrams IV).
If no urine output is observed after NS or lactated Ringer’s solution rehydration, rapidly switch to ½NS: unload the body of the extra sodium by using a diuretic (eg, furosemide 20–40 milligrams IV).
![]() Central diabetes insipidus DI is treated with desmo-pressin with careful monitoring of electrolytes, and urine osmolarity and specific gravity. Consult a specialist.
Central diabetes insipidus DI is treated with desmo-pressin with careful monitoring of electrolytes, and urine osmolarity and specific gravity. Consult a specialist.
In children with a serum sodium level higher than 180 mEq/L, consider peritoneal dialysis using high-glucose, low-[Na+] dialysate in consultation with a pediatric nephrologist.
HYPOKALEMIA ([K+] <3.5 mEq/L)
CLINICAL FEATURES
![]() The signs and symptoms of hypokalemia usually occur at levels below 2.5 mEq/L and affect the multiple body systems: the central nervous system (weakness, cramps, hyporeflexia, paresthesias), gastrointestinal system (ileus), cardiovascular system (dysrhythmias, worsening of digoxin toxicity, hypotension or hypertension, U waves, ST-segment depression, prolonged QT interval), and renal system (metabolic alkalosis, worsening hepatic encephalopathy). Glucose intolerance can also develop.
The signs and symptoms of hypokalemia usually occur at levels below 2.5 mEq/L and affect the multiple body systems: the central nervous system (weakness, cramps, hyporeflexia, paresthesias), gastrointestinal system (ileus), cardiovascular system (dysrhythmias, worsening of digoxin toxicity, hypotension or hypertension, U waves, ST-segment depression, prolonged QT interval), and renal system (metabolic alkalosis, worsening hepatic encephalopathy). Glucose intolerance can also develop.
DIAGNOSIS AND DIFFERENTIAL
![]() Causes can be grouped by decreased [K+] intake, increased [K+] excretion, or transcellular shift. The most common cause is the use of loop diuretics.
Causes can be grouped by decreased [K+] intake, increased [K+] excretion, or transcellular shift. The most common cause is the use of loop diuretics.
![]() Table 6-3 lists the causes of hypokalemia.
Table 6-3 lists the causes of hypokalemia.
TABLE 6-3 Causes of Hypokalemia
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Giving 20 mEq/dose [K+] will raise the [K+] by 0.25 mEq/L.
Giving 20 mEq/dose [K+] will raise the [K+] by 0.25 mEq/L.
![]() In stable patients, oral replacement is preferred (safe and rapid); a 20- to 40-mEq [K+] dose is used.
In stable patients, oral replacement is preferred (safe and rapid); a 20- to 40-mEq [K+] dose is used.
![]() In unstable patients, IV potassium chloride (KC1) in doses of 10 to 20 mEq/h may be given. Add no more than 40 mEq of KC1 to each liter of IV fluid. Infusion rates should not exceed 40 mEq/h.
In unstable patients, IV potassium chloride (KC1) in doses of 10 to 20 mEq/h may be given. Add no more than 40 mEq of KC1 to each liter of IV fluid. Infusion rates should not exceed 40 mEq/h.
![]() Doses greater than 20 mEq/h should be given through a central line. Patients should be monitored continuously for dysrhythmias.
Doses greater than 20 mEq/h should be given through a central line. Patients should be monitored continuously for dysrhythmias.
HYPERKALEMIA ([K+] >5.5 mEq/L)
CLINICAL FEATURES
![]() The most concerning and serious manifestations of hyperkalemia are the cardiac effects.
The most concerning and serious manifestations of hyperkalemia are the cardiac effects.
![]() At levels of 6.5 to 7.5 mEq/L the electrocardiogram (ECG) shows peaked T waves (precordial leads—see Fig. 6-1), prolonged PR intervals, and short QT intervals. At levels of 7.5 to 8.0 mEq/L, the QRS widens and the P wave flattens. At levels above 8 mEq/L, a sine-wave pattern, ventricular fibrillation, and heart blocks occur.
At levels of 6.5 to 7.5 mEq/L the electrocardiogram (ECG) shows peaked T waves (precordial leads—see Fig. 6-1), prolonged PR intervals, and short QT intervals. At levels of 7.5 to 8.0 mEq/L, the QRS widens and the P wave flattens. At levels above 8 mEq/L, a sine-wave pattern, ventricular fibrillation, and heart blocks occur.
![]() Neuromuscular symptoms include weakness and paralysis. GI symptoms include vomiting, colic, and diarrhea.
Neuromuscular symptoms include weakness and paralysis. GI symptoms include vomiting, colic, and diarrhea.
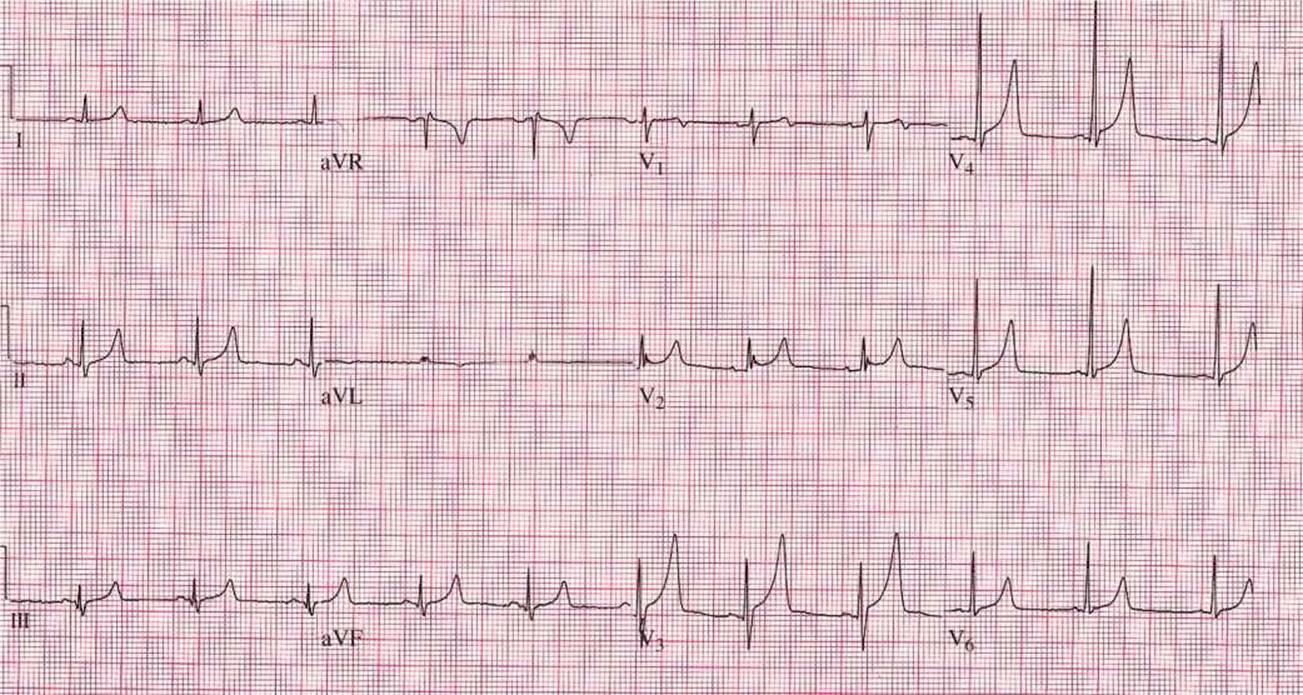
FIG. 6-1. Electrocardiogram of hyperkalemia. Note the narrow, tall, peaked T waves consistent with hyperkalemia. The patient was 3 days overdue for hemodialysis and was found to have a potassium of 7.4 mEq/L. (Figure supplied by David M. Cline, MD, Wake Forest Baptist Health.)
DIAGNOSIS AND DIFFERENTIAL
![]() Beware of pseudohyperkalemia, which is caused by hemolysis associated with blood draws.
Beware of pseudohyperkalemia, which is caused by hemolysis associated with blood draws.
![]() Renal failure with oliguria is the most common cause of true hyperkalemia.
Renal failure with oliguria is the most common cause of true hyperkalemia.
![]() Appropriate tests for management include an ECG, electrolytes, calcium, magnesium, arterial blood gases (ABGs; check for acidosis), urinalysis, and a digoxin level in appropriate patients.
Appropriate tests for management include an ECG, electrolytes, calcium, magnesium, arterial blood gases (ABGs; check for acidosis), urinalysis, and a digoxin level in appropriate patients.
![]() Causes of hyperkalemia are listed in Table 6-4.
Causes of hyperkalemia are listed in Table 6-4.
TABLE 6-4 Causes of Hyperkalemia

EMERGENCY DEPARTMENT CARE AND DISPOSITION
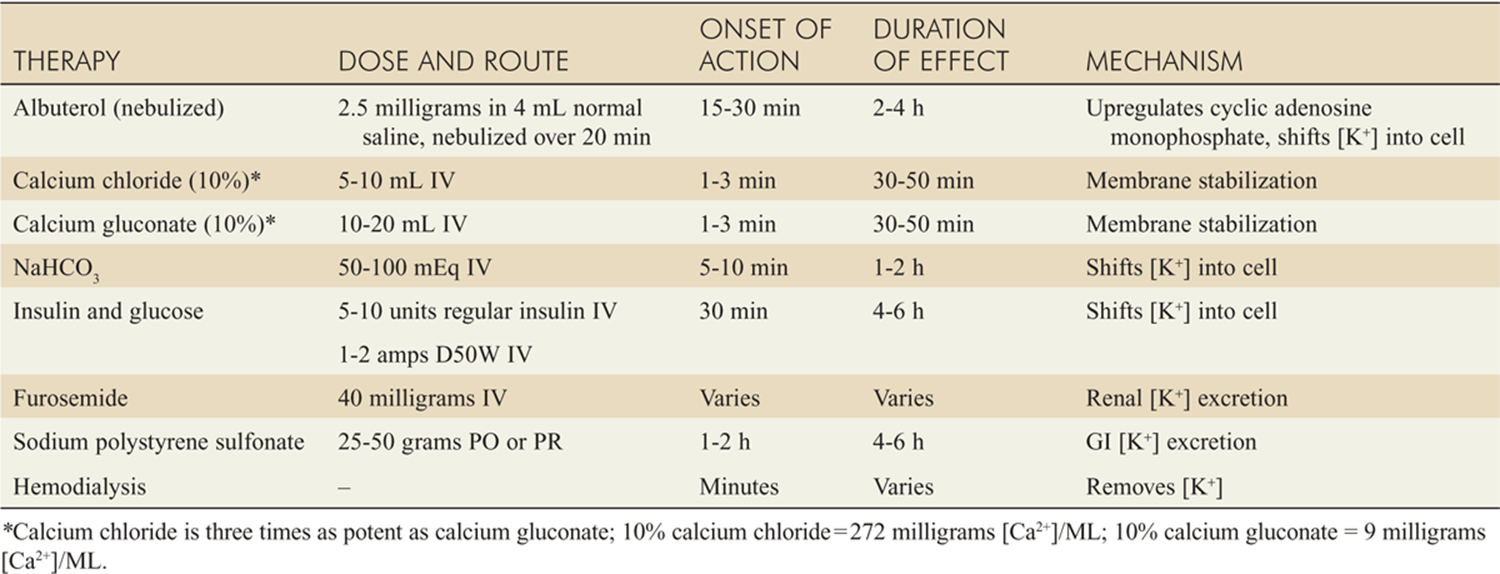
![]() Symptomatic patients are treated in a stepwise approach: stabilize the cardiac membrane with Ca-gluconate or calcium chloride (CaCl2); shift the [K+] into the cell using glucose and insulin and/or bicarbonate and/or albuterol; finally, excrete the [K+] using sodium polystyrene sulfonate, diuretics, or dialysis in severe cases. Table 6-5 summarizes the treatment including medication doses.
Symptomatic patients are treated in a stepwise approach: stabilize the cardiac membrane with Ca-gluconate or calcium chloride (CaCl2); shift the [K+] into the cell using glucose and insulin and/or bicarbonate and/or albuterol; finally, excrete the [K+] using sodium polystyrene sulfonate, diuretics, or dialysis in severe cases. Table 6-5 summarizes the treatment including medication doses.
![]() For levels over 7.0 mEq/L or for any ECG changes, give IV CaCl2 or Ca-gluconate (Table 6-5). In children, Ca-gluconate (10%) 0.5 mL/kg is given.
For levels over 7.0 mEq/L or for any ECG changes, give IV CaCl2 or Ca-gluconate (Table 6-5). In children, Ca-gluconate (10%) 0.5 mL/kg is given.
![]() The presence of digoxin toxicity with hyperkalemia is an indication for digoxin immune Fab (Digibind) therapy (see Chap. 110). Calcium administration should be avoided.
The presence of digoxin toxicity with hyperkalemia is an indication for digoxin immune Fab (Digibind) therapy (see Chap. 110). Calcium administration should be avoided.
![]() In acidotic patients, consider giving sodium bicarbonate 50–100 mEq slow IV In children, 1 mEq/kg is given slow IV.
In acidotic patients, consider giving sodium bicarbonate 50–100 mEq slow IV In children, 1 mEq/kg is given slow IV.
![]() When treating dialysis/renal failure patients with glucose and insulin, reduce the insulin dose to 5 unit regular insulin. In children, 0.5–1 gram/kg of glucose as D10W plus insulin 0.1 units/kg is given.
When treating dialysis/renal failure patients with glucose and insulin, reduce the insulin dose to 5 unit regular insulin. In children, 0.5–1 gram/kg of glucose as D10W plus insulin 0.1 units/kg is given.
![]() Diuresis is maintained with furosemide 20 to 40 milligrams IV.
Diuresis is maintained with furosemide 20 to 40 milligrams IV.
![]() Sodium polystyrene sulfonate (Kayexalate) (PO or rectally [PR]) 1 gram binds 1 mEq of [K+]. Administer 15 to 30 grams Kayexalate PO with sorbitol or 30 to 50 grams PR with sorbitol. Kayexalate can exacerbate CHF. In children, give Kayexalate 1 gram/kg PO or PR.
Sodium polystyrene sulfonate (Kayexalate) (PO or rectally [PR]) 1 gram binds 1 mEq of [K+]. Administer 15 to 30 grams Kayexalate PO with sorbitol or 30 to 50 grams PR with sorbitol. Kayexalate can exacerbate CHF. In children, give Kayexalate 1 gram/kg PO or PR.
![]() Albuterol 5 to 10 milligrams (by nebulization) may also be used to lower [K+].
Albuterol 5 to 10 milligrams (by nebulization) may also be used to lower [K+].
![]() In patients with acute renal failure, consult a neph-rologist for emergent dialysis.
In patients with acute renal failure, consult a neph-rologist for emergent dialysis.
TABLE 6-5 Emergency Therapy of Hyperkalemia
HYPOCALCEMIA ([Ca2+] <8.5 mEq/L OR IONIZED LEVEL <2.0 mEq/L)
CLINICAL FEATURES
![]() The signs and symptoms of hypocalcemia are usually seen with ionized [Ca2+] levels below 1.5 mEq/L. Symptoms include paresthesias, increased deep tendon reflexes (DTRs), cramps, weakness, confusion, and seizures.
The signs and symptoms of hypocalcemia are usually seen with ionized [Ca2+] levels below 1.5 mEq/L. Symptoms include paresthesias, increased deep tendon reflexes (DTRs), cramps, weakness, confusion, and seizures.
![]() Patients may also demonstrate Chvostek’s sign (twitch of the corner of mouth on tapping with a finger over cranial nerve VII at the zygoma) or Trousseau’s sign (more reliable; carpal spasm when the BP cuff is left inflated at a pressure above the systolic BP for greater than 3 minutes). Low [Ca2+] decreased myocardial contractility, and may precipitate CHF or long QT on the EKG.
Patients may also demonstrate Chvostek’s sign (twitch of the corner of mouth on tapping with a finger over cranial nerve VII at the zygoma) or Trousseau’s sign (more reliable; carpal spasm when the BP cuff is left inflated at a pressure above the systolic BP for greater than 3 minutes). Low [Ca2+] decreased myocardial contractility, and may precipitate CHF or long QT on the EKG.
DIAGNOSIS AND DIFFERENTIAL
![]() Causes include shock, sepsis, renal failure, pancreatitis, drugs (usually cimetidine), hypoparathyroidism, hyperphosphatemia, vitamin D deficiency, hypomag-nesemia, and fluoride poisoning.
Causes include shock, sepsis, renal failure, pancreatitis, drugs (usually cimetidine), hypoparathyroidism, hyperphosphatemia, vitamin D deficiency, hypomag-nesemia, and fluoride poisoning.
![]() Alkalosis decreases the ionized [Ca2+] (physiologically active form) without changing the total [Ca2+] level.
Alkalosis decreases the ionized [Ca2+] (physiologically active form) without changing the total [Ca2+] level.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() If asymptomatic, then use calcium gluconate tablets, 1–4 grams/d PO divided every 6 hours with or without vitamin D (calcitriol 0.2 microgram twice daily). Milk is not a good substitute.
If asymptomatic, then use calcium gluconate tablets, 1–4 grams/d PO divided every 6 hours with or without vitamin D (calcitriol 0.2 microgram twice daily). Milk is not a good substitute.
![]() If symptomatic, then use calcium gluconate or calcium chloride, 10 mL of a 10% solution, given over 10 minutes by slow IV injection.
If symptomatic, then use calcium gluconate or calcium chloride, 10 mL of a 10% solution, given over 10 minutes by slow IV injection.
![]() Replace magnesium in conjunction with [Ca2+].
Replace magnesium in conjunction with [Ca2+].
HYPERCALCEMIA ([Ca2+] >10.5 mEq/L OR IONIZED [Ca2+] >2.7 mEq/L)
![]() Several factors affect the serum calcium level: parathyroid hormone (PTH) increases calcium; calcitonin and vitamin D metabolites decrease calcium.
Several factors affect the serum calcium level: parathyroid hormone (PTH) increases calcium; calcitonin and vitamin D metabolites decrease calcium.
![]() Decreased [H+] causes a decrease in ionized [Ca2+].
Decreased [H+] causes a decrease in ionized [Ca2+].
![]() A decrease in albumin causes a decrease in [Ca2+], but not in the ionized portion.
A decrease in albumin causes a decrease in [Ca2+], but not in the ionized portion.
CLINICAL FEATURES
![]() Clinical signs and symptoms develop at levels above 12 milligrams/dL.
Clinical signs and symptoms develop at levels above 12 milligrams/dL.
![]() A mnemonic to aid recall of common hypercalcemia symptoms is stones (renal calculi), bones (osteo-lysis), psychic moans (lethargy, weakness, fatigue, confusion), and abdominal groans (abdominal pain, constipation, polyuria, polydipsia).
A mnemonic to aid recall of common hypercalcemia symptoms is stones (renal calculi), bones (osteo-lysis), psychic moans (lethargy, weakness, fatigue, confusion), and abdominal groans (abdominal pain, constipation, polyuria, polydipsia).
![]() ECG changes include depressed ST segments, widened T waves, shortened QT intervals, and heart blocks.
ECG changes include depressed ST segments, widened T waves, shortened QT intervals, and heart blocks.
DIAGNOSIS AND DIFFERENTIAL
![]() Most cases of hypercalcemia are due to hyperpara-thyroidism or malignancies.
Most cases of hypercalcemia are due to hyperpara-thyroidism or malignancies.
![]() A mnemonic to aid recall the common causes is PAM P. SCHMIDT: parathyroid hormone, Addison’s disease, multiple myeloma, Paget’s disease, sarcoido-sis, cancer, hyperthyroidism, milk-alkali syndrome, immobilization, excess vitamin D, and thiazides.
A mnemonic to aid recall the common causes is PAM P. SCHMIDT: parathyroid hormone, Addison’s disease, multiple myeloma, Paget’s disease, sarcoido-sis, cancer, hyperthyroidism, milk-alkali syndrome, immobilization, excess vitamin D, and thiazides.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Initiate treatment in patients with severe symptoms, [Ca2+] greater than 14 milligrams/dL, or significant dehydration. Treatment therapies include volume repletion, decrease osteoclastic activity, and correct underlying cause.
Initiate treatment in patients with severe symptoms, [Ca2+] greater than 14 milligrams/dL, or significant dehydration. Treatment therapies include volume repletion, decrease osteoclastic activity, and correct underlying cause.
![]() Correct fluid deficits with NS; several liters may be required. Consider invasive monitoring.
Correct fluid deficits with NS; several liters may be required. Consider invasive monitoring.
![]() Furosemide and other loop diuretics are no longer recommended.
Furosemide and other loop diuretics are no longer recommended.
![]() Drugs that inhibit osteoclastic activity include the bisphosphonates, calcitonin, and glucocorticoids. Recommendations for initiating therapy in the ED are lacking; consultation with a specialist is advised.
Drugs that inhibit osteoclastic activity include the bisphosphonates, calcitonin, and glucocorticoids. Recommendations for initiating therapy in the ED are lacking; consultation with a specialist is advised.
HYPOMAGNESEMIA
CLINICAL FEATURES
![]() [Mg2+], [K+], and [PO4–] move together intra- and extracellularly.
[Mg2+], [K+], and [PO4–] move together intra- and extracellularly.
![]() Hypomagnesemia presents nonspecifically, with CNS symptoms (depression, confusion, vertigo, ataxia, tetany, weakness) or cardiac symptoms (arrhythmias, hypotension, and prolonged PR, QRS, and QT intervals).
Hypomagnesemia presents nonspecifically, with CNS symptoms (depression, confusion, vertigo, ataxia, tetany, weakness) or cardiac symptoms (arrhythmias, hypotension, and prolonged PR, QRS, and QT intervals).
![]() Other clinical manifestations of hypomagnesemia include anemia, hypotension, hypothermia, and dysphagia.
Other clinical manifestations of hypomagnesemia include anemia, hypotension, hypothermia, and dysphagia.
DIAGNOSIS AND DIFFERENTIAL
![]() The diagnosis should not be based on [Mg2+] levels as severe depletion can occur before any significant laboratory changes; it must therefore be suspected clinically.
The diagnosis should not be based on [Mg2+] levels as severe depletion can occur before any significant laboratory changes; it must therefore be suspected clinically.
![]() In adults, the most common cause is alcoholism, followed by poor nutrition, cirrhosis, pancreatitis, correction of diabetic ketoacidosis (DKA), excessive GI losses, and renal wasting.
In adults, the most common cause is alcoholism, followed by poor nutrition, cirrhosis, pancreatitis, correction of diabetic ketoacidosis (DKA), excessive GI losses, and renal wasting.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Volume deficits and concomitant electrolyte abnormalities should be cautiously corrected.
Volume deficits and concomitant electrolyte abnormalities should be cautiously corrected.
![]() Oral [Mg2+] replacement is sufficient for most patients.
Oral [Mg2+] replacement is sufficient for most patients.
![]() In patients with severe symptoms (delirium tremens, seizure, dysrhythmias) and normal renal function, magnesium sulfate 2 grams IV is administered over an hour, and may be followed by 6 grams over the first 24 hours. Continuous cardiac monitoring and checking frequent DTRs is recommended.
In patients with severe symptoms (delirium tremens, seizure, dysrhythmias) and normal renal function, magnesium sulfate 2 grams IV is administered over an hour, and may be followed by 6 grams over the first 24 hours. Continuous cardiac monitoring and checking frequent DTRs is recommended.
HYPERMAGNESEMIA
CLINICAL FEATURES
![]() Signs and symptoms manifest progressively; nausea and somnolence occur initially, muscle weakness develops and DTRs disappear above [Mg2+] 4.0 mEq/L; respiratory depression is noted above [Mg2+] 8 mEq/L; and hypotension and EKG changes occur above [Mg2+] 12 mEq/L.
Signs and symptoms manifest progressively; nausea and somnolence occur initially, muscle weakness develops and DTRs disappear above [Mg2+] 4.0 mEq/L; respiratory depression is noted above [Mg2+] 8 mEq/L; and hypotension and EKG changes occur above [Mg2+] 12 mEq/L.
DIAGNOSIS AND DIFFERENTIAL
![]() Hypermagnesemia is rare. Common causes are renal failure with concomitant ingestion of [Mg2+]-containing preparations (antacids) and lithium ingestion. Serum levels are diagnostic. Suspect coexisting increases in potassium and phosphate.
Hypermagnesemia is rare. Common causes are renal failure with concomitant ingestion of [Mg2+]-containing preparations (antacids) and lithium ingestion. Serum levels are diagnostic. Suspect coexisting increases in potassium and phosphate.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() In many patients, stopping [Mg2+] intake is sufficient. More aggressive therapy includes rehydration with NS.
In many patients, stopping [Mg2+] intake is sufficient. More aggressive therapy includes rehydration with NS.
![]() In severely symptomatic patients, CaCl (10% solution) 5 mL IV antagonizes the magnesium effects.
In severely symptomatic patients, CaCl (10% solution) 5 mL IV antagonizes the magnesium effects.
ACID-BASE DISORDERS
CLINICAL FEATURES
![]() Several conditions should alert the clinician to possible acid-base disorders: a history of renal, pulmonary, or psychiatric disorders (drug ingestion); or signs of acute disease: tachypnea, cyanosis, Kussmaul’s respiration, respiratory failure, shock, mental status alteration, vomiting, diarrhea, or other acute fluid losses.
Several conditions should alert the clinician to possible acid-base disorders: a history of renal, pulmonary, or psychiatric disorders (drug ingestion); or signs of acute disease: tachypnea, cyanosis, Kussmaul’s respiration, respiratory failure, shock, mental status alteration, vomiting, diarrhea, or other acute fluid losses.
![]() Acidosis is due to a gain of acid or a loss of base; causes may be metabolic (fall in serum [HCO3–]) or respiratory (rise in PCO2).
Acidosis is due to a gain of acid or a loss of base; causes may be metabolic (fall in serum [HCO3–]) or respiratory (rise in PCO2).
![]() Alkalosis is due to a loss of acid or an addition of base, and is either metabolic (rise in serum [HCO3–]) or respiratory (fall in PCO2).
Alkalosis is due to a loss of acid or an addition of base, and is either metabolic (rise in serum [HCO3–]) or respiratory (fall in PCO2).
![]() The lungs and kidneys primarily maintain the acid-base regulation. Compensatory mechanisms of the lungs and kidneys will return the pH toward but not to normal.
The lungs and kidneys primarily maintain the acid-base regulation. Compensatory mechanisms of the lungs and kidneys will return the pH toward but not to normal.
DIAGNOSIS AND DIFFERENTIAL
![]() The diagnosis and differential begins with measurement and analysis (with the stepwise approach below) of serum [HCO3–] from the electrolyte panel, and the pH and PCO2 from the ABG.
The diagnosis and differential begins with measurement and analysis (with the stepwise approach below) of serum [HCO3–] from the electrolyte panel, and the pH and PCO2 from the ABG.
![]() In a mixed disorder the pH, PCO2, and [HCO3–] may be normal, and the only clue to a metabolic acidosis is a wide anion gap (AG; see step 3 in the next section).
In a mixed disorder the pH, PCO2, and [HCO3–] may be normal, and the only clue to a metabolic acidosis is a wide anion gap (AG; see step 3 in the next section).
STEPWISE METHOD OF ACID-BASE CLINICAL PROBLEM SOLVING
![]() Use the patient’s pre-illness values as a baseline; otherwise, use as normal: pH = 7.4, [HCO3–] = 24 mm/L, PCO2 = 40 mm Hg.
Use the patient’s pre-illness values as a baseline; otherwise, use as normal: pH = 7.4, [HCO3–] = 24 mm/L, PCO2 = 40 mm Hg.
1. Examine the pH for acidemia (pH < 7.4) or alka-lemia (pH > 7.4).
2. Establish the primary mechanism by evaluating the [HCO3-] and PCO2.
![]() Metabolic acidosis: pH < 7.4 and [HCO3–] < 24 mEq/L
Metabolic acidosis: pH < 7.4 and [HCO3–] < 24 mEq/L
![]() Metabolic alkalosis: pH > 7.4 and [HCO3–] > 24 mEq/L
Metabolic alkalosis: pH > 7.4 and [HCO3–] > 24 mEq/L
![]() Respiratory acidosis: pH < 7.4 and PCO2 > 40 mm Hg
Respiratory acidosis: pH < 7.4 and PCO2 > 40 mm Hg
![]() Respiratory alkalosis: pH > 7.4 and PCO2 < 40 mm Hg
Respiratory alkalosis: pH > 7.4 and PCO2 < 40 mm Hg
3. Calculate the AG: [Na+] - ([Cl–] + [HCO3]) = approximately 10–12 mEq/L is normal.
![]() If the AG is greater than 15, then an anion gap metabolic acidosis (AGMA) is present.
If the AG is greater than 15, then an anion gap metabolic acidosis (AGMA) is present.
![]() If the AG is less than 15, and a metabolic acidosis is present (low [HCO3~]), then a nonwidened anion gap (or hyperchloremic) metabolic acidosis (NAGMA) is present.
If the AG is less than 15, and a metabolic acidosis is present (low [HCO3~]), then a nonwidened anion gap (or hyperchloremic) metabolic acidosis (NAGMA) is present.
4. For AGMA, evaluate for a concomitant hidden metabolic process: each 1 mEq/L decrease in [HCO3”] results in a 1 mEq/L increase in the AG. Compare the A Gap (= present gap – 12) to the A [HCO3-] (= 24 – present [HCO3]).
![]() Δ Gap = Δ [HCO3–]: pure AGMA
Δ Gap = Δ [HCO3–]: pure AGMA
![]() Δ Gap > Δ [HCO3–]: concomitant metabolic alkalosis is likely present
Δ Gap > Δ [HCO3–]: concomitant metabolic alkalosis is likely present
![]() Δ Gap < Δ [HCO3–]: concomitant NAGMA is likely present
Δ Gap < Δ [HCO3–]: concomitant NAGMA is likely present
5. For a primary metabolic process, estimate the respiratory compensatory response. If the compensatory response is not as expected, then the compensatory mechanism requires more time for complete mobilization or a secondary acid-base disturbance exists.
![]() Metabolic acidosis: expected PCO2 = (1.5 × [HCO3”] + 8) ± 2. A simpler observation is the PCO2 decreases by 1 mm Hg for every 1-mEq/dL decrease in [HCO3–]. This process takes 12–24 hours.
Metabolic acidosis: expected PCO2 = (1.5 × [HCO3”] + 8) ± 2. A simpler observation is the PCO2 decreases by 1 mm Hg for every 1-mEq/dL decrease in [HCO3–]. This process takes 12–24 hours.
![]() Metabolic alkalosis: expected PCO2 = 0.9 [HCO3–] + 16.
Metabolic alkalosis: expected PCO2 = 0.9 [HCO3–] + 16.
![]() Current PCO2 = expected PCO2: normal respiratory compensation.
Current PCO2 = expected PCO2: normal respiratory compensation.
![]() Current PCO2 < expected PCO2: possible concomitant respiratory alkalosis.
Current PCO2 < expected PCO2: possible concomitant respiratory alkalosis.
![]() Current PCO2 > expected PCO2: possible concomitant respiratory acidosis.
Current PCO2 > expected PCO2: possible concomitant respiratory acidosis.
6. For a primary respiratory process, estimate the compensatory metabolic response. If the compensatory response is not as expected, then the compensatory mechanism requires more time for complete mobilization or a secondary acid-base disturbance exists.
![]() Respiratory acidosis: clinically judge whether the process is acute (<72 hours) or chronic (>72 hours). The [HCO3–] increases 1 mEq/L (acute) or 4 mEq/L (chronic) for every 10-mm Hg increase in PCO2.
Respiratory acidosis: clinically judge whether the process is acute (<72 hours) or chronic (>72 hours). The [HCO3–] increases 1 mEq/L (acute) or 4 mEq/L (chronic) for every 10-mm Hg increase in PCO2.
![]() Respiratory alkalosis: clinically judge whether the process is acute (<72 hours) or chronic (>72 hours). The [HCO3–] decreases 2 mEq/L (acute) or 5 mEq/L (chronic) for every 10-mm Hg decrease in PCO2.
Respiratory alkalosis: clinically judge whether the process is acute (<72 hours) or chronic (>72 hours). The [HCO3–] decreases 2 mEq/L (acute) or 5 mEq/L (chronic) for every 10-mm Hg decrease in PCO2.
![]() Current [HCO3–] = expected [HCO3–]: normal metabolic compensation.
Current [HCO3–] = expected [HCO3–]: normal metabolic compensation.
![]() Current [HCO3–] < expected [HCO3–]: possible concomitant metabolic acidosis.
Current [HCO3–] < expected [HCO3–]: possible concomitant metabolic acidosis.
![]() Current [HCO3 ] > expected [HCO3 ]: possible concomitant metabolic alkalosis.
Current [HCO3 ] > expected [HCO3 ]: possible concomitant metabolic alkalosis.
7. See the later sections in this chapter for determining the etiology and management.
METABOLIC ACIDOSIS
![]() Metabolic acidosis should be divided into a wide and normal AG acidosis. The term anion gap is misleading because the serum has no gap between total positive and negative ions; however, the unmeasured anions exceed the unmeasured cations.
Metabolic acidosis should be divided into a wide and normal AG acidosis. The term anion gap is misleading because the serum has no gap between total positive and negative ions; however, the unmeasured anions exceed the unmeasured cations.
CLINICAL FEATURES
![]() No matter the etiology, acidosis can cause nausea and vomiting, abdominal pain, change in sensorium, tachy-pnea, and sometimes a Kussmaul’s respiratory pattern.
No matter the etiology, acidosis can cause nausea and vomiting, abdominal pain, change in sensorium, tachy-pnea, and sometimes a Kussmaul’s respiratory pattern.
![]() Acidosis causes many negative physiologic effects that result in hypoxia: cardiac contractility decreases; hepatic, renal, and systemic BP decreases; pulmonary vasculature resistance increases; and a catabolic state exists.
Acidosis causes many negative physiologic effects that result in hypoxia: cardiac contractility decreases; hepatic, renal, and systemic BP decreases; pulmonary vasculature resistance increases; and a catabolic state exists.
![]() Patients may present with nonspecific complaints or shock.
Patients may present with nonspecific complaints or shock.
DIAGNOSIS AND DIFFERENTIAL
![]() Causes of metabolic acidosis can be divided into two main groups: (1) those associated with increased production of organic acids (AGMA; see Table 6-6); and (2) those associated with a loss of [HCO3_], failure to excrete [H+], or addition of [H+] (NAGMA; see Table 6-7).
Causes of metabolic acidosis can be divided into two main groups: (1) those associated with increased production of organic acids (AGMA; see Table 6-6); and (2) those associated with a loss of [HCO3_], failure to excrete [H+], or addition of [H+] (NAGMA; see Table 6-7).
![]() A mnemonic to aid recall the causes of AGMA is A MUD PILES: alcohol, methanol, uremia, DKA, paraldehyde,/iron and/soniazid,/actic acidosis, ethylene glycol, salicylates, and starvation.
A mnemonic to aid recall the causes of AGMA is A MUD PILES: alcohol, methanol, uremia, DKA, paraldehyde,/iron and/soniazid,/actic acidosis, ethylene glycol, salicylates, and starvation.
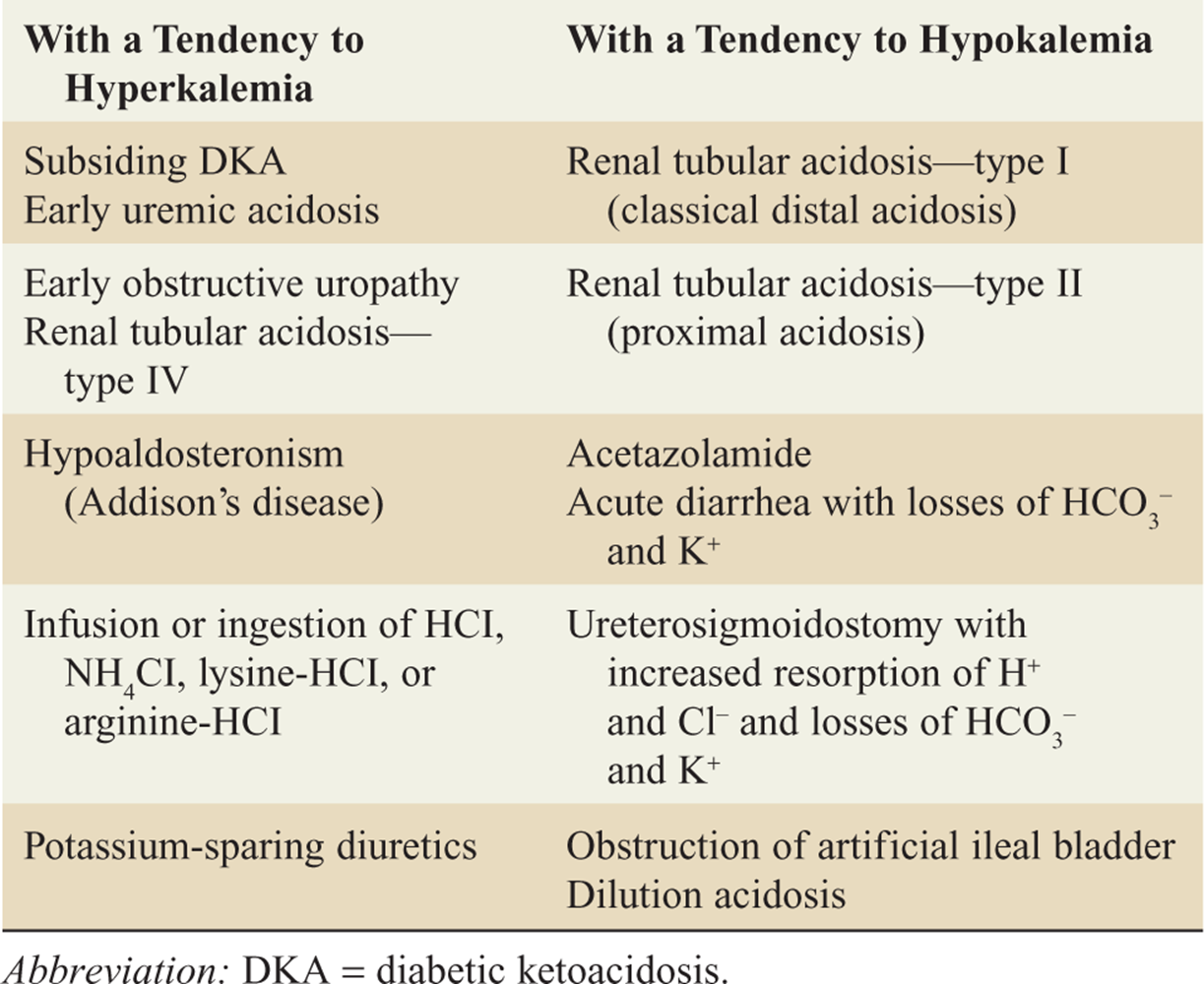
![]() A mnemonic that can aid recall the causes of NAMGA is USED CARP: ureterostomy, small bowel fistulas, extra chloride, diarrhea, carbonic anhydrase inhibitors, adrenal insufficiency, renal tubular acidosis, and pancreatic fistula.
A mnemonic that can aid recall the causes of NAMGA is USED CARP: ureterostomy, small bowel fistulas, extra chloride, diarrhea, carbonic anhydrase inhibitors, adrenal insufficiency, renal tubular acidosis, and pancreatic fistula.
TABLE 6-6 Causes of High Anion Gap Metabolic 1 Acidosis
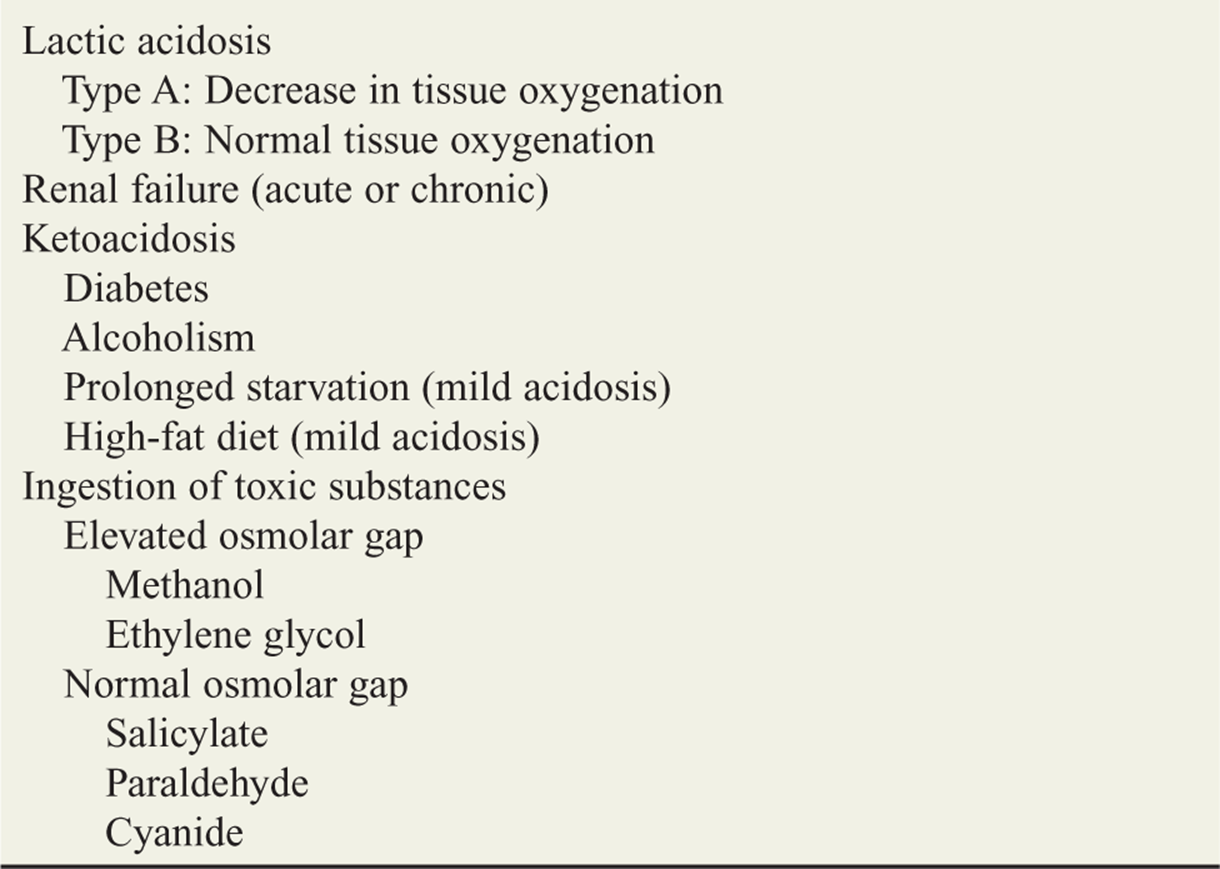
TABLE 6-7 Causes of Normal Anion Gap Metabolic Acidosis
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Supportive care is provided by improving perfusion through NS infusion, and improving oxygenation and ventilation.
Supportive care is provided by improving perfusion through NS infusion, and improving oxygenation and ventilation.
![]() Correct the underlying problem. For specific etiologies, consult the appropriate chapters in this handbook.
Correct the underlying problem. For specific etiologies, consult the appropriate chapters in this handbook.
![]() Indications for bicarbonate therapy are listed in Table 6-8.
Indications for bicarbonate therapy are listed in Table 6-8.
TABLE 6-8 Indications for Bicarbonate Therapy in Metabolic Acidosis

![]() Giving bicarbonate 0.5 mEq/kg for each mEq/L desired rise in [HCO3–] is recommended. The goal is to restore adequate buffer capacity ([HCO3–] >8 mEq/dL) or achieve clinical improvement in shock or dysrhythmias.
Giving bicarbonate 0.5 mEq/kg for each mEq/L desired rise in [HCO3–] is recommended. The goal is to restore adequate buffer capacity ([HCO3–] >8 mEq/dL) or achieve clinical improvement in shock or dysrhythmias.
![]() Bicarbonate should be given as slowly as the clinical situation permits; 75 mEq of 8.4% sodium bicarbonate in 500 mL D5W produces a nearly isotonic solution for infusion.
Bicarbonate should be given as slowly as the clinical situation permits; 75 mEq of 8.4% sodium bicarbonate in 500 mL D5W produces a nearly isotonic solution for infusion.
METABOLIC ALKALOSIS
![]() Metabolic alkalosis is classified as [Cl–] sensitive or [Cl–] insensitive.
Metabolic alkalosis is classified as [Cl–] sensitive or [Cl–] insensitive.
![]() The two most common causes of metabolic alkalosis are excessive diuresis (with loss of potassium, hydrogen ion, and chloride) and excessive loss of gastric secretions (with loss of hydrogen ion and chloride).
The two most common causes of metabolic alkalosis are excessive diuresis (with loss of potassium, hydrogen ion, and chloride) and excessive loss of gastric secretions (with loss of hydrogen ion and chloride).
CLINICAL FEATURES
![]() Symptoms of the underlying disorder (usually fluid loss) dominate the clinical presentation, but general symptoms of metabolic alkalosis include muscular irritability, tachydysrhythmias, and impaired oxygen delivery.
Symptoms of the underlying disorder (usually fluid loss) dominate the clinical presentation, but general symptoms of metabolic alkalosis include muscular irritability, tachydysrhythmias, and impaired oxygen delivery.
![]() In most cases, there is also an associated hypokalemia and hypochloremia.
In most cases, there is also an associated hypokalemia and hypochloremia.
DIAGNOSIS AND DIFFERENTIAL
![]() [Cl–]-sensitive causes present with hypovolemia secondary to vomiting, diarrhea, or diuretic therapy.
[Cl–]-sensitive causes present with hypovolemia secondary to vomiting, diarrhea, or diuretic therapy.
![]() [Cl–]-insensitive causes present with normo- to hyper-volemia associated with excess mineralocorticoid activity (renin-secreting tumors, adrenal hyperplasia, hyperaldosteronism, Cushing’s syndrome).
[Cl–]-insensitive causes present with normo- to hyper-volemia associated with excess mineralocorticoid activity (renin-secreting tumors, adrenal hyperplasia, hyperaldosteronism, Cushing’s syndrome).
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treat the underlying disorder.
Treat the underlying disorder.
![]() Administer NS to treat dehydration.
Administer NS to treat dehydration.
![]() Electrolytes should be carefully monitored.
Electrolytes should be carefully monitored.
![]() Potassium is administered as KCl and no faster than 20 mEq/h, unless serum potassium is above 5.0 mEq/L.
Potassium is administered as KCl and no faster than 20 mEq/h, unless serum potassium is above 5.0 mEq/L.
RESPIRATORY ACIDOSIS
CLINICAL FEATURES
![]() Respiratory acidosis secondary to hypoventilation may be life threatening.
Respiratory acidosis secondary to hypoventilation may be life threatening.
![]() Typically, respiratory acidosis depresses the mental function, which may progressively slow the respiratory rate. Patients may be confused, somnolent, and eventually unconscious.
Typically, respiratory acidosis depresses the mental function, which may progressively slow the respiratory rate. Patients may be confused, somnolent, and eventually unconscious.
![]() In some disorders, the fall in oxygen saturation may lag behind the elevation in PCO2. Pulse oximetry may be misleading, making ABGs essential for the diagnosis.
In some disorders, the fall in oxygen saturation may lag behind the elevation in PCO2. Pulse oximetry may be misleading, making ABGs essential for the diagnosis.
DIAGNOSIS AND DIFFERENTIAL
![]() The differential diagnosis includes drug overdose, CNS disease, chest wall disease, pleural or lung disease, and trauma.
The differential diagnosis includes drug overdose, CNS disease, chest wall disease, pleural or lung disease, and trauma.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Increase ventilation. Depressed mental status is an indication for intubation. An exception to this recommendation is in the event of opioid intoxication where rapid treatment with naloxone may improve ventilation.
Increase ventilation. Depressed mental status is an indication for intubation. An exception to this recommendation is in the event of opioid intoxication where rapid treatment with naloxone may improve ventilation.
![]() Treat the underlying disorder. High-flow oxygen therapy may lead to exacerbation of CO2 narcosis in patients with COPD and CO2 retention. Monitor these patients closely when administering oxygen and intubate if necessary.
Treat the underlying disorder. High-flow oxygen therapy may lead to exacerbation of CO2 narcosis in patients with COPD and CO2 retention. Monitor these patients closely when administering oxygen and intubate if necessary.
RESPIRATORY ALKALOSIS
CLINICAL FEATURES
![]() A number of life-threatening disorders present with tachypnea and anxiety: asthma, pulmonary embolism, DKA, and others.
A number of life-threatening disorders present with tachypnea and anxiety: asthma, pulmonary embolism, DKA, and others.
![]() Symptoms of respiratory alkalosis often are dominated by the primary disorder promoting the hyper-ventilation.
Symptoms of respiratory alkalosis often are dominated by the primary disorder promoting the hyper-ventilation.
![]() Hyperventilation by virtue of the reduction of PCO2, however, lowers both cerebral and peripheral blood flow, causing distinct symptoms.
Hyperventilation by virtue of the reduction of PCO2, however, lowers both cerebral and peripheral blood flow, causing distinct symptoms.
![]() Patients complain of dizziness, carpopedal spasm, and chest tightness or pain.
Patients complain of dizziness, carpopedal spasm, and chest tightness or pain.
DIAGNOSIS AND DIFFERENTIAL
![]() The diagnosis of hyperventilation due to anxiety is a diagnosis of exclusion. ABGs can be used to rule out acidosis and hypoxia.
The diagnosis of hyperventilation due to anxiety is a diagnosis of exclusion. ABGs can be used to rule out acidosis and hypoxia.
![]() Causes of respiratory alkalosis include CNS tumor or stroke, hypoxia, infection or fever, lung disease, hyperthyroidism, toxins (eg, sympathomimetic therapy, aspirin), liver disease, pregnancy, anemia, and anxiety.
Causes of respiratory alkalosis include CNS tumor or stroke, hypoxia, infection or fever, lung disease, hyperthyroidism, toxins (eg, sympathomimetic therapy, aspirin), liver disease, pregnancy, anemia, and anxiety.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Treat the underlying cause.
Treat the underlying cause.
![]() Only when more serious causes of hyperventilation are ruled out should the treatment of anxiety be considered. Anxiolytics may be helpful, such as lorazepam, 1–2 milligrams IV or PO.
Only when more serious causes of hyperventilation are ruled out should the treatment of anxiety be considered. Anxiolytics may be helpful, such as lorazepam, 1–2 milligrams IV or PO.
![]() Rebreathing into a paper bag can cause hypoxia and is not recommended.
Rebreathing into a paper bag can cause hypoxia and is not recommended.
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 19, “Acid-Base Disorders,” by David D. Nico-laou and Gabor D. Kelen; and Chapter 21, “Fluids and Electrolytes,” by Gabor D. Kelen and Edbert Hsu.