473. The answer is e. (Aminoff, p 725.) Without rapid replacement of thiamine stores, the patient with acute Wernicke encephalopathy may die. Usually 50-to-100 mg of thiamine is given intravenously immediately. This is followed over the course of a few days with supplementary thiamine injections of 50-to-100 mg. Without thiamine, the patient will develop periaqueductal and mamillary body lesions, which will be clinically apparent as autonomic failure. With chronic thiamine deficiency, neuronal loss occurs in alcoholic persons at least partly because of this relative vitamin deficiency. Purkinje and other cells in the cerebellar vermis will be lost to so dramatic an extent that gross atrophy of the superior cerebellar vermis will be evident.
474. The answer is c. (Aminoff, pp 1140-1141.) Botulism is a disorder of the neuromuscular junction (NMJ). The characteristic findings are decremental response of the muscles to repetitive stimulation of the nerve at a low frequency (2-5 Hz) and incremental response to repetitive stimulation at high frequency (20-50 Hz). Other disorders of the NMJ, such as myasthenia gravis and Lambert-Eaton myasthenic syndrome (LEMS), also manifest with decremental response to repetitive stimulation at low frequencies due to depletion of acetylcholine in the synaptic cleft. Higher rates of stimulation lead to increased calcium in the presynaptic terminal, which allows more acetylcholine to be released in presynaptic disorders such as botulism and LEMS, thereby increasing the response of muscle. However, in myasthenia gravis, which is characterized by loss of acetylcholine receptors postsynaptically, there is no increase in response at higher rates of stimulation, because there is already a maximal amount of acetylcholine present in the synaptic cleft. Abnormal visual evoked and brainstem auditory evoked potentials would be seen in disorders affecting central pathways, such as MS. Conduction block occurs in demyelinating disorders affecting the nerves. Fibrillation potentials are present in denervation and certain myopathic conditions; they may occur in botulism, as well as in patients treated with botulinum toxin for therapeutic purposes, but this is not diagnostic of clinical botulism.
475. The answer is e. (Swaiman, pp 1577, 1582.) Between birth and 1 year of age, what appears to be a simple febrile seizure may actually be a seizure provoked by a bacterial meningitis. The agents most likely to be responsible in a 6-month-old child are Haemophilus influenzae, Streptococcus pneumoniae, and Neisseria meningitidis. Since the introduction of vaccination against H influenzae, however, the incidence of meningitis due to this organism has been drastically reduced. Below 3 months of age, group B streptococci, Escherichia coli, and Listeria monocytogene must also be considered. All require rapid diagnosis and early treatment if the child is to survive. Even though the child may not have substantial neck stiffness, the CSF will typically reveal glucose content less than two-thirds the serum level, elevated white blood cell count, and increased protein content. The responsible organism may be isolated and cultured, but treatment of the meningitis should begin before the organism is identified. A delay of hours in treatment may be lethal. Intravenous antibiotics should be started as soon as there is convincing evidence that febrile seizures are secondary to a bacterial meningitis. The drug chosen should be the one most effective against the most probable organism. The child’s age, exposure, and symptomatology must all be considered in deciding what organism is most likely responsible for the infection.
476. The answer is a. (Ropper, pp 896-900.) Acute disseminated encephalomyelitis is a demyelinating disease of the brain, brainstem, and spinal cord that is indistinguishable from MS on MRI. It is, however, monophasic, meaning that it occurs acutely on a single occasion and not in a recurrent fashion like MS. It usually develops within days or weeks of a viral illness or an immunization. Childhood exanthems are especially likely to precipitate ADEM, as are smallpox and rabies immunizations. As in MS, the lesions associated with ADEM usually produce perivenous demyelination with sparing of the nerve axons.
477. The answer is c. (Ropper, pp 199-200.) Surgery may eventually be necessary with any intervertebral disk herniation, but with acute, massive cauda equina injury, surgery must be performed before the deficits are irreversible. Signs of cauda equina compression include loss of bladder and bowel control and paraparesis or paraplegia. An acutely evolving focal motor deficit in the legs, such as a footdrop, associated with sphincter dysfunction is justification for emergency laminectomy and disk resection. Pre-operative studies should be obtained to be sure that the responsible lesion is disk herniation, because metastatic cancers, such as prostate and breast carcinoma, may imitate acute disk herniations. Establishing the identity of the lesion is important because many tumors are better managed with high-dose corticosteroids and radiation therapy than with surgery. Osteomyelitis of the vertebral body may also produce cauda equina compression; a decompressive laminectomy is usually indicated with focal infections of this sort to maximize the recovery achieved with antibiotic therapy.
478. The answer is a. (Ropper, p 176.) Oxygen may terminate a cluster headache within minutes. Some physicians recommend inhaling 4 L/minute of 100% oxygen by mask as soon as signs of an impending headache develop. This has prompted many sufferers of cluster headaches to keep a cylinder of compressed oxygen at home during the season when they are most likely to develop such headaches. Cluster headaches usually occur at night when the patient is asleep, and so practical access to the oxygen tank is possible. Methysergide is effective in preventing cluster headaches for many persons, but it does rarely cause the worrisome adverse effect of fibrosis. Retroperitoneal, pulmonary, and endocardial fibroses are potential adverse effects of methysergide. Sublingual nitroglycerin may in fact trigger a headache and is not recommended for patients with migraine or cluster headaches. Propranolol is a β-adrenergic–blocking agent that is useful in the prophylaxis of some vascular headaches, but it is of no value in aborting a cluster headache. Dihydroergotamine suppositories may abort some vascular headaches, but they do not have as obvious an effect in cluster as in classic or common migraine syndromes.
479. The answer is c. (Aminoff, p 725.) Wernicke encephalopathy is a potentially fatal consequence of thiamine deficiency, a problem for which this woman was at risk by virtue of being an alcoholic. When she came to the emergency room, intravenous fluids were started that probably contained glucose. The stress of a large glucose load will abruptly deplete the central nervous system (CNS) of the little thiamine it has available and will precipitate the sort of deterioration evident in this woman. Features characteristic of a Wernicke encephalopathy include deteriorating level of consciousness, autonomic disturbances, ocular motor problems, and gait difficulty. Autonomic disturbances may include lethal hypotension or profound hypothermia. Hemorrhagic necrosis in periventricular gray matter will be evident in this woman’s brain if she dies. The mamillary bodies are especially likely to be extensively damaged.
480. The answer is d. (Ropper, pp 1155-1156.) Malignant hyperthermia is characterized by acute severe fever, tachypnea, tachycardia, and rigidity, and high mortality rate if left untreated. It is typically precipitated by volatile anesthetics, especially halothane, or muscle relaxants such as succinylcholine. Patients may become severely acidotic and develop rhabdomyolysis. Pathology shows diffuse segmental muscle necrosis. It appears to be a metabolic myopathy in which there is abnormal release of calcium from the sarcoplasmic reticulum and ineffectual uptake afterward. Genetic defects in the ryanodine receptor, involved in calcium flux in the sarcoplasmic reticulum, are responsible for about 10% of cases, although as yet unidentified abnormalities of this or related proteins probably play a role in most cases. It is inherited in an autosomal dominant fashion. Certain other myopathies, including Duchenne muscular dystrophy and central core myopathy, are associated with this condition as well. Treatment consists of discontinuation of anesthesia, administration of dantrolene, which prevents release of calcium from the sarcoplasmic reticulum, and supportive measures.
481. The answer is b. (Ropper, p 1278.) The third cranial nerve (the oculomotor nerve) controls several movements of the globe, including upward and medial movements, through its control of the medial rectus, superior rectus, and inferior oblique muscles. Its inactivity leads to displacement of the eye down and out. Fourth-nerve palsy leads to weakness of the superior oblique muscle, with resultant difficulty looking down and medially; patients often complain of trouble walking down stairs. Sixth-nerve palsy produces weakness of the lateral rectus muscle, causing horizontal diplopia. Fractures of the orbit can entrap individual muscles, but there is no history of this here. Thyroid ophthalmopathy, or Graves disease, can produce diplopia, but there is usually proptosis or lid retraction. The inferior and medial recti are most frequently affected. Because this is caused by infiltration of the muscles, there is usually limitation of passive movement of the eyes (ie, forced ductions). Diabetes is a common cause of third-nerve palsy (approximately 10% of cases). Usually, when diabetes is the cause, there is sparing of the pupillomotor parasympathetic fibers, which travel on the outside of the nerve. Diabetes causes third-nerve palsy via nerve infarction, which affects the interior of the nerve but spares the external fibers. Compressive lesions, however, can injure the surface fibers, thereby causing pupillary dilation due to unopposed sympathetic activity.
482. The answer is e. (Ropper, pp 518-519.) Sympathetic innervation of the iris is required for the change in the color of the iris to occur after birth and infancy. Congenital Horner syndrome, which may be inherited as an autosomal dominant trait, is characterized by failure of one eye to develop normal iris color (heterochromia iridis). Any injury to the eye after this early developmental period would not be expected to leave a difference in eye color from one side to the other.
483. The answer is d. (Ropper, p 352.) The GCS was introduced in 1974 by Teasdale and Jennett. It has three parts: best motor response (1-6 points), best verbal response (1-5 points), and eye opening (1-4 points). The total score ranges from 3 to 15 (normal). The presence of coma is defined as GCS of 8 or less, which represents a patient who does not follow commands, speak, or open the eyes. Head injuries may be defined on the basis of the GCS: mild injury (GCS 14-15), moderate injury (GCS 9-13), and severe injury (GCS ≤ 8). Although patients with mild head injuries may receive a score of 15, the maximum on the GCS, they may still have more subtle cognitive difficulties that are not reflected by this easy-to-use and simple scale.
484. The answer is e. (Ropper, pp 847-849.) The presence of periorbital ecchymosis (raccoon eyes), ecchymosis over the mastoid region (Battle sign), hemotympanum (blood behind the eardrum), or CSF rhinorrhea or otorrhea should be considered evidence of a basilar skull fracture.
485. The answer is a. (Ropper, pp 850-851.) Diffuse axonal injury is the most common cause of coma in the head-injured patient without an intracranial mass lesion. It is characterized pathologically by diffusely spread axonal swellings affecting the white matter, corpus callosum, and upper brainstem. These foci are usually hemorrhagic. The etiology is thought to be due to shearing forces on axons in certain susceptible regions of the brain, notably those that are particularly vulnerable to rotational forces, such as the subcortical white matter, corpus callosum, and upper brainstem. Uncontrolled hypertension may occur in patients with hypertension, but would be unlikely to produce this pattern of injury. Amyloid angiopathy causes multiple hemorrhages, but affects elderly patients. The decreased cerebral perfusion pressure associated with brain swelling and increased intracranial pressure could cause ischemic infarction, but this would not be expected to give this appearance on MRI. Coagulopathies also occur in up to 20% of patients.
486. The answer is d. (Ropper, p 869.) Hypothermia has been shown to reduce cerebral injury from ischemia both in experimental models and in clinical studies of patients with traumatic brain injury. Hypothermia decreases cerebral metabolism, reduces acidosis, attenuates changes in the blood–brain barrier, and inhibits the release of excitatory neurotransmitters that can be harmful. Hypothermia may be achieved by packing the body in ice or using intravenous cooling systems. Corticosteroids, prophylactic hyperventilation, and prophylactic anticonvulsants have not been shown to be of benefit in the long-term prognosis of severely head-injured patients. Hyperthermia is detrimental to such patients.
487. The answer is d. (Ropper, pp 1162-63.) The rapid onset of bulbar paresis is consistent with acute inflammatory demyelinating polyneuropathy (AIDP, or Guillain-Barré syndrome), botulism, tick paralysis, and several other conditions. The normal conduction velocities argue against demyelinating neuropathy, which may be associated with C jejuni. Cytomegalovirus and T pallidum may cause several different neurological syndromes, but acute bulbar paresis is not among them. C pneumoniae is under investigation as a cause of atherosclerosis, strokes, and MS, but it does not cause acute motor weakness.
488. The answer is e. (Aminoff, pp 771-772.) The presentation suggests a viral encephalitis. Herpes simplex is the most common cause of viral encephalitis. The diagnosis of herpes encephalitis is more controversial than the treatment. A few authorities believe brain biopsy should be performed whenever the diagnosis is suspected, but the availability of polymerase chain reaction for herpes simplex virus in the CSF and MRI have made diagnosis easier. A high index of suspicion must be maintained, and treatment must be initiated quickly. Acyclovir must be given intravenously for at least 14-to-21 days.
489. The answer is d. (Ropper, pp 1162-63.) Botulinum toxin, a 150-kDa polypeptide chain, is cleaved into two chains: a 100-kDa chain required for neuronal binding and a 50-kDa chain that destroys important proteins required for neurotransmitter packaging. The toxin reduces the amount of acetylcholine available for release when a motor neuron is depolarized. Eight serotypes of botulism toxin are now recognized: A, B, C1, C2, D, E, F, and G. Although the toxins cleave different proteins, they interfere with the same step in vesicle formation.
490. The answer is b. (Ropper, pp 893-894.) Clinical trials have shown that intravenous methylprednisolone for an attack of optic neuritis is associated with a better outcome than oral prednisone. Intravenous methylprednisolone is thus recommended by most experts as appropriate therapy for acute exacerbations of MS involving more than sensory manifestations alone.
491. The answer is e. (Ropper, pp 893-894.) The risk of developing MS after optic neuritis was 74% in women and 34% in men after 15 years of follow-up in one study. Other studies have found similarly high rates. The longer the follow-up period, and the more rigorously signs of MS are sought, the more likely it is that MS will be found. Most patients develop MS within 5 years of the initial attack of optic neuritis. MRI scanning of the brain at the time of optic neuritis is, in fact, abnormal in between 50% and 72% of patients, suggesting the presence of subclinical MS.
492. The answer is d. (Ropper, pp 182-183.) This man has exhibited two different episodes separated in time and space, a clinical pattern that must raise the possibility of MS in a man this age. The pattern of pain is suggestive of trigeminal neuralgia (tic douloureux), a facial pain syndrome that often develops in persons with MS. Alternatives to carbamazepine in the palliation of trigeminal neuralgia include phenytoin and baclofen.
493. The answer is a. (Ropper, p 525.) Bladder dysfunction with MS is usually a consequence of corticospinal tract disease. This lesion of the upper motor neuron produces a spastic bladder. Tricyclic antidepressants such as imipramine exert an anticholinergic effect and thereby inhibit premature emptying of the bladder have been used. Oxybutynin also works through anticholinergic mechanisms. Cholinergic drugs, such as methacholine, are useful if the patient has a flaccid bladder, but that is much less frequently the problem with MS.
494. The answer is d. (Ropper, p 53.) Baclofen affects spasticity through an unknown mechanism and may cause considerable sedation. Sedation is less a concern if spasticity is interfering with the patient’s ability to sleep. The drug is usually given orally at a dose of 10 mg three or four times daily, but most patients must start at a much lower dose and gradually build up tolerance. Baclofen has been given intrathecally with an implanted pump injector, but this highly invasive therapy is appropriate only in patients with extreme spasticity. Candidates for intrathecal treatment are functionally paraplegic and may recover considerable mobility with elimination of the spasticity. Tizanidine is a centrally active α2-adrenergic agonist that appears to relieve spasticity without affecting strength.
495. The answer is b. (Ropper, pp 332-334.) There are several different options in initiating the treatment of status epilepticus. Some clinicians recommend intravenous diazepam as the initial medication, but this has a short-lived effect. Lorazepam is equally effective and has a more persistent effect. Phenytoin should be used in conjunction with a benzodiazepine to prevent relapse after the benzodiazepine’s effect abates, but it must be administered parenterally in the setting of status epilepticus in order to achieve rapid therapeutic levels. Although phenytoin cannot be given at more than 50 mg/minute because of the risk of cardiac depression associated with more rapid infusion rates, the more recently available fosphenytoin can be administered intramuscularly or intravenously at rates up to 150 mg/minute. Carbamazepine and gabapentin are not available as intravenous medications, and their absorption from the gastrointestinal tract is unacceptably slow for the treatment of status epilepticus. Intracranial pressure (ICP) will usually be increased during status epilepticus, but that is of no immediate clinical consequence, and monitoring of the ICP in status epilepticus is inappropriate in the absence of a specific indication such as documented head trauma or other mass lesion. ICP is routinely monitored by neurosurgeons in cases of severe head trauma to provide early warning of catastrophic changes within the head.
496. The answer is d. (Ropper, pp 332-334.) Urinary incontinence is an expected consequence of status epilepticus and consequently should not arouse concern for abdominal or urologic disturbances. Keeping the patient dry is important because of the risk of skin breakdown with any comatose patient, but mechanical intervention is sufficient. An indwelling catheter is unnecessary and introduces the risk of urinary tract infection. A condom catheter will keep the patient dry, allow urine to be collected, and enable the staff to more rigorously monitor fluid output. The urine is likely to be darkened by myoglobin, a pigment that collects in the urine when muscle breaks down after protracted seizure activity.
497. The answer is c. (Ropper, pp 807-808.) An expanding intracranial mass will produce an elevated blood pressure and a slow heart rate. This is called the Cushing response. This man may have a neoplasm in the brain or amyloid bleed. The site of the hemorrhage is unlikely with chronic hypertension or aneurysm. A biopsy of the mass would help identify the underlying lesion, although it is not urgent. Metastatic neoplastic disease is a possibility but is less likely than a glioblastoma multiforme at this age. The administration of TPA is contraindicated because this drug will increase the risk of rebleeding. Placement of a drain is not suggested by the clinical picture because there was no evidence of obstruction to the flow of CSF.
498. The answer is a. (Ropper, pp 622-625.) There are several different grading schemes for astrocytoma, but Kernohan’s classification of grades from I (least malignant) to IV (most malignant) is the one most widely used. Glioblastoma multiforme is an older term for the grade IV astrocytoma and is still in general use. This is a highly malignant tumor that develops most often in the cerebral hemispheres. The most malignant tumors usually exhibit areas of necrosis and have a poor prognosis. Survival with glioblastoma multiforme is usually measured in months rather than years. Treatment generally consists of gross total resection and radiation therapy. Survival may be increased to 40 weeks after this combination of therapies, whereas it is on average only 14 weeks after surgery alone. The intravenous medications listed are antineoplastic agents, but they are not effective against this type of tumor. Some chemotherapy has been generally regarded as useful for this type of primary brain tumor including 1,3-bis (2-chloroethyl)-1-nitrosourea (BCNU), which increases survival only marginally.
499. The answer is a. (Ropper, p 19.) The head CT scan is the mainstay of emergency department diagnosis of acute stroke. It is crucial to exclude intracranial hemorrhage prior to the potential administration of intravenous thrombolytic agents. A cerebral angiogram may play a role in the management of the acute stroke patient, particularly if there is evidence of cerebral or subarachnoid hemorrhage, or if there exists a possibility of performing intra-arterial thrombolysis, but CT scan is required first. In some centers, an MRI of the brain may be obtained nearly as quickly as a head CT and may be an alternative option. In the absence of evidence of trauma at the time of the patient’s fall, C-spine MRI and skull x-rays play no role in management.
500. The answer is a. (Ropper, pp 781-783.) In a large, multicenter randomized trial sponsored by the National Institutes of Health, thrombolytic therapy with intravenous rTPA has been shown to be of benefit to patients with acute ischemic stroke who can be treated early enough. The study demonstrated a statistically significant benefit for the use of rTPA in the treatment of ischemic stroke patients, who can be treated within 3 hours of symptom onset. A total of 624 patients arriving at the hospital within 3 hours of symptom onset underwent CT scan to exclude hemorrhagic stroke. Patients were randomized to receive either 0.9 mg/kg of rTPA or placebo. At 3 months, treated patients were at least 30% more likely to have minimal or no disability on several disability scales. Even with a symptomatic hemorrhage rate of 6.4% within 36 hours among the active treatment patients, the mortality and disability among treated patients was less than that among placebo patients at 3 months. The overall acute neurological deterioration even after accounting for early hemorrhages was the same in treated and placebo patients, indicating that the increased risk of hemorrhage with rTPA therapy is offset by an increased risk of neurological deterioration from progressing stroke, cerebral edema, and other causes in nontreated patients. The benefit of rTPA was not limited to patients with cardioembolic or large-vessel strokes, but also benefited patients with small-vessel strokes, who had a better prognosis.
Appendix: Neuroanatomy Reference Figures

Figure A-1. Cranial and spinal nerves.
(Used, with permission, from JS White. USMLE Road Map: Neuroscience. 2nd ed. New York, NY: McGraw-Hill; 2008.)

Figure A-2. Schematic diagram of the spinal cord. S, sacral; L, lumbar; Th, thoracic; C, cervical
(Modified, with permission, from JH Martin. Neuroanatomy: Text and Atlas. 3rd ed. New York, NY: McGraw-Hill; 2003.)
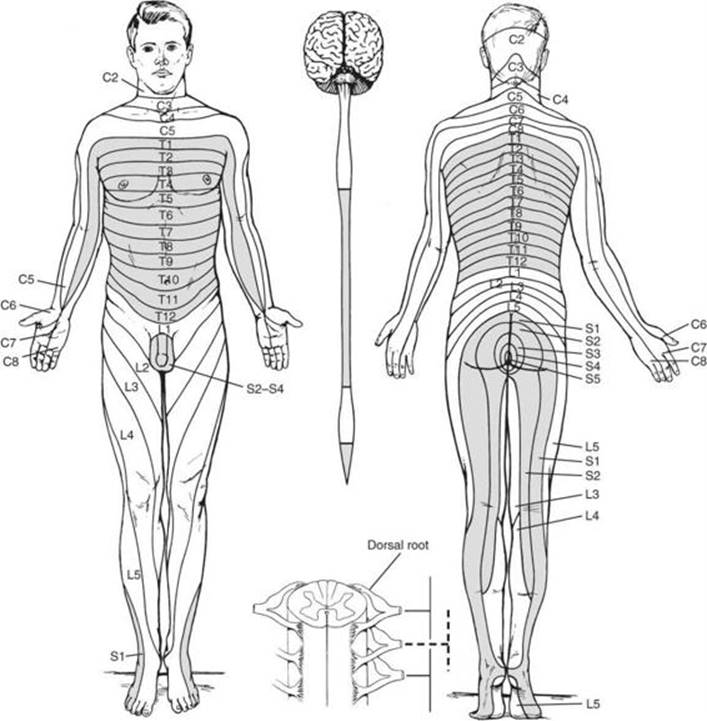
Figure A-3. The dermatomes of the body have a segmental organization. Note the correspondence between the spinal cord divisions (shown on a ventral view of the central nervous system) and dermatome locations. The inset illustrates dermatomal overlap.
(Used, with permission, from JH Martin. Neuroanatomy: Text and Atlas. 3rd ed. New York, NY: McGraw-Hill; 2003.)


Figure A-4. Functional anatomy of the cerebral cortex.
(Used, with permission, from JS White. USMLE Road Map: Neuroscience. 2nd ed. New York, NY: McGraw-Hill; 2008.)

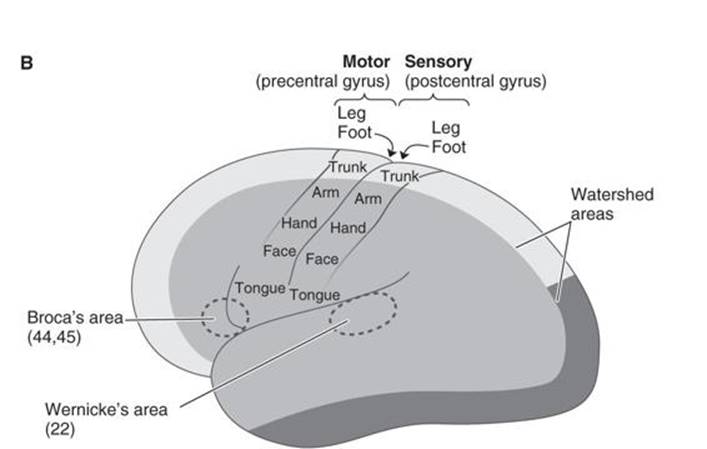
Figure A-5. (A) Coronal and (B) lateral views of the hemisphere showing the regions served by the anterior, middle, and posterior cerebral arteries.
(Used, with permission, from JS White. USMLE Road Map: Neuroscience. 2nd ed. New York, NY: McGraw-Hill; 2008.)


Figure A-6. A: Visual pathways.


Figure A-6. B: Laminae of the lateral geniculate body. C: Common visual field deficits.
(Used, with permission, from JS White. USMLE Road Map: Neuroscience. 2nd ed. New York, NY: McGraw-Hill; 2008.)

Figure A-7. Lateral corticospinal tract. The lateral corticospinal tract originates from neurons located in area 6 and the parietal lobe.
(Used, with permission, from JH Martin. Neuroanatomy: Text and Atlas. 3rd ed. New York, NY: McGraw-Hill; 2003.)

Figure A-8. Organization of the auditory system revealed in cross section of different levels through the brain stem and in coronal section through the diencephalon and cerebral hemispheres.
(Used, with permission, from JH Martin. Neuroanatomy: Text and Atlas. 3rd ed. New York, NY: McGraw-Hill; 2003.)

Figure A-9. Arterial supply at the brain and rostral spinal cord.
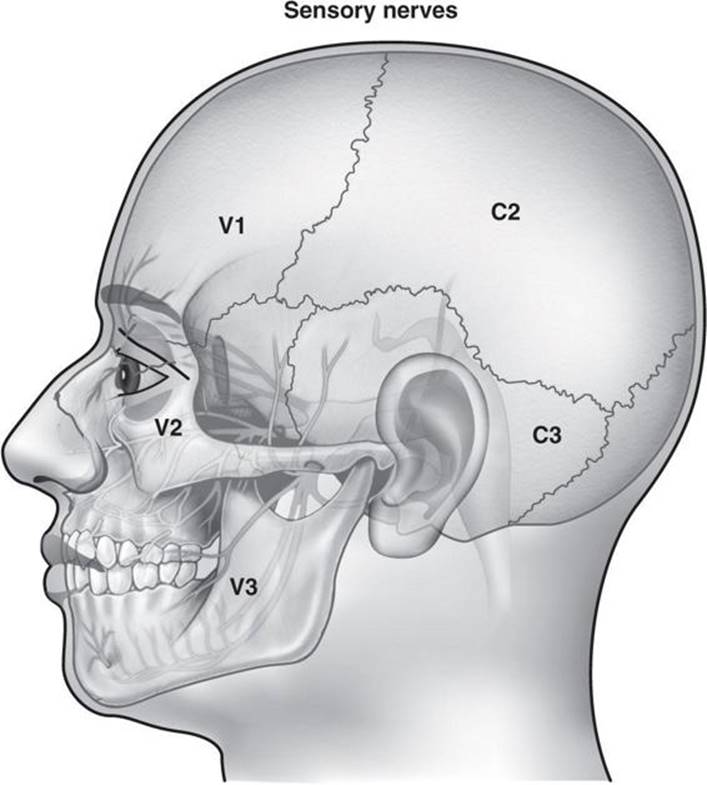
Figure A-10. Sensory innervation of the head. Middle and anterior fossa meninges are innervated by V1. Posterior fossa meninges are innervated by C2.

Figure A-11. Drawing of right eye indicating innervation and action of each of the muscles of extraocular movement.
(Modified, with permission, from Morton DA, Foreman KB, Albertine KH. The Big Picture: Gross Anatomy. New York: McGraw-Hill, 2011.)

Figure A-12. Brachial plexus. L, lateral; P, posterior; M, medial; s, superior; m, middle; i, inferior.

Figure A-13. Thalamic nuclei and their inputs. VA, ventral anterior nucleus; VL, ventral lateral nucleus; VP, ventral posterior nuclei (L, Lateral portion of VP; M, Medial portion of VP); Pulv, pulvinar nucleus; MD, medial dorsal nucleus (M, Medial nucleus); A, Anterior nuclei; LP, Lateral posterior nucleus.