David M. Cline
![]() Malaria must be considered in any person who has traveled to the tropics (even months later) and presents with an unexplained febrile illness.
Malaria must be considered in any person who has traveled to the tropics (even months later) and presents with an unexplained febrile illness.
EPIDEMIOLOGY
![]() Five species of the protozoan Plasmodium infect humans: Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, Plasmodium malariae, and Plasmodium knowlesi.
Five species of the protozoan Plasmodium infect humans: Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, Plasmodium malariae, and Plasmodium knowlesi.
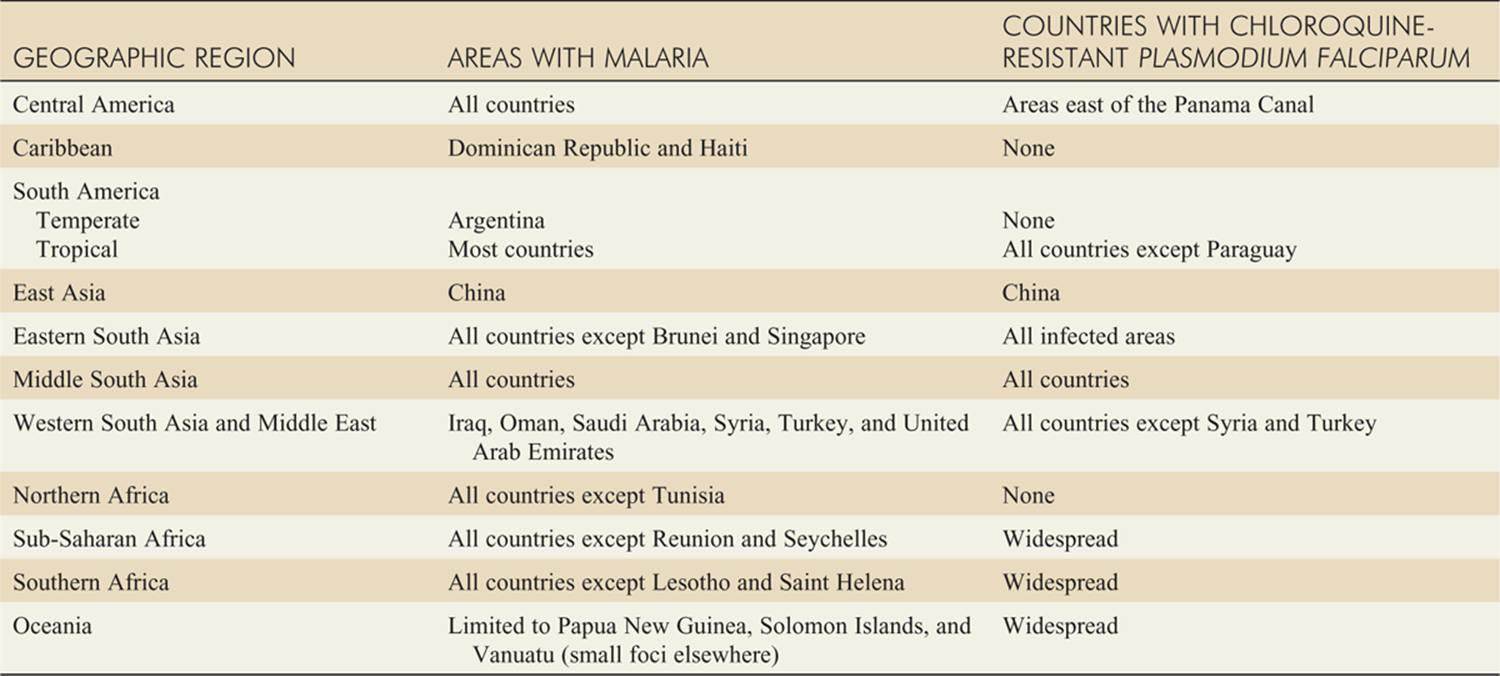
![]() Malaria transmission occurs in large areas of Central and South America, the Caribbean, sub-Saharan Africa, the Indian subcontinent, Southeast Asia, the Middle East, and Oceania (New Guinea, Solomon Islands, etc.). More than 50% of all US cases of malaria, including most cases due to P. falciparum, arise from travel to sub-Saharan Africa. Resistance of P. falciparum to chloroquine and other drugs continues to spread (see Table 97-1). Strains of P. vivaxwith chloroquine resistance have been identified. The Centers for Disease Control and Prevention (CDC) has a malaria hotline: 770–488–7788 M-F, 8 a.m. to 4:30 p.m. EST, and 770–488–7100 after-hours, weekends and holidays. Alternatively, the CDC Web site can be accessed at http://www.cdc.gov/malaria/ for information on resistance patterns in various countries and information on malaria prophylaxis and treatment. When in doubt, chloroquine resistance for initial treatment should be assumed.
Malaria transmission occurs in large areas of Central and South America, the Caribbean, sub-Saharan Africa, the Indian subcontinent, Southeast Asia, the Middle East, and Oceania (New Guinea, Solomon Islands, etc.). More than 50% of all US cases of malaria, including most cases due to P. falciparum, arise from travel to sub-Saharan Africa. Resistance of P. falciparum to chloroquine and other drugs continues to spread (see Table 97-1). Strains of P. vivaxwith chloroquine resistance have been identified. The Centers for Disease Control and Prevention (CDC) has a malaria hotline: 770–488–7788 M-F, 8 a.m. to 4:30 p.m. EST, and 770–488–7100 after-hours, weekends and holidays. Alternatively, the CDC Web site can be accessed at http://www.cdc.gov/malaria/ for information on resistance patterns in various countries and information on malaria prophylaxis and treatment. When in doubt, chloroquine resistance for initial treatment should be assumed.
PATHOPHYSIOLOGY
![]() Transmitted by blood transfusion or passed transpla-centally from mother to fetus.
Transmitted by blood transfusion or passed transpla-centally from mother to fetus.
![]() Plasmodial sporozoites are injected into a host’s bloodstream during the feeding of the female anophe-line mosquito, and travel directly to the liver where they invade hepatic parenchymal cells (exoerythro-cytic stage). In the liver the parasites undergo asexual reproduction, forming thousands of daughter mero-zoites, which after an incubation period of one to several weeks rupture their host hepatic cells and are released into the peripheral circulation.
Plasmodial sporozoites are injected into a host’s bloodstream during the feeding of the female anophe-line mosquito, and travel directly to the liver where they invade hepatic parenchymal cells (exoerythro-cytic stage). In the liver the parasites undergo asexual reproduction, forming thousands of daughter mero-zoites, which after an incubation period of one to several weeks rupture their host hepatic cells and are released into the peripheral circulation.
![]() The merozoites then rapidly invade circulating eryth-rocytes, where they mature and take on various morphologic forms—early ring forms, trophozoites, and schizonts, which are a mass of new merozoites (erythrocytic stage).
The merozoites then rapidly invade circulating eryth-rocytes, where they mature and take on various morphologic forms—early ring forms, trophozoites, and schizonts, which are a mass of new merozoites (erythrocytic stage).
![]() Eventually the target red blood cell (RBC) lyses, releasing the merozoites to invade additional erythro-cytes, continuing the infection. RBC lysis then often recurs at regular 2- to 3-day intervals, corresponding with the classic periodicity of symptoms. This cyclical feature may be absent in P. falciparum infection.
Eventually the target red blood cell (RBC) lyses, releasing the merozoites to invade additional erythro-cytes, continuing the infection. RBC lysis then often recurs at regular 2- to 3-day intervals, corresponding with the classic periodicity of symptoms. This cyclical feature may be absent in P. falciparum infection.
![]() With P. vivax or P. ovale infection, portions of the intrahepatic forms are not released, remain dormant for months, and can later activate, resulting in a clinical relapse.
With P. vivax or P. ovale infection, portions of the intrahepatic forms are not released, remain dormant for months, and can later activate, resulting in a clinical relapse.
![]() Plasmodium infection may also be acquired via transplacental transmission, via infected blood during transfusion, or by sharing of IV needles among drug abusers.
Plasmodium infection may also be acquired via transplacental transmission, via infected blood during transfusion, or by sharing of IV needles among drug abusers.
![]() The classic febrile paroxysm of malaria results from hemolysis of infected RBCs and the resulting release of antigenic agents that activate macrophages and produce cytokines.
The classic febrile paroxysm of malaria results from hemolysis of infected RBCs and the resulting release of antigenic agents that activate macrophages and produce cytokines.
![]() Infected RBCs lose their flexibility and thus are prone to cause congestion and obstruction of the capillary microcirculation of various organs, resulting in sequestration of blood in the spleen and anoxic injury to the lungs, kidneys, brain, and other vital organs.
Infected RBCs lose their flexibility and thus are prone to cause congestion and obstruction of the capillary microcirculation of various organs, resulting in sequestration of blood in the spleen and anoxic injury to the lungs, kidneys, brain, and other vital organs.
![]() Hemolysis is often high with P. falciparum infection because of its predilection for erythrocytes of all ages (while the other three Plasmodium species target young or old RBCs). RBC sequestration accounts for the paucity of observed mature parasites sometimes seen on the peripheral blood smear in P. falciparum infection.
Hemolysis is often high with P. falciparum infection because of its predilection for erythrocytes of all ages (while the other three Plasmodium species target young or old RBCs). RBC sequestration accounts for the paucity of observed mature parasites sometimes seen on the peripheral blood smear in P. falciparum infection.
![]() Immunologic sequelae such as glomerulonephritis, nephrotic syndrome, thrombocytopenia, and polyclo-nal antibody stimulation may occur. Hypersplenism with subsequent pancytopenia may occur, especially with prolonged untreated malaria.
Immunologic sequelae such as glomerulonephritis, nephrotic syndrome, thrombocytopenia, and polyclo-nal antibody stimulation may occur. Hypersplenism with subsequent pancytopenia may occur, especially with prolonged untreated malaria.
TABLE 97-1 Geographic Distribution of Malaria, Including Resistant Strains
CLINICAL FEATURES
![]() The incubation period ranges from 1 to 4 weeks. Partial chemoprophylaxis or incomplete immunity can prolong the incubation period to months or even years.
The incubation period ranges from 1 to 4 weeks. Partial chemoprophylaxis or incomplete immunity can prolong the incubation period to months or even years.
![]() Initially malaria manifests with nonspecific fever and malaise, and then progresses to chills and high-grade fevers; frequent symptoms include headache, myalgia, arthralgia, cough, abdominal pain, nausea, and diarrhea.
Initially malaria manifests with nonspecific fever and malaise, and then progresses to chills and high-grade fevers; frequent symptoms include headache, myalgia, arthralgia, cough, abdominal pain, nausea, and diarrhea.
![]() The patient may have tachycardia, orthostatic dizziness, and extreme weakness.
The patient may have tachycardia, orthostatic dizziness, and extreme weakness.
![]() Classically, cycles of fever and chills followed by profuse diaphoresis and exhaustion occur at regular intervals, reflecting hemolysis of infected erythrocytes.
Classically, cycles of fever and chills followed by profuse diaphoresis and exhaustion occur at regular intervals, reflecting hemolysis of infected erythrocytes.
![]() Physical examination findings are typically nonspecific. During a febrile paroxysm, most patients appear acutely ill, with high fever, tachycardia, and tachypnea.
Physical examination findings are typically nonspecific. During a febrile paroxysm, most patients appear acutely ill, with high fever, tachycardia, and tachypnea.
![]() Splenomegaly is common. In P. falciparum infections, hepatomegaly, edema, and icterus often occur.
Splenomegaly is common. In P. falciparum infections, hepatomegaly, edema, and icterus often occur.
![]() Laboratory features include normocytic normochro-mic anemia with evidence of hemolysis and thrombocytopenia. The white blood cell count is normal or low.
Laboratory features include normocytic normochro-mic anemia with evidence of hemolysis and thrombocytopenia. The white blood cell count is normal or low.
![]() Complications of malaria can occur rapidly, particularly with P. falciparum.
Complications of malaria can occur rapidly, particularly with P. falciparum.
![]() All forms cause hemolysis and splenomegaly, and splenic rupture may occur. Hypersplenism with subsequent pancytopenia may be seen in advanced cases.
All forms cause hemolysis and splenomegaly, and splenic rupture may occur. Hypersplenism with subsequent pancytopenia may be seen in advanced cases.
![]() Glomerulonephritis, most often in P. malariae infections, and nephrotic syndrome may occur.
Glomerulonephritis, most often in P. malariae infections, and nephrotic syndrome may occur.
![]() Cerebral malaria, characterized by somnolence, coma, delirium, and seizures, has a mortality rate greater than
Cerebral malaria, characterized by somnolence, coma, delirium, and seizures, has a mortality rate greater than
![]() Other life-threatening complications associated with P. falciparum include noncardiogenic pulmonary edema and metabolic abnormalities, including lactic acidosis and profound hypoglycemia.
Other life-threatening complications associated with P. falciparum include noncardiogenic pulmonary edema and metabolic abnormalities, including lactic acidosis and profound hypoglycemia.
![]() Blackwater fever is a severe complication seen almost exclusively in P. falciparum infections, with massive intravascular hemolysis, jaundice, hemoglobinuria (dark urine), and acute renal failure.
Blackwater fever is a severe complication seen almost exclusively in P. falciparum infections, with massive intravascular hemolysis, jaundice, hemoglobinuria (dark urine), and acute renal failure.
DIAGNOSIS AND DIFFERENTIAL
![]() The definitive diagnosis is established by identification of the parasite on Giemsa-stained thin and thick smears of peripheral blood.
The definitive diagnosis is established by identification of the parasite on Giemsa-stained thin and thick smears of peripheral blood.
![]() In early infection, especially with P. falciparum, parasitemia may be undetectable initially due to intraor-gan sequestration.
In early infection, especially with P. falciparum, parasitemia may be undetectable initially due to intraor-gan sequestration.
![]() Parasite load in the peripheral circulation fluctuates over time and is highest during an acute rising fever with chills.
Parasite load in the peripheral circulation fluctuates over time and is highest during an acute rising fever with chills.
![]() Therapy should not be withheld if malaria is suspected, even though the parasite is not detected on initial blood smears.
Therapy should not be withheld if malaria is suspected, even though the parasite is not detected on initial blood smears.
![]() If plasmodia are not visualized, repeated smears should be taken at least twice daily (preferably during febrile episodes) for 3 days to fully exclude malaria.
If plasmodia are not visualized, repeated smears should be taken at least twice daily (preferably during febrile episodes) for 3 days to fully exclude malaria.
![]() Once plasmodia are identified, the smear is also evaluated for the degree of parasitemia (percentage of red blood cells infected—which correlates with prognosis), and species type (in particular P. falciparum) is present.
Once plasmodia are identified, the smear is also evaluated for the degree of parasitemia (percentage of red blood cells infected—which correlates with prognosis), and species type (in particular P. falciparum) is present.
![]() Antigen-detecting rapid diagnostic tests are available in certain areas, and are recommended by the World Health Organization (WHO), provided quality control measures are in place.
Antigen-detecting rapid diagnostic tests are available in certain areas, and are recommended by the World Health Organization (WHO), provided quality control measures are in place.
![]() Further, the WHO recommends parasite-based diagnosis except for young children in areas of high transmission when testing availability is limited; in these situations, clinically based diagnoses and treatment are recommended, with monitoring for clinical improvement.
Further, the WHO recommends parasite-based diagnosis except for young children in areas of high transmission when testing availability is limited; in these situations, clinically based diagnoses and treatment are recommended, with monitoring for clinical improvement.
EMERGENCY DEPARTMENT CARE AND DISPOSITION
![]() Unless it is certain that a patient could not have a chloroquine-resistant case, based on history of geographic exposure, the infection must be assumed to be resistant and treated with one of the chloroquine-resistant regimens listed immediately below.
Unless it is certain that a patient could not have a chloroquine-resistant case, based on history of geographic exposure, the infection must be assumed to be resistant and treated with one of the chloroquine-resistant regimens listed immediately below.
![]() Patients with uncomplicated infection with chloroquine-resistant P. falciparum can be treated with one of several regimens.
Patients with uncomplicated infection with chloroquine-resistant P. falciparum can be treated with one of several regimens.
![]() Option 1 is artemether/lumefantrine, dose twice daily for 3 days, a total of six doses. For adults, 20 milligrams/120 milligrams tablets, 4 tablets initially, 4 tablets in 8 hours, then 4 tablets every 12 hours × 2 days. For children, 5 to 15 kg, one tablet initially, one tablet in 8 hours, then one tablet every 12 hours × 2 days; 15 to 25 kg, 2 tablets initially, 2 tablets in 8 hours, then 2 tablets every 12 hours × 2 days; 25 to 35 kg, 3 tablets initially, 3 tablets in 8 hours, then 3 tablets every 12 hours × 2 days; >35 kg, follow adult dosing.
Option 1 is artemether/lumefantrine, dose twice daily for 3 days, a total of six doses. For adults, 20 milligrams/120 milligrams tablets, 4 tablets initially, 4 tablets in 8 hours, then 4 tablets every 12 hours × 2 days. For children, 5 to 15 kg, one tablet initially, one tablet in 8 hours, then one tablet every 12 hours × 2 days; 15 to 25 kg, 2 tablets initially, 2 tablets in 8 hours, then 2 tablets every 12 hours × 2 days; 25 to 35 kg, 3 tablets initially, 3 tablets in 8 hours, then 3 tablets every 12 hours × 2 days; >35 kg, follow adult dosing.
![]() Option 2 is atovaquone-proguanil. For adults, give four adult strength (250 milligrams/100 milligrams) tablets daily × 3 days. For children >41 kg, give adult dose; 31 to 40 kg, three adult tablets × 3 days; 21 to 30 kg, two adult tablets × 3 days; 11 to 20 kg, one adult tablet × 3 days; 9 to 10 kg, three pediatric tablets × 3 days; 5 to 8 kg, two pediatric tablets × 3 days.
Option 2 is atovaquone-proguanil. For adults, give four adult strength (250 milligrams/100 milligrams) tablets daily × 3 days. For children >41 kg, give adult dose; 31 to 40 kg, three adult tablets × 3 days; 21 to 30 kg, two adult tablets × 3 days; 11 to 20 kg, one adult tablet × 3 days; 9 to 10 kg, three pediatric tablets × 3 days; 5 to 8 kg, two pediatric tablets × 3 days.
![]() Option 3 is quinine sulfate 542 milligrams base (= 650 milligrams salt) PO three times daily (10 milligrams salt/kg/dose maximum) for 3 to 7 days plus doxycycline 100 milligrams PO twice daily for 7 days. Options 1 and 2 are preferred for children.
Option 3 is quinine sulfate 542 milligrams base (= 650 milligrams salt) PO three times daily (10 milligrams salt/kg/dose maximum) for 3 to 7 days plus doxycycline 100 milligrams PO twice daily for 7 days. Options 1 and 2 are preferred for children.
![]() A final option is mefloquine plus doxycycline, but mefloquine has an increased frequency of neuropsychiatric reactions, making it the least favored choice.
A final option is mefloquine plus doxycycline, but mefloquine has an increased frequency of neuropsychiatric reactions, making it the least favored choice.
![]() If P. falciparum can be excluded (travelers returning from Central America west of the Panama Canal, Haiti, the Dominican Republic, and most of the Middle East), patients with adequate home care and oral hydration can be treated as outpatients with close follow-up, including repeated blood smears to assess treatment response.
If P. falciparum can be excluded (travelers returning from Central America west of the Panama Canal, Haiti, the Dominican Republic, and most of the Middle East), patients with adequate home care and oral hydration can be treated as outpatients with close follow-up, including repeated blood smears to assess treatment response.
![]() Recommended treatment for uncomplicated malaria infection due to P. vivax, P. ovale, P. malariae, and P. knowlesi is chloroquine plus primaquine phosphate.
Recommended treatment for uncomplicated malaria infection due to P. vivax, P. ovale, P. malariae, and P. knowlesi is chloroquine plus primaquine phosphate.
![]() For adults: chloroquine 600 milligrams base (= 1 gram salt), then 300 milligrams base (= 500 milligrams salt) in 6 hours, then 300 milligrams base per day for 2 days (total dose 1550 milligrams base), plus primaquine phosphate 30 milligrams base per day for 14 days on completion of chloroquine therapy.
For adults: chloroquine 600 milligrams base (= 1 gram salt), then 300 milligrams base (= 500 milligrams salt) in 6 hours, then 300 milligrams base per day for 2 days (total dose 1550 milligrams base), plus primaquine phosphate 30 milligrams base per day for 14 days on completion of chloroquine therapy.
![]() For children: chloroquine 10 milligrams/kg base to maximum of 600 milligrams load, then 5 milligrams/kg base in 6 hours and 5 milligrams/kg base per day for 2 days, plus primaquine phosphate 0.5 milligram/kg base for 14 days on completion of chloroquine therapy.
For children: chloroquine 10 milligrams/kg base to maximum of 600 milligrams load, then 5 milligrams/kg base in 6 hours and 5 milligrams/kg base per day for 2 days, plus primaquine phosphate 0.5 milligram/kg base for 14 days on completion of chloroquine therapy.
![]() Chloroquine has no effect on the exoerythrocytic forms of P. vivax and P. ovale, which remain dormant in the liver.
Chloroquine has no effect on the exoerythrocytic forms of P. vivax and P. ovale, which remain dormant in the liver.
![]() Unless treated with primaquine, relapse will occur. Primaquine should be avoided in patients with glu-cose-6-phosphate dehydrogenase deficiency because of hemolysis.
Unless treated with primaquine, relapse will occur. Primaquine should be avoided in patients with glu-cose-6-phosphate dehydrogenase deficiency because of hemolysis.
![]() Patients with significant hemolysis or with comorbid conditions that can be aggravated by high fevers or hemolysis are best hospitalized, as are infants and pregnant women.
Patients with significant hemolysis or with comorbid conditions that can be aggravated by high fevers or hemolysis are best hospitalized, as are infants and pregnant women.
![]() Plasmodium falciparum infections are best managed in the hospital, as are patients with more than 3% parasitemia (typical in the USA and developed countries).
Plasmodium falciparum infections are best managed in the hospital, as are patients with more than 3% parasitemia (typical in the USA and developed countries).
![]() Patients with complications due to P. falciparum or with high parasitemia but unable to tolerate oral medication should receive intravenous treatment.
Patients with complications due to P. falciparum or with high parasitemia but unable to tolerate oral medication should receive intravenous treatment.
![]() For severe malaria, with chloroquine-resistant P. falciparum, there are two recommended treatments.
For severe malaria, with chloroquine-resistant P. falciparum, there are two recommended treatments.
![]() Option 1 is quinidine, 6.25 milligrams base (=10 milligrams salt)/kg IV load over 2 hours (maximum, 600 milligrams), then 0.0125 milligram base (= 0.02 milligram salt)/kg/min continuous infusion until patient is stabilized and able to tolerate PO therapy (see above). Parenteral quinidine and quinine can cause severe hypoglycemia. They are also myocardial depressants and are contraindicated in patients with heart disease. Cardiac monitoring is required during administration.
Option 1 is quinidine, 6.25 milligrams base (=10 milligrams salt)/kg IV load over 2 hours (maximum, 600 milligrams), then 0.0125 milligram base (= 0.02 milligram salt)/kg/min continuous infusion until patient is stabilized and able to tolerate PO therapy (see above). Parenteral quinidine and quinine can cause severe hypoglycemia. They are also myocardial depressants and are contraindicated in patients with heart disease. Cardiac monitoring is required during administration.
![]() Option 2 is artesunate, which is available from the CDC quarantine station, follow artesunate with atovaquone-proguanil plus doxycycline as above. The dose of artesunate is 2.4 milligrams/kg IV at 0, 12, and 24 hours, and then 2.4 milligrams/kg once daily for 3 days.
Option 2 is artesunate, which is available from the CDC quarantine station, follow artesunate with atovaquone-proguanil plus doxycycline as above. The dose of artesunate is 2.4 milligrams/kg IV at 0, 12, and 24 hours, and then 2.4 milligrams/kg once daily for 3 days.
![]() Aggressive supportive care should be provided to all hospitalized ill patients, including judicious fluid replacement, correction of metabolic derangements, and advanced support (dialysis, mechanical ventilation, etc.).
Aggressive supportive care should be provided to all hospitalized ill patients, including judicious fluid replacement, correction of metabolic derangements, and advanced support (dialysis, mechanical ventilation, etc.).
For further reading in Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 7th ed., see Chapter 153, “Malaria,” by John J. Szela, Josiah J. Tayali, and Jeffrey D. Band.