Andrew M. Intlekofer and Steven M. Horwitz
Definition
• Neoplasms arising from mature T lymphocytes w/1º involvement of skin but potential involvement of blood, BM, LNs, visceral organs
• “CTCL” most often refers to mycosis fungoides or Sézary syndrome but can signify any of the cutaneous lymphoma entities listed below
Epidemiology
• Comprise approximately 4–5% of all NHL, male > female
Clinical Presentation
• Patch = any size skin lesion w/o significant elevation or induration (may have hypo- or hyperpigmentation, scaling, crusting, poikiloderma)
• Plaque = any size skin lesion that is elevated or indurated (may have ulceration)
• Tumor = >1-cm diameter solid or nodular lesion w/depth and/or vertical growth
• Erythroderma = erythema of nearly the entire cutaneous surface
• Systemic sx/signs = pruritus; alopecia; LAN; HSM; B sx (wt loss >10%, fevers, sweats)

Diagnostic Evaluation
• Physical: Complete skin examination w/estimation of %BSA involved
• Bx: Skin bx, LN bx if present
• Immunophenotype (IHC or flow): T-cell markers, CD2, CD3, CD4, CD5, CD7, CD8, CD25, CD26, CD30, CD45RO, CD56, granzyme, perforin, TCR α/β/γ/δ
• Cytogenetics/FISH: Not necessary for dx; IRF4/MUM1 rearrangement present in PCALCL, ALK translocations not present [t(2;var)]
• Molecular diagnostics for clonal TCR β or γ rearrangement
• Lab evaluation: CBC w/diff, peripheral smear, CMP, LDH, HBV sAg/cAb, HCV Ab, HIV, HTLV-1/2, peripheral blood flow cytometry
• BM aspirate & core bx: Not routinely necessary for MF/SS, but should be done if extracutaneous disease suspected or if unexplained cytopenia
• Imaging: CT C/A/P + FDG PET usu required to r/o systemic disease
Staging and Risk Stratification
• TNMB staging system for MF/SS(Blood 2007;110:1713)
T = skin, N = nodes, M = visceral, B = blood; T1 = patches, plaques, or flat lesions on <10% of skin; T2 = >10% of skin; T3 = tumors; T4 = erythroderma >80% of body
N0 = no nodal involvement; N1–N3 = clinically abnl LN
M0 = no visceral organ involvement; M1 = visceral organ involvement
B0 = no significant blood involvement (<5% Sézary cells); B1 = low blood tumor burden (>5% Sezary cells); B2 = high blood tumor burden (>1000/μL Sezary cells)
Adv stages (IIB–IVB) include T3, T4, B2, N3, & M1, respectively
• Poor risk features for MF/SS: T3, T4, any degree of blood involvement, ≠ LDH, large cell transformation, folliculotropic pattern(JCO 2010;28:4730)
• Other cutaneous lymphomas use Ann Arbor staging system (as detailed in prior lymphoma sections) or alternative TNM system (Blood 2007;110:479)
Principles of Treatment
• Skin-directed topical therapies for limited superficial disease: Usu cared for by dermatologist alone or oncologist in collaboration w/dermatologist
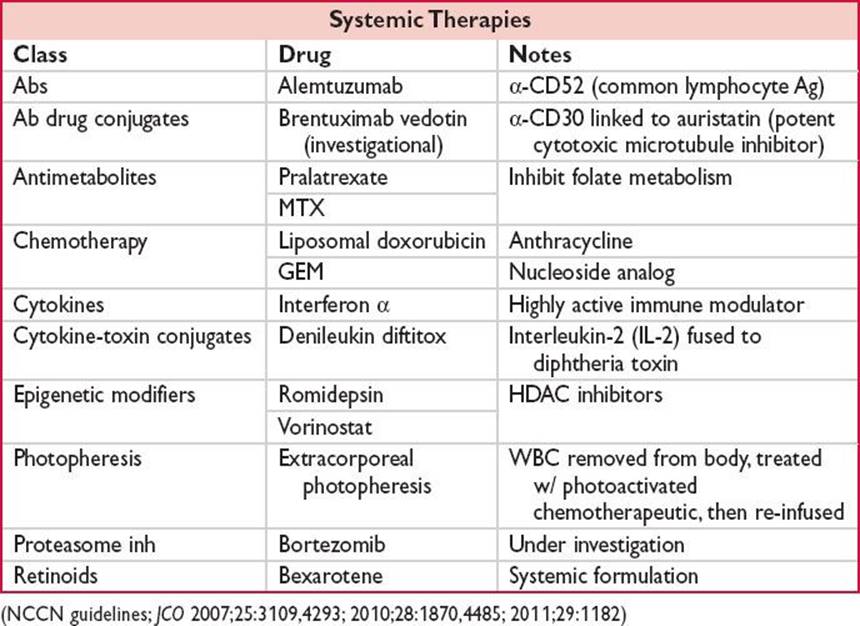
• Systemic therapies reserved for adv stage or refractory cutaneous disease

Supportive Care
• Dermatology: Aggressive dermatologic care for CTCL pts; sometimes burn wound care needed for pts w/extensive desquamation
• Skin CA screening: UV light tx → may increase risk of nonmelanoma skin CA w/long-term use
• Prophylactic abx: Prevent infxn in pts w/extensive skin invlmnt
• Pruritus: Moisturizers, topical steroids, antihistamines, etc.