The peripheral nervous system (PNS) consists of those structures (including cranial nerves III-XII, spinal nerves, nerves of the extremities, and the cervical, brachial and lumbosacral plexi) containing nerve fibers or axons that connect the central nervous system (CNS) with motor and sensory, somatic and visceral, end organs1.

Muscle strength grading usually employs the Royal Medical Research Council of Great Britain (MRC) scale2, a common modification of which is shown in Table 24-1. Muscle stretch reflexes may be graded as shown in Table 24-22.
Upper motor neuron vs. lower motor neuron
Lower motor neurons (LMN) (first-order motor neuron): cell bodies (soma) reside in spinal cord (in anterior gray matter) or in brainstem (for cranial nerve motor nuclei). Axons connect directly to neuromuscular junction of muscles.
Upper motor neurons (UMN) (second-order motor neurons): some soma reside in the primary motor cortex (precentral gyrus) of the brain. Axons project to LMNs.
See Table 24-3 for comparison of weakness due to UMN vs. LMN.
Table 24-2 Muscle stretch reflex (deep tendon reflex) grading scale
|
Grade |
Definition |
|
0 |
no contraction (total paralysis) |
|
0.5+ |
elicitable only with reinforcement* |
|
1+ |
low normal |
|
2+ |
normal |
|
3+ |
more brisk than normal (hyperreflexic) |
|
4+ |
hyperreflexic with clonus |
|
5+ |
sustained clonus |
* In the LEs, reinforcement consists of having the patient hook the tips of the fingers of the left hand into the tips of the hooked fingers of the right hand and pulling (Jendrassik maneuver). Reinforcement in the UEs consists of having the patient clench their teeth
Table 24-3 Upper vs. lower motor neuron paralysis
|
Upper motor neuron paralysis |
Lower motor neuron paralysis |
|
|
possible etiologies |
stroke (motor strip, internal capsule…), spinal cord injury, cervical spondylotic myelopathy |
herniated intervertebral disk, nerve entrapment syndrome, polio, progressive muscular atrophy (PMA) |
|
muscle tone |
initially flaccid; later spastic with clasp-knife resistance |
flaccid |
|
tendon reflexes |
hyperactive; clonus may be present |
absent |
|
pathologic reflexes (e.g. Babinski, Hoffman) |
present (after days to weeks) |
absent |
|
muscle manifestations |
spontaneous spasms may occur; some atrophy of disuse may occur |
fibrillations*, fasciculations*. Atrophy after days to weeks due to trophic influence |
*Fasciculations vs. fibrillations
 Fasciculations are coarse muscle contractions that are visible to the naked eye, whereas fibrillations are not visible and require EMG to detect (AKA fibrillation potentials - see page 270).
Fasciculations are coarse muscle contractions that are visible to the naked eye, whereas fibrillations are not visible and require EMG to detect (AKA fibrillation potentials - see page 270).
Fasciculations represent discharge of a group of muscle fibers (all or part of an entire motor unit), and occur most often in diseases involving anterior horn cells, including:
1. amyotrophic lateral sclerosis (ALS): see page 65
2. spinal muscular atrophy: see page 1191
3. polio
4. syringomyelia
MUSCLE INNERVATION
THUMB
Flexion/extension: occurs in the plane of the palm.
Abduction/adduction: occur in a plane at right angles to palm.
Opposition: bringing the thumb across the hand.
Table 24-5 The 3 innervations of the thumb
|
Action |
Nerve |
Muscle(s) |
|
abduction, flexion, opposition* |
median |
abductor pollicis brevis, flexor pollicis brevis, opponens pollicis |
|
adduction |
ulnar |
adductor pollicis |
|
extension |
radial† |
extensor pollicis brevis & longus |
* occasional anomalous innervation by ulnar nerve
† via the posterior interosseous nerve

24.1. Some basic points about peripheral nerve injury/surgery
NERVE ACTION POTENTIALS
Stimulating a healthy nerve fiber with an electrical stimulus of an amplitude and duration that exceeds its threshold will produce a conducted impulse, or nerve action potential (NAP)4 (p 103). Medium-sized axons (fibers) have a lower threshold than large ones which have lower threshold than small or fine axons4 (p 103).
Use of NAP with lesion in continuity
There is some degree of continuity in ≥ 60% of nerve injuries4 (p 104).
For a lesion in continuity (LIC), if surgical repair is needed, it may be too late if one waits until there is failure of anticipated clinical improvement. Presence of a NAP (regardless of amplitude or latency) distal to an LIC in the first few months after an injury usually indicates that operative intervention will not be needed. For recommended timing to obtain NAP recording, see Table 24-74 (p 106).
Table 24-7 Recommended timing to obtain NAP recording
|
Injury |
Timing |
|
relatively focal contusions |
2-4 months |
|
stretch injuries (esp. brachial plexus) |
4-5 months |
|
partial injuries & entrapments, compressive lesions and tumors |
any time |
|
to identify an area of conduction block (regardless if lesion is from neuropraxia, axonotmesis, or neurotmesis) |
acutely |
TIMING OF SURGICAL REPAIR
The longer the distance from the injury site to the functional unit to be reinnervated, the earlier surgical intervention should be considered4 (p 74.
24 month rule4 (p 74): after 24 months of denervation, most muscles cannot recover useful function even with reinnervation. Exceptions: facial muscles, large bulky muscles such as biceps, brachialis, gastrocs, and some lesions in continuity with some preserved innervation.
24.2. Brachial plexus
Formed by ventral rami (the dorsal rami innervate the paraspinal muscles), most commonly of nerve roots C5-T1 (schematically depicted in Figure 24-1).
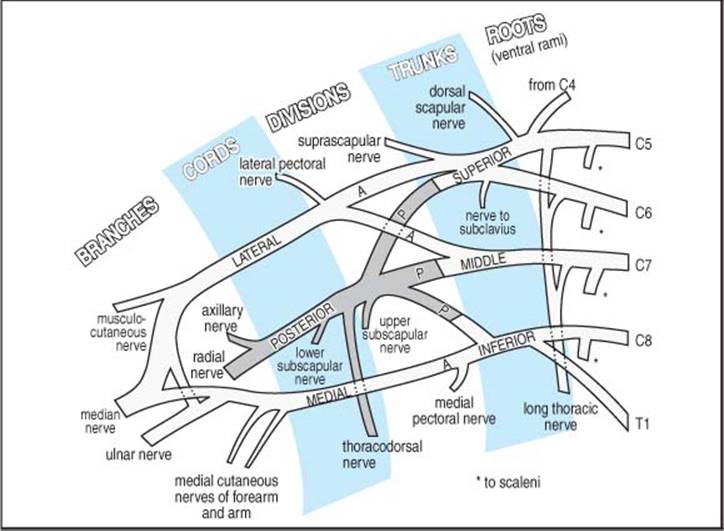
Figure 24-1 Schematic diagram of the brachial plexus
(By Permission: Churchill Livingstone, Edinburgh, 1973, R. Warwick & P. Williams: Gray’s Anatomy 35th Edition © Longman Group UK Limited)
BRACHIAL PLEXUS BRANCHES
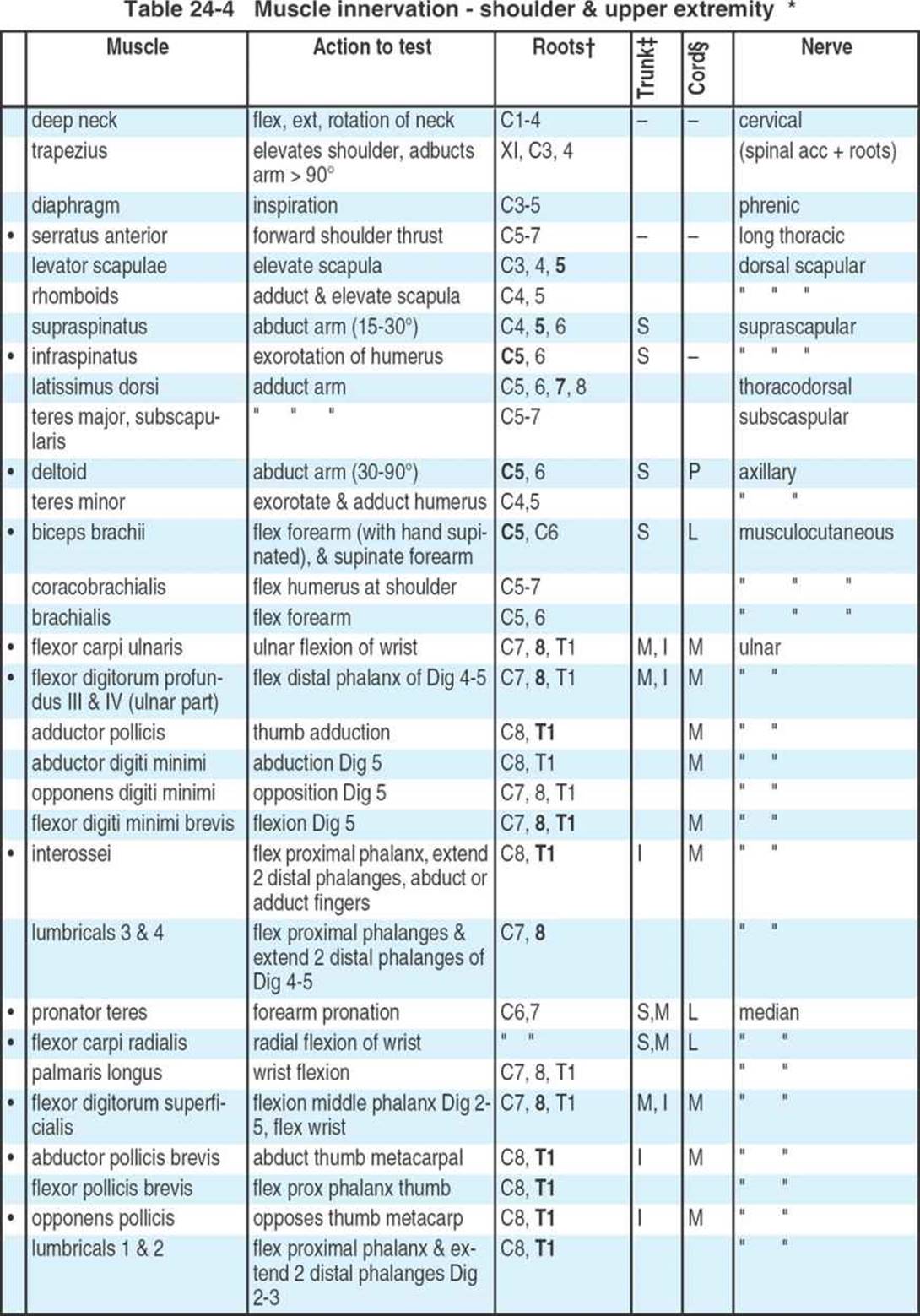
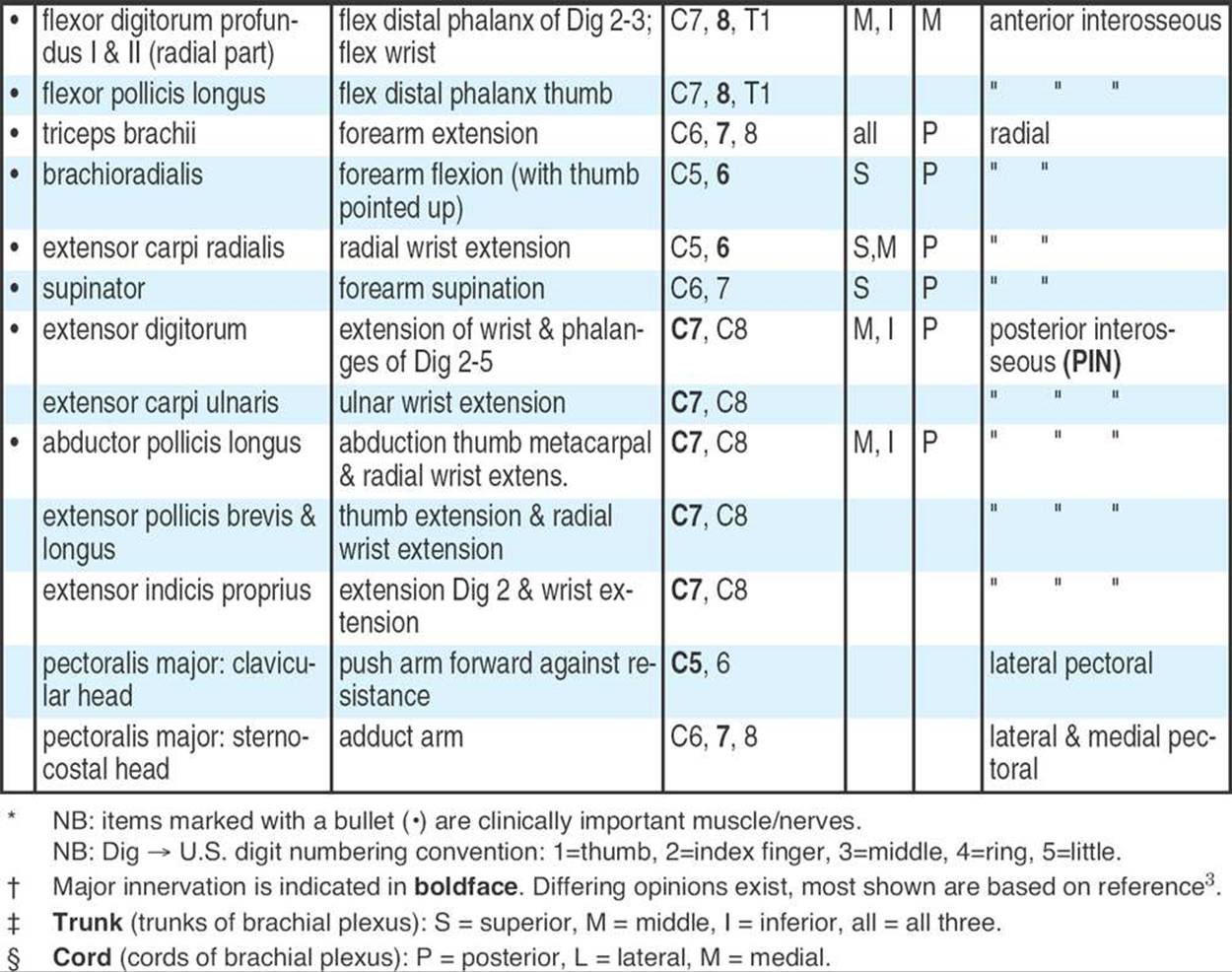
Table 24-4 shows action, etc. of specific muscles. Also see Figure 24-1. “![]() ” indicates that the nerve supplies the muscles listed; “
” indicates that the nerve supplies the muscles listed; “![]() ” denotes a branch of the preceding nerve.
” denotes a branch of the preceding nerve.
Radial nerve (C5-C8)
See Figure 24-2. Radial nerve (and its branches) innervate the extensors of arm and forearm:
![]() triceps (all 3 heads)
triceps (all 3 heads)
![]() anconeus
anconeus
![]() brachioradialis
brachioradialis
![]() extensor carpi radialis longus & brevis (latter originates ≈ at terminal branch)
extensor carpi radialis longus & brevis (latter originates ≈ at terminal branch)
![]() supinator (originates near the terminal branch)
supinator (originates near the terminal branch)
![]() continues into forearm as posterior interosseous nerve (C7, C8)
continues into forearm as posterior interosseous nerve (C7, C8)
![]() extensor carpi ulnaris
extensor carpi ulnaris
![]() extensor digitorum
extensor digitorum
![]() extensor digiti minimi
extensor digiti minimi
![]() extensor pollicis brevis & longus
extensor pollicis brevis & longus
![]() abductor pollicis longus
abductor pollicis longus
![]() extensor indicus
extensor indicus
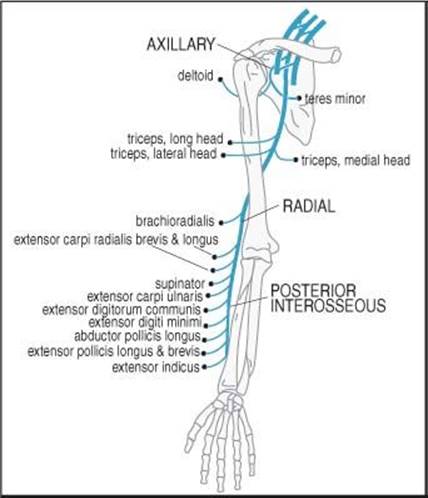
Figure 24-2 Muscles of the radial and axillary nerves
Axillary nerve (C5, C6)
See Figure 24-2.
![]() teres minor
teres minor
![]() deltoid
deltoid
Median nerve (C5-T1)A
A. also, see page 792 for Martin-Gruber anastomosis
See Figure 24-3.
1. nothing in arm
2. all forearm pronators and flexors except the two supplied by ulnar nerve
![]() pronator teres
pronator teres
![]() flexor carpi radialis
flexor carpi radialis
![]() palmaris longus
palmaris longus
![]() flexor digitorum superficialis
flexor digitorum superficialis
3. in the hand ⇒ only the “LOAF muscles”
![]() L umbricals 1 & 2
L umbricals 1 & 2
![]() O pponens pollicis
O pponens pollicis
![]() A bductor pollicis brevis
A bductor pollicis brevis
![]() F lexor pollicis brevis (C8, T1)
F lexor pollicis brevis (C8, T1)
![]() branch at or just distal to elbow anterior interosseous nerve (purely motor)
branch at or just distal to elbow anterior interosseous nerve (purely motor)

Figure 24-3 Muscles of the median and ulnar nerves
![]() flexor digitorum profundus I & II
flexor digitorum profundus I & II
![]() flexor pollicis longus
flexor pollicis longus
![]() pronator quadratus
pronator quadratus
Ulnar nerve (C8, T1)A
See Figure 24-3.
1. nothing in arm
2. only 2 muscles in forearm:
![]() flexor carpi ulnaris
flexor carpi ulnaris
![]() half of flexor digitorum profundus (parts III & IV)
half of flexor digitorum profundus (parts III & IV)
3. all hand muscles excluding “LOAF” muscles (see above), viz.:
![]() adductor pollicis
adductor pollicis
![]() all interossei (4 dorsal & 3 palmar)
all interossei (4 dorsal & 3 palmar)
![]() lumbricals 3 & 4
lumbricals 3 & 4
![]() 3 hypothenar muscles: abductor, opponens & flexor digiti minimi
3 hypothenar muscles: abductor, opponens & flexor digiti minimi
![]() deep part of flexor pollicis brevis (by deep branch of ulnar nerve)
deep part of flexor pollicis brevis (by deep branch of ulnar nerve)
![]() palmaris brevis (by the superficial branch of the ulnar nerve)
palmaris brevis (by the superficial branch of the ulnar nerve)
Musculocutaneous nerve (C5, C6)
Supplies arm flexors
![]() coracobrachialis
coracobrachialis
![]() biceps
biceps
![]() brachialis
brachialis
![]() lateral cutaneous nerve of the forearm (terminal branch) supplies cutaneous sensation to radial aspect of forearm
lateral cutaneous nerve of the forearm (terminal branch) supplies cutaneous sensation to radial aspect of forearm
Dorsal scapular nerve (C4, C5)
![]() rhomboids (major & minor)
rhomboids (major & minor)
![]() levator scapulae
levator scapulae
Suprascapular nerve (C5, C6)
![]() supraspinatus
supraspinatus
![]() infraspinatus
infraspinatus
Subscapular nerve (C5-7)
![]() teres major
teres major
![]() subscapularis
subscapularis
Thoracodorsal nerve (C6, C7, C8)
![]() latissimus dorsi
latissimus dorsi
Long thoracic nerve (C5-7)
Originates off of proximal nerve roots
![]() serratus anterior (holds scapula to chest wall): lesion → winging of the scapulaA (to test: patient leans forward against wall with arms outstretched, scapula separates from posterior chest wall if the serratus anterior is not contracting)
serratus anterior (holds scapula to chest wall): lesion → winging of the scapulaA (to test: patient leans forward against wall with arms outstretched, scapula separates from posterior chest wall if the serratus anterior is not contracting)
A. this is classic winging of the scapula. A variant of winging can occur with loss of trapezius muscle (e.g. with accessory nerve injury), and typically manifests when the patient pushes forward with the elbow held at the side of the thorax
Anatomic variants
Martin-Gruber anastomosis5: Anastomosis between median and ulnar nerves in the forearm found in 16 of 70 (23%) cadavers, bilateral in 3 (19%). Pattern I (90%): 1 anastomotic branch, Pattern II (10%) had 2.
Classification based on the origin from the median nerve: Type a (47.3%) from the branch to the superficial forearm flexor muscles, Type b (10.6%) from the common trunk, and Type c (31.6%) from the anterior interosseous nerve. Pattern II was a duplication of Type c (10.5%). The anastomotic branch was undivided in 15 cases, and divided into two branches in four cases. The anastomosis took an oblique angle or arched course to the ulnar nerve and passed superficial to the ulnar artery in four cases, deep to it in six, and in nine cases it was related to the anterior ulnar recurrent artery5.
Richie-Cannieu anastomosis: Motor connections from median to ulnar nerve at the palm. Found in 70% of patients.
24.3. Peripheral neuropathies
Definitions
|
peripheral neuropathy |
(the term polyneuropathy is also sometimes used) diffuse lesions of peripheral nerves producing weakness, sensory disturbance, and/or reflex changes |
|
mononeuropathy |
a disorder of a single nerve, often due to trauma or entrapment |
|
mononeuropathy multiplex |
involvement of 2 or more nerves, usually due to a systemic abnormality (e.g. vasculitis, rheumatoid arthritis, DM…). Treatment is directed at the underlying disorder |
A mnemonic for etiologies of peripheral neuropathies is “GRAND THERAPIST” (see Table 24-8). Diabetes, alcoholism, and Guillain-Barré (underscored in table) account for 90% of cases. Other etiologies include: arteritis/vasculitis, monoclonal gammopathy (see page 799), hepatitis C virus-associated cryoglobulinemia, acute idiopathic polyneuritis, Sjögren’s syndrome (disease).
Table 24-8 Mnemonic for etiologies of peripheral neuropathy
|
Guillain-Barré (see page 66) Renal (uremic neuropathy -see page 800) Alcoholism (see below) Nutritional (B12 deficiency…) Diabetes (see below) or Drugs (see page 797) |
Traumatic Hereditary Endocrine or Entrapment Radiation Amyloid (see page 800) or AIDS (see page 798) Porphyria or Psychiatric or Paraneoplastic (see below) or Pseudoneuropathy (see below) or PMR (see page 75) Infectious/post-infectious (e.g. Hansen’s disease) Sarcoidosis (neurosarcoidosis, see page 71) or “Systemic” Toxins (including heavy metals, e.g lead toxicity (plum-bism), see page 998) |
Clinical
Peripheral neuropathies can present as loss of sensation, pain, weakness, incoordination and difficulty ambulating.
Evaluation
Initial (generic) work-up for peripheral neuropathies of unknown etiology:
1. bloodwork: Hgb-A1C, TSH, ESR and vitamin B12
2. EMG
Classification
1. inherited neuropathies
A. Charcot-Marie-Tooth (CMT) (AKA peroneal muscular atrophy, AKA Hereditary Motor and Sensory Neuropathy (HMSN)): Up to 7 types, (the most common form is autosomal dominant, but X-linked recessive forms also exist). CMT Types 1 & 2 together make up the most common inherited disorder of peripheral nerves (up to 40/100,000). The most common forms involve demyelination. Progressive loss of motor (primarily distal LE) and, to a lesser degree, sensory function (predominantly proprioception and vibration), with atrophy in UEs & LEs. Earliest findings: pes cavus with hammer toes, foot drop and frequent ankle sprains. Patients are more susceptible to entrapment neuropathies due to underlying compromise of peripheral nerves. Patients with Type 1 usual maintain ability to ambulate, whereas Type 2 usually lose ambulation by their teenage years
B. hereditary neuropathy with liability to pressure palsies (HNPP): similar to CMT but due to focal areas of irregular thickening of myelin sheaths (“tomaculous” changes), mild trauma or pressure can produce nerve palsies that may last for months
2. acquired neuropathies: see sections below for details
A. acquired pure sensory neuropathies (in the absence of autonomic dysfunction) are rare. May be seen with pyridoxine therapy or paraneoplastic syndromes (see below)
B. entrapment neuropathies: see page 804
3. pseudoneuropathy
A. definition: psychogenic somatoform disorders or malingering, reproducing the pains, paresthesias, hyperalgesia, weakness, and even objective findings such as changes in color and temperature which may mimic neuropathic symptoms6
CRITICAL ILLNESS POLYNEUROPATHY (CIP)
AKA neuropathy of critical illness, ICU neuropathy… For DDx, see page 68 under Guillain-Barré syndrome.
Diagnostic criteria:
1. presence of sepsis, multi-organ failure, respiratory failure, or septic inflammatory response syndrome (SIRS)
2. difficulty weaning from ventilator or extremity weakness
3. EMG: ↓ amplitudes of compound muscle action potentials (CMAP) & SNAP
4. widespread muscle denervation potentials
5. normal or only mild increase in serum CPK levels
May occur in up to 70% of septic patients (not all are significantly symptomatic). Affects primarily distal muscles. Recovery occurs in weeks to months (faster than Guillain-Barré). Treatment is supportive. Complete recovery in 50%
PARANEOPLASTIC SYNDROMES AFFECTING THE NERVOUS SYSTEM
Occurs in < 1% of cancer patients. Peripheral sensory neuropathy of unknown etiology has been associated with cancer since its earliest description7. Therefore, in patients with sensory neuropathy of unknown etiology, occult neoplasms should be ruled out. If the work-up is negative, the patient should be followed since up to 35% of patients will be found to have cancer after a mean interval of 28 months 8.
ALCOHOL NEUROPATHY
Characteristically produces a diffuse sensory neuropathy, with absent achilles reflexes.
BRACHIAL PLEXUS NEUROPATHY9 (918)
Differential diagnosis of etiologies of brachial plexopathy:
1. Pancoast syndrome or Pancoast tumor AKA superior sulcus tumor. Clinical: various combinations of pain in the shoulder radiating into the upper extremity in the ulnar nerve distribution from involvement of the lower brachial plexus, atrophy of hand muscles, Horner’s syndrome (see page 833), UE edema. Etiologies:
A. neoplasms:
1. most common: bronchogenic cancer, usually non-small cell (NSCLC) (squamous cell or adenocarcinoma) arising in the pulmonary apex
2. metastases
B. infections
C. inflammatory: granulomas, amyloid
2. (idiopathic) brachial plexitis: most commonly upper plexus or diffuse (see below)
3. cervical rib
4. viral
5. following radiation treatment: often diffuse (see below)
6. diabetes
7. vasculitis
8. inherited: dominant genetics
9. trauma (see page 801)
Evaluation: when the etiology is unclear, check CXR (with apical lordotic view), glucose, ESR and ANA. Idiopathic brachial plexitis will usually start to show some improvement by about 4 weeks. Obtain MRI through the plexus if no improvement by ≈ this time.
NEURALGIC AMYOTROPHY OF THE UPPER EXTREMITY
AKA idiopathic brachial plexus neuropathy AKA (paralytic) brachial neuritis, AKA brachial plexitis, AKA Parsonage-Turner syndrome10, among others. Idiopathic. Not clearly infectious or inflammatory; allergic mechanism possible. Prognosis is generally good. Common patterns: single or multiple mononeuropathy, plexopathy, or some combination. Demographics are shown in Table 24-9.
In a review of 99 cases11: predominant symptom is acute onset of intense pain, with weakness developing simultaneously or after a variable period (70% occur within 2 weeks of pain) usually as the pain lessened10, 12. Weakness never preceded pain, onset of weakness was sudden in 80%. Pain was usually constant, and described as “sharp”, “stabbing”, “throbbing” or “aching”. Arm movement exacerbated pain, and muscle soreness was noted in 15%. Pain lasted hours to several weeks. Paresthesias occurred in 35%. Pain usually lacked radicular features. When bilateral, weakness is usually asymmetric.
Exam
Weakness or paralysis in 96%, confined to shoulder girdle in 50%. In descending order of involvement: deltoid, spinati, serratus anterior, biceps brachii, and triceps. Winging of the scapula occurred in 20%. Sensory loss occurred in 60% of plexus lesions, of mixed variety (superficial cutaneous and proprioceptive). Sensory loss most common in outer surface of upper arm (circumflex nerve distribution) and radial aspect of forearm. Reflexes were variable.
Overall distribution judged to predominantly involve upper plexus in 56%, diffuse plexus in 38%, and lower in 6%.
Table 24-9 Neuralgic amyotrophy
|
incidence |
1.64 per 100,000 population |
|
male:female |
2.4:1 |
|
age range at onset |
3 mos - 75 years |
|
prodrome |
• ≈ 45% had viral prodrome (URI in 25%) • may follow vaccination |
|
onset |
rapid onset of pain or paralysis/paresis |
|
initial symptom |
pain in 95% |
|
weakness |
• 50% confined to shoulder girdle • 10% confined to a single peripheral nerve |
|
sensory deficit |
67%, usually axillary and antebrachial cutaneous |
|
laterality |
• 66% unilateral (right side 54%) • 34% bilateral |
|
lab tests |
normal |
EMG/NCV
May help localize the portion of the plexus involved, and may detect subclinical involvement of the contralateral extremity. Must wait ≥ 3 weeks from onset for findings. Differentiating from cervical radiculopathy: SNAP should be normal in radiculopathy whereas some involvement usually occurs in plexitis. Cervical paraspinals will usually be normal in plexitis (except for very severe cases where there can be some retrograde involvement), and will be abnormal (fibrillations) in radiculopathy (except in cases where there has been enough time that significant recovery has occurred).
Outcome
Functional recovery is better in patients with primarily upper plexus involvement. After 1 year, 60% of upper plexus lesions were functioning normally, whereas none with lower involvement were (latter took 1.5-3 years). Rate of recovery estimated to be 36% within 1 year, 75% within 2, and 89% by 3 years. Recurrence was seen in only 5%. No evidence that steroids altered the course of the disease although it is still often prescribed in the acute phase.
RADIATION INDUCED BRACHIAL PLEXUS NEUROPATHY
Often follows external beam irradiation in the region of the axilla for breast carcinoma. Produces sensory loss with or without weakness. CT or MRI or biopsy may be needed to rule-out tumor invasion of the brachial plexus.
LUMBOSACRAL PLEXUS NEUROPATHY13
Analogous to idiopathic brachial plexitis (see above). It is controversial whether this actually exists in isolation without diabetes. Often starts with LE pain of abrupt onset, followed in days or a few weeks by weakness with or without muscle atrophy. Sensory symptoms are less prominent, and usually involve paresthesias. Objective sensory loss is only occasionally seen. There may be tenderness over the femoral nerve.
Differential diagnosis
May be confused with femoral neuropathy or L4 radiculopathy when quadriceps weakness and wasting occurs. Similarly, L5 radiculopathy or peroneal neuropathy may be erroneously suspected when foot drop is seen. Straight leg raising may occasionally be positive. Conspicuously absent are: back pain, exacerbation of pain by Valsalva maneuver or back motion, and significant sensory involvement. For differential diagnosis of foot drop, see page 1194. For other causes of sciatica, see page 1188.
Etiologies
Other etiologies are similar to that for brachial plexus neuropathy (see above) except that under tumor, a pelvic mass should be considered (check prostate on rectal exam).
Evaluation
Evaluation is as for brachial plexus neuropathy (see above), except that instead of a brachial plexus MRI, a lumbar MRI and pelvic CT should be done to rule out masses.
EMG is key to diagnosis: evidence of patchy denervation (fibrillation potentials, and motor unit potentials that are either decreased in number or increased in amplitude or duration and polyphasic) involving at least 2 segmental levels with sparing of the paraspinal muscles is highly diagnostic (once diabetes, etc. have been ruled-out).
Recovery from pain precedes return of strength. Improvement is generally monophasic, slow (years), and incomplete.
DIABETIC NEUROPATHY
≈ 50% of patients with DM develop neuropathic symptoms or show slowing of nerve conduction velocities on electrodiagnostic testing. Neuropathy may sometimes be the initial manifestation of diabetes. Diabetic neuropathy is reduced by tight control of blood glucose14. Disagreement exists over the number of distinct clinical syndromes; there is probably a continuum15 and they likely occur in various combinations. Some of the more readily identified syndromes include:
1. primary sensory polyneuropathy: symmetric, affecting feet and legs more than hands. Chronic, slowly-progressive. Often with accelerated loss of distal vibratory sense (normal loss with aging is ≈ 1% per year after age 40). Presents as pain, paresthesias, and dysesthesias. Soles of feet may be tender to pressure. Meralgia paresthetica (see page 818) may be first manifestation
2. autonomic neuropathy: involving bladder, bowel, and circulatory reflexes (resulting in orthostatic hypotension). May produce impotence, impaired micturition, diarrhea, constipation, impaired pupillary light response
3. diabetic plexus neuropathy 16 or proximal neuropathy: possibly secondary to vascular injury to nerves (similar to a diabetic mononeuritis):
A. one that occurs in patients > 50 years old with mild diabetes type II that is often confused with femoral neuropathy. Causes severe pain in the hip, anterior thigh, knee, and sometimes medial calf. Weakness of the quadriceps, iliopsoas, and occasionally thigh adductors. Loss of knee jerk. Possible sensory loss over medial thigh and lower leg. Pain usually improves in weeks, the weakness in months
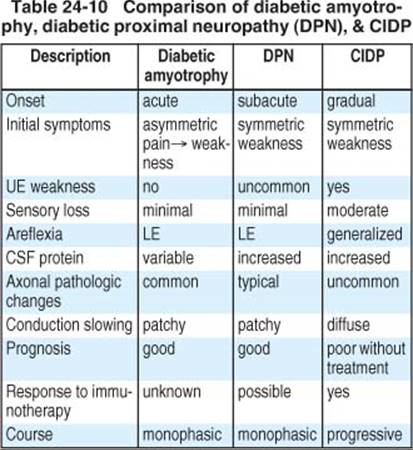
![]() B. diabetic amyotrophy: occurs in similar patient population often with recently diagnosed DM. Alternative names include17: Bruns-Garland syndrome, ischemic mononeuropathy multiplex…18. Abrupt onset of asymmetric pain (usually deep aching/burning with superimposed lancinating paroxysms, most severe at night) in back, hip, buttocks, thigh, or leg. Progressive weakness in proximal or proximal and distal muscles, often preceded by weight loss. Patellar reflexes are absent or reduced. Sensory loss is minimal. Proximal muscles (especially thigh) may atrophy. EMG findings consistent with demyelination invariably accompanied by axonal degeneration, with involvement of paraspinals and no evidence of myopathy. Symptoms may progress steadily or stepwise for weeks or even up to 18 months, and then gradually resolve. Opposite extremity may become involved during the course or may occur months or years later. Sural nerve biopsy may suggest demyelination
B. diabetic amyotrophy: occurs in similar patient population often with recently diagnosed DM. Alternative names include17: Bruns-Garland syndrome, ischemic mononeuropathy multiplex…18. Abrupt onset of asymmetric pain (usually deep aching/burning with superimposed lancinating paroxysms, most severe at night) in back, hip, buttocks, thigh, or leg. Progressive weakness in proximal or proximal and distal muscles, often preceded by weight loss. Patellar reflexes are absent or reduced. Sensory loss is minimal. Proximal muscles (especially thigh) may atrophy. EMG findings consistent with demyelination invariably accompanied by axonal degeneration, with involvement of paraspinals and no evidence of myopathy. Symptoms may progress steadily or stepwise for weeks or even up to 18 months, and then gradually resolve. Opposite extremity may become involved during the course or may occur months or years later. Sural nerve biopsy may suggest demyelination
C. diabetic proximal neuropathy (DPN): fairly similar findings to diabetic amyotrophy except for subacute onset of symmetric LE involvement that usually start with weakness may be a variant19. Table 24-10(adapted19) compares DPN to diabetic amyotrophy and chronic inflammatory demyelinating polyradiculoneuropathy (CIDP)
TREATMENT
Treatment of Bruns-Garland syndrome is primarily expectant, although immunotherapy (steroids, immune globulin, or plasma exchange) may be considered in severe or progressive cases (efficacy is unproven)19.
For sensory polyneuropathy, good control of blood sugar contributes to reduction of symptoms. Adjunctive agents that have been used include:
1. mexiletine (Mexitil®): start at 150 mg q 8 hrs, and titrate to symptoms to a maximum of 10 mg/kg/d
2. amitriptyline (Elavil®) and fluphenazine (Prolix-in®): Rx: start with 25 mg amitriptyline PO q hs and 1 mg fluphenazine PO TID; and work up to 75 mg amitriptyline PO q hs20 (≈ 100 mg qd amitriptyline alone may also be effective21). Usefulness has been challenged22, but many studies do show benefit21, 23. SIDE EFFECTS: that may limit use include sedation, confusion, fatigue, malaise, hypomania, rash, urinary retention, and orthostatic hypotension
3. desipramine (Norpramin®): more selective blocker of norepinephrine reuptake (which seems more effective for this condition than serotonin reuptake blockers). Effectiveness at mean doses of 110 mg/day ≈ same as amitriptyline and therefore may be useful for patients unable to tolerate amitriptyline21. SIDE EFFECTS: include insomnia (may be minimized by AM dosing), orthostatic hypotension, rash, bundle branch block, tremor, pyrexia. SUPPLIED: 10, 25, 50, 75, 100 & 150 mg tablets
4. capsaicin (Zostrix®): effective in some (see Capsaicin, on page 566)
5. paroxetine (Paxil®): a selective serotonin reuptake inhibitor (SSRI) antidepressant. Rx: 20 mg PO q AM. If necessary, increase by 10 mg/d q week up to a maximum of 50 mg/day (except in elderly, debilitated, or renal or hepatic failure where maximum is 40 mg/day). SUPPLIED: 20 mg (scored) & 30 mg tablets
6. gabapentin (Neurontin®) doses of 1800-3600 mg/d produces at least moderate pain relief from painful diabetic neuropathy in 60% of patients24 and was ≈ as efficacious as amitriptyline25. Dosage must be reduced with renal insufficiency. For details, see page 416
7. pregabalin (Lyrica®) Rx: start with 50 mg TID and increase up to a maximum of 100 mg PO TID within 1 week in patients with creatinine clearance ≥ 60 ml/min (see Eq 3-1, page 46 to estimate). Dosage must be reduced with renal insufficiency. SUPPLIED: 25, 50, 75, 100, 150, 200, 225, 300 mg capsules
DRUG INDUCED NEUROPATHY
Many drugs have been implicated as possible causes of peripheral neuropathy. Those that are better established or more notorious include:
1. thalidomide: neuropathy may occur with chronic use, and may be irreversible26
2. metronidazole (Flagyl®)
3. phenytoin (Dilantin®)
4. amitriptyline (Elavil®)
5. dapsone: a rare complication reported with use in nonleprosy patients is a reversible peripheral neuropathy that may be due to axonal degeneration, producing a Guillain-Barré-like syndrome (see page 66for Guillain-Barré syndrome)
6. nitrofurantoin (Macrodantin®): may additionally cause optic neuritis
7. cholesterol lowering drugs: e.g. lovastatin (Mevacor®), indapamide (Lozol®), gemfibrozil (Lopid®)
8. thallium: may produce tremors, leg pains, paresthesias in the hands and feet, polyneuritis in the LE, psychosis, delerium, seizures, encephalopathy
9. arsenic: may produce numbness, burning and tingling of the extremities
10. chemotherapy: cisplatin, vincristine…
FEMORAL NEUROPATHY
Manifests as:
1. motor deficits:
A. wasting and weakness of the quadriceps femoris (knee extension)
B. weakness of iliopsoas (hip flexion): if present, indicates very proximal pathology (lumbar root or plexus lesion) as the branches to the iliopsoas arise just distal to the neural foramina
2. diminution of the patellar (knee jerk) reflex
3. sensory findings:
A. sensory loss over the anterior thigh and medial calf
B. pain in same distribution may occur
4. mechanical signs: positive femoral stretch test (see page 444)
Differential diagnosis:
1. L4 radiculopathy: L4 radiculopathy should not cause iliopsoas weakness (see L4 involvement, page 1190)
2. diabetic plexus neuropathy (see Diabetic neuropathy above)
3. (idiopathic) lumbosacral plexus neuropathy (see above)
Etiologies:
1. diabetes: the most frequent cause
2. femoral nerve entrapment: rare
A. may occur secondary to inguinal hernia or may be injured by deep sutures placed during herniorrhaphy
B. secondary to prolonged pelvic surgery from retractor compression (usually bilateral)
3. intraabdominal tumor
4. femoral arterial catheterization: see Neuropathy after cardiac catheterization below
5. retroperitoneal hematoma (e.g. in hemophiliac or on anticoagulants)
6. during surgery (see page 800)
AIDS NEUROPATHY
3.3% of patients with AIDS will develop peripheral nerve disorders27 (whereas none who were just HIV positive developed neuropathy). The most common disorder is distal symmetric polyneuropathy (DSP), usually consisting of vague numbness and tingling, and sometimes painful feet (although it may also be painless). There may be subtle reduction of light tough and vibratory sense. Other neuropathies include mononeuropathies (usually meralgia paresthetica, see page 818), mononeuropathy multiplex, or lumbar polyradiculopathy. Drugs used to treat HIV can also cause neuropathies (see below).
The DSP in AIDS patients is often associated with CMV infection, Mycobacterium avium intracellulare infection, or may be due to lymphomatous invasion of the nerve or lymphomatous meningitis. May demonstrate a mixed axonal demyelinating type of neuropathy on electrodiagnostic testing.
Neuropathies associated with drugs used to treat HIV:
1. nucleoside reverse transcriptase inhibitors
A. zidovudine (Retrovir®) (formerly AZT)
B. didanosine (ddI; Videx®): can cause a painful dose-related neuropathy28
C. stavudine (d4T; Zerit®): can cause sensory neuropathy which usually improves when d4T is discontinued, and may not recur if restarted at lower dose28
D. zalcitabine (ddC; Hivid®): dose-related neuropathy can be severe and persistent. More common in patients with DM or didanosine treatment28
2. protease inhibitors
A. ritonavir (Norvir®): can cause peripheral paresthesias
B. amprenavir (Agenerase®): can cause perioral paresthesias
NEUROPATHY ASSOCIATED WITH MONOCLONAL GAMMOPATHY
Monoclonal gammopathies include myeloma (see page 740), Waldenstrom’s macroglobulinemia, and non-malignant entities such as monoclonal gammopathy of undetermined significance (MGUS). Much effort has gone into determining which benign gammopathies are or are not likely to progress, and will not be addressed here.
≈ 10% of patients with neuropathy with no apparent etiology will be determined to have a monoclonal gammopathy (malignant or otherwise).
Etiologies:
1. antibodies directed primarily against oligosaccharides of peripheral nerves, e.g. myelin associated glycoprotein (MAG), producing demyelinating neuropathy
2. cryoglobulins may damage vaso-nervorum (small blood vessels nourishing peripheral nerves)
3. in malignant gammopathies, tumor cells can invade the peripheral nerves (lymphomatosis)
4. amyloidosis: deposition of amyloid in peripheral nerves (see page 800)
5. thalidomide used to treat some myelomas may cause neuropathy (see page 797)
Treatment:
1. IgM monoclonal gammopathies: reduce the IgM antibody concentration
2. IgG or IgA monoclonal gammopathies:
A. treatment for myeloma related neuropathy is directed at treating the myeloma
B. solitary plasmacytoma: excision or XRT can improve the neuropathy
PERIOPERATIVE NEUROPATHIES
Also, see Neuropathy after cardiac catheterization below. Most often involves ulnar nerve or brachial plexus. In many cases, a nerve that is abnormal but asymptomatic may become symptomatic as a result of any of the following factors: stretch or compression of the nerve, generalized ischemia or metabolic derangement. The injury may be permanent or temporary. Occurs almost exclusively in adults29.
1. ulnar neuropathy: controversial. Often blamed on external nerve compression or stretch as a result of malpositioning. Although this may be true in some cases, in one series this was a factor in only ≈ 17%30. Patient-related characteristics are shown in Table 24-1131. Many of these patients have abnormal contralateral nerve conduction, suggesting a possible predisposing condition32. Many patients do not complain of symptoms until > 48 hours post-op31-33. Risk may be reduced by padding the arm at, and especially distal to, the elbow, and avoiding flexion of the elbow (avoid > 110° flexion which tightens the cubital tunnel retinaculum) and by reducing the amount of time convalescing in the recumbent position33
2. brachial plexus neuropathy: may be mistaken for ulnar neuropathy. May be associated with:
A. median sternotomy (most common with internal mammary dissection). Posterior sternal retraction displaces the upper ribs and may stretch or compress the C6 through T1 roots (major contributors to the ulnar nerve)
B. head-down positions where the patient is stabilized with a shoulder brace. The brace should be placed over the acromioclavicular joint(s), and non-slip mattresses and flexion of the knees may be used as adjuncts29
C. prone position (rare): especially with shoulder abduction and elbow flexion with contralateral head rotation29
3. median neuropathy: perioperative median nerve injury may result from stretch of the nerve. Rare. Seems to occur primarily in middle-aged muscular males. Padding should be placed under the forearms and hands to maintain mild elbow flexion29
4. lower extremity neuropathies: most occur in patients undergoing procedures in the lithotomy position29. Frequency of involvement in a large series of patients undergoing procedures in the lithotomy position34: common peroneal 81%, sciatic 15%, and femoral 4%. Risk factors other than position: prolonged duration of procedure, extremely thin body habitus, and cigarette smoking in the preoperative period
Table 24-11 Patient-related characteristics in anesthesia-related ulnar neuropathy
|
male gender |
|
obesity (body mass index ≥ 38) |
|
prolonged post-op bed rest |
A. common peroneal neuropathy: susceptible to injury in the posterior popliteal fossa where it wraps around the fibular head. May be compressed by leg holders, which should be padded in this area
B. femoral neuropathy: compression of the nerve by self-retaining abdominal wall retractor or rendering the nerve ischemic by occlusion of the external iliac artery29. Hemorrhage into the iliopsoas muscle may also compress the nerve. Cutaneous branches of the femoral nerve may be injured during labor and/or delivery35 (most are transient)
C. sciatic neuropathy: stretch injuries may occur with hyperflexion of the hip and extension of the knee as may occur in the lithotomy position
D. meralgia paresthetica36: tends to occur bilaterally in young, slender males positioned prone, with operations lasting 6-10+ hours. Onset: 1-8 days postop. Spontaneous recovery typically occurs over an average of 5.8 months
Management
Once a neuropathy is detected, determine if it is sensory, motor, or both. Pure sensory neuropathies are more often temporary than motor31, and expectant management for ≈ 5 days is suggested (have the patient avoid postures or activities that may further injure the nerve). Neurologic consultation should be requested for all motor neuropathies and for sensory neuropathies persisting > 5 days29 (EMG evaluation will not usually be helpful earlier than ≈ 3 weeks after onset).
OTHER NEUROPATHIES
Amyloid neuropathy
Amyloid is an insoluble extracellular protein aggregate that can be deposited in peripheral nerves. Amyloidosis occurs in a number of conditions, e.g. in ≈ 15% of patients with multiple myeloma (also, see page 740). The neuropathy predominantly produces a progressive autonomic neuropathy and symmetric dissociated sensory loss (reduced pain and temperature, preserved vibratory sense). There is usually less prominent motor involvement. May predispose to pressure injury of nerves (especially carpal tunnel syndrome, see page 810 for laboratory tests).
Uremic neuropathy
Occurs in chronic renal failure. Early symptoms include calf cramps (“Charlie horses”), dysesthetic pain in feet (similar to painful diabetic neuropathy) and “restless legs”. Achilles reflexes are lost. A stocking sensory loss is followed later by LE weakness that starts distally and ascends. The offending toxin is not known. Dialysis or renal transplantation relieves the symptoms.
Neuropathy after cardiac catheterization
In a series of ≈ 10,000 patients followed after femoral artery catheterization37 (e.g. for coronary angiography or angioplasty), neuropathy occurred in 0.2% (with an estimated range in the literature up to ≈ 3%). Risk factors identified include: patients developing retroperitoneal hematomas or pseudoaneurysms after the procedure, procedures requiring larger introducer sheaths (e.g. angioplasty & stent placement > diagnostic catheterization), excessive anticoagulation (PTT > 90 for at least 12 hours).
Two groups of patients were identified and are shown in Table 24-12.
Excruciating pain after the catheterization procedure often preceded the development or recognition of neuropathy.
Table 24-12 Neuropathy after cardiac catheterization (N = 9585)37
|
Catheterization complication |
Neurologic complication |
|
Group I (4 patients) |
|
|
groin hematoma or pseudoaneurysm |
sensory neuropathy in all 4 cases • in distribution of medial & intermediate femoral cutaneous nerves → isolated sensory neuropathy (dysesthesia & sensory loss) of the anterior and medial thigh • no motor deficit |
|
Group II (16 patients) |
|
|
large retroperitoneal hematoma |
femoral neuropathy • sensory in all 16 cases: dysesthesia of the anterior/medial thigh & medial calf • motor in 13 cases: iliopsoas & quadriceps weakness |
|
obturator neuropathy in 4 cases • sensory: upper medial thigh • motor: obturator weakness |
|
|
lateral femoral cutaneous nerve → meralgia paresthetica |
|
Treatment:
After considering available information, the recommendation is to repair pseudoaneurysms surgically, but to treat the neuropathy conservatively. A case could not be made that surgical drainage of hematoma reduced the risk of neuropathy. Weakness from femoral or obturator neuropathy was treated with inpatient rehabilitation.
Outcome:
Group I patients all had resolution in < 5 mos. In group II, 50% had complete resolution in 2 mos. 6 patients had persistent symptoms, 5 had mild femoral sensory neuropathy (1 of whom felt it was at least somewhat disabling), 1 had mild persistent quadriceps weakness and occasionally walks with a cane.
PERIPHERAL NERVE INJURIES
ANATOMY OF PERIPHERAL NERVES (see Figure 24-4)
Endoneurium surrounds myelinated and unmyelinated axons. These bundles are gathered into fascicles surrounded by perineurium. The epineurium encases the nerve trunk, containing fascicles separated by interfascicular epineurium or mesoneurium.
NERVE REGENERATION
Peripheral nerves regenerate ≈ 1 mm/day (about 1 inch/month). Divide this figure into distance that the nerve has to traverse (from knowledge of anatomy) for guide as to how long to wait before considering failure of therapy (either operative or non-operative). However, this rule may not be applicable to long distances (> ≈ 12 inches), and it may take longer to traverse regions of entrapment, scar or nerve injury. There may also be fibrosis of the muscle beyond salvage.
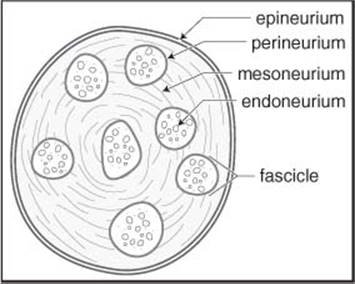
Figure 24-4 Anatomy of a peripheral nerve
PERIPHERAL NERVE INJURY CLASSIFICATION
There are numerous classification systems. The Seddon classification is an older 3-tiered system, The Sunderland system has 5 tiers, essentially dividing axonotmesis into 3 subgroups. Others have added a 6th category as shown in Table 24-13.
BRACHIAL PLEXUS INJURIES
Etiologies include:
1. penetrating trauma
2. traction (stretch injuries): more likely to affect the posterior and lateral cords than the medial cord and median nerve
3. first rib fractures
4. compression by hematoma
Initial exam seeks to differentiate preganglionic injuries (proximal to dorsal root ganglion) which cannot be repaired surgically, from postganglionic injuries. Clues to a preganglionic injury include:
1. Horner’s syndrome: pre-ganglionic injury interrupts white rami communicantes
2. paralysis of serratus anterior (long thoracic nerve): produces winging of scapula
3. paralysis of rhomboids (dorsal scapular nerve)
4. early neuropathic pain suggests nerve root avulsion. MRI or myelogram will show pseudomeningoceles at the avulsed levels
5. EMG: requires ≥ 3 weeks from injury for some findings. Look for:
A. denervation potentials in paraspinal muscles due to loss of neural input. The posterior ramus of the spinal nerve originates just distal to the dorsal root ganglion. Due to overlap, cannot localize to a specific segment
B. normal sensory nerve action potential (SNAP): preganglionic injuries leave the dorsal ganglion sensory cell body and the distal axon intact, so that normal SNAP can be recorded proximally even in an anesthetic region
6. pseudomeningocele on myelography or MRI: suggests nerve root avulsion (very proximal), however, 15% of pseudomeningoceles are not associated with avulsions, and 20% of avulsions do not have pseudomeningoceles38, 39
Table 24-13 Classification of peripheral nerve injury*
|
Seddon system |
Sunderland system |
|
Neuropraxia |
First-degree |
|
Features common to both systems Physiologic transection (nerve in continuity). Basement membrane intact. Compression or ischemia → local conduction block (impaired axonal transport). |
|
|
Recovers in hours to months; average is 6-8 weeks |
Focal demyelination may occur. Recovery is usually complete in 2-3 weeks (not the “1 mm/day rule”) |
|
Axonotmesis |
Second-degree |
|
Features common to both systems Complete interruption of axons and myelin sheaths. Supporting structures (including endoneurium) intact. |
|
|
Recovers at 1 mm/day as axon follows “tubule”. Sometimes may only be diagnosed retrospectively. Recovery is poor in lesions requiring > 18 months to reach target muscle |
|
|
Third-degree |
|
|
Endoneurium disrupted, epineurium & perineurium intact. Nerve may not appear seriously damaged on gross inspection. Recovery may range from poor to complete and depends on degree of intrafascicular fibrosis |
|
|
Fourth-degree |
|
|
Interruption of all neural & supporting elements. Epineurium intact. Grossly: nerve is usually indurated & enlarged |
|
|
Neurotmesis |
Fifth-degree |
|
Nerve completely severed or disorganized by scar tissue. Spontaneous regeneration impossible |
Complete transection with loss of continuity |
|
Sixth-degree‡ |
|
|
Mixed lesion. Combination of elements of first through fourth degree. There may be some preserved sensory fascicles (may produce a positive Tinel’s sign) |
|
* comparing and showing approximate equivalence of Seddon and Sunderland systems
† wallerian degeneration AKA orthograde degeneration, AKA secondary degeneration: degeneration of the axon distal to a focal lesion
‡ not part of original Sunderland system
(Duchene)-Erb’s palsy
Upper brachial plexus injury (C5 & 6, some authors include C7) e.g. from forceful separation of humeral head from shoulder, commonly due to difficult parturition (see below) or motorcycle accident (downward force on shoulder can cause traumatic nerve root avulsion from the spinal cord). Paralysis of deltoid, biceps, rhomboids, brachioradialis, supra- & infraspinatus, and occasionally supinator. C7 involvement produces weak wrist extension.
Motor: arm hangs at side internally rotated & extended at elbow and flexed at the wrist (“Bellhop’s tip position”). Hand motion is unaffected.
Klumpke’s palsy
Injury to lower brachial plexus (C8 & T1, some authors include C7), from traction of abducted arm e.g. in catching onesulf during a fall from a height, or by Pancoast tumor (lung apex tumor - check CXR with apical lordotic view). Characteristic claw deformity (also seen with ulnar nerve injury) with weakness and wasting of small hand muscles. Possible Horner’s syndrome if T1 involved.
Birth brachial plexus injury (BBPI)
Incidence is 0.3-2.0 per 1000 live births (0.1% in infants with birthweight < 4000 gm40). Rarely, a congenital case may be mistaken for BBPI41. Some contend that the plexus injury may occur when uterine contractions push the shoulder against the mother’s pubic bone or with lowering of the shoulder with opposite inclination of the cervical spine41.
Classification of BBPI injuries: Upper plexus injuries are most common, with about half having C5 & C6 injuries, and 25% involving C7 also42. Combined upper and lower lesions occur in ≈ 20%. Pure lower lesions (C7-T1) are rare, constituting only ≈ 2% and seen most commonly in breech deliveries. Lesions are bilateral in ≈ 4%. A 4-level scale of intensity is shown in Table 24-1443.
Risk factors:
1. shoulder dystocia
2. high birth weight
3. primiparous mother
4. forceps44 or vacuum assisted delivery
5. breech presentation45
6. prolonged labor
7. previous birth complicated by BBPI

Management of BBPI: Most surgeons observe all patients until age 3 months. Conservative surgeons may wait up to 9 months. More aggressive surgeons will explore the plexus at age 3 months if not anti-gravity in deltoid, biceps or triceps. In cases of proven avulsion (pseudomeningocele and EMG indicative of a preganglionic injury), nerve transfers are a valid option at 3 months46. EMG may show signs of reinnervation, but the recovery may not be robust enough.
MANAGEMENT OF BRACHIAL PLEXUS INJURIES
1. most injuries show maximal deficit at onset. Progressive deficit is usually due to vascular injuries (pseudoaneurysm, A-V fistula, or expansile clot), these should be explored immediately
2. clean, sharp, relatively fresh lacerating injuries (usually iatrogenic, scalpel induced) should be explored acutely and repaired with tension-free end-to-end anastomoses within 24-48 hours (after that then ends will more edematous and therefore more difficult to suture)
3. penetrating non-missile injuries with severe or complete deficit should be explored as soon as the primary wound heals
4. gunshot wounds (GSW) to the brachial plexus: deficit is usually due to axonotmesis or neurotmesis (see below). Sometimes nerves may be divided. Nerves showing partial function usually recover spontaneously; those with complete dysfunction rarely do so. Surgery is of little benefit for discrete injuries to the lower trunk, medial cord, or C8/T1 roots. Most are managed conservatively for 2-5 months. Indications for surgery are shown in Table 24-15
5. traction injuries: incomplete postganglionic injuries tend to improve spontaneously. If recovery is not satisfactory, perform EMG at 4-5 months and explore at 6 months
Table 24-15 Indications for neurosurgical intervention in GSW to the brachial plexus4
|
1. complete loss in the distribution of at least one element A. no improvement clinically or on EMG in 2-5 months B. deficit in distribution that is responsive to surgery (e.g. C5, C6, C7, upper or middle trunk, lateral or posterior cords or their outflows) C. injuries with loss only in lower elements are not operated 2. incomplete loss with failure to control pain medically 3. pseudoaneurysm, clot or fistula involving plexus 4. true causalgia requiring sympathectomy |
6. neuromas in continuity: those that do not conduct a SNAP have complete internal disruption and require resection and grafting. Methods of repair:
A. neurolysis:
1. external neurolysis: most commonly performed in exploration. Value is questionable
2. internal neurolysis: splitting the nerve into fascicles. Not recommended unless a clear neuroma in continuity is found eccentric in the nerve that conducts SNAP
B. nerve grafting. Sural nerve is the most commonly used interposition graft following resection of neuroma in continuity
C. nerve transfers. Donor nerve options:
1. spinal accessory nerve
2. intercostal nerves to musculocutaneous nerve
3. fascicles of the ulnar nerve for the median nerve (Oberlin procedure)
4. anterior interosseous nerve to median nerve
24.3.1. Missile injuries of peripheral nerves
Most injuries from a single bullet are due to shock and cavitation from the missile causing axonotmesis or neurotmesis, and are not from direct nerve transection. Approximately 70% will recover with expectant management.
However, if there is a lack of improvement on serial examinations including electrodiagnostic studies, intervention should be undertaken by about 5-6 months to avoid further difficulties due to nerve fibrosis and muscle atrophy.
See Table 24-15 for indications for surgery for missile injuries of the brachial plexus.
24.3.2. Entrapment neuropathies
Entrapment neuropathy is a peripheral nerve injury resulting from compression either by external forces or from nearby anatomic structures. Mechanism can vary from one or two significant compressive insults to many localized, repetitive mild compressions of a nerve. Certain nerves are particularly vulnerable at specific locations by virtue of being superficial, fixed in position, traversing a confined space, or in proximity to a joint. The most common symptom is pain (frequently at rest, more severe at night, often with retrograde radiation causing more proximal lesion to be suspected) with tenderness at the point of entrapment. May be associated with:
1. diabetes mellitus
2. hypothyroidism: due to glycogen deposition in Schwann cells
3. acromegaly
4. amyloidosis: primary or secondary (as in multiple myeloma)
5. carcinomatosis
6. polymyalgia rheumatica: see page 77
7. rheumatoid arthritis: 45% incidence of 1 or more entrapment neuropathies
8. gout
Mechanism of injury
Brief compression primarily affects myelinated fibers, and classically spares unmyelinated fibers (except in cases of severe acute compression). Acute compression compromises axoplasmic flow which can reduce membrane excitability. Chronic compression affects both myelinated and unmyelinated fibers and can produce segmental demyelination in the former, and if the insult persists, axolysis and wallerian degeneration will occur in both types. The issue of ischemia is more controversial47. Some contend that simultaneous venous stasis at the site of compression can produce ischemia which can lead to edema outside the axonal sheath which may further exacerbate the ischemia. Eventually, fibrosis, neuroma formation, and progressive neuropathy can occur.
OCCIPITAL NERVE ENTRAPMENT
Greater occipital nerve (nerve of Harnold) is a sensory branch of C2 (see Figure 20-1, page 551 for dermatome). Entrapment presents as occipital neuralgia: pain in occiput usually with a trigger point near the superior nuchal line. Pressure here reproduces pain radiating up along back of head towards vertex.
More common in women.
Differential diagnosis:
1. headache
A. may be mimicked by migraine headache
B. may be part of muscle contraction (tension) headache
2. myofascial pain48: the pain may be widely separated from the trigger point
3. vertebrobasilar disease including aneurysm and SAH
4. cervical spondylosis
5. pain from Chiari I malformation (see page 233)
Possible causes of entrapment:
1. trauma
A. direct trauma (including iatrogenic placement of suture through the nerve during surgical procedures, e.g. in closing a posterior fossa craniectomy)
B. following traumatic cervical extension49 which may crush the C2 root and ganglion between the C1 arch and C2 lamina
C. fractures of the upper cervical spine (see page 961 and page 961)
2. atlanto-axial subluxation (AAS) (e.g. in rheumatoid arthritis) or arthrosis
3. entrapment by hypertrophic C1-2 (epistrophic) ligament50
4. neuromas
5. arthritis of the C2-3 zygapophyseal joint
TREATMENT
|
Σ |
For idiopathic occipital neuralgia: available evidence is from small, retrospective, case series studies and is insufficient to conclude that either local injection or surgery are effective. Nerve blocks with steroids and local anesthetics provide only temporary relief. Surgical procedures such as nerve root decompression or neurectomy may provide effective pain relief for some patients; however, patient-selection criteria for these procedures have not been defined, and recurrence is common. |
In idiopathic cases with no neurologic deficit, the condition is usually self limited.
Non surgical treatment
1. greater occipital nerve block with local anesthetic and steroids (see below)
A. may provide relief typically lasting ≈ 1 month51
B. is no longer considered diagnostic because it is not sufficiently specific
2. physical therapy: massage and daily stretching exercises
3. TENS unit: provided ≥ 50% relief in 13 patients for up to 5 yrs52
4. oral anti-inflammatory agents
5. centrally acting pain medications: Neurontin, Paxil, Elavil…
6. botulinum toxin injection53: although this study had quite a few placebo responders
If these measures do not provide permanent relief in disabling cases, surgical treatment may be considered, although caution is advised by many due to poor results48, 54. Alcohol neurolysis may be tried. A collar is not indicated as it may irritate the condition.
Occipital nerve block: Inject trigger point(s) if one or more can be identified (there is usually a trigger point near the superior nuchal line). The nerve may also be blocked at the point where it emerges from the dorsal neck muscles.
If the pathology is more proximal (e.g. at C2 spinal ganglion), then block of the ganglion may be required. Technique55 (done under fluoroscopy): shave hair below the mastoid process; prep with iodine; infiltrate with local; insert a 20 gauge spinal needle midway between C1 and C2, halfway between the midline and the lateral margin of the dorsal neck muscles. Aim rostrally, the final target is the midpoint of the C1-2 joint on AP fluoro, and almost but not touching the inferior articular process of C1. Infiltrate 1-3 ml of anesthetic and check for analgesia in the C2 distribution.
Surgical treatment
1. decompression of C2 nerve root if compressed between C1 and C250
2. in cases of AAS, decompression and atlanto-axial fusion (see page 183) may work
Surgical treatment options for idiopathic occipital neuralgia:
1. peripheral occipital nerve procedures: these may not be effective for proximal compression of the C2 root or ganglion:
A. occipital neurectomy (see below)
1. peripheral avulsion of the nerve
2. avulsion of the greater occipital nerve as it exits between the transverse process of C2 and the inferior oblique muscle
B. alcohol injection of greater occipital nerve
2. occipital nerve stimulators
3. release of the nerve within the trapezius muscle. Immediate results: relief in 46%, improvement in 36%. Only 56% reported improvement at 14.5 mos56
4. intradural division of the C2 dorsal route via a posterior intradural approach
5. ganglionectomy
Occipital neurectomy: The occipital nerve usually pierces the cervical muscles ≈ 2.5 cm lateral to the midline, just below the inion. Palpation or doppler localization of the pulse of the accompanying greater occipital artery sometimes helps to locate the nerve. However, relief only occurs in ≈ 50%, and recurrence, usually within a year, is common.
MEDIAN NERVE ENTRAPMENT
The two most common sites of entrapment of the median nerve:
• at the wrist by transverse carpal ligament: carpal tunnel syndrome (see below)
• in upper forearm by pronator teres: pronator teres syndrome (see page 809)
ANATOMY
Contributing nerve roots: C5 through T1. The median nerve arises from the medial and lateral cords of the brachial plexus (see Figure 24-1, page 790), and descends the upper arm adjacent to the lateral side of the brachial artery. It crosses to the medial side of the artery at the level of the coracobrachialis. In the cubital fossa, the median nerve passes behind the lacertus fibrosus (bicipital aponeurosis) and enters the upper forearm between the two heads of the pronator teres and supplies this muscle.
Just beyond this point, it branches to form the purely motor anterior interosseous nerve which supplies all but 2 muscles of finger and wrist flexion. It descends adherent to deep surface of flexor digitorum superficialis (FDS), lying on the flexor digitorum profundus. Near the wrist, it emerges from the lateral edge of FDS becoming more superficial, lying medial to the tendon of flexor carpi radialis, just lateral to and partially under the cover of the palmaris longus tendon. It passes under the transverse carpal ligament (TCL) through the carpal tunnel which also contains the tendons of the flexor digitorum profundus and superficialis deep to the nerve (9 tendons total, 2 to each finger, 1 to the thumb57). The motor branch arises deep to the TCL, but may anomalously pierce the TCL. It supplies the “LOAF muscles” (Lumbricals 1 & 2, Opponens pollicis, and Abductor and Flexor pollicis brevis).
The TCL attaches medially to pisiform and hook of hamate, laterally to trapezium and tubercles of scaphoid. TCL is continuous proximally with fascia over FDS and antebrachial fascia, distally with the flexor retinaculum of the hand. The TCL extends distally into the palm to ≈ 3 cm beyond the distal wrist crease. The palmaris longus tendon, which is absent in 10% of population, partially attaches to the TCL.
Palmar cutaneous branch (PCB) of median nerve: arises from the radial aspect of the median nerve approximately 5.5 cm proximal to styloid process of the radius, underneath the cover of FDS of the middle finger. It crosses the wrist above the TCL to provide sensory innervation to the base of the thenar eminence (and is thus spared in carpal tunnel syndrome).
The sensory distribution of the average median nerve is shown in Figure 24-5.
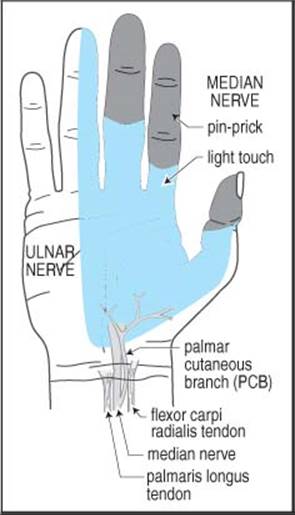
Figure 24-5 Sensory distribution of the median and ulnar nerves in the hand
INJURIES TO THE MAIN TRUNK OF THE MEDIAN NERVE
Above the elbow, the median nerve may rarely be compressed by Struther’s ligament (see below). At the elbow and forearm, the median nerve may rarely be trapped at any of three sites: 1) lacertus fibrosus (bicipital aponeurosis)58, 2) pronator teres, 3) sublimis bridge. Neuropathy may also result from direct or indirect trauma or external pressure (“honeymoon paralysis”)58. Longstanding compression of the main trunk of the median nerve produces a “benediction hand” when trying to make a fist (index finger extended, middle finger partially flexed; due to weakness of flexor digitorum profundus I & II).
STRUTHER’S LIGAMENT
(Distinct from struthers arcade which is a normal finding, see page 813). The supracondylar process (SCP) is an anatomical variant located 5-7 cm above medial epicondyle, present in 0.7-2.7% of population. Struther’s ligament bridges the SCP to the medial epicondyle. The median nerve and brachial artery pass underneath, the ulnar nerve may also. Usually asymptomatic, but occasionally may cause typical median nerve syndrome.
PRONATOR (TERES) SYNDROME
From direct trauma or repeated pronation with tight hand-grip. Trapped where nerve dives between 2 heads of pronator teres. Causes vague aching and easy fatiguing of forearm muscles with weak grip and poorly localized paresthesias in index finger and thumb. Nocturnal exacerbation is absent. Pain in palm distinguishes this from carpal tunnel syndrome (CTS) since the median palmar cutaneous branch (PCB)exits before the TCL and is spared in CTS.
Treat with resting forearm. Surgical decompression indicated for cases that progress while on rest or when continued trauma is unavoidable.
ANTERIOR INTEROSSEOUS NEUROPATHY
![]() Key concepts:
Key concepts:
• weakness of 3 muscles: FDP I & II, FPL, & pronator quadratus. No sensory loss
• loss of flexion of the distal phalanges of the thumb and index finger (pinch sign)
The anterior interosseous nerve is a purely motor branch of the median nerve that arises in the upper forearm. Anterior interosseous neuropathy (AIN) produces no sensory loss and weakness of the 3 muscles supplied by the nerve:
1. flexor digitorum profundus (FDP) I & II: flexion of distal phalanx of digits 2 & 3
2. flexor pollicis longus (FPL): flexion of distal phalanx of thumb
3. pronator quadratus (in the distal forearm): difficult to isolate clinically
Etiologies of AIN
Include: idiopathic, amyotrophy, ulna/radius fractures, penetrating injuries, forearm lacerations.
Clinical
Symptoms: Patients complain of difficulty grasping small objects between the thumb and the index finger. Idiopathic cases may be preceded with forearm aching.

Figure 24-6 “Pinch sign” seen with AIN
Physical exam: Sensory: no sensory loss.
Strength: digits 1, 2 & 3 are examined individually. The proximal interphalangeal joints are stabilized by the examiner and the patient is asked to flex the DIP. With AIN, there is no significant flexion of the DIP.
Pinch sign: the patient attempts to forcefully pinch the tips of the index finger and thumb as in making an “OK” sign (Figure 24-6, left), with AIN the terminal phalanges extend and the pulps touch instead of the tips59 (Figure 24-6, right).
Diagnosis
In addition to the physical exam, EMG may be helpful.
EMG: primarily assesses pronator quadratus & flexor pollicis longus (FDP I & II is difficult on EMG because it has dual innervation with the ulnar nerve innervated portion being more superficial than the median nerve innervated portion). Important to evaluate pronator teres (abnormalities suggest involvement more proximal than forearm).
Management
In the absence of an identifiable cause of nerve injury, expectant management is recommended for 8-12 weeks, following which exploration is indicated which may reveal a constricting band near the origin.
CARPAL TUNNEL SYNDROME
![]() Key concepts:
Key concepts:
• the most common compression neuropathy. Involves median nerve in the wrist
• symptoms: tingling in the hand, worse at night and with elevation of hands
• physical exam is not very sensitive:
![]() sensory: decreased pinprick in digits 1-3 and the radial half of 4
sensory: decreased pinprick in digits 1-3 and the radial half of 4
![]() sensitivity: Tinels (tapping on wrist) 60%, Phalens (flexion of wrist) 80%
sensitivity: Tinels (tapping on wrist) 60%, Phalens (flexion of wrist) 80%
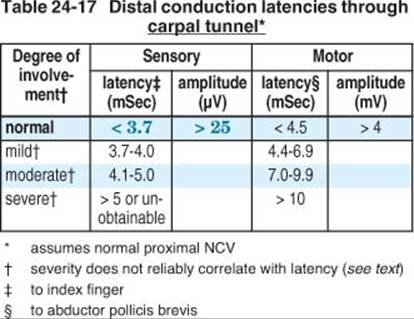
• electrodiagnostics: sensory latency @ wrist > 3.7 ms is the most sensitive test
• treatment:
![]() mild cases: nonsurgical treatment (NSAIDs, neutral position splint…)
mild cases: nonsurgical treatment (NSAIDs, neutral position splint…)
![]() severe cases (neurologic deficits, duration > 1 year): surgical neurolysis of the median nerve at the wrist has 70% satisfaction rate
severe cases (neurologic deficits, duration > 1 year): surgical neurolysis of the median nerve at the wrist has 70% satisfaction rate
Carpal tunnel syndrome (CTS) is the most common entrapment neuropathy in the upper extremity. The median nerve is compressed within its course through the carpal tunnel just distal to the wrist crease. Table 24-16 shows the effect of pressure within the carpal tunnel.
Usually occurs in middle aged patients. Ratio of female:male = 4:1. It is bilateral in over 50% of cases, but is usually worse in the dominant hand.
Table 24-16 Pressure within carpal tunnel
|
Pressure (mm Hg) |
Description |
|
< 20 |
normal |
|
20-30 |
venular flow retarded |
|
30 |
axonal transport impaired |
|
40 |
sensory & motor dysfunction |
|
60-80 |
blood flow ceases |
COMMON ETIOLOGIES60
In most cases, no specific etiology can be identified. CTS is very common in the geriatric population without any additional risk factors. The following etiologies tend to be more common in younger patients:
1. “classic” CTS: chronic time course, usually over a period of months to years
A. trauma: often job-related (may also be associated with avocations)
1. repetitive movements of hand or wrist
2. repeated forceful grasping or pinching of tools or other objects
3. awkward positions of hand and/or wrist, including wrist extension, ulnar deviation, or especially forced wrist flexion
4. direct pressure over carpal tunnel
5. use of vibrating hand tools
B. systemic conditions: in addition to systemic causes listed for entrapment neuropathies on page 804 (especially rheumatoid arthritis, diabetes), also consider:
1. obesity
2. local trauma
3. pregnancy: 54% remained symptomatic 1 year post-partum, and patients with onset early in pregnancy were less likely to improve61
4. mucopolysaccharidosis V
5. tuberculous tenosynovitis
6. multiple myeloma (amyloid deposition in flexor retinaculum) see page 740
C. patients with A-V dialysis shunts in the forearm have an increased incidence of CTS, possibly on an ischemic basis (steal and/or venous stasis) or possibly from the underlying renal disorder
2. “acute” CTS: an uncommon condition where the symptoms of CTS appear suddenly and severely, usually following some type of exertion or trauma. Etiologies:
A. median artery thrombosis: < 10% of individuals have a persistent median artery
B. hemorrhage or hematoma in the transverse carpal ligament
SIGNS AND SYMPTOMS
The physical exam for CTS is fairly insensitive. Signs and symptoms may include:
1. dysesthesias:
A. characteristically patients are awakened at night by a painful numbness in the hand that often subjectively feels like a loss of circulation of blood. They often seek relief by: shaking or dangling or swinging the hand, opening and closing or rubbing the fingers, running hot or cold water over the hand, or pacing the floor. It may radiate up the arm, occasionally as far as shoulder
B. daytime activities that characteristically elicit symptoms usually involve prolonged hand elevation: holding a book or newspaper to read, driving a car, holding a telephone receiver, brushing the hair
C. distribution of symptoms:
1. on palmar side in radial 3.5 fingers (palmar side of thumb, index finger, middle finger, and radial half of ring finger)
2. dorsal side of these same fingers distal to the PIP joint
3. radial half of palm
4. subjective involvement of little finger occurs not infrequently
2. weakness of hand, especially grip. May be associated with thenar atrophy (late change, severe atrophy is seldom seen with current awareness of CTS by most physicians). An occasional patient may present with severe atrophy and no history of pain
3. clumsiness of the hand or difficulty with fine motor skills: due mostly to numbness more than a motor deficit. Often presents as difficulties buttoning buttons…
4. hypesthesia in median nerve sensory distribution: usually best appreciated in finger tips, loss of 2-point discrimination may be more sensitive test
5. Phalen’s test: 30-60 secs of complete wrist flexion exaggerates or reproduces pain or tingling. Positive in 80% of cases62
6. Tinel’s sign at the wrist: paresthesias or pain in median nerve distribution produced by gently percussing over the carpal tunnel. Positive in 60% of cases. May also be present in other conditions. Reverse Tinel’s sign: produces symptoms radiating up the forearm for variable distance
7. ischemic testing: place blood pressure cuff proximal to wrist, inflation x 30-60 seconds may reproduce CTS pain
DIFFERENTIAL DIAGNOSIS
Differential diagnosis includes (modified63):
1. cervical radiculopathy: coexists in 70% of patients with either median or ulnar neuropathy (C6 radiculopathy may mimic CTS). Usually relieved by rest, and exacerbated by neck movement. Sensory impairment has dermatomal distribution. It has been postulated that cervical nerve root compression may interrupt axoplasmic flow and predispose the nerve to compressive injury distally (the term double-crush syndrome was coined to describe this64), and although this has been challenged65 it has not been disproven
2. thoracic outlet syndrome: loss of bulk in hand muscles other than thenar. Sensory impairment in ulnar side of hand and forearm (see page 822)
3. pronator teres syndrome: more prominent palmar pain than with CTS (median palmar cutaneous branch does not pass through carpal tunnel, see page 807)
4. de Quervain’s syndrome: tenosynovitis of the abductor pollicis longus and extensor pollicis brevis tendons often caused by repetitive hand movements. Results in pain and tenderness in the wrist near the thumb. Onset in 25% of cases is during pregnancy, and many in 1st postpartum year. Usually responds to wrist splints and/or steroid injections. NCVs should be normal. Finkelstein’s test: the thumb is passively abducted while thumb abductors are palpated, positive if this aggravates the pain66
5. reflex sympathetic dystrophy: may respond to sympathetic block (see page 216)
6. tenosynovitis of any of the flexor ligaments: may occasionally be due to TB or fungus. Usually a long, indolent course. Fluid accumulation may be present
DIAGNOSTIC TESTS
Electrodiagnostics
Electromyogram (EMG) and nerve conduction velocities (NCV): may help confirm the diagnosis of CTS and distinguish it from cervical root abnormalities and from tendonitis.
NCV: it has been said the NCV can be normal in 15-25% of cases of CTSA. Sensory latencies are more sensitive than motor.
A. NB: normal sensory electrodiagnostics effectively rules-out CTS; great reservation should be exercised in considering operating on CTS with normal sensory NCV and amplitude
Normal findings are shown in Table 24-17. Abnormal values also listed are a rough guide, but the degree of latency prolongation does not reliably correlate with the severity of symptoms, ![]() grading should not be based on this alone. More validated definitions:
grading should not be based on this alone. More validated definitions:
• mild: abnormal midplamar median velocity compared to radial or ulnar nerve
• moderate: prolonged antidromic or prolonged motor latency with amplitude loss
• severe: loss of motor axons on needle exam (EMG)
In uncertain cases, compare median nerve sensory conduction velocity to that of the ulnar nerve (or radial nerve): normal median nerve should be at least 4 m/sec faster than the ulnar, reversal of this pattern suggests median nerve injury. Alternatively, the sensory latencies for the palmar median and ulnar nerves can be compared; the median nerve latency should not be ≥ 0.3 mS longer than the ulnar.
EMG: normal in up to 31% of cases of CTS. In advanced CTS, it may show increased polyphasicity, positive waves, fibrillation potentials, and decreased motor unit numbers on maximal voluntary thenar muscle contraction. EMG may detect cervical radiculopathy if motor involvement is present.
With severe “end stage” CTS, sensory and motor potentials may not be recordable, and EMG is not helpful in localizing (i.e. differentiating CTS from other etiologies).
Laboratory tests
Recommended in cases where etiology is unclear (e.g. young individual with no history of repetitive hand use).
1. thyroid hormone levels (T4 (total or free) & TSH): to R/O myxedema
2. CBC: anemia is common in multiple myeloma, also to R/O amyloidosis
3. electrolytes:
A. to R/O chronic renal failure that could cause uremic neuropathy
B. blood glucose: R/O diabetes
4. in cases suspicious for multiple myeloma: (see page 741 for full details)
A. 24 hour urine for kappa Bence-Jones protein
B. bloodwork: serum protein electrophoresis (SPEP) and immune electrophoresis (IEP) (looking for IgG kappa band)
C. skeletal radiologic survey
D. anemia is common on the CBC
Imaging studies
Not routinely done unless a mass lesion is suspected.
Wrist MRI: very sensitive. Findings with CTS include: flattening or swelling of the nerve, palmar bowing of the flexor retinaculum. May also demonstrate ganglion cysts, lipomas… Enhancement may occur with hypervascular edema.
Diagnostic ultrasound: faster and less expensive than MRI, and can assess blood-flow and changes with different wrist positions. 18 MHz probes may improve images.
NON-SURGICAL MANAGEMENT
Recommended for cases of recent onset, mild involvement, or where exacerbating phenomena are expected to be corrected67 (p 1776) (e.g. post-partum). 89% with severe CTS (constant numbness, or sensory loss or weakness/atrophy) had a recurrence within 1 year, compared to 60% with mild CTS (intermittent numbness and no sensory or motor deficits)104. Options include:
1. rest
2. medications: non-steroidal anti-inflammatory drugs (NSAIDs), diuretics, and pyridoxine (vitamin B6) have been studied with no evidence of efficacy57
3. treatment of associated conditions (e.g. hypothyroidism or DM) is appropriate, but there is no data as to whether this relieves CTS57
4. neutral position splints: alleviates symptoms in > 80% of patients102 (usually within a few days) and reduces prolonged sensory latencies103. Relapse is common. A trial of at least 2-4 weeks is recommended
5. steroid injection: symptoms improve in > 75% of patients57. 33% relapse within 15 mos. Repeat injections are possible, but most clinicians limit to 3/year
A. use 10-25 mg hydrocortisone. Avoid local anesthetics (may mask symptoms of intraneural injection)
B. inject into carpal tunnel (deep to transverse carpal ligament) to ulnar side of palmaris longus to avoid median nerve (in patients without palmaris longus, inject in line with fourth digit)
C. median nerve injuries have been reported with this technique68, primarily due to intraneural injection (all steroids are neurotoxic upon intrafascicular injection, and so are some of the carrier agents)
D. risk factors for recurrence: severe electrodiagnostic abnormalities, constant numbness, impaired sensation, & weakness or atrophy of thenar muscles57
SURGICAL TREATMENT
Indications: Surgical intervention is recommended for: constant numbness, symptoms > 1 year duration, sensory loss, or thenar weakness/atrophy57. Surgical treatment of cases due multiple myeloma is also effective.
The operation is commonly called a carpal tunnel release, AKA neurolysis of the median nerve at the wrist.
With bilateral CTS, in general one operates on the more painful hand first. However if the condition is severe in both hands (on EMG) and if it has progressed beyond the painful stage and is only causing weakness and/or numbness, it may be best to operate on the “better” hand first in order to try and maximize recovery of the median nerve at least on that side. Simultaneous bilateral procedures may also be done69. In severe cases, nerve recovery may not occur, it may be necessary to wait up to a year to tell.
Success rate:> 70% of patients report satisfaction with their surgical results105, with 70-90% being free of nocturnal pain105, 106.
Surgical techniques
A number of techniques are popular, including: incision through palm of hand, transverse incision through wrist crease (with or without a retinaculatome70), and endoscopic techniques (using single or dual incisions). The efficacies of the various approaches have not been compared in an adequately powered randomized study57.
Transpalmar approach: (see Figure 24-7) Usually performed under local or regional anesthesia on outpatient basis. Magnification (operating loupes) are helpful.
Incision along imaginary line extending proximally from space between digits 3 and 4 (usually stay just to the ulnar side of the interthenar crease to avoid the PCB). The location of the median nerve may also be estimated by the palmaris longus tendon (stay slightly to ulnar side of tendon). Incision starts at distal wrist flexion crease, and the length depends on thickness of hand (it may extend as far distally as a line even with the crotch of the thumb). Optionally: curve ulnarward at proximal wrist flexion crease (to facilitate retraction).
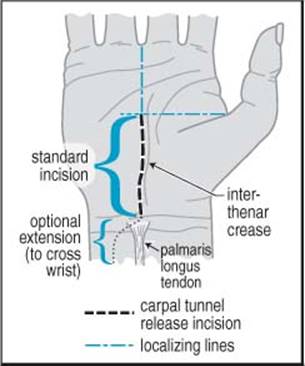
Figure 24-7 transpalmar incision for carpal tunnel syndrome
The median nerve is carefully approached through the TCL with progressively deepening incisions made with a 15 blade. All approaches to CTS surgery require complete division of TCL in the wrist. If tendons of the flexor digitorum superficialis are encountered, you need to look radially (towards the thumb) to find the nerve. In selected cases, the epineurium may be opened; however, internal neurolysis probably does more harm than good and should be avoided.
Close with absorbable 4-0 inverted sutures. Approximate skin edges with 4-0 nylon running or interrupted vertical mattress. Pad palm with several fluffs (opened dressing sponge). Cover with Kerlix®.
Post-op: wrap hand with thumb exposed. Wrist elevation and rest is recommended for several days. Analgesics for mild-to-moderate pain (e.g. acetaminophen with codeine) for 3-4 days. Sutures are removed at 7-10 days. No heavy work with hand for 2-3 weeks.
Complications of carpal tunnel surgery71
1. pain due to neuroma formation following transection of palmar cutaneous branch (PCB) of the median nerve
• branches of PCB may cross interthenar crease
• avoid by: using magnification, avoiding transverse wrist incision, and making incision slightly to ulnar side of interthenar crease
• treated by ligating this branch where it originates from median nerve in forearm (results in small area of numbness at base of thenar eminence)
2. neuroma of dorsal sensory branch of radial nerve
• caused by extending incision proximally and radially
• may be treated by neurolysis of neuroma
3. injury to recurrent thenar (motor) branch of median nerve
• anomaly may cause nerve to lie above or to pierce TCL
• avoided by: staying to ulnar side of midline
4. direct injury to median nerve
5. volar displacement and entrapment of median nerve in healing edges of TCL
6. hypertrophic scar causing compression of median nerve
• usually caused by incision crossing wrist perpendicular to flexion crease
• avoid by not crossing flexion crease, or in cases where necessary cross wrist obliquely at 45° angle directed toward ulnar side71 (see optional extension line in Figure 24-7)
7. failure to improve symptoms
• incorrect diagnosis: if EMG or NCV not done pre-op, they should be done after surgical failure (to R/O e.g. cervical root involvement (look for posterior myotome involvement), or generalized peripheral neuropathy)
• incomplete transection of TCL: the most common cause for failure if diagnosis is correct (also possibility of accessory ligament or fascial band proximal to TCL). When this is identified on re-exploration, 75% of patients will be cured or improved after division is completed
8. joint stiffness
• caused by excessively long immobilization of wrist and fingers
9. injury to superficial palmar arch (arterial): usually results from “blind” distal division of TCL
10. bowstringing of flexor tendons
11. complex regional pain syndrome AKA reflex sympathetic dystrophy: exact incidence is unknown, reported in 4 of 132 patients in one series (probably too high, most surgeons will see only one or two cases in their career). Treatment with IV phentolamine has been suggested, but most cases are self limited after ≈ 2 weeks
12. infection: usually causes exquisite tenderness
13. hematoma: also usually quite painful and tender
ULNAR NERVE ENTRAPMENT
Ulnar nerve has components of C7, C8 and T1 nerve roots. Even though this is the second most prevalent entrapment neuropathy after CTS, it is still relatively uncommon. Four potential sites of compression:
1. above elbow: possibly by the arcade of Struthers
2. at the elbow: retroepicondylar groove (“ulnar groove”): between the medial epicondyle and the olecranon process. Compression by fascia or by dynamic compression or repetitive trauma (see page 813)
3. forearm: just distal to the ulnar groove, under the aponeurosis between the heads of the flexor carpi ulnaris (FCU)
4. wrist: Guyon’s canal
Motor findings include:
1. wasting of the interossei may occur, and is most evident in the first dorsal interosseous (in the thumb web space)
2. Wartenberg’s sign: one of the earliest findings of ulnar nerve entrapment (abducted little finger due to weakness of the third palmar interosseous muscle)
3. Froment’s prehensile thumb sign: grasping a sheet of paper between thumb and the extended index finger results in extension of the proximal phalanx of the thumb and flexion of the distal phalanx as a result of substituting flexor pollicis longus (innervated by anterior interosseous nerve) for the weak adductor pollicis72 (p 18)
4. claw deformity of the hand (main en griffe): in severe ulnar nerve injuries on attempted finger extension (some have called this “benediction hand”, which differs from that with the same name in median nerve injury where the named sign occurs on trying to make a fist - see page 807). Fingers 4 and 5 and to a lesser extent 3 are hyperextended at the MCP joints (extensor digitorum is unopposed by interossei and “ulnar” lumbricals III & IV) and flexed at the interphalyngeal joints (due to pull of long flexor muscles). NB: C8 radiculopathy can also cause benediction sign73)
INJURY ABOVE ELBOW
May occur with injury to the medial cord of the brachial plexus.
In the upper arm, the ulnar nerve descends anterior to the medial head of triceps; in 70% of people it passes under arcade of Struthers (distinct from Struther’s ligament = see page 807) a flat, thin, aponeurotic band. This is not normally a point of entrapment, but may cause kinking after ulnar nerve transposition if not adequately divided67 (p 1781).
ENTRAPMENT AT ELBOW
Entrapment at or just distal to the elbow produces the cubital tunnel syndromeA. AKA tardy ulnar palsy because initial case reports occurred 12 or more years following injury at the elbow, with the majority commencing > 10 years following the original injury. The elbow is the most vulnerable point of ulnar nerve: here the nerve is superficial, fixed, and crosses a joint. Most cases are idiopathic, although there may be a history of elbow fracture (especially lateral condyle of the humerus, with associated cubitus valgus deformity), dislocation, arthritis, or repeated minor trauma. The aponeurotic arch extending over the ulnar groove and attaching on the medial epicondyle may become thickened and can compress the nerve, especially with elbow flexion74 (p 884). The ulnar nerve may also be injured during anesthesia75 (see page 799).
A. technically, the cubital tunnel is formed by the fibrous arch between the two heads of the FCU74 (p 877), the proximal entrance to which is just distal to the retrocondylar groove. However, common vernacular usually includes entrapment within the groove itself as being “cubital tunnel syndrome”
Table 24-18 McGowan classification of ulnar nerve injury
|
Grade |
Description |
|
1 |
purely subjective symptoms & mild hypesthesia |
|
2 |
sensory loss & weakness of intrinsic hand muscles ± slight wasting |
|
3 |
severe sensorimotor deficit |
PRESENTATION
Typically presents with discomfort (pain, numbness and/or tingling) in little finger and ulnar half of ring finger, elbow pain, and hand weakness. Early symptoms may be purely motor (see Froment’s sign and claw deformityabove) - unlike the median nerve where sensory involvement is almost always present. Symptoms may be exacerbated by the cold, and are often somewhat vague and may be described as a loss of finger coordination or clumsiness. Cramping and easy fatiguing of the ulnar innervated muscles of the hand may occur. Pain may not be a significant feature, but if present tends to be aching in nature along the ulnar aspect of the elbow or forearm. Atrophy of interossei is common.
The ulnar nerve is usually tender and may be palpably enlarged in the ulnar groove.
Grading: the McGowan classification76 is shown in Table 24-18.
EVALUATION
Electrodiagnostic studies
Sensory tests are not localizing for ulnar neuropathy (in contradistinction to median nerve/carpal tunnel), the motor component of the exam for the ulnar nerve is more useful for localization of the site of entrapment.
Summary of electrodiagnostic criteria for ulnar neuropathy at the elbow (not all need to be present)77, 78:
1. absolute motor nerve conduction velocity (NCV) < 50 m/sec from below elbow (BE) to above elbow (AE)
2. drop of NCV > 10 m/sec comparing BE to wrist segment to the AE to BE segment
3. amplitude of compound motor action potential (CMAP) normally decreases with distance, but a drop > 20% from BE to AE is abnormal (in the absence of anomalous innervation, e.g. Martin-Gruber anastomosis - see page 792)
4. EMG needle exam: not required. Can be normal in cases of neuropraxia (axonal loss causes abnormalities). It may be performed depending on results of above NCVs:
A. gauges severity: severe involvement show signs of axonal loss such as fibrillation potentials, positive waves or giant waves
B. helps differentiate ulnar neuropathy from cervical radiculopathy or brachial plexopathy. Check ulnar nerve innervated muscles including: the first dorsal interosseous (FDI) should routinely be tested, abductor digiti quinti/minimi (ADQ), FDP to ring or little finger, FCU. If ulnar innervated muscles are abnormal, then check non-ulnar innervated C8/medial cord/lower trunk muscles & cervical paraspinals (e.g. opponens pollicis)
Diagnostic ultrasound
Localizing ulnar nerve lesions with electrodiagnostic studies can be difficult. There has been a recent renewed interest in diagnostic ultrasound using high frequency (18 MHz) probes to help with localization, and also for identification of pathology, including nerve swelling, transection79, and neuroma, that exceeds MRI in some aspects and at a lower cost and with faster acquisition time.
NON-SURGICAL TREATMENT
Avoid elbow trauma: patient education, an elbow pad may help. Results are often better when definite traumatic etiology can be identified and eliminated.
SURGICAL TREATMENT
Most operations utilize a “lazy omega” skin incision centered over the medial epicondyle, extending at least ≈ 6 cm proximal and distal to elbow with the central “hump” directed anteriorly. The ulnar nerve is most constant and therefore most easily found immediately at the entrance to the ulnar groove. It may then be followed proximally and distally. Nerve branches that should be preserved include: posterior branches of the medial antebrachial cutaneous nerve (or else numbness or dysesthesias along medial forearm may occur) and branches to the flexor carpi ulnaris (which may branch early). Small articular branches at or proximal to the elbow joint can be preserved with simple decompression but may need to be sacrificed in transposition if they cannot be dissected far enough along the ulnar nerve. Internal neurolysis should be avoided as it may promote intraneural fibrosis.
The choice of one of the options below will determine subsequent steps.
Surgical options primarily consist of:
1. simple nerve decompression without transposition80 (see below). Includes all of the following:
A. at the elbow: division of the cubital tunnel retinaculum
B. distal to the elbow: dividing the aponeurosis connecting the two heads of the flexor carpi ulnaris, some advocate resuturing the aponeurosis underneath the nerve
C. proximal to the elbow: dividing the medial intermuscular septum (between distal biceps and triceps muscles) and the arcade of Struthers (if present)
D. preservation of the branch to the flexor carpi ulnaris and the dorsal cutaneous branch to the hand (arises 5 cm proximal to wrist)
2. nerve decompression and transposition (extent of surgery differs because degree of entrapment varies; all forms of transposition require fashioning a sling to retain the nerve in its new location). Transposition may be to:
A. subcutaneous tissue: this leaves the nerve fairly superficial and vulnerable
B. within the flexor carpi ulnaris muscle (intramuscular transposition): some contend this actually worsens the condition due to intramuscular fibrosis
C. a submuscular position: see Submuscular transposition below
3. medial epicondylectomy. Usually combined with decompression. Normally reserved for patients with a bony deformity
4. sometimes excision of neuroma and possibly jump graft may be required
Submuscular transposition
Placement under pronator teres, within a groove fashioned in the flexor carpi ulnaris (FCU). Usually requires general anesthesia (endotracheal or laryngeal mask airway).
Some key concepts4 (p 247, 260-5), 81:
1. the skin incision must extend at least ≈ 8 cm distal and proximal to the medial epicondyle to mobilize the nerve (spare the medial antecubital cutaneous nerve in the subcutaneous fatty tissue just distal to the elbow)
2. the nerve is mobilized, sparing branches to flexor carpi ulnaris (FCU) and the ulnar flexor profundi branch(es) (usually arise 2-4 cm distal to olecranon)
3. the medial intermuscular septum (between distal biceps and triceps muscles) must be cut in the distal arm to prevent the nerve from being kinked over it
4. the pronator teres muscle must be sectioned completely through just distal to the medial epicondyle
A. start by undermining the muscle just distal to the medial epicondyle
B. a mosquito hemostat may be passed under the muscle to assist
C. the muscle is cut sharply, cautery is used to treat bleeding areas
5. a trough is cut in the volar aspect of the FCU to accommodate the nerve
6. after the pronator teres is reattached over the nerve, make sure that the nerve can slide back-and-forth easily under the muscle
7. test the elbow through a range of motion after the transposition to look for snapping of the medial portion of the triceps over the medial epicondyle82
Transposition vs. decompression
|
Σ |
For most cases, simple decompression is recommended over transposition. Possible exceptions include: bony deformity, nerve subluxation |
Randomized studies have shown similar success but lower complication rate with simple decompression vs. transposition83, 84. Advantages of simple decompression include85, 86: shorter operation that can be done more easily under local anesthesia, avoidance of nerve kinking and muscular fibrosis around the transposed nerve, and preservation of cutaneous branches, ulnar branches, and nourishing blood vessels that are sometimes sacrificed with transposition, rendering portions of the nerve ischemic.
Arguments against simple decompression: Continued dynamic compression with elbow flexion, possible nerve subluxation (if present pre-op, simple decompression may make this worse)A and incomplete release of pressure points.
A. to avoid nerve subluxation and loss of vascular supply with simple decompression, avoid a 360° freeing of the nerve
Results with surgery
Not as good as with CTS, possibly due in part to the fact that patients tend to present much later. Overall, a good to excellent result is obtained in 60%, fair result in 25%, and a poor result (no improvement or worsening) in 15%87 (p 2530). These results may be worse in patients with symptoms present > 1 year, with only 30% of these symptomatically improved in one series80. Lower success rate is also seen in older patients and those with certain medical conditions (diabetes, alcoholism…). Pain and sensory changes respond better than muscle weakness and atrophy.
ENTRAPMENT IN THE FOREARM
Very rare. Just distal to the elbow, the ulnar nerve passes from the retroepicondylar groove to pass under the fascial band connecting the two heads of the flexor carpi ulnaris (FCU), superficial to the flexor superficialis and pronator teres. Findings with entrapment in the forearm are similar to tardy ulnar nerve palsy (see above).
Surgical treatment consists of steps outlined for nerve distal to the elbow in ulnar nerve decompression (see above). A technique for locating the course of the ulnar nerve distal to the elbow: the surgeon takes the little finger of his/her own hand (using the hand contralateral to the patient’s side that is being decompressed) and places the proximal phalanx in the ulnar groove aiming it toward the ulnar side of the wrist4 (p 262).
ENTRAPMENT IN THE WRIST OR HAND
At the wrist, the terminal ulnar nerve enters Guyon’s canal, the roof of which is the palmar fascia and palmaris brevis, the floor is the flexor retinaculum of the palm and the pisohamate ligament.
Guyon’s canal is superficial to the transverse carpal ligament (which overlies the carpal tunnel and compresses the median nerve in carpal tunnel syndrome).
The canal contains no tendons, only the ulnar nerve and artery. At the middle of the canal the nerve divides into deep and superficial branch. The superficial branch is mostly sensory (except for the branch to palmaris brevis), and supplies hypothenar eminence and ulnar half of ring finger. The deep (muscular) branch innervates hypothenar muscles, lumbricals 3 & 4, and all interossei. Occasionally the abductor digiti minimi branch arises from the main trunk or superficial branch.
Shea and McClain88 divided lesions of the ulnar nerve in Guyon’s canal into 3 types shown in Table 24-19. Injury to the distal motor branch can also occur in the palm and produces findings similar to a Type II injury.
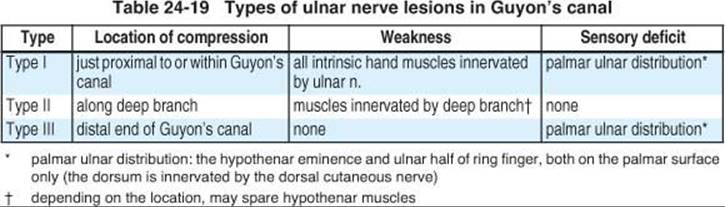
Injury is most often due to a ganglion of the wrist89, but also may be due to trauma (pneumatic drill, pliers, repetitively slamming a stapler, leaning on palm while riding bicycle). Symptoms are similar to those of ulnar nerve involvement at the elbow, except there will never be sensory loss in the dorsum of the hand in the ulnar nerve territory because the dorsal cutaneous branch leaves the nerve in the forearm 5-8 cm proximal to the wrist (sparing of flexor carpi ulnaris and flexor digitorum profundus III & IV is not helpful in localizing because these are so rarely involved even in proximal lesions). Electrodiagnostics are usually helpful in localizing the site of the lesion. Pain, when present, may be exacerbated by tapping over pisiform (Tinel’s sign). It may also radiate up the forearm.
Surgical decompression may be indicated in refractory cases. To locate: find the ulnar artery, and the nerve is on the ulnar side of the artery. Controversial whether simple decompression vs. subcutaneous transposition is best, the outcome is similar but there may be more complications in the transposition group83, 84 but studies are small.
RADIAL NERVE INJURIES16 (1443-45)
Radial nerve arises from the posterior divisions of the 3 trunks of the brachial plexus. Receives contributions from C5 to C8. The nerve winds laterally along the spiral groove of the humerus where it is vulnerable to compression or injury from fracture.
Distinguish radial nerve injury from injury of posterior cord of brachial plexus by sparing of deltoid (axillary nerve) and latissimus dorsi (thoracodorsal nerve).
AXILLARY COMPRESSION
Less common than compression in mid-upper arm.
Etiologies: crutch misuse; poor arm position during (drunken) sleep.
Clinical: weakness of triceps and more distal muscles innervated by radial nerve.
MID-UPPER ARM COMPRESSION
Sites of compression: in spiral groove, at intermuscular septum, or just distal to this.
Etiologies:
1. “Saturday night palsy”: improper positioning of arm in sleep (especially when drunk and therefore less likely to self-reposition in response to the accompanying discomfort, e.g. due to a bed-mate’s head resting on the arm)
2. from positioning under general anesthesia
3. from callus due to old humeral fracture
Clinical: weakness of wrist extensors (wrist drop) and finger extensors. ![]() Key: triceps is normal because takeoff of nerve to triceps is proximal to spiral groove. Involvement of distal nerve is variable, may include thumb extensor palsy and paresthesias in radial nerve distribution. Differential diagnosis: isolated wrist and finger extensor weakness can also occur in lead poisoning (usually bilateral, more common in adults).
Key: triceps is normal because takeoff of nerve to triceps is proximal to spiral groove. Involvement of distal nerve is variable, may include thumb extensor palsy and paresthesias in radial nerve distribution. Differential diagnosis: isolated wrist and finger extensor weakness can also occur in lead poisoning (usually bilateral, more common in adults).
FOREARM COMPRESSION
The radial nerve enters the anterior compartment of the arm just above the elbow. It gives off branches to brachialis, brachioradialis, and extensor carpi radialis (ECR) longus before dividing into the posterior interosseous nerve and the superficial radial nerve. The posterior interosseous nerve dives into the supinator muscle through a fibrous band known as the arcade of Frohse (see page 791 for muscles supplied).
POSTERIOR INTEROSSEOUS NEUROPATHY
Posterior interosseous neuropathy (“PIN”) may result from: lipomas, ganglia, fibromas, arthritis, entrapment at the arcade of Frohse (rare), and strenuous use of arm.
Clinical: marked extensor weakness of thumb and fingers (finger drop). Distinguished from radial nerve palsy by less wrist extensor weakness (no wrist drop) due to sparing of ECR brevis and longus (there will be radial deviation due to palsy of extensor carpi ulnaris). No sensory loss (c.f. what would occur with C8 radiculopathy).
Treatment: cases that do not respond to 4-8 weeks of expectant management should be explored, and any constrictions lysed (including arcade of Frohse).
RADIAL TUNNEL SYNDROME
AKA supinator syndrome. Controversial. The “radial tunnel” extends from just above the elbow to just distal to it, and is composed of different structures (muscles, fibrous bands…) depending on the level90. It contains the radial nerve and its two main branches (posterior interosseous and superficial radial nerves). Repeated forceful supination or pronation or inflammation of supinator muscle attachments (as in tennis elbow) may traumatize the nerve (sometimes by ECR brevis). Characteristic finding: pain in the region of the common extensor origin at the lateral epicondyle on resisted extension of the middle finger which tightens the ECR brevis. May be mistakenly diagnosed as resistant “tennis elbow” (lateral epicondylitis must be excluded). There may also be paresthesias in the distribution of the superficial radial nerve and local tenderness along the radial nerve anterior to the radial head. Even though the site of entrapment is similar to PIN, unlike PIN, there is usually no muscle weakness. Surgery: rarely required, consists of nerve decompression90.
INJURY IN THE HAND
The distal cutaneous branches of the superficial radial nerve cross the extensor pollicis longus tendon, and can often be palpated at this point with the thumb in extension. Injury to the medial branch of this nerve occurs commonly e.g. with handcuff injuries, and causes a small area of sensory loss in the dorsal web-space of the thumb.
AXILLARY NERVE INJURIES
Isolated neuropathy of the axillary nerve may occur in the following situations91:
1. shoulder dislocation: the nerve is tethered to the joint capsule92
2. sleeping in the prone position with the arms abducted above the head
3. compression from a thoracic harness
4. injection injury in the high posterior aspect of the shoulder
5. entrapment of the nerve in the quadrilateral space (bounded by the teres major and minor muscles, long head of triceps, and neck of humerus) which contains the axillary nerve and the posterior humeral circumflex artery. Arteriogram may show loss of filling of the artery with the arm abducted and externally rotated
SUPRASCAPULAR NERVE
The suprascapular nerve is a mixed peripheral nerve arising from the superior trunk of the brachial plexus, with contributions from C5 & C6. There is often a history of shoulder trauma or frozen shoulder. Entrapment results in weakness & atrophy of infra-and supraspinatus (IS & SS) and deep, poorly localized (referred) shoulder pain (the sensory part of the nerve innervates the posterior joint capsule but has no cutaneous representation).
Etiologies:
1. nerve entrapment within the suprascapular notch beneath the transverse scapular (suprascapular) ligament (TSL)93
2. repetitive shoulder trauma: may be bilateral when the injury is from activities such as weight-lifting
3. ganglion or tumor94 (MRI is the test of choice for imaging these)
4. paralabral cyst from labral tear (the tendon of the long head of the biceps attaches to the superior glenoid labrum; test of choice for labral tears is MR arthrography)
Differential diagnosis includes93:
1. pathology in or around shoulder joint
A. rotator cuff injuries (distinction may be very difficult)
B. adhesive capsulitis
C. bicipital tenosynovitis
D. arthritis
2. cases of Parsonage-Turner syndrome limited to the suprascapular nerve (see Neuralgic amyotrophy, page 794)
3. cervical radiculopathy (≈ C5) } NB: these two will also produce rhomboid and deltoid weakness and, usually, cutaneous sensory loss
4. upper brachial plexus lesion } NB: these two will also produce rhomboid and deltoid weakness and, usually, cutaneous sensory loss
Diagnosis requires temporary relief with nerve block, and EMG abnormalities of SS & IS (in rotator cuff tears, fibrillation potentials will be absent). Transient pain relief with a suprascapular nerve block helps verify the diagnosis95.
Treatment:
In cases where a mass is not the underlying cause, initial treatment consists of resting the affected UE, PT (including gentle conditioning), NSAIDs, topical capsaicin cream, and sometimes corticosteroid injection.
Surgical treatment is indicated for documented cases that fail to improve with conservative treatment (PT, NSAIDs, steroid/local anesthetic injection…). Position: lateral decubitus. Incision: 2 cm above and parallel to the scapular spine (atrophy of SS facilitates this). Only the trapezius needs to be split along its fibers (caution re spinal accessory nerve). To locate suprascapular notch, follow omohyoid to where it attaches to scapula and palpate just lateral to this. The suprascapular artery and vein pass over the TSL and should be preserved. Elevate the TSL with a dull nerve hook and divide it (exposure of the nerve and/or resection of the bony notch are not necessary).
MERALGIA PARESTHETICA
Originally known as the Bernhardt-Roth syndrome, and sometimes called “swashbuckler’s disease”, meralgia paresthetica (MP) (Greek: meros - thigh, algos - pain) is a condition often caused by entrapment of the lateral femoral cutaneous nerve (LFCN) of the thigh, (a purely sensory branch with contributions from L2 and L3 nerve roots, see Figure 5-13, page 94 for distribution) where it enters the thigh though the opening between the inguinal ligament and its attachment to the anterior superior iliac spine (ASIS). Anatomic variation is common, and the nerve may actually pass through the ligament, and as many as four branches may be found. May also be an initial manifestation of diabetes (diabetic neuropathy).
Signs and symptoms
Burning dysesthesias in the lateral aspect of the upper thigh, occasionally just above the knee, usually with increased sensitivity to clothing (hyperpathia). There may be decreased sensation in this distribution. Spontaneous rubbing or massaging the area in order to obtain relief is very characteristic96. MP may be bilateral in up to 20% of cases. Sitting or lying prone usually ameliorates the symptoms.
There may be point tenderness at the site of entrapment (where pressure may reproduce the pain), which is often located where the nerve exits the pelvis medial to the ASIS. Hip extension may also cause pain.
Occurrence
Usually seen in obese patients, may be exacerbated by wearing tight belts or girdles, and by prolonged standing or walking. Recently found in long distance runners. Higher incidence in diabetics. May also occur post-op in slender patients positioned prone, tends to be bilateral (see page 800).
Possible etiologies are too numerous to list, more common ones include: tight clothing or belts, surgical scars post-abdominal surgery, cardiac catheterization (see page 800), pregnancy, iliac crest bone graft harvesting, ascites, obesity, metabolic neuropathies, and abdominal or pelvic mass.
DIFFERENTIAL DIAGNOSIS
1. femoral neuropathy: sensory changes tend to be more anteromedial than MP
2. L2 or L3 radiculopathy: look for motor weakness (thigh flexion or knee extension)
3. nerve compression by abdominal or pelvic tumor (suspected if concomitant GI or GU symptoms)
The condition can usually be diagnosed on clinical grounds. When it is felt to be necessary, confirmatory tests may help (but frequently are disappointing), including:
1. EMG: may be difficult, the electromyographer cannot always find the nerve)
2. MRI or CT/myelography: when disc disease is suspected
3. pelvic imaging (MRI or CT)
4. somatosensory evoked potentials
5. response to local anesthetic injections
6. recent promise of diagnostic ultrasound using high frequency (18 MHz) probes
TREATMENT
Tends to regress spontaneously, but recurrence is common. Nonsurgical measures achieve relief in ≈ 91% of cases and should be tried prior to considering surgery97:
1. remove offending articles (constricting belts, braces, casts, tight garments…)
2. in obese patients: weight loss and exercises to strengthen the abdominal muscles is usually effective, but is rarely achieved by the patient
3. elimination of activities involving hip extension
4. application of ice to the area of presumed constriction x 30 minutes TID
5. NSAID of choice x 7-10 days
6. capsaicin ointment applied TID (see page 566)
7. lidoderm patches in areas of hyperesthesia may help98 (see page 549)
8. centrally acting pain medications (e.g. gabapentin, carbamazepine…) are rarely effective
9. if the above measures fail, injection of 5-10 ml of local anesthetic (with or without steroids) at the point of tenderness, or medial to the ASIS may provide temporary or sometimes long lasting relief, and confirms the diagnosis
Surgical treatment
Options include:
1. surgical decompression (neurolysis) of the nerve: higher failure and recurrence rate than neurectomy
2. decompression and transposition
3. selective L2 nerve stimulation
4. division of the nerve (neurectomy) may be more effective, but risks denervation pain, and leaves an anesthetic area (usually a minor nuisance). May be best reserved for treatment failures
Technique97:
The operation is best performed under general anesthesia. A 4-6 cm oblique incision is centered 2 cm distal to the point of tenderness. Since the course of the nerve is variable, the operation is exploratory in nature, and generous exposure is required. If the nerve can’t be located, it is usually because the exposure is too superficial. If the nerve still cannot be found, a small abdominal muscle incision can be made and the nerve may be located in the retroperitoneal area. CAUTION: cases have occurred where the femoral nerve has erroneously been divided.
If neurectomy instead of neurolysis is elected, electrical stimulation should be performed prior to sectioning to rule out a motor component (which would disqualify the nerve as the LFCN). If the nerve is to be divided, it should be placed on stretch and then cut to allow the proximal end to retract back into the pelvis. Any segment of apparent pathology should be resected for microscopic analysis. Neurectomy results in anesthesia in the distribution of the LFCN that is rarely distressing and gradually reduces in size.
A supra-inguinal ligament approach has also been described99.
OBTURATOR NERVE ENTRAPMENT
Controversial if this exists. The obturator nerve is composed of L2-4 roots. It courses along the pelvic wall to provide sensation to the inner thigh, and motor to the thigh adductors (gracilis and adductors longus, brevis, and magnus). It may be compressed by pelvic tumors, also from the pressure of the fetal head or forceps during parturition.
The result is numbness of the medial thigh and weak thigh adduction.
FEMORAL NERVE ENTRAPMENT
Composed of roots L2-4. Entrapment is a rare cause of femoral neuropathy. More commonly due to fracture or surgery. Femoral neuropathy on page 798.
COMMON PERONEAL NERVE PALSY
The peroneal nerve is the most common nerve to develop acute compression palsy.
Functional anatomy: the sciatic nerve (L4-S3) consists of 2 separate nerves within a common sheath that separate at a variable location in the thighA (see Table 35-4, page 1195):
A. the peroneal division of the sciatic nerve is more vulnerable to injury than the tibial division
1. posterior tibial nerve, or, just tibial nerve (AKA medial popliteal nerve) which provides for foot inversion among other motor functions
2. common peroneal nerve (CPN), or, just peroneal nerve (AKA lateral popliteal nerve): high injuries may involve the lateral hamstring (short head of the biceps femoris) in addition to the following. The CPN passes behind the fibular head where it is superficial and fixed, making it vulnerable to pressure or trauma (e.g. from crossing the legs at the knee). Just distal to this, the CPN divides into:
A. deep peroneal nerve (AKA anterior tibial nerve): primarily motor
1. motor: foot and toe extension (extensor hallicus longus (EHL), anterior tibialis (AT), extensor digitorum longus (EDL))
2. sensory: very small area between great toe and second toe
B. superficial peroneal nerve (AKA musculocutaneous nerve)
1. motor: foot eversion (peroneus longus and brevis)
2. sensory: lateral distal leg and dorsum of foot
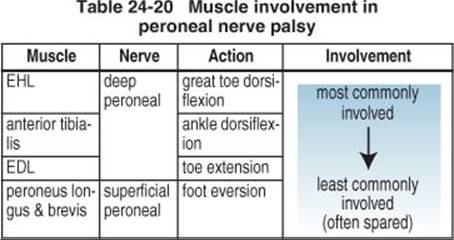
Findings in peroneal nerve palsy
• sensory changes (uncommon): involves lateral aspect of lower half of leg
• muscle involvement: see Table 24-20
Common peroneal nerve palsy (most common) produces weak ankle dorsiflexion (foot drop) due to anterior tibialis palsy, weak foot eversion, and sensory impairment in areas innervated by deep and superficial peroneal nerve (lateral calf and dorsum of foot). There may be a Tinel’s sign with percussion over the nerve near the fibular neck. Occasionally, only the deep peroneal nerve is involved, resulting in foot drop with minimal sensory loss. Must differentiate from other causes of foot drop (see Foot drop, page 1194).
Examination/clinical correlation4 (p 293)
• buttock level injury: unless the injury is one that permits spontaneous regeneration, prognosis is poor for return of peroneal nerve function even with surgery
• thigh level injury: also difficult to get improvement with surgical repair. Some peroneus function may occur at ≥ 6 mos, early contraction of AT may take ≥ 1 yr
• knee level injury: with successful regeneration, peroneus contraction may begin by 3-5 months. First signs: quivering of muscle lateral to the proximal fibula on attempted foot eversion, or tightening of tendon posterior and behind the lateral malleolus on attempted ankle dorsiflexion
Causes of common peroneal nerve injury
The most frequent cause of serious peroneal nerve injury is knee injury ± fracture (for causes of foot drop other than peroneal nerve palsy see page 1195).
1. entrapment as it crosses the fibular neck or as it penetrates the peroneus longus
2. diabetes mellitus and other metabolic peripheral neuropathies
3. inflammatory neuropathy: including Hansen’s disease (leprosy)
4. traumatic: e.g. clipping injury in football players, stretch injury due to dislocating force applied to the knee, fibular fracture, injury during hip or knee replacement surgery
5. penetrating injury
6. masses in the area of the fibular head/proximal lower leg: popliteal fossa cysts (Baker cyst), anterior tibial artery aneurysm100 (rare)
7. pressure at fibular head: e.g. from crossing the legs at the knee, casts, obstetrical stirrups (see page 799)…
8. traction injuries: severe inversion sprains of the ankle
9. intraneural tumors: neurofibroma, schwannoma, ganglion cysts
10. vascular: venous thrombosis
11. weight loss
Evaluation
EMG: EMG takes 2-4 weeks from the onset of symptoms to become positive. Stimulate above and below fibular head for prognostic information: if absent in both sites, the prognosis is poor (indicates retrograde degeneration has occurred). Wallerian degeneration takes ≈ 5 days to cause deterioration.
In addition to the expected findings of denervation (PSWs & fibs - see page 270) in the anterior tibialis, evaluate:
1. L5 innervated muscles outside the distribution of the common peroneal nerve:
A. posterior tibialis
B. flexor digitorum longus
2. L5 muscles whose nerve originates above the knee (these muscles are spared in cases of compression of the peroneal nerve at the fibular head due to the fact that the nerve takeoff is proximal to the popliteal fossa):
A. biceps femoris (short or long head)
B. tensor fascia lata
3. paraspinal muscles: signs of denervation solidifies the location of the lesion as nerve root; not helpful if negative
MRI: May demonstrate causes such as a ganglion cyst arising from the superior tibiofibular articulation.
Treatment
When treatment can eliminate a reversible cause, the outcome is usually good. Surgical exploration and decompression may be considered when there is no reversible cause or when improvement does not occur.
Bracing: ankle-foot-orthosis (AFO) compensates for loss of ankle dorsiflexion which inserts unobtrusively into a shoe. If this is inadequate, or to stabilize the ankle, a spring-loaded kick-up foot brace built into a shoe may be used. The patient should be instructed in techniques to avoid contracture of the Achilles tendon (heel cord) which would impair ankle dorsiflexion if nerve function returns.
Surgical technique: At the level of the popliteal fossa the skin incision is made just medial to the tendon of the short head of the biceps femoris (lateral hamstring) as the peroneal nerve is best located deep to or slightly medial to this tendon. The incision is carried distally slightly laterally along the surgical neck of the fibula. The biceps femoris is retracted laterally and the nerve is isolated and tagged with a Penrose drain. The sensory sural nerve branches off the peroneal nerve at variable sites ranging from the sciatic portion of the nerve (proximal to the flexor crease) or distal to this.
In cases of compression, the fascia from the lateral gastrocnemius and soleus over-lying the nerve distal to the fibular head is lysed and the nerve is exposed in 360°. As the nerve crosses the fibular neck it divides into superficial and deep branches. The superficial branch travels directly distally to supply the peroneus longus and brevis (foot evertors). The deep branches curve anteriorly to the anterior tibialis, EHL, and toe extensors.
If a graft is needed, the contralateral sural nerve is usually used, which may be supplemented with the ipsilateral sural nerve if needed.
TARSAL TUNNEL
Entrapment of (posterior) tibial nerve may occur in the tarsal tunnel, posterior and inferior to medial malleolus. The tunnel is covered by the flexor retinaculum (lancinate ligament) which extends downward from the medial malleolus to the tubercle of the calcaneus. There is often (but not necessarily) a history of old ankle dislocation or fracture. The nerve may be trapped at the retinacular ligament. This results in pain and paresthesias in the toes and sole of foot (often sparing the heel because the sensory branches often originate proximal to the tunnel), typically worse at night. May cause clawing of toes secondary to weakness of intrinsic foot muscles. Often caused by fracture or dislocation, also rheumatoid arthritis, rarely tumors.
Exam
Percussion of nerve at medial malleolus produces paresthesias that radiate distally (Tinel’s sign). Maximal inversion and eversion of the foot tend to exacerbate. Dorsiflexion-eversion test: examiner maximally everts and dorsiflexes the ankle while dorsiflexing the toes at the MTP joints for 5-10 seconds. Positive test reproduces the pain.
Diagnosis
EMG and NCV studies may help.
Treatment
External ankle support to improve foot mechanics.
Surgical decompression is indicated for confirmed cases that fail to improve. A curvilinear incision is used, ≈ 1.5 cm posterior and inferior to the medial malleolus. The flex-or retinaculum is divided, as are any septa underneath, and the distal branches should be followed until they dive into the muscle.
24.4. Thoracic outlet syndrome
The thoracic outlet is a confined area at the apex of the lung bordered by the 1st rib below and the clavicle above through which passes the subclavian artery, vein, and brachial plexus.
Thoracic outlet syndrome (TOS) is a term implying compression of one or more of the enclosed structures producing a heterogeneous group of disorders. TOS tends to be diagnosed more often by general and vascular surgeons than by neurologists and neurosurgeons. Four unrelated conditions with different structures involved:
1. arterial vascular: producing arm, hand and finger pallor and ischemia } “noncontroversial”, with characteristic symptom complex, reproducible clinical findings, confirmatory laboratory tests. Low incidence101
2. venous vascular: producing arm swelling and edema } “noncontroversial”, with characteristic symptom complex, reproducible clinical findings, confirmatory laboratory tests. Low incidence101
3. true neurologic: compressing the lower trunk or median cord of the brachial plexus (see below) } “noncontroversial”, with characteristic symptom complex, reproducible clinical findings, confirmatory laboratory tests. Low incidence101
4. disputed neurologic: (see below) } “noncontroversial”, with characteristic symptom complex, reproducible clinical findings, confirmatory laboratory tests. Low incidence101
Differential diagnosis
1. herniated cervical disc
2. cervical arthrosis
3. lung cancer (pancoast tumor)
4. tardy ulnar nerve palsy
5. carpal tunnel syndrome
6. orthopedic shoulder problems
7. complex regional pain syndrome (reflex sympathetic dystrophy)
TRUE NEUROLOGIC TOS
A rare condition primarily affecting adult women, usually unilateral.
Neurologic structures involved
1. most common: compression of the C8/T1 roots
2. or proximal lower trunk of the brachial plexus (BP)
3. less common: compression of the median cord of the BP
Etiologies
1. constricting band extending from the first rib to a rudimentary “cervical rib” or to an elongated C7 transverse process
2. scalenus (anticus) syndrome: controversial (see Scalenus (anticus) syndrome (disputed neurologic TOS) below)
3. compression beneath the pectoralis minor tendon under the coracoid process: may result from repetitive movements of the arms above the head (shoulder elevation and hyperabduction)
Signs & symptoms include:
1. ![]() sensory changes in distribution of median cord (mainly along medial forearm), sparing median nerve sensory fibers (pass through upper and middle trunks)
sensory changes in distribution of median cord (mainly along medial forearm), sparing median nerve sensory fibers (pass through upper and middle trunks)
2. hand clumsiness or weakness and wasting, especially abductor pollicis brevis and ulnar hand intrinsics (C8/T1 denervation/atrophy)
3. there may be tenderness over Erb’s point (2 to 3 cm above the clavicle in front of the C6 transverse process)
4. may be painless
5. usually unilateral
Confirmatory tests:
1. EMG: unreliable (may be negative). Most common abnormality in neurogenic TOS is loss of medial antebrachial cutaneous SNAP
2. MRI does not show bony abnormalities well, but may occasionally demonstrate a kink in the lower BP. Can also rule-out conditions that may mimic TOS such as herniated cervical disc
3. cervical spine x-rays with obliques and apical lordotic CXR may demonstrate bony abnormalities. However, not every cervical rib produces symptoms.
Treatment
Controversial. Conservative treatment (usually including stretching and physical therapy) is about as effective as surgery and avoids attendant risks.
Decompression can be achieved by removing the muscles that surround the nerves (scalenectomy), by transaxillary first rib resection, or both.
SCALENUS (ANTICUS) SYNDROME (DISPUTED NEUROLOGIC TOS)
Controversial. More commonly diagnosed in the 1940’s and 50’s. There is a lack of consensus regarding the pathophysiology (including structures involved), clinical presentation, helpful tests, and optimal treatment. Removal of first thoracic rib is often advocated for treatment, frequently via a transaxillary approach. Unfortunately, injuries, especially to the lower trunk of the brachial plexus, may result from the surgery.
Other variations include an “upper plexus” type for which total anterior scalenectomy is advocated. Again, very controversial.
24.5. Miscellaneous peripheral nerve
Nerve block
For example, to block greater occipital nerve in occipital neuralgia.
Rx: add 40 mg methylprednisolone aqueous suspension (Depo-Medrol®) to 10 ml of 0.75% bipuvicaine (Marcaine®) and inject into region of irritated or inflamed nerve.
24.6. References
1. Fernandez E, Pallini R, La Marca F, et al.: Neurosurgery of the peripheral nervous system - part I: Basic anatomic concepts. Surg Neurol 46: 47-8, 1996.
2. Dyck P J, Boes C J, Mulder D, et al.: History of standard scoring, notation, and summation of neuromuscular signs. A current survey and recommendation. J Peripher Nerv Syst 10 (2): J Peripher Nerv Syst: 158-73, 2005.
3. Medical Research Council: Aids to the examination of the peripheral nervous system. Her Majesty’s Stationery Office, London, 1976.
4. Kline D G, Hudson A R: Nerve injuries: Operative results for major nerve injuries, entrapments, and tumors. W. B. Saunders, Philadelphia, 1995.
5. Rodriguez-Niedenfuhr M, Vazquez T, Parkin I, et al.: Martin-Gruber anastomosis revisited. Clin Anat 15 (2): 129-34, 2002.
6. Ochoa J L, Verdugo R J: Reflex sympathetic dystrophy: A common clinical avenue for somatoform expression. Neurol Clin 13: 351-63, 1995.
7. Denny-Brown D: Primary sensory neuropathy with muscular changes associated with carcinoma. J Neurol Neurosurg Psychiatry 11: 73-87, 1948.
8. Camerlingo M, Nemni R, Ferraro B, et al.: Malignancy and sensory neuropathy of unexplained cause: A prospective study of 51 patients. Arch Neurol 55: 981-4, 1998.
9. Adams R D, Victor M: Principles of neurology. 2nd ed. McGraw-Hill, New York, 1981.
10. Turner J W, Parsonage M J: Neuralgic amyotrophy (paralytic brachial neuritis); with special reference to prognosis. Lancet 273: Lancet: 209, 1957.
11. Tsairis P, Dyck P J, Mulder D W: Natural history of brachial plexus neuropathy: Report on 99 patients. Arch Neurol 27: 109-17, 1972.
12. Misamore G W, Lehman D E: Parsonage-Turner syndrome (acute brachial neuritis). J Bone Joint Surg 78 (9): J Bone Joint Surg: 1405-8, 1996.
13. Evans B A, Stevens J C, Dyck P J: Lumbosacral plexus neuropathy. Neurology 31: 1327-30, 1981.
14. The Diabetes Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulindependent diabetes mellitus. N Engl J Med329: 977-86, 1993.
15. Asbury A K: Proximal diabetic neuropathy. Ann Neurol 2: 179-80, 1977.
16. Dyck P J, Thomas P K: Peripheral neuropathy. 2nd ed. W. B. Saunders, Philadelphia, 1984.
17. Garland H: Diabetic amyotrophy. BMJ 2: 1287-90, 1955.
18. Barohn R J, Sahenk Z, Warmolts J R, et al.: The Bruns-Garland syndrome (diabetic amyotrophy): Revisited 100 years later. Arch Neurol 48: 1130-5, 1991.
19. Pascoe M K, Low P A, Windebank A J: Subacute diabetic proximal neuropathy. Mayo Clin Proc 72: 1123-32, 1997.
20. Davis J L, Lewis S B, Gerich J E, et al.: Peripheral diabetic neuropathy treated with amitriptyline and fluphenazine. JAMA 21: 2291-2, 1977.
21. Max M B, Lynch S A, Muir J, et al.: Effects of desipramine, amitriptyline, and fluoxetine on pain in diabetic neuropathy. N Engl J Med 326: 1250-6, 1992.
22. Mendel C M, Klein R F, Chappell D A, et al.: A trial of amitriptyline and fluphenazine in the treatment of painful diabetic neuropathy. JAMA 255: 637-9, 1986.
23. Mendel C M, Grunfeld C: Amitriptyline and fluphenazine for painful diabetic neuropathy. JAMA 256: 712-4, 1986.
24. Backonja M, Beydoun A, Edwards K R, et al.: Gabapentin for the symptomatic treatment of painful neuropathy in patients with diabetes mellitus: A randomized controlled trial. JAMA 280 (21): 1831-6, 1998.
25. Morello C M, Leckband S G, Stoner C P, et al.: Randomized double-blind study comparing the efficacy of gabapentin with amitriptyline on diabetic peripheral neuropathy pain. Arch Intern Med 159 (16): 1931-7, 1999.
26. New uses of thalidomide. Med Letter 38: 15-6, 1996.
27. Fuller G N, Jacobs J M, Guiloff R J: Nature and incidence of peripheral nerve syndromes in HIV infection. J Neurol Neurosurg Psychiatry 56: 372-81, 1993.
28. Drugs for HIV infection. Med Letter 42 (1069): 1-6, 2000.
29. Warner M A: Perioperative neuropathies. Mayo Clin Proc 73: 567-74, 1998.
30. Wadsworth T G, Williams J R: Cubital tunnel external compression syndrome. Br Med J 1: 662-6, 1973.
31. Warner M A, Marner M E, Martin J T: Ulnar neuropathy: Incidence, outcome, and risk factors in sedated or anesthesthetized patients. Anesthesiology 81: 1332-40, 1994.
32. Alvine F G, Schurrer M E: Postoperative ulnar-nerve palsy: Are there predisposing factors? J Bone Joint Surg 69A: 255-9, 1987.
33. Stewart J D, Shantz S H: Perioperative ulnar neuropathies: A medicolegal review. Can J Neurol Sci 30: 15-9, 2003.
34. Warner M A, Martin J T, Schroeder D R, et al.: Lower-extremity motor neuropathy associated with surgery performed on patients in a lithotomy position. Anesthesiology 81: 6-12, 1994.
35. O’Donnell D, Rottman R, Kotelko D, et al.: Incidence of maternal postpartum neurologic dysfunction. Anesthesiology 81 (Suppl): A1127, 1994 (abstract).
36. Sanabria E A M, Nagashima T, Yamashita H, et al.: Postoperative bilateral meralgia paresthetica after spine surgery: An overlooked entity? Spinal Surgery 17 (3): 195-202, 2003.
37. Kent C K, Moscucci M, Gallagher S G, et al.: Neuropathies after cardiac catheterization: Incidence, clinical patterns, and long-term outcome. J Vasc Surg 19: 1008-14, 1994.
38. Carvalho G A, Nikkhah G, Matthies C, et al.: Diagnosis of root avulsions in traumatic brachial plexus injuries: Value of computerized tomography myelography and magnetic resonance imaging. J Neurosurg 86 (1): J Neurosurg: 69-76, 1997.
39. Hashimoto T, Mitomo M, Hirabuki N, et al.: Nerve root avulsion of birth palsy: Comparison of myelography with CT myelography and somatosensory evoked potential. Radiology 178 (3): Radiology: 841-5, 1991.
40. Rouse D J, Owen J, Goldenberg R L, et al.: The effectiveness and costs of elective cesarean delivery for fetal macrosomia diagnosed by ultrasound. JAMA 276 (18): 1480-6, 1996.
41. Gilbert A, Brockman R, Carlioz H: Surgical treatment of brachial plexus birth palsy. Clin Orthop 264: 39-47, 1991.
42. Boome R S, Kaye J C: Obstetric traction injuries of the brachial plexus: Natural history, indications for surgical repair and results. J Bone Joint Surg 70B: 571-6, 1988.
43. van Ouwerkerk W J, van der Sluijs J A, Nollet F, et al.: Management of obstetric brachial plexus lesions: State of the art and future developments. Childs Nerv Syst 16 (10-11): 638-44, 2000.
44. Piatt J H, Hudson A R, Hoffman H J: Preliminary experiences with brachial plexus explorations in children: Birth injury and vehicular trauma. Neurosurgery 22: 715-23, 1988.
45. Hunt D: Surgical management of brachial plexus birth injuries. Dev Med Child Neurol 30: 821-8, 1988.
46. Anand P, Birch R: Restoration of sensory function and lack of long-term chronic pain syndromes after brachial plexus injury in human neonates. Brain 125 (Pt 1): 113-22, 2002.
47. Neary D, Ochoa J L, Gilliatt R W: Subclinical entrapment neuropathy in man. J Neurol Sci 24: 283-98, 1975.
48. Graff-Radford S B, Jaeger B, Reeves J L: Myofascial pain may present clinically as occipital neuralgia. Neurosurgery 19: 610-3, 1986.
49. Hunter C R, Mayfield F H: Role of the upper cervical roots in the production of pain in the head. Am J Surg 48: 743-51, 1949.
50. Poletti C E, Sweet W H: Entrapment of the C2 root and ganglion by the atlanto-epistrophic ligament: Clinical syndrome and surgical anatomy. Neurosurgery 27: 288-91, 1990.
51. Anthony M: Headache and the greater occipital nerve. Clin Neurol Neurosurg 94 (4): 297-301, 1992.
52. Weiner R L, Reed K L: Peripheral neurostimulation for control of intractable occipital neuralgia. Neuro-modulation 2 (3): 217-21, 1999.
53. Freund B J, Schwartz M: Treatment of chronic cervical-associated headache with botulinum toxin a: A pilot study. Headache 40 (3): 231-6, 2000.
54. Weinberger L M: Cervico-occipital pain and its surgical treatment. Am J Surg 135: 243-7, 1978.
55. Bogduk N: Local anesthetic blocks of the second cervical ganglion. A technique with application in occipital headache. Cephalalgia 1: 41-50, 1981.
56. Bovim G, Fredriksen T A, Stolt-Nielsen A, et al.: Neurolysis of the greater occipital nerve in cervicogenic headache. A follow up study. Headache 32 (4): 175-9, 1992.
57. Katz J N, Simmons B P: Clinical practice. Carpal tunnel syndrome. N Engl J Med 346 (23): N Engl J Med: 1807-12, 2002.
58. Laha R K, Lunsford L D, Dujovny M: Lacertus fibrosus compression of the median nerve. J Neurosurg 48: 838-41, 1978.
59. Nakano K K, Lundergan C, Okihiro M: Anterior interosseous nerve syndromes: Diagnostic methods and alternative treatments. Arch Neurol 34: 477-80, 1977.
60. Feldman R G, Goldman R, Keyserling W M: Classical syndromes in occupational medicine: Peripheral nerve entrapment syndromes and ergonomic factors. Am J Ind Med 4: 661-81, 1983.
61. Padua L, Aprile I, Caliandro P, et al.: Carpal tunnel syndrome in pregnancy: Multiperspective follow-up of untreated cases. Neurology 59: 1643-6, 2002.
62. Phalen G S: The carpal tunnel syndrome. Clinical evaluation of 598 hands. Clin Ortho Rel Res 83: 31, 1972.
63. Sandzen S C: Carpal tunnel syndrome. Am Fam Physician 24: 190-204, 1981.
64. Upton R M, McComas A J: The double crush in nerve entrapment syndromes. Lancet 11: 359-62, 1973.
65. Wilbourn A J, Gilliatt R W: Double-crush syndrome: A critical analysis. Neurology 49: 21-9, 1997.
66. Rempel D M, Harrison R J, Barnhart S: Work-related cumulative trauma disorders of the upper extremity. JAMA 267: 838-42, 1992.
67. Wilkins R H, Rengachary S S, (eds.): Neurosurgery. McGraw-Hill, New York, 1985.
68. Linskey M E, Segal R: Median nerve injury from local steroid injection in carpal tunnel syndrome. Neurosurgery 26: 512-5, 1990.
69. Pagnanelli D M, Barrer S J: Bilateral carpal tunel release at one operation: Report of 228 patients. Neurosurgery 31: 1030-4, 1992.
70. Pagnanelli D M, Barrer S J: Carpal tunel syndrome: Surgical treatment using the paine retinaculatome. J Neurosurg 75: 77-81, 1991.
71. Louis D S, Greene T L, Noellert R C: Complications of carpal tunnel surgery. J Neurosurg 62: 352-6, 1985.
72. Brazis P W, Masdeu J C, Biller J: Localization in clinical neurology. 2nd ed. Little Brown and Company, Boston, 1990.
73. Harrop J S, Hanna A, Silva M T, et al.: Neurological manifestations of cervical spondylosis: An overview of signs, symptoms, and pathophysiology. Neurosurgery 60: Diagnosis and treatment of cervical spondylosis: S1-14-20, 2007.
74. Dumitru D: Elecctrodiagnostic medicine. Hanley and Belfus, Philadelphia, 1995: pp 1233.
75. Bonney G: Iatrogenic injuries of nerves. J Bone Joint Surg 68B: 9-13, 1986.
76. McGowan A J: The results of transposition of the ulnar nerve for traumatic ulnar neuritis. J Bone Joint Surg 32B: 293-301, 1950.
77. Practice parameter: Electrodiagnostic studies in ulnar neuropathy at the elbow. American association of electrodiagnostic medicine, American Academy of Neurology, and American academy of physical medicine and rehabilitation. Neurology 52 (4): 688-90, 1999.
78. Campbell W W: Guidelines in electrodiagnostic medicine. Practice parameter for electrodiagnostic studies in ulnar neuropathy at the elbow. Muscle Nerve Suppl 8: S171-205, 1999.
79. Cartwright M S, Chloros G D, Walker F O, et al.: Diagnostic ultrasound for nerve transection. Muscle Nerve 35 (6): Muscle Nerve: 796-9, 2007.
80. Le Roux P D, Ensign T D, Burchiel K J: Surgical decompression without transposition for ulnar neuropathy: Factors determining outcome. Neurosurgery 27: 709-14, 1990.
81. Janjua R M, Fernandez J, Tender G, et al.: Submuscular transposition of the ulnar nerve for the treatment of cubital tunnel syndrome. Neurosurgery 63 (4 Suppl 2): Neurosurgery: 321-4; discussion 324-5, 2008.
82. Spinner R J, O’Driscoll S W, Jupiter J B, et al.: Unrecognized dislocation of the medial portion of the triceps: Another cause of failed ulnar nerve transposition. J Neurosurg 92 (1): J Neurosurg: 52-7, 2000.
83. Bartels R H, Verhagen W I, van der Wilt G J, et al.: Prospective randomized controlled study comparing simple decompression versus anterior subcutaneous transposition for idiopathic neuropathy of the ulnar nerve at the elbow: Part 1. Neurosurgery 56 (3): Neurosurgery: 522-30; discussion 522-30, 2005.
84. Biggs M, Curtis J A: Randomized, prospective study comparing ulnar neurolysis in situ with submuscular transposition. Neurosurgery 58 (2): Neurosurgery: 296-304; discussion 296-304, 2006.
85. Tindall S C: Comment on LeRoux P D, et al.: Surgical decompression without transposition for ulnar neuropathy: Factors determining outcome. Neurosurgery 27: 714, 1990.
86. Bartels R H M A, Menovsky T, Van Overbeeke J J, et al.: Surgical management of ulnar nerve compression at the elbow: An analysis of the literature. J Neurosurg 89: 722-7, 1988.
87. Youmans J R, (ed.) Neurological surgery. 3rd ed., W. B. Saunders, Philadelphia, 1990.
88. Shea J D, McClain E J: Ulnar-nerve compression syndromes at and below the wrist. J Bone Joint Surg 51A: 1095-103, 1969.
89. Cavallo M, Poppi M, Martinelli P, et al.: Distal ulnar neuropathy from carpal ganglia: A clinical and electrophysiological study. Neurosurgery 22: 902-5, 1988.
90. Roles N C, Maudsley R H: Radial tunnel syndrome: Resistant tennis elbow as a nerve entrapment. J Bone Joint Surg 54B: 499-508, 1972.
91. McKowen H C, Voorhies R M: Axillary nerve entrapment in the quadrilateral space: Case report. J Neurosurg 66: 932-4, 1987.
92. de Laat E A T, Visser C P J, Coene L N J E M, et al.: Nerve lesions in primary shoulder dislocations and humeral neck fractures. J Bone Joint Surg 76B: 381-3, 1994.
93. Hadley M N, Sonntag V K H, Pittman H W: Suprascapular nerve entrapment: A summary of seven cases. J Neurosurg 64: 843-8, 1986.
94. Fritz R, Helms C A, Steinbach L S, et al.: Suprascapular nerve entrapment: Evaluation with MR imaging. Radiology 182: 437-44, 1992.
95. Callahan J D, Scully T B, Shapiro S A, et al.: Suprascapular nerve entrapment: A series of 27 cases. J Neurosurg 74: 893-6, 1991.
96. Stevens H I: Meralgia paresthetica. Arch Neurol Psychiatry 77: 557-74, 1957.
97. Williams P H, Trzil K P: Management of meralgia paresthetica. J Neurosurg 74: 76-80, 1991.
98. Devers A, Galer B S: Topical lidocaine patch relieves a variety of neuropathic pain conditions: An open-label study. Clin J Pain 16 (3): Clin J Pain: 205-8, 2000.
99. Aldrich E F, Van den Heever C: Suprainguinal ligament approach for surgical treatment of meralgia paresthetica. Technical note. J Neurosurg 70: 492-4, 1989.
100. Kars H Z, Topaktas S, Dogan K: Aneurysmal pero-neal nerve compression. Neurosurgery 30: 930-1, 1992.
101. Wilbourn A J: The thoracic outlet syndrome is over-diagnosed. Arch Neurol 47: 328-30, 1990.
102. Burke D T, Burke M M, Stewart G W, et al.: Splinting for carpal tunnel syndrome: In search of the optimal angle. Arch Phys Med Rehabil 75 (11): 1241-4, 1994.
103. Walker W C, Metzler M, Cifu D X, et al.: Neutral wrist splinting in carpal tunnel syndrome: A comparison of night-only versus full-time wear instructions. Arch Phys Med Rehabil 81 (4): 424-9, 2000.
104. Gelberman R H, Aronson D, Weisman M H: Carpal-tunnel syndrome. Results of a prospective trial of steroid injection and splinting. J Bone Joint Surg 62 (7): 1181-4, 1980.
105. Katz J N, Keller R B, Simmons B P, et al.: Maine carpal tunnel study: Outcomes of operative and non-operative therapy for carpal tunnel syndrome in a community-based cohort. J Hand Surg Am 23 (4): 697-710, 1998.
106. Brown R A, Gelberman R H, Seiler J G, 3rd, et al.: Carpal tunnel release. A prospective, randomized assessment of open and endoscopic methods. J Bone Joint Surg 75 (9): 1265-75, 1993.