I. DEVELOPMENTAL DISORDERS
Developmental disorders occasionally cause pain or progressive neurologic dysfunction in adults. Others are found incidentally.
A. Chiari’s malformations are characterized by descent of the cerebellar tonsils by 5 mm beyond the foramen magnum, with downward displacement of the medulla and kinking of the cervical spinal cord. Hydrocephalus, bony abnormalities of the skull base, and syringomyelia in the cervical cord are frequently found. Chiari I malformations (not associated with meningomyelocele) frequently do not manifest themselves until adulthood. Approximately 80% of patients will have syringomyelia.
1. No treatment is warranted if the patient has no symptoms. Cranial nerve signs, a history of sleep apnea, and radiologic evidence of syringomyelia should be sought. Neurologic and radiologic follow-up evaluation is warranted, especially for children and young adults.
2. If the patient has symptoms, decompressive suboccipital craniectomy and upper cervical laminectomy with or without ventricular shunting are required. However, patients may be stratified to a more or less aggressive surgical approach, based on structural features of the cisterna magna, extent of tonsillar descent, presence of a syrinx, and intraoperative ultrasound findings.
a. Respiratory depression is the most common postoperative complication necessitating close monitoring.
b. Approximately 50% of patients benefit, 25% have no change, and 25% deteriorate.
B. Spina bifida occulta is the anomalous development of the posterior neural arch without an extraspinal cyst. The condition is found in 5% of the population. Cutaneous anomalies often overlie the bony defect. Evidence of other lumbosacral anomalies may be found by means of ultrasonography in infants younger than 3 months or by means of MRI in older patients. Dermal sinus tracts can cause recurrent meningitis. Lipomas and dermoids can impinge on the cord or the cauda equina.
1. Dermal sinus tracts are closed to prevent meningitis.
2. Biopsy is indicated for tissue diagnosis of mass lesions.
3. Surgery is indicated for progressive deficits.
C. Tethering of the cord by adhesions, lipomas, or a tight filum terminale is the most common finding associated with spina bifida occulta. The syndrome often manifests itself after growth spurts or minor trauma. Pain can be the predominant presentation in adults, whereas scoliosis is more common in children. Bladder and bowel symptoms are common in both.
1. Surgery is controversial in the care of children who have no symptoms. Arguments for early prophylactic surgery are strong because symptoms stabilize but rarely are relieved after surgery. Patients should undergo electromyography (EMG) and urodynamic evaluations before a final decision is made.
2. Surgical release stabilizes progression without a marked effect on bladder dysfunction. Results are mixed for the relief of pain. In follow-up care, the possibility of retethering of the spinal cord has to be monitored.
D. Diastematomyelia is splitting of the spinal cord by a bony or fibrous septum. The anomaly can become evident during growth spurts or minor trauma. Spina bifida occulta often is present. Pain is prominent in adults but not in children.
1. The septum is removed in children in response to expected progression.
E. Platybasia (upward displacement of the floor of the posterior fossa) and basilar invagination (protrusion of the odontoid through the foramen magnum) decrease the diameter of the foramen magnum. In adults, these conditions manifest as spastic tetraparesis or lower cranial nerve dysfunction.
1. Surgical options include decompressive suboccipital craniectomy with upper cervical laminectomy.
2. Counseling is indicated for the apparent genetic basis of skull-base disorders.
F. Syringomyelia is a congenital pericentral cavity of the cervical spinal cord that may extend into the thoracic cord or upward into the medulla (syringobulbia). Most lesions are between C2 and T9. It most frequently occurs in the setting of Chiari I malformation, but other etiologies include Klippel–Feil’s syndrome, tethered spinal cord, postinfectious, postinflammatory, post-traumatic, and spinal neoplasms.
1. Syringomyelia usually manifests itself in adolescence or adulthood. The classic syndrome of upper-extremity weakness and atrophy (often asymmetric) with dissociated sensation in a “cape distribution” is found in 75% of cases. Enlargement of the syrinx can result in Horner’s syndrome and myelopathy. Sleep-related respiratory disturbances are not uncommon, especially in syringobulbia.
2. Although this disorder often is slowly progressive, long periods of stabilization, as well as of acute deterioration, can occur. Neck or arm pain often is a prominent problem among older patients. Scoliosis may be prominent in younger patients.
a. Surgery may not be indicated if symptoms are minimal or very severe, if symptoms have been present longer than 5 years, or if the cord is of normal size on MRI.
b. Surgery may be indicated in the presence of mild deficits of short duration, enlargement of the cord on MRI, and predominant symptoms of pain or spasticity.
3. Surgery is indicated in progressive cases.
a. Results of surgery. The condition of approximately one-third of patients improves, of < one-half stabilizes, and of approximately one-fourth deteriorates.
(1) Pain and paraparesis show the best responses.
(2) Sensory loss, lower motor neuron signs, and brainstem findings are the symptoms least likely to be relieved.
II. VITAMIN DEFICIENCIES
A. Vitamin B12 (cobalamin) deficiency is the most common disorder of the spinal cord for which specific medical therapy exists.
1. Pernicious anemia is the most common cause of vitamin B12 deficiency and is thought to be an autoimmune disorder affecting all races and both sexes. Antibodies to parietal cells are found in almost 90% of patients, and antibodies to intrinsic factor are found in somewhat more than 60%. Increased clinical suspicion, automated RBC indices, and insidious onset (it takes 5 to 10 years to deplete normal body stores of cobalamin) make the fully developed classic hematologic and neurologic manifestations clinical rarities today.
2. Other causes of vitamin B12 deficiency include gastrectomy, diseases of the terminal ileum (Crohn’s disease and diverticulosis), and less severe gastric atrophy (causing food-bound malabsorption). Dietary causes, once thought to be uncommon except in vegans and their breast-fed infants, may be an increasing problem among the elderly. Nitrous oxide exposure during anesthesia can result in precipitous neurologic manifestations in patients with “silent” deficiencies or marginal body stores. Nitrous oxide can also be the cause of an insidious myelopathy if abused.
3. Clinical features.
a. Hematologic features. The classic severe megaloblastic anemia of insidious onset is relatively rare. Approximately 25% of patients have normal hemoglobin values, 25% have normal RBC indices, and 10% to 20% have completely normal CBCs.
b. Neurologic features. Approximately 25% to 50% of patients with vitamin B12 deficiency have neurologic symptoms or signs at diagnosis. One study showed that 27% of patients were without neurologic problems but had abnormal signs. Most patients experience leg dysesthesia as the first symptom. Neurologic presentations include the following:
(1) Polyneuropathy, autonomic disturbances, and decreased visual acuity.
(2) Subacute combined degeneration of the spinal cord affecting the posterior and lateral columns. T2 hyperintensity in the posterior columns may be apparent on spinal MR.
(3) Personality changes, dementia, and psychiatric illness, including psychosis.
4. Diagnosis. In large-scale screening of elderly persons without symptoms, between 10% and 20% may have cobalamin deficiency.
a. Serum vitamin B12 (cobalamin). The sensitivity, specificity, and accuracy of this commonly used assay are controversial. Patients can have normal levels and cobalamin-responsive neurologic disorders; low levels and nonresponsive deficits; or low levels but no other evidence of deficiency. Despite these severe shortcomings, measurement of cobalamin in the serum is the screening test that is the most widely available. For most patients, serum folate should be measured at the same time. Cobalamin levels in blood are light and temperature sensitive.
b. The peripheral blood smear should be examined for macroovalocytes and hypersegmentation of neutrophils. It may be abnormal in the absence of clinically significant anemia, although the sensitivity is low in mild vitamin B12 deficiency.
c. Methylmalonic acid (MMA) (urine and serum) and serum homocysteine (HCYS) accumulate in vitamin B12 deficiency. HCYS level is also elevated in folate deficiency. Assays for these metabolites can be helpful in selected cases. In comparison with serum cobalamin measurement, these assays are characterized by the following:
(1) Advantages include possibly better sensitivity and specificity.
(2) Disadvantages are expense and limited availability.
(a) Elevated MMA and HCYS levels are found in hypovolemia, renal failure, and inherited disorders.
(b) HCYS level is elevated in hypothyroidism, pyridoxine deficiency, and psoriasis.
d. Intrinsic factor antibody testing is specific but suffers from low sensitivity (<60%). However, its low cost and simplicity make this test useful as an alternative confirmation of pernicious anemia.
e. Parietal cell antibody testing is sensitive (>90%) but suffers from low specificity. A negative result makes pernicious anemia unlikely.
5. Treatment.
a. For patients with pernicious anemia, severe deficits, or poor compliance, the usual treatment is cyanocobalamin in the following dosages: 1 mg per day intramuscularly (IM) for 7 to 12 days, then 1 mg per week IM for 3 weeks, and then 1 mg every 1 to 3 months IM for life. Less severe deficiencies can be initially treated with every other day injections for the first week, then weekly injections for the first month. Monthly injection is the standard maintenance regimen and provides the greatest ease of compliance. If longer intervals are used, MMA levels should document adequate treatment and compliance.
b. The unusual patient with pernicious anemia and a strong aversion to injections may be offered oral therapy after initial cobalamin repletion. Large doses are needed, because only 1% to 3% of cobalamin is absorbed independently of intrinsic factor. Monitoring of cobalamin levels is needed until compliance is assured. The usual dosage is 1 to 2 mg per day by mouth for life. Recent evidence suggests oral therapy is at least as efficacious as parenteral therapy in reversing the clinical and biochemical indicators of vitamin B12 deficiency.
c. For patients who are compliant, absorb oral vitamin B12 (the results of a standard Schilling test is normal and serum cobalamin level normalizes), have mild deficits, and want to avoid monthly injections, cyanocobalamin can be given at 50 to 1,000 µg per day by mouth for life. Cobalamin or MMA levels or both should document adequacy of the dosing schedule.
6. Prognosis. Degree of recovery depends on the severity and duration of deficits at diagnosis. Severe deficits or symptoms that have existed for more than 1 year often respond incompletely. Most improvement occurs within 6 to 12 months. If a patient has not shown some improvement after 3 months, a response is unlikely. Either the diagnosis was in error or a vitamin B12 deficiency was coexistent but not causal (commonly observed in dementia).
7. Therapeutic strategy. Predicting which neurologic deficits will respond to vitamin B12 is imprecise. Patients with symptoms or signs consistent with vitamin B12 deficiency and laboratory evidence of a possible vitamin B12deficiency should be given a 6-to 12-month trial of vitamin B12 if other treatable disorders (including folic acid deficiency) have been eliminated.
B. Folic acid deficiency is not generally appreciated as a cause of neurologic dysfunction similar to that found in vitamin B12 deficiency. As in vitamin B12 deficiency, the neurologic deficits can develop with normal or mildly abnormal hematologic values. The incidence of severe neurologic deficits is lower in folate deficiency than in cobalamin deficiency.
1. Dietary inadequacy is the most common cause of folate deficiency, especially among the elderly. Pregnancy, alcoholism, generalized malabsorption, antiepileptic medication, chemotherapy, and congenital defects in absorption or one-carbon enzymes are other potential causes.
2. Clinical features.
a. Instances of dementia, depression, psychosis, polyneuropathy, and subacute combined degeneration of the spinal cord all have been shown to be responsive to folate supplementation. Changes in mental status and higher cortical functions may be the most common presentations in adults.
b. An association between maternal folate supplementation and prevention of neural tube defects in the offspring has been found. Folate appears to correct a subtle block in one-carbon metabolism rather than replenish a deficiency.
3. Diagnosis.
a. A low-serum folate level indicates a negative balance and predicts the likelihood of folate deficiency if uncorrected. The serum level is a poor predictor of total body stores. Because RBC folate level is much greater than serum folate level, hemolyzed specimens should be rejected.
b. RBC folate level indicates body stores during the lifetime of the RBC. The specificity, sensitivity, and usefulness of the value obtained by means of radioassay (the most common technique) are controversial. If both the serum and RBC folate levels are low, ongoing folate deficiency is suggested.
c. Elevated serum HCYS level with a normal serum MMA level is also a marker of folate deficiency and can be helpful in equivocal cases. Because cobalamin deficiency also elevates HCYS level, MMA has to be measured at the same time to differentiate the two deficiencies.
d. A search for a gastrointestinal disorder should be undertaken when signs of malabsorption exist or if a dietary cause is not clear. Gastroenterologic referral and jejunal biopsy should be considered. Concurrent vitamin B12deficiency can cause folate malabsorption and result in low serum and RBC folate levels. (Vitamin B12 deficiency is more likely to elevate serum folate levels consistent with the methylfolate trap hypothesis.)
4. Treatment with folic acid at a dosage of 2.5 to 10.0 mg per day by mouth is sufficient in dietary deficiency. Parenteral (IM) doses are given in malabsorption syndromes. Treatment is for life or until body stores are replete and etiologic factors corrected. A multivitamin should also be taken. Compliance and adequacy of treatment can be monitored with HCYS levels.
5. There is uncertainty concerning the possible epileptogenic properties of folic acid. Folate deficiency should be confirmed with serum HCYS measurement in the care of patients with seizures. Unless severe hematologic or neurologic deficits are present, less aggressive dosing (1 to 2 mg per day) may be best. Normalization of serum HCYS level is necessary to document compliance and to verify adequate treatment.
6. Prognosis is generally good if treatment is started early. Poor responses in cases of dementia or depression with folate deficiency probably represent the concurrence of two common disorders in the elderly.
C. Vitamin E deficiency can cause polyneuropathy, myopathy, scotomata, and demyelination within the posterior columns and spinocerebellar tracts of the spinal cord. The ataxia and posterior column manifestations of abetalipoproteinemia, a rare autosomal recessive disorder of lipoprotein metabolism are responsive to vitamin E supplementation. Rare cases of vitamin E deficiency usually manifest as long-standing malabsorption and steatorrhea. An isolated autosomal recessive defect in transport also exists. Reversal of neurologic deficits with vitamin E supplementation is variable but can be dramatic. Because prognosis appears related to duration of symptoms, a high index of symptoms is warranted. Large oral dosages of vitamin E (800 to 3,600 U per day) or semiweekly injections of α-tocopherol have been used.
D. Copper deficiency can cause a myelopathy marked by a spastic gait and sensory ataxia. An axonal, sensorimotor polyneuropathy frequently coexists. The myelopathy is most pronounced in the cervical cord compared with the thoracic and lumbar segments. It most frequently presents in the fifth and sixth decades and is more common in women. The clinical and radiographic features are often similar to those seen in subacute combined degeneration from B12 deficiency. In fact, the two conditions may coexist. Causes of copper deficiency include prior gastric surgery, malabsorption (e.g., in celiac disease), parenteral feeding deficiency, and excessive zinc intake (as can be seen with use of certain denture creams). However, in many cases, the cause remains unclear. Hematologic manifestations of copper deficiency include anemia or neutropenia. Treatment with copper supplementation may prevent further neurologic deterioration, and variably can improve symptoms. Supplementation is typically oral, at 6 mg per day for 1 week, then 4 mg per day for 1 week and 2 mg per day thereafter.
III. VASCULAR MALFORMATIONS OF THE SPINAL CORD
A. Classification. Spinal cord vascular malformations can be classified into intramedullary arteriovenous malformations (AVMs), perimedullary AVMs, spinal-dural arteriovenous fistulas, epidural AVMs, paravertebral vascular malformations, vertebral hemangiomas, and complex angiomatosis. Of these, spinal-dural arteriovenous fistulas are the most common, making up about 70% of all lesions, and thus the rest of this section will focus on this entity.
B. Clinical features. Patients present with a variety of symptoms distal to the malformation, including progressive paraparesis or radiculopathy, sensory impairment, sphincter disturbances, and pain. When hemorrhage occurs within the lesion, it may result in an acute medullary syndrome.
C. Diagnosis. Most fistulas are located in the mid to lower dorsal spinal cord (T6–T12). Enhanced MRI is the screening modality of choice, but a spinal-dural fistula may escape detection even on high quality MRI. Therefore, selective spinal arteriography is usually indicated.
D. Treatment. Endovascular embolization can often cure these lesions. Open surgery is indicated if embolization fails. In some patients, a combination of both embolization and open surgery is the best therapeutic option.
E. Prognosis. Fistulas in the mid to lower thoracic cord respond best to treatment. Motor symptoms tend to improve most (up to two-thirds of patients), followed by pain and sensory disturbances (up to one-third of patients), and finally sphincteric dysfunction, which is seldom reversible.
IV. SPINAL CORD INFARCTION
Although spinal cord infarctions account for only about 1% of all strokes, they are a cause of significant morbidity. Some common etiologies include prolonged episodes of arterial hypotension, surgical procedures, and pathologies affecting the aorta, disk prolapse or herniation, and arteriopathy; however, in some cases, no cause can be identified. Rarely, spinal cord infarction may be a complication of transforaminal cervical epidural steroid injection. In terms of prevention, motor evoked potentials are commonly been used during aortic surgeries (e.g., during thracoabdominal aortic aneurysm repair) to alert the surgeon to impending spinal cord ischemia, thus reducing the incidence of paraplegia. The neurological symptoms of spinal cord ischemia are referable to the involved artery or segment of the spinal cord. Pain at the level of infarction is also a common finding. Diagnosis is aided by contrast-enhanced MRI. This should include diffusion-weighted imaging as well, as it may take up to 24 hours for ischemic lesions to appear on conventional sequences (Fig. 45.1). Therapeutic interventions include lumbar CSF drainage with or without vasopressor therapy. Treatment is also supportive and focused on the underlying pathology and secondary stroke prevention (patients generally receive an antiplatelet unless there is a contraindication). Unilateral infarcts have a more favorable prognosis; however, prognosis is largely dependent on the severity of the initial deficit. There is some evidence to suggest that intact proprioception at the onset of the deficit also carries a more favorable prognosis.
V. ACUTE SPINAL CORD INJURY
A. Etiology. The major causes of acute spinal cord injury are motor vehicle accidents, falls, recreational injuries, and acts of violence. Fracture and compromise of the spinal cord (or cauda equina) occur most often at cervical and thoracolumbar levels. Although thoracic fractures are less common, neurologic injury is more common because of the narrowness of the spinal canal.
B. Prevention. Proper use of passive and active restraints in automobiles and use of helmets by motorcyclists and bicyclists prevent head and spinal injuries. For example, the Think First program, which addresses educational issues for youth in kindergarten through 12th grade and is actively supported by the neurosurgical community, should be embraced by health care providers.
C. Prognosis. Improvement of even one level can have a dramatic effect on function, especially in cervical cord injuries (Table 45.1). Final neurologic function depends on severity of initial injury, prevention of secondary damage, and successful management of the complications and sequelae of the acute injury and intensive rehabilitation. Neurologic assessment 72 hours after injury according to American Spinal Injury Association guidelines is useful in estimating outcome.
1. Features suggesting a possibility of neurologic improvement are as follows:
a. Motor or sensory function below neurologic level (incomplete lesion).
b. Degree to which motor strength is preserved below neurologic level.
c. Preservation of pinprick response in addition to light touch below neurologic level.
d. Age < 30 years.
e. Residual anal sphincter tone.
f. Relatively well-preserved vertebral alignment.
2. Features suggesting a poor prognosis are as follows:
a. Absence of residual function (complete lesion).
b. Hemorrhage or multilevel edema on MRI.
D. Principles of treatment.
1. Immobilization of the spine at the scene, in transport, and in the emergency department is critical in preventing further damage.
2. ABCs of trauma care; supplemental oxygen should be provided.
3. Primary survey of associated damage.
a. Alteration of sensorium necessitates investigation for accompanying head injury.
b. Neurologic level may mask the usual symptoms and signs of thoracic, abdominal, pelvic, or extremity injury. More reliance is placed on objective tests.
4. Radiologic evaluation of level of skeletal injury.
5. Skeletal traction for stabilization and closed reduction if indicated.
6. Assessment of neurologic level of injury.
a. The neurologic level of injury is the most caudal segment at which both motor function and sensory function are intact bilaterally (Table 45.2).
b. The completeness of the injury is defined by American Spinal Injury Association classes grades A through E, which describe function at least three levels below the neurologic level of injury. Grade A indicates a complete level, grade E indicates recovery, and grades B through D describe incomplete levels.

FIGURE 45.1 A 33-year-old woman with systemic lupus erythematosus, antiphospholipid antibody syndrome, status post-quintuple coronary-artery-bypass graft, who developed acute cardiac tamponade and hepato-renal syndrome. She was found to have flaccid paraplegia of the lower extremities. Pre- and post-contrast MRI (sagittal and axial) of the lower thoracic spinal cord and conus medullaris demonstrates abnormal high signal intensity most prominent at the levels of T11 and T12, as seen on the T2-weighted images. These findings are consistent with spinal cord ischemia. (Courtesy of José Biller.)
7. Secondary survey and stabilization of patient’s condition.
8. Transport to spinal cord injury center.
9. Surgical decompression preferably done within 24 hours in select cases.
10. Medications to prevent secondary (oxidative) damage.
a. The National Acute Spinal Cord Injury Study 2 (NASCIS 2) showed a modest but significant benefit compared with placebo for high-dose methylprednisolone if started within 8 hours of injury. The initial dose of 30 mg/kg intravenous bolus is followed by 5.4 mg/kg/hour infusion for 23 hours. Complications include pneumonia, sepsis, and gastrointestinal hemorrhage.
b. NASCIS 3 showed an additional 24 hours of steroid infusion to be beneficial to patients who received the initial bolus between 3 and 8 hours after injury. Treatment started at later than 8 hours after injury resulted in poorer outcomes than did placebo treatment.
11. Restoration and maintenance of spinal alignment.
VI. SEQUELAE OF SPINAL CORD INJURIES
A. Pressure sores are the most preventable complication of spinal cord injury.
1. Prevention. Patient and family education are important. Pressure is relieved by turning in bed every 2 hours and “wheelchair” lifts for 5 to 10 seconds every 15 to 30 minutes. Special mattresses and wheelchair cushions do not obviate proper positioning and frequent repositioning. The skin is kept clean, dry, and inspected daily. Attention is paid to nutritional requirements.
TABLE 45.1 Expected Functional Outcomes in Spinal Cord Injury
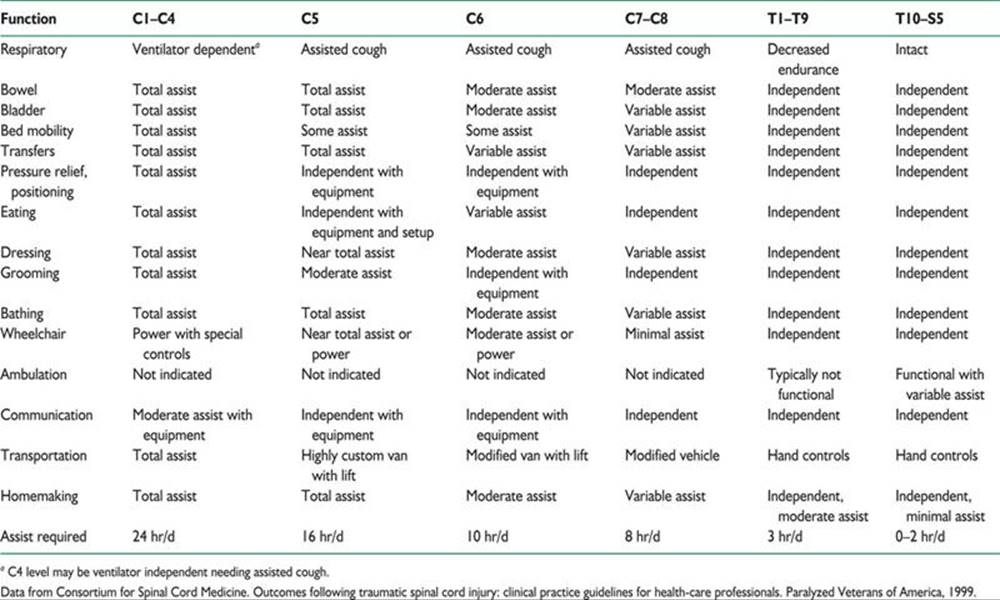
TABLE 45.2 Key Muscles and Sensory Areas for Determination of Neurologic Level of Injury

2. Pressure relief. A repositioning schedule ensuring that the sore is always pressure free needs to be rigidly followed because the reduced number of possible weight-bearing position makes another sore more likely. Simultaneous management of more than one pressure sore requires special frames or flotation beds.
3. Débridement. Saline wet-to-dry gauze and whirlpool therapy are standard, but commercial enzyme preparations are less labor intensive. If the eschar is hard and blackened, necrotic tissue is removed surgically.
4. Dressings. Shallow ulcers are covered with sterile gauze. Occlusive dressings may promote more rapid healing and have to be changed less often but are much more expensive. Deeper, pear-shaped ulcers are loosely packed with saline-soaked gauze to prevent abscess formation and to promote “bottom-up” healing. The goal is to keep the wound moist, whereas the surrounding tissue is kept dry.
5. Electrical stimulation may accelerate wound healing.
6. Surgical excision with a myocutaneous flap to fill the cavity is usually required for deeper ulcers. Reduction of bony prominences may be necessary.
B. Deep venous thrombosis is a serious concern after spinal cord injury. Pain may not be felt below a sensory level, and swelling may be masked by edema and vasomotor changes.
1. Prophylaxis is needed for up to 3 months or until discharge from the rehabilitation unit. Intermittent pneumatic compression devices or compression stockings are used for the 2 weeks after injury. Anticoagulation with low-molecular-weight heparin or adjusted-dose unfractionated heparin should be started 48 to 72 hours after injury and continued 8 to 12 weeks depending on associated risk factors. Vena caval filters are placed in patients with contraindications to or who have undergone unsuccessful anticoagulation therapy. Filters should also be considered in addition to anticoagulation in the care of patients with complete C2 or C3 neurologic levels of injury.
2. Treatment is the same as that of patients without spinal cord injury. Mobilization and exercise of the lower extremities should be withheld 48 to 72 hours until anticoagulation is adequate. Pain relief should be provided to lessen the possibility of autonomic dysreflexia.
C. Autonomic dysreflexia. From 30% to 85% of patients with quadriplegia or high paraplegia have paroxysmal episodes of severe hypertension, sweating, flushing, and piloerection accompanied by headache, chest pain, and bradycardia or tachycardia in response to relatively benign stimuli below the level of injury. Pulmonary edema, intracranial hemorrhage, cerebral infarction, seizures, or death can result. Bladder and bowel distention, instrumentation, or irritation are the most common precipitating stimuli.
1. Etiology. In the setting of a spinal lesion above the major splanchnic outflow tract (T6–L2), reflex activation of sympathetic discharge occurs below the lesion unchecked by descending inhibitory pathways from supraspinal centers.
2. Management. Initial treatment entails removal of the precipitating stimulus and medication for the hypertensive crisis.
a. Removal of precipitating stimulus.
(1) Stop procedure.
(2) Check for urinary catheter blockage.
(3) Remove tight clothing, shoes, straps, and other restrictive items.
(4) Catheterize carefully with 2% lidocaine jelly.
(5) Perform kidney, ureter, and bladder and rectal examination with lidocaine jelly to check for impaction.
(6) Check for sores, infection, trauma, and fractures.
(7) Consider acute abdomen and deep venous thrombosis.
b. Management of hypertension.
(1) Elevate head of bed or place patient in sitting position to induce postural changes in blood pressure.
(2) Drug therapy.
(a) Nifedipine 10 mg by mouth (immediate release form—bite through capsule and swallow); monitor response or
(b) Nitroglycerin 2% ointment—1 inch (2.5 cm) applied above neurologic site of injury; monitor response.
(3) If blood pressure remains critical, intravenous protocols (e.g., hydralazine, diazoxide, and sodium nitroprusside) for hypertensive crisis must be initiated.
c. Management of profuse sweating without hypertension. Give propantheline at 15 mg by mouth (may be repeated after 10 minutes) or oxybutynin at 5 mg by mouth (may be repeated after 10 minutes).
3. Prophylactic medications.
a. Nifedipine 10 mg by mouth 30 minutes before procedure.
b. Phenoxybenzamine 10 to 20 mg by mouth three times a day.
c. Scopolamine patch may help with reflex sweating.
D. Depression must be continually assessed and managed.
E. Central pain syndrome. Development of chronic dysesthesia or central (neuropathic) pain above, at, or distal to the level of injury poses therapeutic challenges. Central pain is in addition to the musculoskeletal and visceral pain experienced by patients with spinal cord injuries.
1. Etiology.
a. Above level of injury. Compressive mononeuropathy (e.g., ulnar and median) and post-traumatic syringomyelia formation.
b. At level of injury. Central pain from cord damage, radicular pain from root damage, and complex regional pain syndrome.
c. Below level of injury. Central pain.
2. Pharmacologic approach is trial and error.
a. Tricyclic antidepressants for nonlancinating pain.
(1) Amitriptyline (Elavil) or nortriptyline (Pamelor) 10 to 25 mg by mouth at bedtime; increase by 10 to 25 mg every 5 to 7 days as tolerated to 75 to 150 mg at bedtime.
(2) Side effects include sedation, anticholinergic effects, orthostatic hypotension, weight gain, and cardiac arrhythmia.
(3) If side effects are not tolerable, a chemically unrelated compound, such as duloxetine (Cymbalta) at 30 to 60 mg per day by mouth, may be tried.
b. Anticonvulsants (frequently in combination with tricyclic antidepressants) for lancinating central pain.
(1) Carbamazepine (Tegretol) 100 mg twice a day increased 100 mg every 3 days as tolerated to a serum level of 8 to 10 mg per ml in three or four doses per day.
(a) Side effects include sedation, diplopia, gastrointestinal upset, ataxia, weakness, rash, and bone marrow suppression.
(b) Monitor CBC with platelets every 2 weeks for 3 months, then CBC, platelets, and liver function every 3 to 6 months.
(2) Gabapentin (Neurontin) 100 mg three times a day increased 100 to 300 mg every 3 days as tolerated up to 600 to 900 three or four times a day.
(a) Side effects include drowsiness and dizziness.
(b) Blood levels are not used clinically, and no monitoring is needed.
(3) Pregabalin (Lyrica) 50 mg three times a day increased to 100 mg three times a day after 1 week as tolerated.
(a) Side effects include peripheral edema, weight gain, constipation, dizziness, and somnolence.
(b) Blood levels are not used clinically and no monitoring is needed.
3. Physical methods may provide some temporary relief for central pain at the level of the injury.
a. Transcutaneous electrical nerve stimulation.
b. Warm or cool packs and ultrasound.
4. Surgical treatment should be considered only after conservative therapy has failed.
a. Dorsal root entry zone (DREZ) surgery.
(1) Laminectomy and radiofrequency ablation of DREZ is performed two levels above and one level below the site of injury.
(2) Improvement is realized in 60% to 90% of patients. Best results are achieved in patients with pain at or just below the level of injury.
(3) Complications include loss of one or two sensory levels, CSF leakage, hematoma, and bowel, bladder, and sexual dysfunction.
b. Avoid sympathectomy, rhizotomy, and cordotomy.
5. Narcotic therapy is indicated only after both conservative and surgical therapies have failed.
a. Combination with tricyclic antidepressants may be synergistic.
b. The patient must be carefully selected and carefully supervised.
c. Methadone (Dolophine) sustained release oxycodone (Oxycontin), and an intrathecal morphine pump (if possible) are options for selected patients.
(1) A formal contract detailing expectations and criteria for termination of treatment are made with the patient.
(2) Periodic attempts should be made to wean the medication.
(3) Side effects include sedation and cognitive slowing, respiratory depression, constipation, and reduced sexual function.
VII. SPINAL EPIDURAL ABSCESS
A. Etiology. Epidural abscesses occur in patients with predisposing conditions, such as a chronic disease (alcoholism and immunodeficiency states), a spinal abnormality or intervention, or a source for local or systemic infection. Bacteria seed the epidural space by either contiguous spread or hematogenous dissemination. Staphylococcus aureus accounts for 60% of cases, whereas other gram-positive cocci account for 13% and gram-negative bacteria occur in about 15% of cases.
B. Clinical features. Back pain, fever, and neurological deficits are the most common symptoms; however, this triad is not often found in all patients. The clinical features are divided into four stages:
1. Back pain at the level of the abscess.
2. Radicular pain from the involved level of the spinal column.
3. Motor weakness, sensory deficit, and bowel and bladder dysfunction.
4. Paralysis.
The rate of progression between stages can vary between a few hours to days.
C. Diagnosis. Two-thirds of patients will have a leukocytosis. The vast majority of patients will also have an elevated erythrocyte sedimentation rate upon presentation. CRP levels are also useful, but processing can take hours to days, which may unnecessarily delay the diagnosis. The initial CRP value is useful for comparison to repeat values as a measure of treatment response. Bacteremia can be detected in up to 60% of cases. However, definitive diagnosis is best established by contrast-enhanced MRI of the affected area.
D. Treatment. Emergent surgical decompression and debridement combined with systemic antibiotics for at least 6 weeks is the treatment of choice. The most common causative organism is S. aureus (up to 70% of cases). Empiric antibiotic therapy should provide coverage against staphylococci and gram-negative bacilli.
E. Prognosis. Prompt diagnosis and the patient’s neurologic status prior to surgical drainage are the most important predictors of outcome.
VIII. DEMYELINATING LESIONS OF THE SPINAL CORD
The most common cause of demyelination in the spinal cord is multiple sclerosis (MS). Up to 50% of cases will involve the spinal cord. The lesions are typically dorsolateral, longitudinal, and flame-shaped. Another less common cause of demyelination in the spinal cord is neuromyelitis optica (NMO) or Devic’s disease. It is currently recognized as its own distinct disorder, separate from MS. Newly proposed diagnostic criteria for NMO include optic neuritis, acute myelitis, and at least two of the three following supportive criteria: (1) contiguous spinal cord MRI lesion extending three or more vertebral segments (Fig. 45.2), (2) brain MRI not meeting diagnostic criteria for MS, and (3) NMO-IgG seropositivity. The NMO-IgG antibody has a sensitivity of 74% and a specificity of >90%. Treatment of acute attacks of optic neuritis or myelitis often only partially respond, or do not respond at all to high-dose glucocorticoids. In this setting, plasmapheresis is often used. Maintenance of remission in NMO requires long-term immunosuppressive therapy. There has been evidence for the use of azathioprine, methotrexate, mitoxantrone, mycophenolate mofetil, and rituximab.
IX. CENTRAL CORD SYNDROME
A. Etiology. Hyperextension injuries may produce a spinal cord contusion primarily affecting the central gray matter. Lamination of tracks in the cervical cord (sacral fibers, lateral; cervical fibers, and medial) explains the clinical signs and symptoms.
B. Clinical features. Patients have “inverted quadriparesis,” in which upper-extremity weakness exceeds lower-extremity weakness. Transient burning dysesthesia in the hands with little weakness, or urinary dysfunction can also occur. With recovery, the leg, bladder, and upper-extremity weaknesses improve. The fingers are last to recover.
C. Treatment.
1. Conservative therapy consists of rigid immobilization of the neck, physical therapy, and consideration of a course of corticosteroids.
2. Surgical therapy. On the basis of neuroimaging findings, patients whose condition has not improved or has plateaued or who have instability of the spine are considered for surgical decompression.

FIGURE 45.2 A 44-year-old African American man with neuromyelitis optica (Devic’s disease). MRI of the cervical spine without and with contrast shows contiguous cord signal abnormality identified involving the cervical spinal cord from the craniocervical junction to the C6–C7 level. The spinal cord signal abnormality involves nearly the entire central spinal cord symmetrically with relative sparing of the lateral portions bilaterally. The cervical spinal cord signal abnormality is associated with tapered cord expansion resulting in circumferential, partial to complete effacement of the thecal sac at the involved levels. (Courtesy of José Biller)
D. Prognosis. Almost all patients have improvement, but often to an incomplete degree among the elderly. Delayed progressive myelopathy can develop in approximately 25% of cases.
X. HYPEREXTENSION–FLEXION INJURY (WHIPLASH INJURY)
A. Etiology. Automobile accidents account for approximately 85% of whiplash injuries. The cardinal symptoms of neck pain and headache are musculoskeletal. Concomitant symptoms may include dizziness, visual impairments, nausea, tinnitus, deafness, paresthesias, lower back pain, arm or shoulder pain, post-traumatic stress disorder, and cognitive dysfunction. The roles of mild CNS injury and psychosocial factors are controversial and have led to biopsychosocial models of outcome in the disorder.
B. Prevention. Automobile head restraints reduce flexion–hyperextension motion of the head in automobile accidents, especially during rear-end collisions. However, surveys have shown that the restraints frequently are adjusted incorrectly.
C. Natural history. Rear-end collisions are involved in most whiplash injuries. Cynicism and controversy exist over the cause of chronic whiplash syndrome. Although figures vary widely, approximately 15% to 30% of patients continue to have symptoms 6 months after the injury. By 12 months, 80% of patients have no symptoms, whereas 5% of patients remain severely affected. Results of fluoroscopically guided nerve block studies suggest that zygapophyseal joint pain (usually C2–C3) accounts for 50% of chronic neck pain after whiplash.
D. Treatment. Compensation concerns hinder controlled clinical trials of treatment.
1. Positive attitude and encouragement.
2. Ice for first 24 hours.
3. Muscle relaxants, nonsteroidal anti-inflammatory drugs, and adequate pain relief in the first 7 to 14 days.
4. Resumption of most normal activities together with active therapy or home exercises results in better outcome than with conventional regimens of restricted activity, rest, and soft cervical collar.
5. Heat, ultrasound, massage, and trigger-point injections often make patients more comfortable but remain unproven.
6. Percutaneous radiofrequency neurotomy for cervical zygapophysial joint pain has been showed to be effective in several studies, but the pain frequently returns and necessitates repeated procedures.
XI. SPASTICITY
Spasticity is one of the cardinal manifestations of chronic spinal cord disease. In acute spinal lesions, spasticity develops after a variable period of spinal shock, whereas in disorders with insidious onset, it may be the first symptom noticed.
A. The decision to treat a patient must be made on an individual basis. Treatment is indicated when the advantages of spasticity outweigh the disadvantages. Specific treatment goals need to be formulated.
1. Advantages.
a. Bowel training maintains sphincter tone.
b. “Internal crutches” are available for ambulation.
c. Weight bearing is possible in transfers.
d. Osteopenia is reduced.
e. Muscle bulk is increased.
f. Venous tone is increased, and deep venous thrombosis may be decreased.
2. Disadvantages.
a. Pain and falls result from paroxysmal spasms.
b. Hygiene is impaired owing to hip adductor spasticity.
c. Joint contractures occur.
d. Pressure sores form.
e. Renal damage occurs because of external sphincter spasticity.
f. Movements required for activities of daily living are impaired or interrupted.
B. Assessment of severity can be made with the modified Ashworth scale (Table 45.3).
C. A changing pattern in a previously stable degree of spasticity should alert the clinician to varying etiologic factors.
1. Medication: fluoxetine, sertraline, or trazodone.
2. Anxiety.
3. Tight clothing or shoes.
4. Inadequate or prolonged postures.
5. Formation of pressure sores.
6. Development of deep venous thrombosis.
7. Ingrown toenails.
8. Spinal instability.
9. Fractures.
10. Post-traumatic syringomyelia.
11. Gastrointestinal dysfunction: impaction, hemorrhoids, and acute abdomen.
12. Genitourinary dysfunction: infection, stones, blocked catheters, and disorders of testicle, prostate, vagina, uterus, or ovary.
D. Management is based on a multidisciplinary approach with a rigorous program of both passive and active stretching.
TABLE 45.3 Modified Ashworth Scale for Measuring Spasticity
Grade 0: Normal muscle tone
Grade 1: Slight increase in muscle tone; “catch” or minimal resistance at end of ROM
Grade 2: Slight increase; “catch” followed by minimal resistance for remainder of ROM
Grade 3: More marked increase in tone through most of ROM; parts moved easily
Grade 4: Considerable increase in tone; passive movement difficult
Grade 5: Affected part or parts rigid in flexion or extension
Total score is the average of bilateral hip flexion and abduction, knee flexion, and ankle dorsiflexion.
Abbreviation: ROM, range of motion.
Adapted from McLean BN. Intrathecal baclofen in severe spasticity. Br J Hosp Med. 1993;49:262–267.
1. Physical modalities.
a. Range of motion and stretching exercises.
b. Heat or cold.
c. Vibration (increases presynaptic spinal inhibition).
d. Splints, casts, and orthotics to prevent contractures and increase mobility.
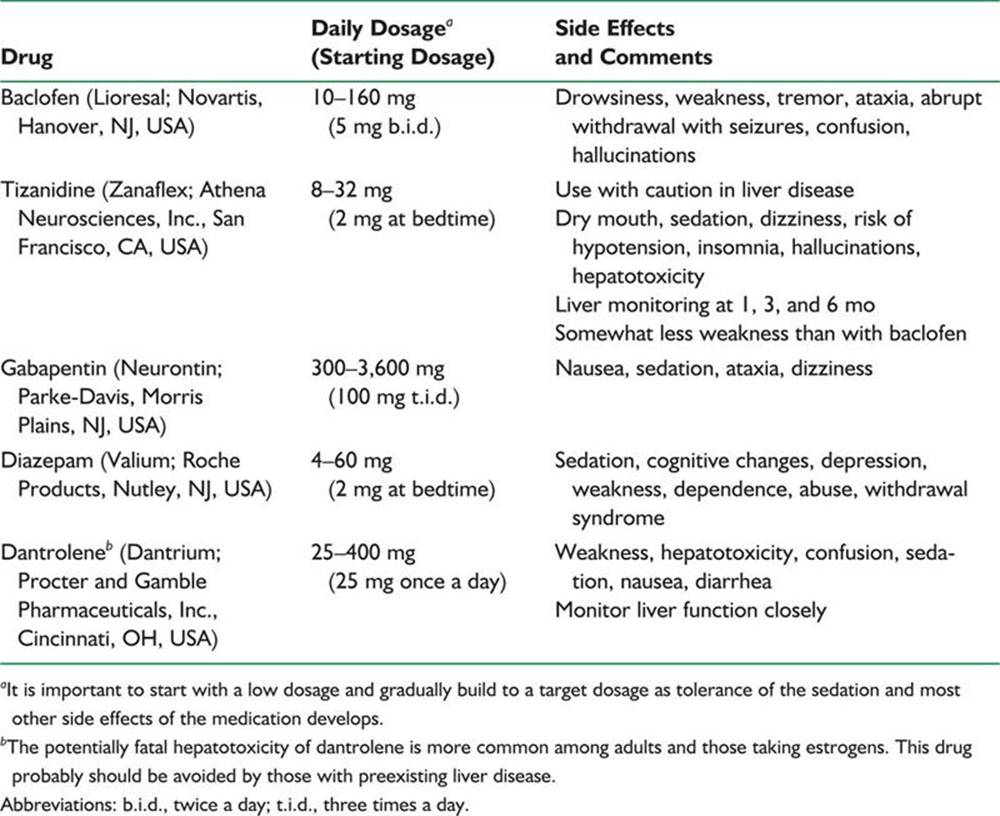
2. Useful medications are summarized in Table 45.4. Muscle relaxants (antispasmodics) are not used in the long-term management of spasticity.
3. Nerve blocks.
Botulinum toxin type A (Botox; Allergan, Irvine, CA, USA) injection has been found effective for focal spasticity at a variety of sites.
a. The discomfort and expense of numerous injections in large lower extremity muscles limit this technique to relatively small muscles.
b. Transient postinjection discomfort and side effects are generally well-tolerated. Excessive weakness and flu-like syndromes may be experienced at initiation of treatment. Botulinum injections should be avoided by patients receiving aminoglycosides. Neutralizing antibodies are more common with larger, more frequent doses.
c. Advantages are reversible block (2 to 6 months) and selectivity toward motor fibers.
d. Disadvantages are expense and need for repeated injections.
4. Neurosurgical procedures.
a. An intrathecal baclofen pump is a safe alternative to ablative surgery for intractable spasticity at experienced centers.
(1) Referral to an experienced center should be considered for patients with stable neurologic disorders accompanied by spasticity seriously interfering with quality of life. Oral agents should have been found ineffective or limited owing to intolerable side effects.
(2) Patients are selected after a test dose of 50 to 75 mg baclofen administered by lumbar puncture. Spasticity is assessed 1, 2, 4, and 8 hours after injection with the modified Ashworth scale (Table 45.3). If two-point improvement is not documented and side effects are tolerable, a second larger test dose (75 to 100 mg) is given the next day.
(3) During the first year after implantation, daily doses generally increase before stabilizing in the range of 300 to 800 mg per day.
(4) Improvement is observed in muscle tone, mobility, and bladder function, and spasms and musculoskeletal pain are relieved. There is little or no relief of central pain.
(5) Systemic side effects are less than with oral therapy. Drowsiness, nausea, hypotension, headache, and weakness may be experienced during the dose titration phase. Infections and catheter or pump complications are rare but potentially serious side effects.
(6) Depletion of the pump battery in 5 to 7 years necessitates replacing the entire pump unit.
TABLE 45.4 Drug Management of Spasticity
(7) Although life-threatening, all instances of drug overdose have been completely reversible. Experience and better pump design have decreased the complication rate to <5%. In early series of patients, surgical revision was needed in 20% of cases for catheter-related problems.
b. Selective posterior rhizotomy with intraoperative EMG selection of lumbosacral rootlets for sectioning is useful in the management of cerebral palsy. Two-thirds of patients’ conditions are improved with minimal sensory loss and few side effects. DREZ operations are functionally similar microsurgical procedures.
c. Percutaneous posterior rhizotomy is technically more difficult, and recurrence may be more of a problem.
d. Efficacy of spinal cord stimulators is controversial.
e. Peripheral neurectomy is occasionally used to relieve specific joint contractures.
f. Longitudinal myelotomy, nonselective posterior rhizotomy, and anterior rhizotomy are rarely performed.
5. Orthopedic procedures are used most often performed in a supportive role to relieve pain, increase mobility, and decrease deformity in cerebral palsy.
a. Tendon release, lengthening, and transfer.
b. Osteotomy and arthrodesis.
![]()
Recommended Readings
Belanger E, Levi AD. The acute and chronic management of spinal cord injury. J Am Coll Surg. 2000;190:603–618.
Bryce TN, Ragnarsson KT. Pain after spinal cord injury. Phys Med Rehabil Clin N Am. 2000;11:157–168.
Darouiche RO. Spinal epidural abscess. N Engl J of Med. 2006;355:2012–2020.
Davis EC, Barnes MP. Botulinum toxin and spasticity. J Neurol Neurosurg Psychiatry. 2000;69:143–147.
Green R, Kinsella LJ. Current concepts in the diagnosis of cobalamin deficiency. Neurology. 1995;45:1435–1440.
Kita M, Goodkin DE. Drugs used to treat spasticity. Drugs. 2000;59:487–495.
Kumar N. Copper deficiency myelopathy. Mayo Clin Proc. 2006;81(10):1371–1384.
Maynard FM Jr, Bracken MB, Creasey G, et al. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association. Spinal Cord. 1997;35:266–274.
Milhorat TH, Chou MW, Trinidad EM, et al. Chiari I malformation redefined: clinical and radiographic findings for 364 symptomatic patients. Neurosurgery. 1999;44:1005–1017.
Newey ML, Sen PK, Fraser RD. The long-term outcome after central cord syndrome: a study of the natural history. J Bone Joint Surg Br. 2000;82:851–855.
Shamji MF, Ventureyra EC, Baronia B, Nzau M, Vassilyadi M. Classification of symptomatic Chiari I malformation guide to surgical strategy. Can J Neurol Sci. 2010;37:482–487.
Teasell RW, Mehta S, Aubut JA, et al. A systematic review of pharmacologic treatments of pain after spinal cord injury. Arch Phys Med Rehabil. 2010;91:816–831.
Tompkins M, Panuncialman I, Lucas P, et al. Spinal epidural abscess. J Emerg Med. 2010;39(3):384–390.
Van Suijlekom H, et al. Whiplash-associated disorders. Pain Practice. 2010;10(2):131–136.